
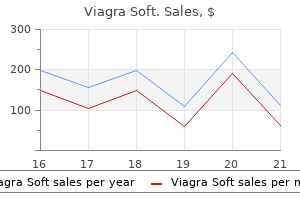
Viagra Soft dosages: 100 mg, 50 mg
Viagra Soft packs: 10 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

50 mg viagra soft generic visa
Mechanism of Action Inhibits the dipeptidyl peptidase-4 enzyme to gradual inactivation of incretin hormones erectile dysfunction drugs viagra viagra soft 50 mg buy discount line. When blood glucose stage is elevated icd 9 code erectile dysfunction 2011 viagra soft 50 mg purchase without prescription, incretin hormones improve insulin synthesis and launch from pancreatic beta cells. Contraindications Diabetic ketoacidosis, hypersensitivity to alogliptin or its components including anaphylaxis, angioedema, or severe cutaneous antagonistic reactions, sort 1 diabetes � Emphasize the necessity to observe an exercise program and a food plan control program throughout alogliptin remedy. Also look ahead to evidence of ischemic colitis, corresponding to rectal bleeding, bloody diarrhea, or new or worsening belly ache. Replaces the enzyme alpha1-antitrypsin, which normally inhibits the proteolytic enzyme elastase in patients with alpha1antitrypsin deficiency. Without alpha1proteinase inhibitor, elastase assaults and destroys alveolar membranes and causes emphysema. Tell her to stop taking alosetron immediately and to notify prescriber if evidence of ischemic colitis or constipation arises. After stoppers are dry, remove protecting cover from diluent end of transfer system and insert into center of upright diluent vial. Then remove protective cover from drug end of transfer gadget, invert diluent vial with connected switch device, and utilizing minimal drive, insert drug end of transfer system into heart of rubber stopper of upright drug vial. Make certain flange of transfer system rests on stopper surface in order that diluent flows into drug vial. If opposed reactions happen, sluggish infusion price or stop infusion till signs subside. A � Tell patient to report immediately early proof of allergic response, similar to chest tightness, hassle breathing, faintness, hives, wheezing, and another unusual signs. No greater than 2 doses, separated by 1 hr, must be given on a single day throughout preliminary titration section. If no response, dosage increased in increments to 500 or 1,000 mcg till erection suitable for intercourse (not exceeding 1-hr duration) is achieved. A naturally occurring prostaglandin, alprostadil interacts with specific membrane-bound receptors within the corpora cavernosa cells of the penis. These chemical reactions trigger the trabecular easy muscle tissue to relax and the cavernosal arteries to dilate. Blood move to the penis is then increased, which distends the penile lacunar spaces and compresses the veins, trapping blood within the penis and causing it to become enlarged and inflexible. Be aware that this system makes use of a superfine 29 gauge needle, so care must be taken to prevent needle breakage. In addition, patient should be assessed intently for drug effectiveness, as system malfunction or failure has occurred with this product. Notify prescriber, and be prepared to treat patient for priapism if erection lasts longer than four hours. Teach him how to correctly administer intracavernous injections or urethral suppositories. Inform him that the aim of treatment is to produce an erection that lasts no longer than 1 hour. Inform affected person using urethral suppositories not to exceed two doses in a 24-hour interval. If needle breaks throughout injection and he can see and grasp damaged end, he ought to take away it and contact prescriber. Tell affected person to hold penis upright after insertion and to roll it firmly between his palms to distribute drug. Urge him to use a condom to decrease threat of blood-borne disease, as a outcome of injection may cause minor bleeding at injection web site. To avoid acute bleeding issues, treatment for acute ischemic stroke should start inside three hr after onset of stroke signs and solely after computed tomography or different diagnostic imaging method excludes intracranial hemorrhage. Plasmin breaks down fibrin, fibrinogen, and other clotting components, which dissolves the thrombus. Indications and Dosages gastric hyperacidity, gastritis, hiatal hernia, peptic esophagitis, and peptic ulcers; to forestall phosphate renal calculus formation; to scale back hyperphosphatemia in continual renal failure alvimopan aluminum carbonate capsules, suspension, tablets forty five Adults. Varies Peak Duration Unknown 20�40 min* Mechanism of Action Neutralizes or reduces gastric acidity, increasing stomach and duodenal alkalinity. Binds with phosphate ions in gut to type insoluble aluminumphosphate compounds, which decrease blood phosphate stage. Initial: 12 mg 30 min to 5 hr before surgical procedure, followed by 12 mg twice daily, starting the day after surgery for up to 7 days or until discharge. This motion alleviates postoperative ileus by causing bowel operate to return extra rapidly after a part of bowel has been removed and an end-to-end anastomosis performed. For sufferers with impaired renal function, dosage adjusted to 200 mg on day 1 and then to a hundred mg every day if creatinine clearance is 30 to 50 ml/min/1. To prevent and deal with respiratory tract capsules, syrup, tablets forty seven postsynaptic receptors more delicate to dopamine. Amantadine may inhibit influenza A viral replication by blocking uncoating of virus and release of viral nucleic acid into respiratory epithelial cells. It additionally might intervene with early replication of viruses that have already penetrated cells. A Contraindications Angle-closure glaucoma, hypersensitivity to amantadine or its parts an infection brought on by influenza A Interaction medicine Adults and children age 12 and over. Amantadine additionally may stimulate dopamine receptors or make * Antidyskinetic motion; antiviral motion unknown. If therapeutic response declines, count on to improve dosage or discontinue drug briefly, as ordered. During an influenza epidemic, anticipate drug to be given every day all through the epidemic, which typically lasts 6 to eight weeks. If affected person has previously received inactivated influenza A vaccine, prescriber may discontinue it when positive that patient has developed lively immunity in opposition to the virus. If affected person receives inactivated influenza A vaccine on the identical time amantadine remedy starts, expect amantadine to be given for two to three weeks. These embody fever, hypertension or hypotension, involuntary motor exercise, psychological changes, muscle rigidity, tachycardia, and tachypnea. Be ready to present supportive remedy and additional drug therapy, as prescribed. Initial: 5 mg 3 times daily or 4 occasions every day, elevated at 1- to 2-day intervals to optimum dosage primarily based on affected person response. Usual: Highly individualized but usually 5 to 50 mg three times day by day or four occasions day by day. Onset Peak Duration 20�30 min Unknown 3�8 hr Mechanism of Action Attaches to acetylcholinesterase and blocks its breakdown. Then count on to scale back dosage to previous effective stage and to use this as upkeep dosage. If patient receives greater than 200 mg daily, watch intently for overdose (cholinergic crisis), similar to belly cramps, diarrhea, nausea, vomiting, increased salivation, diaphoresis, difficulty swallowing, blurred vision, miosis, hypertension, fasciculations, and voluntary muscle paralysis. Rapid Peak Duration Immediate Unknown Unknown Unknown Unknown amiloride hydrochloride irritation, maintain hydration during therapy. Contraindications Hypersensitivity to amiloride; impaired renal function; serum potassium degree above 5.
