
Solian dosages: 100 mg, 50 mg
Solian packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
Purchase solian 50 mg with amex
Meyer S et al: A 13-year-old girl with arterial hypertension - mid-aortic syndrome symptoms 9dpo bfp generic 100 mg solian with amex. Mohammadi A et al: Bilateral tardus-parvus waveforms in a patient with aortic coarctation medications used for depression order solian 100 mg with mastercard. A massive graft (green) has been positioned between the ascending & descending aorta to enhance flow. No collaterals were seen, & no vital gradient was detected on this affected person with pseudocoarctation of the aorta. Ren X et al: the significance of aortic valve calcification in patients with bicuspid aortic valve disease. Bernal Garnes N et al: Magnetic resonance imaging within the evaluation of anomalous pulmonary venous connections. Dirks V et al: Modified Blalock Taussig shunt: a not-so-simple palliative process. Murtuza B et al: the effect of morphologic subtype on outcomes following the Sano-Norwood process. Kutty S et al: Role of imaging in the analysis of single ventricle with the Fontan palliation. Kiraly L et al: Three-dimensional printed prototypes refine the anatomy of post-modified Norwood-1 advanced aortic arch obstruction and permit presurgical simulation of the restore. This is the classic look of a Lecompte maneuver as a half of the Jatene arterial change process. Dodge-Khatami A et al: Past, present, and way ahead for the arterial change operation: historical evaluate. Note the 2 central metallic dots (indicating the ends of the device waist) & the flat discs on either facet of the waist. Note the probe from the transesophageal echocardiogram & the catheter in the inferior vena cava from the recent launch of the system. Jalal Z et al: Long-term issues after transcatheter atrial septal defect closure: a evaluation of the medical literature. The publish analysis native T1 value was 1047 ms, which is > the 990 ms threshold outlined for sensitivity in detecting edema in myocarditis patients. Both views are utilized to acquire a correlative septal measurement (along the purple line). The delayed enhancement is extreme (though patchy) on the 1st image (left), becoming extra intensive & practically full thickness on the follow-up examination (right). Currently, this method is especially used to examine subtle changes in response to therapeutics. Tandon A et al: Myocardial fibrosis burden predicts left ventricular ejection fraction and is related to age and steroid treatment period in duchenne muscular dystrophy. It is slightly hyperintense to myocardium, a attribute finding of rhabdomyomas. Rhabdomyomas could grow throughout being pregnant however often spontaneously regress postnatally. Demographics � Age 75% identified earlier than 1 year of age � Epidemiology Cardiac tumors rare (1:30,000-1:one hundred,000) Rhabdomyoma most common pediatric cardiac tumor 318 radiologyebook. A chest radiograph obtained 6 days earlier (not shown) demonstrated a traditional cardiac silhouette. The septum additionally demonstrated a no-reflow phenomenon as a result of continued microvascular occlusion. A fusiform aneurysm of the left anterior descending coronary artery can be visualized. The left atrium splays the carina & creates a double shadow over the right coronary heart border. This is commonly seen in patients with Marfan syndrome & causes gentle tissue prominence along the proper facet of the mediastinum on the chest radiograph. Franken R et al: Increased aortic tortuosity indicates a more severe aortic phenotype in adults with Marfan syndrome. Note the postoperative changes of a prior sternotomy for restore of the aortic root. In addition, radiologists should do not neglect that kids are more sensitive to the results of ionizing radiation than adults. This ought to be thought of when deciding on essentially the most applicable imaging research to diagnose a suspected situation. Many imaging modalities can be found for diagnosing stomach pathology in kids. Depending on the patient age, presentation, & specific medical question, each modality has distinctive advantages & disadvantages. Radiography Constipation, pain, vomiting/bowel obstruction, & necrotizing enterocolitis are frequent indications for obtaining pediatric abdominal radiographs. Modifications for children embrace a single view for suspected constipation & the decubitus view or cross-table lateral view to search for free air in infants. Fluoroscopy Methods to reduce radiation publicity to the affected person include minimizing fluoroscopy time, pulsed fluoroscopy, fluoroscopic image hold or clips somewhat than digital spot exposures, small picture intensifier-to-patient distance, appropriate collimation, & low-dose fluoroscopy settings for pediatric patients primarily based on size. Contrast Enema Common indications for a contrast enema embrace the failure of a new child to move meconium, new child bilious emesis (if the radiograph suggests a distal obstruction), & chronic constipation. The typical single distinction enema approach includes the next pictures: An early left-side-down lateral view of the rectum through the splenic flexure (especially to evaluate the rectosigmoid ratio) whereas contrast is flowing, a frontal view of the rectum via the splenic flexure during active filling, an overhead frontal view of the abdomen when crammed just barely to the cecum, & an overhead frontal view of the stomach after spontaneous contrast evacuation. In newborns with a suspected distal bowel obstruction, reflux of distinction into the terminal ileum is helpful. If in search of a stricture after necrotizing enterocolitis, cautious consideration to refined caliber change is required in real time throughout distinction move, significantly if the colon overlaps at any point. Enema