Generic viagra soft 50 mg amex
Tell him that patch ought to remain in place for 4 hours or till the sumatriptan iontophoretic transdermal system mild has turned off erectile dysfunction treatment after prostatectomy generic viagra soft 100 mg online. Teach him how to erectile dysfunction drugs malaysia buy cheap viagra soft 100 mg line eliminate the used patch, keeping it away from youngsters and pets. Tacrine binds with and inhibits cholinesterases, making extra intact acetylcholineavailable in cholinergic synapses, as shown under proper. Nursing Considerations � Instruct affected person to take tacrine on an empty stomach, and advise caregiver to ensure that the patient swallows the drug. For patients with postoperative oliguria, initial dose administered no sooner than 6 hr and inside 48 hr of transplantation, however may be delayed till renal perform reveals proof of restoration. This inhibition might stop dephosphorylation and translocation of nuclear issue of activated Tcells, a nuclear element thought to provoke gene transcription for the formation of lymphokines. Mechanism of Action To prevent organ rejection in patients Adults having kidney or liver transplantation. For patients with hepatic or renal impairment, dosage saved at decrease end of vary with potential need for additional discount. When Hecoria or Prograf formulation is used to forestall both kidney or heart transplant rejection, azathiprine could additionally be substituted for mycophenolate mofetil. Make certain emer gency equipment and drugs, such as aqueous solution of epinephrine and oxygen, are instantly available. Evidence of encephalopathy consists of headache, impaired consciousness, lack of motor perform, psychiatric disturbance, seizures, and tremors. T 1126 tadalafil tablets � Emphasize the importance of getting repeated laboratory tests while taking tacrolimus, and urge compliance. Tell him to report frequent urination or an increase in thirst, hunger, or fatigue. To deal with benign prostatic hyperplasia tadalafil Adcirca, Cialis Class and Category Chemical class: Phosphodiesterase inhibitor Therapeutic class: Antiimpotence Pregnancy class: B To deal with erectile dysfunction Adults. For sufferers with a creatinine clearance of 30 to 50 mg/ ml, preliminary dosage reduced to 2. To treat benign prostatic hyperplasia tablets and erectile dysfunction Indications and Dosages tablets Adults. Initial: 10 mg taken 1 hr earlier than sexual activity; dosage decreased to 5 mg or increased to 20 mg, as prescribed, primarily based on medical response. For patients with a creatinine clearance of 30 to 50 ml/min, who take drug on an asneeded basis, initial dosage decreased to 5 mg every day and maximum dosage not to exceed 10 mg every 48 hr. To deal with pulmonary arterial hyper tablets (adcirca) tension so as to improve train capability in patients categorized as group 1 by the world well being organization Adults. For patient already taking tadalafil and being pre scribed ritonavir, tadalafil temporarily discontinued for no much less than 24 hours before ritonavir starts. Then, after at least 1 week of ritonavir, tadalafil restarted at 20 mg once day by day and then elevated to forty mg as quickly as day by day, as tolerated. Peak Duration Unknown 30 min�6 hr Unknown tadalafil 1127 Mechanism of Action Enhances the impact of nitric oxide launched in the penis during sexual stimulation. Alternatively, if the affected person chooses to take a smaller dose of tadalfil every day, encourage him to take it at about the identical time daily, whatever the timing of sexual activity. Tell him to seek instant medical consideration if he has a sudden loss of vision or listening to. Mechanism of Action May block the effects of estrogen on breast tissue by competing with estrogen for estrogenreceptor binding websites. Contraindications Hypersensitivity to tamoxifen or its compo nents; ladies at high risk for breast cancer sure that affected person has been informed about serious or doubtlessly life threatening opposed effects related to tamoxifen earlier than therapy begins. Be aware that girls with ductal carcinoma in situ and those at excessive threat for breast cancer are extra doubtless to develop uterine cancer, stroke, or pulmonary emboli than others receiving tamoxifen. Urge affected person to seek the assistance of prescriber if adverse reactions, similar to nausea and vomiting, are interfering with dosage schedule. Mechanism of Action T Contraindications Interaction drugs Hypersensitivity to tamsulosin, quinazolines, or their components alpha blockers: Additive effects of both drugs cimetidine: Risk of decreased tamsulosin clearance 1130 tapentadol increase risk for complications with cataract surgical procedure. Maximum: seven hundred mg on first day; 600 mg day by day thereafter dosage adjustment On first day of therapy, second dose may be given as soon as 1 hour after first dose, if wanted. Initial: 50 mg followed by dosage elevated, as needed with subsequent doses cut up into two equal doses given twice every day. Initial: 50 mg adopted by dosage elevated, as needed no ahead of each three days with subsequent doses break up into two equal doses given twice day by day. Onset Unknown Peak 1 hr Duration four hr Mechanism of Action Binds with and activates opioid receptors (mainly mu receptors) in mind and spinal cord and inhibits norepinephrine reuptake to produce analgesia. Also use cautiously in patients with head injury or situations during which increased intracranial strain could occur as a result of drug could obscure the signs and signs. Also use cautiously in sufferers with delicate to average renal or hepatic dysfunction and in patients with biliary tract illness, together with acute pancreatitis, as a outcome of drug may trigger spasm of the sphincter of Oddi. If respiratory fee drops under 10 breaths per minute, notify prescriber, count on drug to be discontinued, and supply needed supportive care, which may embody an opioid antagonist such as naloxone, as ordered. Onset Unknown Peak 1�2 hr Duration 24 hr Mechanism of Action Inhibits cell wall synthesis and alters the permeability of bacterial membranes, inflicting cell wall lysis and cell demise. If renal function declines, notify prescriber and anticipate to discontinue telavancin. When able to administer drug, further Nursing Considerations patient instructing dilute doses of a hundred and fifty mg to 800 mg in a hundred to 250 ml of 5% dextrose injection, zero. Doses lower than one hundred fifty mg or higher than 800 mg should be further diluted in a volume that yields a last concentration of 0. Provide supportive care, such as fluid and electrolyte replacement, protein supplementation, antibiotic therapy to deal with C. Collect blood samples for coagulation tests as close as potential to administration of next dose of telavancin to reduce interference. For patients with severe renal impairment and coexisting hepatic impairment, dosage reduced to four hundred mg as soon as daily for 7 to 10 days. If it occurs, notify prescriber and anticipate to withhold drug and give fluids, electrolytes, protein, and an antibiotic efficient against Clostridium difficile. Explain that telithromycin can cause hassle focusing eyes, especially for first 30 minutes after a dose. Be ready to deal with symptomatic hypotension by placing affected person in supine place and giving normal saline solution, as ordered. If current, discon tinue temazepam immediately, notify prescriber, and supply supportive care. Plasmin breaks down fibrin, fibrinogen, and other clotting factors, resulting in dissolution of a coronary artery thrombus. Contraindications Active internal bleeding, aneurysm, arteriovenous malformation, bleeding issues, mind tumor, history of cerebro vascular accident, hypersensitivity to tenecteplase or its parts, intracranial or intraspinal surgical procedure or trauma inside previous 2 months, severe uncontrolled hypertension tenecteplase for injection immediately before use as a end result of drug incorporates no antibacterial preser vatives. Withdraw 10 ml of supplied (preservativefree) sterile water for injection into syringe, and inject complete contents into vial containing tenecteplase dry powder, directing stream of diluent into powder.
Purchase viagra soft 50 mg without prescription
Current standing of sporadic and neurofibromatosis kind 1-associated malignant peripheral nerve sheath tumors erectile dysfunction doctors tucson az viagra soft 50 mg buy on line. Alteration in a new gene encoding a putative membrane-organizing protein causes neurofibromatosis type 2 erectile dysfunction agents buy viagra soft 50 mg line. A novel moesin-, ezrin-, radixin-like gene is a candidate for the neurofibromatosis 2 tumor suppressor. Brain tumors in individuals with familial adenomatous polyposis: a cancer registry experience and pooled case report evaluation. Xeroderma pigmentosum: cutaneous, ocular, and neurologic abnormalities in 830 revealed circumstances. Homozygous deletion in Wilms tumours of a zinc-finger gene recognized by chromosome leaping. Retinoblastoma and long arm deletion of chromosome 13: makes an attempt to outline the deleted section. Chromosomal translocations in lymphoid neoplasia: a reappraisal of the recombinase mannequin. Site-specific recombination of the tal-1 gene is a standard occurrence in human T cell leukemia. The Bcr gene recombines preferentially with Alu components in advanced Bcr-Abl translocations of persistent myeloid leukaemia. Alternating purine-pyrimidine tracts could promote chromosomal translocations seen in a variety of human lymphoid tumours. Different genetic pathways in leukemogenesis for patients presenting with therapy-related myelodysplasia and therapy-related acute myeloid leukemia. Therapy-related acute myeloid leukemia following remedy with epipodophyllotoxins: estimating the risks. Translocations, grasp genes, and differences between the origins of acute and persistent leukemias. Structural and functional chimerism outcomes from chromosomal translocation in lymphoid tumors. Activation and somatic mutation of the translocated c-myc gene in Burkitt lymphoma cells. The 2p breakpoint of a 2;eight translocation in Burkitt lymphoma interrupts the V kappa locus. Translocation of an immunoglobulin kappa locus to a area three of an unrearranged c-myc oncogene enhances c-myc transcription. C-myc and immunoglobulin kappa gentle chain constant genes are on the 8q+ chromosome of three Burkitt lymphoma strains with t(2;8) translocations. A novel alteration within the construction of an activated c-myc gene in a variant t(2;8) Burkitt lymphoma. Gene encoding the alpha chain of the T-cell receptor is moved instantly downstream of c-myc in a chromosomal 8;14 translocation in a cell line from a human T-cell leukemia. Chromosomal translocation in a human leukemic stem-cell line disrupts the T-cell antigen receptor delta-chain diversity region and results in a beforehand unreported fusion transcript. The tal gene undergoes chromosome translocation in T cell leukemia and probably encodes a helix-loop-helix protein. Segmental and developmental regulation of a presumptive T-cell oncogene in the central nervous system. The t(11;14)(p15;q11) in a T-cell acute lymphoblastic leukemia cell line prompts multiple transcripts, including Ttg-1, a gene encoding a potential zinc finger protein. A novel human homeobox gene lies at the chromosome 10 breakpoint in lymphoid neoplasias with chromosomal translocation t(10;14). The tcl-3 proto-oncogene altered by chromosomal translocation in T-cell leukemia codes for a homeobox protein. Isolation of a yeast artificial chromosome spanning the eight;21 translocation breakpoint t(8;21)(q22;q22. Activation of Evi-1 gene expression in human acute myelogenous leukemias by translocations spanning 300�400 kb on chromosome 3q26. Genes on chromosomes 4, 9, and 19 concerned in 11q23 abnormalities in acute leukemia share sequence homology and/or frequent motifs. The t(15;17) translocation of acute promyelocytic leukaemia fuses the retinoic acid receptor alpha gene to a novel transcribed locus. Molecular analysis of acute promyelocytic leukemia breakpoint cluster area on chromosome 17. Rearrangements and aberrant expression of the retinoic acid receptor alpha gene in acute promyelocytic leukemias. Fusion between a novel Kr�ppel-like zinc finger gene and the retinoic acid receptor locus because of a variant t(11;17) translocation associated with acute promyelocytic leukaemia. A novel class of zinc finger/leucine zipper genes recognized from the molecular cloning of the t(10;11) translocation in acute leukemia. The translocation (6;9) (p23;q34) shows constant rearrangement of two genes and defines a myeloproliferative disorder with particular scientific features. Involvement of a human gene related to the Drosophila spen gene within the recurrent t(1;22) translocation of acute megakaryocytic leukemia. Translocation of c-ab1 oncogene correlates with the presence of a Philadelphia chromosome in persistent myelocytic leukaemia. Specification of Drosophila hematopoietic lineage by conserved transcription elements. Molecular genetics of childhood cancer: implications for pathogenesis, diagnosis, and therapy. Fusion with E2A converts the Pbx1 homeodomain protein right into a constitutive transcriptional activator in human leukemias carrying the t(1;19) translocation. E2A-Pbx1, the t(1;19) translocation protein of human pre-B-cell acute lymphocytic leukemia, causes acute myeloid leukemia in mice. Involvement of a homolog of Drosophila trithorax by 11q23 chromosomal translocations in acute leukemias. A trithorax-like gene is interrupted by chromosome 11q23 translocations in acute leukemias. Therapy-related acute nonlymphocytic leukemia with monocytic features and rearrangement of chromosome 11q. Acute leukemias associated with the 4;11 chromosome translocation have rearranged immunoglobulin heavy chain genes. Clinical and laboratory characteristics of acute leukemia with the 4;11 translocation. Interferon and c-ets-1 genes within the translocation (9;11) (p22;q23) in human acute monocytic leukemia. Human acute leukemia cell line with the t(4;11) chromosomal rearrangement reveals B lineage and monocytic characteristics.