Reduction of Intussusception Various methods can be utilized to scale back an ileocolic intussusception; however, air reduction is utilized in many hospitals. Note that an enema discount is contraindicated with peritoneal indicators or pneumoperitoneum. Sonographic modifications for youngsters include the number of an appropriate transducer & distraction of the patient throughout scanning. Modifications for children include the use of weight/sizebased protocols & automatic tube present modulation strategies. Specific indications will assist drive the selection of the suitable contrast agent & protocol. Diffusion-weighted imaging can be particularly helpful in rising the conspicuity of inflammatory & neoplastic pathologies against collapsed normal bowel loops. Modifications for children embrace the usage of video goggles for distraction, pretest practice/simulation to put together younger sufferers for the noise & comparatively small bore dimension, & the usage of sedation or common anesthesia for many sufferers underneath 6 years of age. The most typical stomach malignancies affecting children are Wilms tumor, neuroblastoma, & hepatoblastoma. It often encases & displaces vessels, crosses the midline, & contains Ca� (~ 90%). It is typically a big heterogeneous strong liver mass, often presenting outdoors the newborn interval.
Purchase 50 mg solian with visa
Transjugular intrahepatic portosystemic shunt in hepatorenal syndrome: Effects on renal function and vasoactive methods treatment ulcerative colitis discount solian 50 mg with mastercard. Extracorporeal liver help with molecular adsorbents recirculating system in patients with severe acute alcoholic hepatitis medications dictionary solian 50 mg purchase on line. Effects of fractionated plasma separation and adsorption on survival in patients with acute-on-chronic liver failure. Continuous arterio-venous ultrafiltration within the administration of the renal complications of liver illness. Long-term survival and renal function following liver transplantation in patients with and without hepatorenal syndrome-experience in 300 sufferers. Pretransplant renal perform predicts survival in patients present process orthotopic liver transplantation. Hepatorenal syndrome: Combined liver kidney transplants versus isolated liver transplant. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: A double-blind, placebocontrolled trial. Terlipressin plus albumin infusion: An efficient and protected remedy of hepatorenal syndrome. Long-term terlipressin administration improves renal operate in cirrhotic patients with kind 1 hepatorenal syndrome: A pilot examine. Effect of terlipressin (Glypressin) on hepatorenal syndrome in cirrhotic sufferers: Results of a multicentre pilot study. Terlipressin remedy with and without albumin for sufferers with hepatorenal syndrome: Results of a prospective, nonrandomized study. Renal failure in cirrhotic sufferers: Role of terlipressin in clinical method to hepatorenal syndrome kind 2. Terlipressin in patients with cirrhosis and sort 1 hepatorenal syndrome: A retrospective multicenter study. Beneficial results of terlipressin in hepatorenal syndrome: A prospective, randomized placebo-controlled medical trial. A randomized, prospective, doubleblind, placebo-controlled trial of terlipressin for kind 1 hepatorenal syndrome. Terlipressin and albumin vs albumin in sufferers with cirrhosis and hepatorenal syndrome: A randomized study. Treatment of hepatorenal syndrome as defined by the International Ascites Club by albumin and furosemide infusion in accordance with the central venous strain: A prospective pilot study. Vasopressin, not octreotide, could additionally be useful in the treatment of hepatorenal syndrome: A retrospective research. Noradrenalin vs terlipressin in patients with hepatorenal syndrome: A potential, randomized, unblinded, pilot study. Russ Renal impairment can alter drug pharmacokinetics and pharmacodynamics, and consequently sufferers with renal impairment are at threat of adverse results. In addition, these sufferers take a number of drugs and are at high risk of drug interactions and drug-related issues. This chapter describes pharmacokinetic principles and highlights frequent prescribing points in patients with renal impairment, dialysis, and transplantation. Increased absorption in sufferers with renal impairment from decreased first-pass metabolism is seen with some -blockers, dextropropoxyphene, and dihydrocodeine. Comorbidities in renal sufferers also have an impact; for example, absorption may be erratic because of diabetic gastrointestinal neuropathy. If protein binding is decreased, a greater free fraction is on the market for any given complete drug concentration, which may improve drug exercise. Organic acids normally have a single binding site on albumin, whereas natural bases have a number of binding sites on glycoproteins. Protein binding may be altered in patients with renal impairment, especially when serum albumin is low. Predicting the impact of modifications in protein binding is tough as a result of even though extra free drug is out there at the web site of action, more is available for metabolism or renal excretion. Hence, decrease plasma concentrations can occur and drug half-life might lower rather than improve. Phenytoin, for example, has marked decreases in protein binding in sufferers with renal impairment, and toxicity can happen despite regular or low total plasma concentrations due to an increase in free fraction. With albuminuria, certain drug may also be misplaced, which may partially explain the refractoriness of nephrotic patients to diuretics. Volume of Distribution Bioavailability (F) is the portion of a drug dose that appears in the systemic circulation after administration by a nonintravenous route. Whereas medicine