Purchase viagra soft 100 mg line
Prostaglandins additionally play a role in peripheral pain transmission to the spinal wire what do erectile dysfunction pills look like 50 mg viagra soft cheap with mastercard. Contraindications rheumatoid arthritis To relieve signs and symptoms of capsules Adults erectile dysfunction treatment with exercise viagra soft 100 mg cheap otc. For those weighing less than 50 kg (110 lb), expect to begin with lowest recommended dose. Stress the necessity to seek immediate medical consideration if indicators or signs develop, corresponding to epigastric or abdominal pain, indigestion, black or tarry stools, and vomiting blood or materials that resembles espresso grounds. Advise quick medical consideration if signs or signs develop, corresponding to rash, blisters, fever, itching, or other evidence of hypersensitivity. Indications and Dosages To deal with streptococcal tonsillitis, pharyngitis, and pores and skin and soft-tissue infections capsules, oral suspension, tablets Adults and adolescents age 15 and over. This mechanism of motion is handiest towards micro organism that divide quickly, together with many grampositive and gramnegative bacteria. Also, monitor fluid intake and output; decreasing urine output may indicate nephrotoxicity. Mechanism of Action � Instruct patient to report extreme diarrhea or evidence of blood dyscrasia or tremendous infection to prescriber immediately. C cephradine Velosef Class and Category Chemical class: Firstgeneration cephalosporin, 7aminocephalosporanic acid Therapeutic class: Antibiotic Pregnancy class: B To deal with respiratory tract infections capsules, oral suspension Contraindications Hypersensitivity to cephalosporins or their components Interactions drugs Indications and Dosages aminoglycosides, loop diuretics: Increased threat of nephrotoxicity probenecid: Increased and prolonged blood cephradine level Adverse Reactions (other than lobar pneumonia) and pores and skin and soft-tissue infections Adults. Also monitor fluid consumption and output; 234 certolizumab pegol � Tell affected person that yogurt and buttermilk assist maintain intestinal flora and may decrease diarrhea throughout remedy. If hypersensitivity develops, be ready to cease drug and administer antihistamines, corticosteroids, and vasopressors, as ordered. Also prepare to administer oxygen, maintain an open airway, and help with endotracheal intubation, as acceptable. Keep in thoughts that this critical adverse reaction can occur during remedy or as much as several weeks after remedy ends. Also avoid giving anti peristaltic antidiarrheals, similar to atropine and diphenoxylate or loperamide, because they could delay elimination of poisons from the bowel and harm the colon from toxin retention. For reasonable or extreme cases, be ready to administer fluids, electrolytes, and protein replacement as ordered. Maintenance: 400 mg (given as two 200mg injections) each 4 wk if clinical response happens. Maintenance: 200 mg each different wk, or four hundred mg (given as two 200mg injections) every four wk if scientific response happens. Be aware that a falsely negative antigen and antibody check for histoplasmosis could happen in some patients during certolizumab therapy, even when an lively an infection is current. Assess affected person for proof of hepatitis B viral an infection earlier than starting and periodically via out certolizumab therapy. If skin check is positive (induration 5 mm or greater), remedy of latent tuberculosis must start before certolizumab is given, as prescribed. Be aware that a falsely adverse check for latent tuberculosis might occur throughout certolizumab remedy, so any signs and symptoms suggestive of tuberculosis must be rigorously evaluated. Instruct him to report persistent cough, wasting or weight reduction, and lowgrade fever to prescriber. Advise affected person to avoid folks with infections and to comply with all prescribed exams. Emphasize have to hold followup visits and to report unusual or sudden indicators or signs. Then depart vials undisturbed for up to half-hour to enable time for powder to utterly dissolve. Do not depart at room temperature, once reconstituted, for greater than 2 hours earlier than administration. If administration might be delayed, recon stituted drug could be refrigerated as much as 24 hours. Using a 20G needle, withdraw drug from vial utilizing a separate syringe and needle for every vial. Although uncommon, malignancies (especially lymphomas and leukemias) have been reported in patients receiving these medication, including kids. Mechanism of Action As a cholinergic agonist, binds to and activates muscarinic receptors of the parasympathetic nervous system and increases secretions of the exocrine glands, such as salivary glands. Contraindications Acute iritis, angleclosure glaucoma, hypersensitivity to cevimeline or its parts, uncontrolled asthma of absorption, delaying peak concen tration. Advise taking it exactly as prescribed and to not cease taking it abruptly because withdrawal symptoms may occur. Mechanism of Action Produces a bacteriostatic effect on suscep tible organisms by inhibiting protein synthesis, thus preventing amino acids from being transferred to growing polypeptide chains. Keep in thoughts that therapeutic peak levels are 10 to 20 mcg/ml and trough levels are 5 to 10 mcg/ml. Contraindications Hypersensitivity to chlordiazepoxide or its components Indications and Dosages To provide short-term administration of delicate anxiety capsules, tablets Interactions drugs To present short-term management of capsules, tablets Adults. Repeated in 2 to four hr followed by individualized oral dosage if wanted to control signs. Maximum: 1,000 mg daily for ages 2 to 12; 375 mg daily for ages 6 months to 2 years. Admin istered on an intermittent schedule, if wanted, such as alternate days or three to 5 days/wk. Maximum: 1,000 mg every day for kids ages 2 to 12; 375 mg day by day for children ages 6 months to 2 years. Initially, chlorothiazide may scale back blood strain by decreasing extracellular fluid volume, plasma quantity, and cardiac output. After a quantity of weeks, extracellular fluid and plasma quantity and cardiac output return to regular, but peripheral vascular resistance remains decreased. Reconstituted resolution is appropriate with dextrose resolution or normal saline answer for infusion. If used to treat hyper tension, examine blood strain often; antihypertensive effect may not appear for days. After 1 or 2 days, dose elevated by 20 to 50 mg semiweekly till patient is calm. After 2 wk of calmness, dosage steadily reduced to maintenance level of 200 to 800 mg day by day in equally divided doses. Increased progressively over several days up to four hundred mg every 4 to 6 hr for severe instances until conduct is controlled. Maximum: 75 mg/day for children ages 5 to 12 or weighing 50 to a hundred lb; 40 mg daily for youngsters up to age 5 years or weighing up to 50 lb.
50 mg viagra soft best
It provides the pores and skin of the lower leg erectile dysfunction caused by hemorrhoids viagra soft 100 mg generic overnight delivery, pierces the crural fascia in the distal third of the leg does erectile dysfunction cause low sperm count viagra soft 100 mg overnight delivery, and then splits into medial and lateral branches. The larger medial branch Spinal Nerves 261 offers sensory innervation on the medial aspect of the good and the adjoining sides of the second and third toes, communicating with the saphenous nerve on the medial border of the foot. The lateral branch provides the lateral surface of the ankle joint and the adjacent sides of the third and fifth toes, connecting to the sural nerve. Interruption of the superficial fibular nerve happens in lateral compartment syndrome, leading to numbness and burning sensation on the dorsum of the foot. Impaired eversion, but not total loss, because of intactness of the extensor digitorum longus and fibularis tertius can additionally be noticed. Plantar flexion can also be compromised as a outcome of paralysis of the fibularis longus and brevis; nevertheless, dorsiflexion stays potential. Patients stroll with the foot in inverted place, and if prolonged, pes equinovarus may ensue. Injury to the superficial fibular nerve can even happen as the nerve pierces the deep fascia of the distal leg in its course to the dorsum of the foot. In this occasion, the dysfunction is proscribed to a burning sensation in the area of distribution of the nerve on the dorsum of the foot. Trauma to the dorsum of the foot, poorly fitting casts or sneakers, or forceful plantar flexion or eversion of the foot might simply damage the deep fibular nerve. Since the anterior compartment is a confined house sealed by a bony wall and connective tissue septum, which permits no expansion, leg cast (shin splint) can produce compression of the associated vessels and nerves with resultant edema. The stress from the developed edema may be adequate to produce ischemic necrosis of the constructions and signs of anterior compartment syndrome. An intense ache, redness, and swelling confined anterior to the tibia characterize this syndrome. In addition to the above deficits, slight weak point of eversion and inversion of the foot may also be the deep fibular (peroneal) nerve arises from the widespread fibular nerve between the upper a part of fibularis longus and fibula after which descends deep to the extensor digitorum longus and anterior to the interosseous membrane. In the proximal a part of the anterior compartment of the leg, the deep fibular nerve is accompanied by the anterior tibial vessels with various relationship to the vessel (being lateral and then anterior). It innervates the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and fibularis tertius. Immediately proximal to the ankle joint, the deep fibular nerve passes deep to the superior exterior retinaculum and then divides into medial and lateral branches. The medial department, primarily sensory, accompanies the dorsalis pedis artery, coursing in the area between the tendon of the extensor hallucis longus and extensor hallucis brevis muscle. Continuing its descent posterior to the inferior extensor retinaculum, the medial branch passes deep to the extensor hallucis brevis on the dorsum of the foot, operating between the tendons of the extensor hallucis brevis and extensor digitorum longus to supply the net of skin between the massive toe and second toe. The lateral branch (motor) passes anterior to the ankle joint, crosses deep to the extensor digitorum brevis, which supplies, and follows an anterolateral course on the dorsum of the foot. Through its small twigs, the lateral branch provides the extensor hallucis brevis, metatarsophalangeal joints of the middle three toes, and the second dorsal interosseous muscle. The trunk of the deep fibular nerve innervates the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and the fibularis tertius muscle. It carries sensation from the dorsal floor of the skin web between the good toe and the second toe. Injury to the terminal part of the deep fibular nerve on the ankle joint because it courses deep extensor retinaculum produces manifestation of anterior tarsal tunnel syndrome. Injuries to the deep fibular nerve can also occur subsequent to a ganglion cyst, osteophyte, hypertrophied extensor hallucis brevis, or surgical procedure of the foot to scale back Lisfranc fracture (fractures of the cuboid, navicular bones, and the metatarsals bones and their subsequent displacement). This type of damage occurs when the foot is plantar flexed and the toes are dorsiflexed particularly in sufferers wearing high heels. Numbness and tingling in the dorsal web skin between the big and second toes and aching ache within the dorsum of the foot and the ankle joint are exacerbated by activity such as strolling or inactivity as in sleeping. Motor deficits are negligible due to the compensatory action of the extensor digitorum longus and the extensor halluces longus. Abnormalities detected in the sural nerve might help analysis of sarcoidosis, main amyloidosis, and first biliary cirrhosis. Disorders of the adrenocorticotropic and thyroid hormones can also produce modifications on this nerve. Before its division deep to the flexor retinaculum, the tibial nerve gives off a medial calcaneal branch, which carries sensation from the skin of the heel. The medial plantar nerve, the most important department, proceeds anteriorly lateral to the lateral plantar artery, deep to the abductor hallucis, and then between the latter muscle and the flexor digitorum brevis. It supplies cutaneous branches that pierce the plantar aponeurosis and supply the pores and skin of the medial two-thirds of the plantar floor of the foot. At the bases of the metatarsal bones, the medial plantar nerve provides off three common plantar digital nerves. Each branch additional divides into two branches to supply the adjoining sides of the hallux and the second toe, and second and third toes, in addition to the third and fourth toes. Following its division from the sciatic nerve, it descends vertically posterior to the popliteal fossa, superficial to the popliteal vein, where it provides rise to the sural nerve. It descends anterior to the triceps surae muscle (gastrocnemius and soleus), anterior to the fibrous band between the tibial and fibular origin of the soleus accompanied by the posterior tibial vessels. It innervates the popliteus muscle, the muscle tissue of the posterior compartment of the leg, and the sole of the foot. The sural nerve joins a communicating branch from the widespread fibular nerve and later courses between the 2 heads of the gastrocnemius muscle, accompanied by the brief saphenous nerve. In its downward course, it lies lateral to the calcaneal tendon after which between the lateral malleolus and calcaneus. During its course with the brief saphenous vein within the upper leg, it connects to the terminal branches of the posterior cutaneous nerve of the thigh and later on the lateral side of the foot it connects to the superficial fibular nerve. The sural nerve provides sensory branches to the decrease lateral and posterior leg and the lateral border of the foot and fifth toe. The lateral plantar nerve courses anteriorly on the lateral facet of the lateral plantar artery, between the flexor digitorum brevis and quadratus plantae. The nerve trunk supplies the quadratus plantae and abductor digiti minimi and carries sensation from the lateral one and a half of the plantar surface of the foot. The lateral plantar nerve then passes between the abductor digiti minimi and flexor digitorum brevis to divide into superficial and deep branches. Through the superficial branch, it supplies the pores and skin of the lateral side of the fifth toe, the flexor digiti minimi, interossei in the fourth intermetatarsal space, and adjoining parts of the fourth and fifth toes. The deep branch of the lateral plantar nerve innervates all lumbricals excluding the first, the adductor halluces, and all interossei aside from these within the fourth intermetatarsal space. Damage to the tibial nerve can occur in a fracture of the distal finish of the femur, or as a end result of trauma to the popliteal fossa, or subsequent to entrapment inside the tarsal tunnel.