given intravenously have 100 percent bioavailability, medicine given by alternative routes pass via a collection of biologic membranes earlier than entering the systemic circulation so that only a fraction may reach the circulation. The gastrointestinal mucosa additionally acts as a barrier to absorption by metabolizing medication or retarding absorption. Nausea and vomiting from uremia can impair absorption and contact time between the drug and gastrointestinal mucosa. In patients with superior uremia, the alkalinizing effect of salivary urea may decrease absorption of medicine optimally absorbed in an acid milieu. Metabolism Drug metabolism is primarily a hepatic function by which medication are converted to more water-soluble entities to promote elimination by the kidneys and bile. Despite the belief that nonrenal clearance is unchanged, renal impairment can alter and slow drug metabolism. Physicians should use clinical judgment to evaluate every state of affairs individually, select a dosage regimen primarily based on components in that patient, and regularly reevaluate response to remedy. Initial Assessment and Laboratory Data A targeted historical past is necessary in assessing dose in patients with renal impairment. Previous drug efficacy or toxicity should be decided and the current drug listing reviewed for potential interactions or nephrotoxins. Physical and laboratory parameters indicate quantity standing, top, weight, and extrarenal illness. Estimating Renal Function for Drug Dosage Table 77-3 Protein binding of drugs in renal disease. Quantitation of drug elimination by the kidney is expressed as renal clearance, which is determined by renal blood circulate and the ability of the kidney to take away the drug. Glomerular filtration is decided by molecular dimension (<10 kd), cost, and protein binding (increased when binding decreases). Secretion of medication eradicated by tubular transport may change with renal disease, however measurement of tubular operate is tough. The higher the degree of renal impairment, the larger the potential for dose modification. The Cockcroft-Gault equation has been the most broadly used and accepted technique for drug dosage calculation. An essential limitation of many renal operate estimates is inaccuracy of singlepoint estimates when renal function is rapidly altering. This may result in overestimation or underestimation of renal operate and underdose or overdose. Activity and Toxicity of Metabolites It is important to think about the activity (or toxicity) of drug metabolites in addition to that of the mother or father drug itself.
Diseases
- Sialidosis
- Secernentea Infections
- Body dysmorphic disorder
- Marles Greenberg Persaud syndrome
- Pyomyositis
- Inborn metabolic disorder
- Hypotelorism cleft palate hypospadias
- Schweitzer Kemink Malcolm syndrome
- Trigonomacrocephaly tibial defect polydactyly
- Wolfram syndrome
Order 100 mg solian otc
Rarely and nearly completely on the right aspect treatment internal hemorrhoids generic solian 100 mg with visa, the recurrent laryngeal nerve arises from the vagus nerve on the degree of the bifurcation and runs directly to medications for gout solian 50 mg generic otc the larynx (nonrecurrent recurrent laryngeal nerve). Extremely light dissection of the bifurcation is necessary to stop dislodgement and downstream embolization of material from underlying artherosclerotic plaque. When completed, this dissection ought to allow light lifting of the vessels toward the floor of the wound and greatly ease shunt insertion when needed. The arteriotomy must be closed with a patch, ideally vein or bovine pericardium. After completion of the endarterectomy and achieving hemostasis, closure is simple. If essential, drains must be positioned throughout the carotid sheath and introduced out via a separate web site posterior and inferior to the incision. Sloping minimize through intima Endarterectomy carried out Vein or prosthetic patch used to widen vessel if necessary. Comparison of saphenous vein patch, polytetrafluoroethylene patch and direct arteriotomy closure after carotid endarterectomy: postoperative outcome. Disease of the aortoiliac arteries can manifest as aneurysmal or occlusive illness. Aneurysmal disease is principally of the juxtarenal or infrarenal aorta and may or might not contain the widespread iliac arteries. The exterior iliac arteries are usually spared, so an in depth midline abdominal incision provides all the publicity necessary. This procedure requires a smaller stomach incision, often ending slightly below the umbilicus, and two groin incisions, transverse or longitudinal, relying on surgeon choice. Although angiography was once the mainstay of preoperative planning, it has a more restricted function today. A midline abdominal incision is produced from the xiphoid course of to below the umbilicus for an applicable distance. If groin incisions might be used, the groin is opened first within the affected person with no previous stomach incision, with minimal difficulty predicted in exposing the abdominal aorta. In patients with previous stomach surgery, the author usually begins with the abdominal incision because of the next probability of enterotomy throughout lysis of adhesions, and the groin would stay unscarred. In patients with extensive prior surgery, especially involving an infection with peritonitis, a retroperitoneal or low thoracoabdominal strategy may be warranted. A simple anastomosis to the common femoral artery or the anastomosis, together with the primary centimeter of superficial femoral artery or profunda femoris (deep femoral) artery, may be uncovered with a transverse incision. Complexity within the groin necessitating more intensive or expansile exposure of the superficial femoral artery, or more often the profunda femoris