Viagra soft 100 mg buy discount line
It equally impacts men and women with some variations in course and onset between the sexes erectile dysfunction causes nhs 100 mg viagra soft discount amex. Greater than half of all male schizophrenics erectile dysfunction herbal treatment buy 50 mg viagra soft, however less than one-third of feminine schizophrenics, could show manifestations earlier than the age of 25. Studies have shown that the peak age of onset for males is 15�25 years, whereas for ladies, it ranges between the ages of 25 and 35. In common, the result for female schizophrenics may be better than the end result for male schizophrenics. A notably fascinating finding is that individuals who later develop schizophrenia usually tend to have been born in the winter and early spring months and less prone to have been born in late spring or summer time. The disturbances associated with schizophrenia embody incoherence of thought (hallucinations or false perception), feeling, and behavior. Patients could have issue establishing social relationships and experience delusions, mood disturbances, auditory hallucination, and even motor overactivity and violent or bizarre conduct. These symptoms, that are variable in severity, may be categorized into positive, adverse, and disorganized signs. Positive manifestations principally comprise delusions (paranoia, grandiosity, bizarre ideas, and tactile delusions) and hallucinations (mainly auditory). Withdrawal, lethargy, lack of spontaneity and initiative, motivational impairment, and indifference to emotional stimuli represent the adverse manifestations of this psychotic dysfunction. Lack of thought content, illogical ideas, and incoherence are the first disorganizational symptoms of this illness. Some patients are categorized as schizotypal when gentle constructive and disorganizational signs are present. When mood-related modifications are predominant on this disease, a schizoaffective dysfunction is produced. Genetic, environmental, and neurophysiological components may be responsible for this illness. One mannequin for the integration of organic, social, and environmental components is the stress-diathesis model. This mannequin states that an individual with a particular vulnerability (diathesis) might develop signs of schizophrenia when subjected to specific environmental stress components. Recent research has implicated a pathophysiological role for the limbic system, prefrontal cortex, and basal nuclei. According to the ontogenic speculation of schizophrenia, the dendrites of the pyramidal cells of the hippocampal gyrus seem to bear disorientation subsequent to deranged embryological improvement. The degree of deviation of the apical shafts of the pyramidal cells could stay proportional to the severity of symptoms and a quantity of hospitalizations. Due to this directional deviation, abnormal afferents converge on these dendrites. Additionally, throughout development, primitive neurons migrate from the neuroepithelial zone to the hippocampus via the radial glial cells. These radial glial cells operate both as directional guides and a structural help for the migrating neuroblasts. Without this support and steerage, the neuroblasts fail to develop and migrate correctly. This mechanism is crucial for correct migration, alignment, and lamination leading to cluster of cells lined up facet by facet with explicit polar orientation. Since neuronal migration happens in the second trimester of gestation, mobile derangement, subsequent to insult by maternal illness, must occur during this stage of growth. This concept is supported by the remark that the variety of cases of schizophrenia in offspring of moms contaminated with influenza virus confirmed vital improve. Other investigators problem the ontogenic principle on the idea of the reality that schizophrenia happens in youngsters and that the signs wax and wane with progressive deterioration and remission. They claim that an infection or damage might result in miswiring and aberrant regeneration, resulting in irregular sprouting and synaptic reorganization of projection sites and increased excitability and abnormal behavioral sample of the affected neurons. This reorganization can also lead to abnormal functioning of the buildings that receive enter from the hippocampal gyrus. In reality, numerous glucocorticoid receptors exist in the hippocampal gyrus, and hormonal role in the development of dendrites of the granule cells seems apparent. During adolescence, the frequency of hippocampal neuronal firing is proportional to the hormonal release. This massive firing predisposes the cells to harm, initiating sprouting and mobile reorganization. Dopamine is considered the primary neurotransmitter concerned in the growth of schizophrenia. The easiest form of dopamine hypothesis relies upon the overactivity of the mesolimbic dopaminergic system. This principle relies upon the truth that, first, most antipsychotics are antagonists to the dopamine type (D2) receptors, and second, medicine that increase dopaminergic neuronal exercise, similar to amphetamine, are psychotomimetic. The theory additionally suggests that dopamine sort (D1) receptor may be responsible for the socalled adverse symptoms of schizophrenia. Another a part of dopamine theory is the significant improve in plasma ranges of the dopamine metabolite, homovanillic acid, in schizophrenics. The issues with dopamine hypothesis are twofold: the truth that antipsychotic medicines are useful in the therapy of virtually all psychotic states suggests that dopaminergic hyperactivity is exclusive to schizophrenia; and some electrophysiological knowledge suggest that the firing fee of dopaminergic neurons may very well improve in response to long-term treatment with antipsychotics (see also dopamine in Chapter 12). Excitatory amino acids can also play a role within the pathophysiology of schizophrenia. Treatment of schizophrenia may be completed by dopamine receptor antagonists (D2 receptors that are coupled to adenylyl cyclase) corresponding to risperidone clozapine, melperone, sertindole, and ziprasidone. Also, dopamine receptor antagonists are associated with unwanted side effects corresponding to akathesia (restlessness), rigidity, tremor, tardive dyskinesia (tongue darting), and neuroleptic malignant syndrome. Clozapine can additionally be an efficient antipsychotic drug, which primarily antagonizes the D4 receptor and, to a lesser diploma, the D2 and serotonin receptors. Since clozapine is related to agranulocytosis in 1%�2% of patients, cautious monitoring of the blood may be required. The induseum griseum and the fasciolar gyrus are considered as posterior extensions of the dentate gyrus. Anteriorly and inferiorly, it continues into the uncus as the band of Giacomini or the tail of the dentate gyrus. The axons of the granular cell neurons project to the hippocampal gyrus through the polymorphic layer, whereas their dendrites remain confined to the overlying molecular layer, a primary web site of projection of the entorhinal cortex. Association fibers confined to the identical facet are the primary component of the polymorphic layer of this gyrus. Glutamate and/or aspartate are utilized by the afferents to the dentate gyrus that emanate from the entorhinal cortex. The subiculum consists of a middle pyramidal neuronal layer that sends dendrites to kind the superficial molecular layer and a deep polymorphic layer. Major projections arise from the pyramidal layer of the subiculum destined to the septal area, anterior thalamus, nucleus accumbens septi, entorhinal area, and the mammillary nuclei of the hypothalamus. The presubiculum lies medial to the subiculum and consists of a middle pyramidal cell layer, a superficial plexiform layer, and a deep layer that continues with the subiculum or entorhinal cortex. This intrinsic loop is interrupted by projections of the pyramidal neurons to the lateral septal nucleus and subicular efferents to the amygdala, ventral striatum, mammillary our bodies, and anterior thalamus.