artery, requires a longitudinal incision, the length of which could be modified to suit the scenario. The small bowel is moved to the best and superiorly in the stomach, and the sigmoid colon is gently retracted to the left. This method allows the surgeon to dissect the best frequent iliac bifurcation, retracting the peritoneum and its hooked up fats to the proper. Remember that the ureter crosses the iliac vessels anteriorly and on the level of the frequent iliac bifurcation bilaterally. Depending on the level of bypass, vessel loops could be placed around the best external and inside iliac arteries or across the distal frequent iliac artery, respecting the intimate relationship between the iliac arteries and veins. The commonest atherosclerotic sample demonstrates illness on the distal frequent iliac artery, so vessel loops across the external and internal iliac arteries are preferred. The vessels are normally gentle at this location and will provide probably the most flexibility in developing the anastomosis. The left widespread iliac bifurcation reveals the identical anatomic pattern of ureter anteriorly and a close relationship between the arteries and the delicate veins. Accessing the left common iliac bifurcation is harder due to the colonic mesentery. The writer normally pulls on this mesentery to visualize the specified airplane to go underneath. A layer of tissue that often accommodates sympathetic nerves is left over the left frequent iliac artery, and the left iliac bifurcation is palpated. The ureter is then found, and the whole mass of tissue containing the ureter and sigmoid colon mesentery is gently retracted to dissect the bifurcation and carefully place vessel loops. This approach is helpful in sufferers with a big, left common iliac artery aneurysm, or if the retractors used to entry the left iliac bifurcation from the medial facet place too much tension on the ureter or sigmoid colon mesentery. The widespread iliac artery may be ligated and an end-to-side anastomosis to the external iliac artery constructed, permitting backward circulate to the left inside iliac artery and ahead flow to the left leg. The anastomosis may be done within the extra hospitable lateral exposure to the external iliac artery instead of the deeper space of the left iliac bifurcation. This option ought to be thought-about to hold the complete operation to a single midline stomach incision, thus avoiding a groin dissection. Arteries of ureters and urinary bladder Abdominal aorta Superior mesenteric artery Renal artery and vein Ureteric branch from renal artery Ovarian artery Ureter Inferior mesenteric artery (cut) Ureteric department from aorta Ureteric branches from ovarian and common iliac arteries Common iliac artery Median sacral artery Internal iliac artery Iliolumbar artery Superior gluteal artery Lateral sacral artery Inferior gluteal and inner pudendal arteries Umbilical artery (patent part) Obturator artery Uterine artery Inferior vesical artery and ureteric department Superior vesical arteries Inferior epigastric artery Ureteric branch from superior vesical artery Medial umbilical ligament Sigmoid colon (reflected) Sigmoid mesocolon Intersigmoid recess Ureter B. An incision is made alongside the best lateral border of the nonaneurysmal aorta and on the best facet of an aneurysmal aorta. This approach is used to keep away from injuring the inferior mesenteric artery or any collateral circulate to the sigmoid colon. The duodenum comes into view, and the peritoneum is incised about 2 cm across the inferior fringe of the duodenum, to entry the plane beneath the duodenum and on the anterior floor of the aorta. The 2 cm of peritoneal cuff provides sufficient tissue to shut at the end of the aortic restore. The aircraft on the anterior surface of the aorta is then developed, and the duodenum is retracted cephalad and slightly to the right. The inferior mesenteric vein often may be ligated to facilitate this plan and exposure. Be positive to palpate the bundle in which the inferior mesenteric vein travels; if an accompanying arch of Riolan is contributing to total rectosigmoid blood provide, this bundle should be retracted. The left renal vein is seen to the proper, the vena cava superiorly, and the suction system pointing to the proper renal artery. The left renal vein can be dissected free and retracted cephalad to achieve greater exposure of the aorta and renal arteries. These vessels originate from the posterior half of the aorta between lumbar vertebrae. [newline]Therefore, instrument or finger dissection posterior to the aorta has a transparent space in the concavity of the lumbar vertebrae, between precise discs. To accomplish this, the surgeon decides whether or not the renal vein should be retracted or divided and subsequently repaired. If the left renal vein must be cut, its adrenal, gonadal, and lumbar branches ought to remain intact. The left renal vein is then secured with large bulldog clamps 2 cm aside and reduce between, leaving a cuff of 1 cm on both side to repair when the process is completed. The retroaortic left renal vein is usually not perpendicular to the aorta, as is the conventional left renal vein. Abdominal wall Lesser omentum Hepatic portal vein and correct hepatic artery in proper margin of lesser omentum Omental bursa (lesser sac) Stomach Middle colic artery Transverse mesocolon T12 Omental (epiploic) foramen (of Winslow) Celiac trunk Splenic vessels Renal vessels L1 L2 L3 Pancreas Superior mesenteric artery Lumbar vessels Inferior (horizontal, or 3rd) part of duodenum Abdominal aorta Transverse colon Greater omentum Small gut L4 L5 S1 S2 Parietal peritoneum (of posterior stomach wall) Mesentery of small gut B. The groin incisions are made transversely or horizontally relying on the complexity of the femoral reconstruction.