Viagra soft 100 mg cheap amex
Like the cortical projections erectile dysfunction pump hcpc 100 mg viagra soft generic overnight delivery, these tectal inputs to the gaze facilities discharge very shortly before the saccadic movement begins and is linked to the presentation of the visible image impotence age 40 viagra soft 100 mg buy generic on-line. Thus, through this connection, the ipsilateral abducens nucleus is activated, whereas the contralateral abducens nucleus is inhibited. Cerebellar diseases might produce overshooting and undershooting of saccadic movements. Damage to the frontal eye area leads to lack of capability to produce saccadic actions to the contralateral facet and deviations of the eyes toward the lesion facet (see also cortical dysfunctions, Chapter 8). Vestibulo-ocular eye motion Vestibulo-ocular motion (reflex) is designed to fixate gaze during speedy head movement. Slow movement, motion with eyes closed or head movement in darkness often elicits minimal transient vestibulo-ocular response. The latter kind of motion prompts the optokinetic system, which may comply with the vestibulo-ocular reflex when the top movement begins to dissipate. It is a conjugate ocular motion that involves compensatory eye motion the identical distance as the head but in the wrong way, mediated by the frontal eye fields that preserve connections with the parietotemporal cortex, and also with the primary, secondary, and tertiary visible cortices that initiate and information the graceful pursuit movement. The mechanical stimuli generated in the vestibular receptors are transduced to impulses that travel within the primary vestibular fibers (axons of the bipolar neurons of the Scarpa ganglia) terminating within the cerebellum and the vestibular nuclei. Cerebellar dysfunctions and administration of sedatives and analgesics produce fragmentation of this movement into a sequence of saccades. DisorDers oF oCular moVemeNts these issues embrace nystagmus, conjugate gaze palsy, ocular dysmetria, oculogyric reflex, opsoclonus, ocular flutter, ocular bobbing ocular myoclonus, oscillopsia, and congenital ocular motor apraxia. Nystagmus is an involuntary, rhythmic oscillation of the eye in response to an imbalance within the vestibular impulses (see additionally the vestibular system). Lateral gaze palsy refers to the inability to look to the facet of the lesion ensuing from destruction of the abducens nucleus. Vertical gaze palsy is characterized by the lack to look up-or downward and is associated with lesions of the vertical gaze center within the rostral midbrain. Ocular dysmetria denotes an error in ocular fixation, producing overshooting of the intended target followed by oscillation of the eyeball. The oculogyric reflex is characterised by upward or side-to-side rolling movements of the eyes accompanied by abnormal contractions of the facial muscle tissue. This reflex may be the result of metabolic problems of dopamine and could additionally be alleviated with anticholinergic medicines. Opsoclonus (dancing eyes in infants) is another ocular disorder that displays a random, conjugate saccadic motion of the eyes in all instructions with unequal amplitudes. Ocular flutter, seen in people with cerebellar lesions, is characterised by sudden, speedy, and spontaneous to-and-fro oscillations of the eyes. It is related to blurred vision and could additionally be seen with modifications in fixation whatever the course of the gaze. Ocular bobbing refers to the fast, spontaneous (not rhythmic) downward deviation of each eyes, adopted by sluggish synchronous return of the eyes to the unique place. This phenomenon may be seen in comatose individuals with lesions of the pons, cerebellum, or cerebral cortex. Ocular myoclonus is a time period used to describe the rhythmic, rotatory, or pendular actions of the eyes synchronously with related movements of the palatal, pharyngeal, laryngeal, lingual, and diaphragmatic muscular tissues. Oscillopsia may be vertical or horizontal or exhibit a number of types of ocular movements. It is often seen within the Arnold�Chiari malformation, superior canal dehiscence syndrome, and vestibular dysfunction. Unilateral oscillopsia in the type of shimmering and shaking of vision in one eye might be as a end result of myokymia, a condition associated with spontaneous and involuntary contraction of the muscular tissues due to vascular compression of the ocular muscular tissues, particularly the superior indirect (superior indirect myokymyia), or excessive alcohol or caffeine intake. Congenital ocular motor apraxia (Cogan syndrome) is a disorder of conjugate deviation of the eyes in which voluntary saccades are absent. The head abruptly turns to the aspect to visualize the object whereas the eyes transfer in the other way of the movement. This reflex is mediated by the optic nerve (afferent limb) and the oculomotor nerve (efferent limb). Information, which is carried by the optic nerve, is delivered to the optic tract and bilaterally to the oculomotor nuclei. This reflex is misplaced in Argyll Robertson pupil, a pupillary dysfunction that happens in neurosyphilis, diabetes mellitus, and epidemic encephalitis and alcoholism. It is mediated by the bilateral connection of the optic tract to the oculomotor neurons via the central commissural connections. The latter exhibits loss of pupillary constriction in gentle reflex, while sustaining it in accommodation. It requires the utilization of the visual cortex as well as the optic nerve, optic tract, and oculomotor nuclei. The ciliospinal reflex reveals pupillary dilatation in response to painful stimulation of a dermatomal area. This reflex is dependent upon the integrity of the cervical postsynaptic sympathetic fibers as properly as the presynaptic neurons of the primary and second thoracic spinal segments. The oculocardiac reflex is characterized by bradycardia (slowing of heart rate) in response to a stress applied on the eyeball. Loss of the oculocephalic reflex is an ominous discovering, which signifies metabolic melancholy or a lesion in the brainstem that disrupts the connection between the third and eighth cranial nerves. Suppression of the ascending reticular activating system and lack of consciousness happen when the lesion is positioned rostral to the pontine and midbrain gaze centers. Impaired oculocephalic response may also occur on account of malpositioning or insufficient head rotation. It is characterized by contraction of the posterior auricular muscle tissue and the next movement of the ear posteriorly, contralateral to the stimulated side. The blink reflex of Descartes is produced by an object that abruptly and unexpectedly approaches the eye. This reflex is mediated by the optic and facial nerves and is characterised by contraction of the orbicularis oculi in response to this stimulus. The supranuclear mechanism for upward gaze is situated nearer to the third ventricle than the middle for downward gaze. This area features a pulse generator for quick eye actions and an integrator that determines the ultimate word resting place of the attention. It tasks to the ipsilateral abducens nucleus, which controls the contralateral medial rectus muscle, and the ipsilateral lateral rectus muscle. The corticotectal tract, which is derived from the frontal eye area (Brodmann area 8), carries data that tasks to the contralateral gaze middle and regulates contralateral voluntary conjugate eye actions. Corticotectal fibers that are derived from the occipital lobe (Brodmann areas 17, 18, and 19) control involuntary smooth pursuit eye motion.