100 mg solian cheap with amex
The three ossification centers type a triangle symptoms ringworm buy 50 mg solian otc, with the lateral lots forming a V-shaped "tent" over the spinal canal treatment centers of america solian 100 mg purchase otc. The complete length of the spine must be scanned within the transverse plane ensuring the spinal twine is completely enclosed by this triangle. Splaying or divergence of the posterior elements is an important discovering in the analysis of neural tube defects. When imaging within the sagittal aircraft, the spine is seen as two parallel curvilinear echogenic traces (vertebral body and posterior elements). Variations of those normal curves warrant further evaluation for an underlying abnormality. Coronal imaging is helpful for evaluation of vertebral physique anomalies and scoliosis. The normal ultrasound appearance of the posterior components in the coronal plane is paired echogenic traces, which are flared within the cervical spine on the craniocervical junction and widen slightly within the lumbar backbone. When alignment is irregular, cautious investigation for hemivertebrae, block vertebrae, and butterfly vertebrae, in addition to spinal dysraphism, ought to be performed. The relative dimension of the vertebral bodies must also be assessed to search for circumstances such as platyspondyly. Counting the variety of vertebral bodies, particularly in the lumbar area, is crucial to make positive the distal spine is correctly fashioned. Additionally, imaging in the axial plane is essential to be positive that all of the vertebral our bodies are properly fashioned, including the presence of the posterior parts. Amniotic fluid must be visualized between the backbone and the uterine wall to make positive the overlying skin is unbroken. Although an open spinal defect is extra common in the lumbar spine, it could have an effect on both the cervical and thoracic backbone. Cystic posterior plenty may point out a meningocele (meninges and cerebrospinal fluid only), myelomeningocele (also contains neural elements), or terminal myelocystocele (dilation of the spinal twine central canal, which herniates through a spinal defect). Solid lots embody a twine lipoma or a sacrococcygeal teratoma, which might invaded into the spinal canal. Nearly 100% of Chiari 2 malformations of the mind are in association with spina bifida. By 18 weeks, the conus should be superior to L3-L4, with progressive ascent to above L2-L3 by time period. Approach to Abnormal Fetal Spine Complete analysis of the spine is an important a part of every second and third-trimester fetal scan. Fetal movement, positioning, and shadowing of the vertebral bodies can make imaging difficult. Establishing a search sample and checklist for analysis of the spine will ensure correct diagnosis. Real-time evaluation of the complete length of the backbone in both the longitudinal and axial planes will full the evaluation. Ideally, alignment ought to be evaluated in both the coronal and sagittal planes, but this is usually not potential. Additional imaging of the spine is indicated to determine if this curvature is fastened in position. Vertebral bodies and posterior components are seen within the cervical/thoracic spine, but the alignment is "twisted" with lateral masses seen in the lumbar backbone. This fetus has myeloschisis, confirming the significance of imaging the backbone in 2 planes. Meningoceles contain solely cerebrospinal fluid, whereas myelomeningoceles also contain neural elements. The neural tube defect is uncovered (no sac) in myeloschisis and contains the spinal cord or nerve roots. Classic Chiari 2 hindbrain compression findings are virtually at all times present with open spina bifida. Khalil A et al: Prenatal prediction of want for ventriculoperitoneal shunt in open spina bifida. The cerebellum (calipers and) wraps around the midbrain, taking on the everyday banana shape described with Chiari 2 malformation. The spinal twine itself is a part of the neural components in myeloschisis (open spina bifida and not using a sac). The presence of Chiari 2 malformation (not shown) led to the correct prognosis of meningocele. The lack of Chiari 2 findings is concordant with the ultrasound analysis of a big, skin-covered spina bifida. They are sometimes not related to Chiari 2 malformation, and, subsequently, small ones are often missed at the time of the anatomy scan. Note the big dimension of the pinnacle relative to the physique (a results of absent cervical and upper thoracic vertebrae). The sacrum is lacking, causing the iliac wings to contact medially, thus creating the basic protect appearance. There is abrupt termination of the lumbar backbone and the femurs are held in an abducted position. It is necessary to notice, nevertheless, that solely 12-16% of instances happen within the setting of maternal diabetes, so the distal backbone have to be rigorously checked in all fetuses. Only three lumbar vertebral ossification facilities have been visualized on this fetus of a diabetic mom. Wei Q et al: Value of 3-dimensional sonography for prenatal prognosis of vertebral formation failure. The inset reveals the tuft of hair and sacral dimple, 2 skin stigmata related to tethered wire. Postnatal imaging confirms the tethered twine at the L5 degree and the small bony defect associated with the meningocele sac. On the identical 3D sweep, the coronal image reveals a lowlying conus medullaris in the lower lumbar backbone. A small subcutaneous lipoma and an intraspinal lipoma had been related by a fistulous tract (not shown). On the right, a coronal picture shows splaying of the posterior element of the lumbar spine in a fetus with a myelomeningocele. The proper hemicord additionally has syringohydromyelia, which can be seen in 1 or both cords in 50% of cases. Type 1 is predominately exterior with minimal presacral element; kind 2 extends into the presacral space; kind three extends up into the abdomen; and sort four is totally internal. This remained stable all through gestation and the prenatal course was uncomplicated.
Trusted 100 mg solian
Note irregular sulcation and the irregular cortical white matter interface within the affected regions treatment uti infection 50 mg solian order free shipping. The fetus was known to have advanced congenital heat disease however the mind findings had not been appreciated at the referring facility medicine 75 yellow purchase 100 mg solian with mastercard. The quantity of the frontal white matter is diminished, and the frontal horns are massive. The cerebellum in this case is normal in measurement; cerebellar hypoplasia is usually associated with diffuse cortical malformation. The center fossa is expanded, the overlying bone is thin, and the temporal lobe is displaced posteriorly. The temporal lobe is displaced posteriorly, and the middle cranial fossa is expanded. De Keersmaecker B et al: Outcome of 12 antenatally recognized fetal arachnoid cysts: Case collection and review of the literature. Natural History & Prognosis � Evolving hydrocephalus in < 2% � Hydrocephalus extra probably if Early gestational age at prognosis Progressive improve in dimension 152 radiologyebook. Note the related ventriculomegaly with bilateral dilated occipital horns (cerebellum). In addition, the ependymal lining of the ventricles is thickened and echogenic, and the 3rd ventricle is mildly dilated. Hemosiderin staining alongside the ventricle wall is additional evidence of evolving hemorrhage. Demographics � Epidemiology Uncommonly diagnosed in utero Usually diagnosed between 26- to 33-weeks gestation if identified 156 6. Also notice the thickened echogenic ependyma, a standard discovering with prior hemorrhage. High T1 signal and lack of enhancement further substantiated a fancy hematoma somewhat than neoplasm. The thin cerebral tissue and ventriculomegaly are proof of associated ischemic encephalomalacia. Note the scalp edema; the fetus was also hydropic as a outcome of highoutput cardiac failure. Because the extent of the bran injury was identified, the affected person elected no intervention for the infant. The function of presurgical neuroimaging in a young case of a giant porencephalic cyst with intractable epilepsy. The left ventricular wall has been fully destroyed, leaving 1 large, irregular, porencephalic cyst. The thalami are preserved and there are fragments of medial cerebral hemisphere tissues. The lack of a standard cortical rind is the hallmark statement in hydranencephaly. The falx divides a fluid-filled calvarium with no cerebral tissue however preserved thalami. With the proper analysis of hydranencephaly (with dismal prognosis) labor was induced at 32 weeks to keep away from operative supply. The mass impact of the supratentorial ventricular dilatation is compressing the cerebellum. The posterior fossa is normal, together with a well-seen normal 4th ventricle and vermis. Corral E et al: Prenatal three-dimensional ultrasound detection of adducted thumbs in X-linked hydrocephaly: two case stories with molecular genetic research. Even at this early gestational age, the head was measuring 10 days ahead of the other measurements. This condition is related to extreme intellectual impairment and carries a 50% recurrence danger in male fetuses. Other findings include callosal dysgenesis, tectal beaking, an enlarged massa intermedia, and a medullary spur on the cervicomedullary junction. Progressive ventriculomegaly is common with Chiari 2, most likely because of progressive compressive pressure on the 4th ventricle. It is crucial to discover the dearth of fluid in the cisterna magna as a clue to Chiari 2 and never await the banana sign to make the right analysis. The future cisterna magnum is a 2nd lucency behind the echogenic linear choroid plexus throughout the 4th ventricle. Chapman T et al: Diagnostic imaging of posterior fossa anomalies within the fetus and neonate: half 2, posterior fossa disorders. The temporal horns of the lateral ventricles are dilated in addition to the 3rd ventricle. Similar views could be obtained prenatally using an endovaginal probe if the fetus is in a cephalic presentation. A cerebellar hemisphere has rotated into the place of the inferior vermis, similar to the prior path specimen. This resolved in follow-up, according to interval fenestration of the foramen of Magendie. Plane A will show the vermis but airplane B will present an apparent vermian defect as it goes by way of the cyst. One prenatal sequence confirmed an obvious association between congenital heart disease and Blake pouch cyst. The cavum septi pellucidi is visible, confirming the proper scan plane for measurement of the cisterna magna depth. These characterize remnants of the walls of Blake pouch, which enlarges when fenestration is delayed. There is elevated cerebrospinal fluid volume within the posterior fossa, but the vermis is structurally regular and not rotated. The vermis was present on this case however rotated superiorly, resulting within the keyhole appearance seen between the cerebellar hemispheres. Data summarized from Sherer et al 2007, Zalel et al 2002, and Malinger et al 2001. Measure craniocaudal diameter (red line) from culmen superiorly to uvula inferiorly. Kobayashi Y et al: G�mez-L�pez-Hern�ndez syndrome in a Japanese affected person: a case report. In this case, the malformation drains into the straight sinus, as depicted beforehand. Subsequent analysis for indicators of high-output cardiac failure should be performed. There are diffuse ischemic changes (R > L) with areas of hemorrhage, that are frequent issues, particularly with large shunts. The brain looks normal on this case and the infant was developmentally regular on follow-up. Corral E et al: Thrombosis of the torcular herophili within the fetus: a sequence of eight cases.
Syndromes
- Stop taking any blood thinners, such as aspirin, heparin, or warfarin 5 - 7 days before the procedure
- Blurred vision
- Fainting or feeling light-headed
- Nerve conduction velocity
- Find uterine or cervical cancer
- Nerve conduction velocity (NCV) test
- Lung problems
- Biopsy of lymph node or lung
Solian 100 mg effective
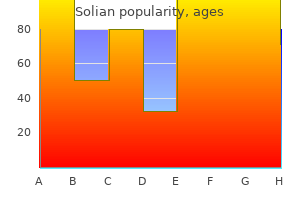
The left-to-right (blue line) & anterior-to-posterior (sagittal yellow line) diameters are measured treatment 001 100 mg solian buy otc, & the ratio is calculated as X/Y treatment keloid scars buy solian 50 mg low cost. Chest Wall Aggressive Lesions � Firm, painful mass � rib destruction, pleural effusion 8. Note the small left postoperative pleural effusion & passive left lower lobe atelectasis. There is complete opacification of the best hemithorax with mass impact on the mediastinum. A heterogeneous mass in the left higher hemithorax is partly cystic & extends into the soft tissues of the left decrease neck. Some lesions reveals abnormal fatty deposition compared to normal (for this age) vertebral marrow, whereas other lesions show elevated fluid sign depth. Situs Evaluation of situs involves the designation of an individual as normal (situs solitus), reversed (situs inversus), or some other mixture (situs ambiguous). The tracheobronchial branching in situs solitus features a trilobed lung & primary bronchus that sits posteriorly &/or superiorly to the pulmonary artery (eparterial bronchus) on the best & a bilobed lung with a major bronchus sitting beneath the pulmonary artery on the left (hyparterial bronchus). In the heart, concentrate on symmetric atria & appendages in patients with heterotaxy as these may characterize 2 proper atria or 2 left atria in right or left isomerism. It is often not troublesome to differentiate the ventricles based mostly on the prominence of the trabeculations. The proper ventricle might extra confidently be identified by the presence of a moderator band (muscular fibers connecting the free wall of the right ventricle to the interventricular septum). Also, pay attention to the tracheobronchial branching relative to the pulmonary arteries: It could also be abnormal bilateral left-sided branching (hyparterial bronchi) or bilateral right-sided branching (eparterial bronchi). These embrace pig bronchus, congenital stenosis, & bilateral right- or left-sided tracheobronchial branching seen with heterotaxy syndromes. More common than congenital airway anomalies is airway compression from cardiomegaly & enlarged or anomalous vasculature. Atria & Veins It is necessary to ensure the venous drainage empties into the appropriate chamber of the guts. As expertise advances, the flexibility to evaluate valvular & septal structures may also enhance. Ventricles A ventricular septal defect is any communication of the proper & left ventricles. These defects are most commonly in the membranous portion of the interventricular septum. In advanced congenital heart patients, defects are additionally regularly seen within the muscular