Discount viagra soft 100 mg mastercard
Head stability requires a reduction within the firing fee from one horizontal duct coupled with increased firing price from the contralateral facet impotence synonym purchase 100 mg viagra soft free shipping. When this steadiness is disturbed with a peripheral vestibular lesion erectile dysfunction at the age of 30 discount 50 mg viagra soft visa, the firing fee on the affected facet is decreased, which is interpreted as head turning. Nystagmus, an abnormal rhythmic oscillation of the eyeball, is produced visually by watching stationary targets from a moving vehicle (optokinetic nystagmus) or by extreme gaze to one aspect. It can also be produced iatrogenically by instilling chilly or warm water into the ear (caloric test) or rotating within the Barany chair. Clinically, it could result from peripheral or central vestibular lesions (see additionally the vestibular system, Chapter 15). In a unilateral peripheral vestibular lesion, the firing fee of the horizontal semicircular canal is reduced, inflicting sluggish eye movement (slow phase of nystagmus) toward the affected side followed by corrective fast eye motion (rapid section of nystagmus) section to the contralateral side. This nystagmus, which is gaze dependent, becomes more pronounced when the patient looks towards the affected aspect. The site of entry of the cochlear nerve into the pons and its course within the internal acoustic meatus are identical to that of the vestibular nerve. The dendrites of the bipolar neurons of the spiral ganglia obtain auditory impulses from the organ of Corti (site of auditory neuroepithelial cells) within the cochlea and convey these impulses to the dorsal and ventral cochlear nuclei within the caudolateral a half of the pons. Postsynaptic fibers synapse within the ipsilateral and contralateral superior olivary nuclei, whereas others proceed to the opposite side, ascending within the lateral lemniscus. Postsynaptic neurons of the superior olivary nuclei project within the ipsilateral lateral lemniscus to the inferior colliculus. Fibers from the inferior colliculus journey rostrally to the medial geniculate nucleus after which by way of the auditory radiation to the transverse gyri of Heschl. Damage to the cochlear nerve, because of acoustic neuroma, or fracture involving the petrous temporal bone, produces sensorineuronal deafness on the facet of the lesion. This sort of deafness could also be accompanied by tinnitus and is distinguished from conduction deafness by Rinne and Weber checks (see the auditory system, Chapter 14). Tinnitus refers to a unilateral or bilateral condition that ranges from a soft hissing sound or ringing noise to devastating loud constant roaring. It could additionally be continuous or intermittent and is an important manifestation of injury to the cochlear nerve. Fractures of the posterior cranial fossa involving the interior acoustic meatus and tumors of the cerebellopontine angle (acoustic neuroma) may result in combined vestibular, cochlear, and facial nerve dysfunctions. This kind of injury is characterized by deafness on the facet of the lesion, vertigo (sense of rotation of the surroundings or self), nystagmus, ataxia, and indicators of ipsilateral infranuclear facial palsy. It has two ganglia, a superior somatic sensory and an inferior visceral sensory ganglia. This nerve offers off tympanic, carotid sinus, lingual, pharyngeal, tonsillar, muscular, and auricular branches. This nerve conveys sensations from the mucosa of the center ear, auditory tube, and mastoid air cells to the spinal trigeminal nucleus. Visceral afferent fibers within the carotid sinus department establish synaptic connections via interneurons in the reticular formation of the medulla with the dorsal motor nucleus of the vagus and, simultaneously, with the neurons of the reticulospinal tracts. In flip, the dorsal motor nucleus of the vagus sends preganglionic parasympathetic fibers to the cardiac plexus, reducing cardiac contractility (negative chronotropic effect) whereas the medullary reticulospinal tract inhibits or reduces the firing price of the preganglionic sympathetic neurons that offer the cardiac plexus and the cutaneous arterioles. The lower within the sympathetic output combined with the vagal inhibition ends in a lower of cardiac fee and output. The decrease in the peripheral vascular resistance leads to a decrease in blood pressure. This plexus supplies the oropharyngeal mucosa and mediate the pharyngeal (gag) reflex by way of its connections to the spinal trigeminal, dorsal motor and ambiguus nuclei. The gag reflex, characterized by elevation of the stimulated part of the taste bud, is elicited by mild stimulation of the oropharynx and taste bud. Unilateral lack of gag reflex may point out damage to the glossopharyngeal nerve or the vagus nerve and may be noticed in lateral medullary syndrome. It additionally supplies fibers to the cranial a part of the accent nerve and to the vagus nerve, innervating the laryngeal, pharyngeal, and palatine muscular tissues. The glossopharyngeal nerve may be damaged in fractures of the posterior cranial fossa and stenosis of the jugular foramen. Demyelination attributable to multiple sclerosis, tumors of the posterior cranial fossa, aneurysm of the interior carotid artery, and injuries involving the retroparotid house may also injury this nerve. Isolated glossopharyngeal nerve injury causes hypertension due to involvement of the carotid department of the nerve, lack of sensation over the soft palate, fauces, oropharynx, and posterior third of the tongue on the aspect of the lesion in addition to ipsilateral lack of parotid secretion and lowered or lack of gag and pharyngeal reflexes. Although isolated damage to the glossopharyngeal nerve is uncommon, the following are some of the situations associated with irritation, compression, or harm to this nerve. Disorders of this situation are analogous to the mixed deficits related to these particular person nerves. Glossopharyngeal neuralgia is a rare situation, which is characterized by spontaneous episodic assaults of excruciating pain within the tonsillar area, posterior third of the tongue, and exterior acoustic meatus, radiating to the throat, facet of the neck, and again of the lower jaw. It is provoked by yawning, laughing, chewing, or swallowing of particularly chilly liquid and may be associated with peritonsillar abscess, oropharyngeal carcinoma, and ossified stylohyoid ligament. When ear pain is felt without signs of middle ear disease, oropharyngeal most cancers should even be thought of. Glossopharyngeal neuralgia could also be related to episodes of fainting, syncope, and reflex bradycardia on account of involvement of the carotid sinus nerve Table 11. It travels ventrolaterally in the caudal medulla and passes through the spinal trigeminal tract and nucleus in shut proximity to the nucleus ambiguus and spinal lemniscus. This nerve leaves the medulla through the postolivary sulcus, as a collection of rootlets, and exits the skull via the jugular foramen, accompanied by the glossopharyngeal and accessory nerves. During its course within the superior and posterior mediastina, it provides rise to branches to the cardiac and pulmonary plexuses. Later, the vagus nerves on both sides contribute to the formation of the anterior and posterior vagal trunks across the belly a half of the esophagus, getting into the abdomen through the esophageal hiatus of the diaphragm. In the abdomen, it contributes presynaptic parasympathetic fibers to the celiac, superior mesenteric, and aortic plexuses. The vagal (parasympathetic) contribution to the stomach viscera terminates at the junction of the proper two-thirds and left one-third of the transverse colon. The vagus nerve has a superior and inferior ganglion, containing neurons for somatic and visceral sensations, respectively. Within this nerve, the motor fibers belong to the cranial a part of the accent nerve, which distribute to the laryngeal, pharyngeal, and palatal muscle tissue. Through its course, the vagus nerve offers rise to branches within the cranial cavity, thorax, and stomach, which embody the meningeal, auricular, pharyngeal, carotid physique, superior and inferior laryngeal, cardiac, pulmonary, esophageal, celiac, and superior mesenteric branches. Through this plexus, the vagus nerve innervates most of pharyngeal muscle tissue (with the exception of the stylopharyngeus) and palatine muscular tissues (with the exception of the tensor palatini). These fibers join the pharyngeal branches of the glossopharyngeal nerve and the cervical a part of the sympathetic trunk, to kind the pharyngeal plexus. Taste sensation from the intense posterior a part of the tongue and the epiglottic vallecula is also conveyed by this nerve to the solitary nucleus. During its course within the tracheoesophageal sulcus and medial to the thyroid gland, it runs in close proximity to the inferior thyroid artery, a relationship that bears important medical significance in thyroidectomies.