portion of the ventricular septum. Included within the evaluation of the ventricles are the best & left ventricular outflow tracts. Outflow tract analysis consists of assuring the patency (no atresias), separation (no truncus anomaly), & connection to the suitable great vessel (no transposition). Basic measurements of the size of the aorta are made at the sinuses of Valsalva, aortic valve annulus, sinotubular junction of the ascending aorta, transverse aortic arch, & descending aorta. Basic measurements are made for the main pulmonary artery on the pulmonary valve annulus, mid main pulmonary artery, & proximal & distal right & left pulmonary arteries. A patent ductus arteriosus is often present in advanced congenital heart sufferers. Coronary Arteries the origin, course, & termination of the coronary arteries should be evaluated when potential. Visualization of the coronaries is variable depending on the type of examination performed. It is necessary to observe that sure coronary anomalies that can alter the surgical approach. Sudden demise can happen in patients (typically athletes) with an interarterial (malignant) course of the coronary arteries. This is most commonly seen when the left coronary arises from the right coronary sinus or when the right coronary artery arises from the left coronary sinus. The aberrant artery then programs between the proper & left ventricular outflow tracts. Coronary artery fistulas are incessantly seen in patients with a hypoplastic proper ventricle. It is common to see a partial interarterial course of the right coronary artery in a patient with tetralogy of Fallot since clockwise rotation of the aortic root is seen in a big percentage of these patients. Finally, for any anomaly where a coronary artery courses in entrance of an outflow tract, alert the surgeon so she or he can avoid severing the vessel throughout surgery. Routine useful evaluation includes calculating the volumes & ejection fractions of both ventricles. Indexed volumes are obtained by dividing the gross volume by the physique floor area. Standardized data is out there to compare quantity & muscle mass results with different measurement & age matched information units. A pulmonary to systemic move ratio (Qp/Qs) is routinely supplied by interrogating the circulate from the best & left ventricular outflow tracts. In sufferers with pulmonic & aortic regurgitation, velocity-encoded phase-contrast imaging can be utilized to calculate regurgitant fractions. The regurgitant fraction is calculated by dividing the regurgitant quantity by the stroke quantity. Similar purposes can be used to evaluate other veins, arteries, & valves as needed. Regurgitant fractions are usually followed yearly in sufferers with a pulmonary homograft to assess the severity of pulmonic regurgitation. These might include cardiac tumors, cardiomyopathies, ischemic coronary heart illness, myocarditis, & coronary artery abnormalities. Adjusting for dimension & utilizing prospective gating, in addition to different strategies, can considerably reduce the radiation dose. Cardiac 3D Models Segmentation of the anatomy in a patient with advanced illness is often performed, & 3D pictures are utilized in presurgical planning. Once the photographs are segmented, they are often exported to 3D printers to create bodily fashions of the center. Simple resin models of the heart can be printed & utilized in educating dad and mom, sufferers, & different well being professionals. Examples embody the coiling of aneurysms, sizing of gadgets for closure of intramuscular ventricular septal defects, & Melody valve placement along the pulmonary outflow tract. Echocardiography offers glorious delineation of the intracardiac anatomy, great artery relationships, & perform of the guts. Extracardiac anatomy may be tough to utterly evaluate by echocardiography in complicated circumstances. Bilateral upper extremity injections were performed to get even contrast enhancement of the pulmonary arteries & exclude embolism. Notice the tortuous path of a patent ductus arteriosus (green) arising from the left subclavian & inserting into the left pulmonary artery, finishing the vascular ring.
Solian 100 mg buy cheap on line
Another group of agents treatment water on the knee solian 50 mg purchase on-line, organic nitrites (eg medications and grapefruit juice purchase solian 100 mg amex, amyl nitrite, isobutyl nitrite), include the nitrite functional group. Sublingual dosing relieves acute assaults, whereas long-acting medication (oral, transdermal) with a slow onset of action are used for extended prophylaxis. Loss of nitrate efficacy brought on by tolerance can be reversed by use of sulfhydrylyielding brokers such as N-acetylcysteine. Rupture often happens in lipid-rich and foam cell-rich peripheral margins and may lead to thrombosis and arterial occlusion. Drugs are given long-term to scale back the number of assaults, simply earlier than sure actions to prevent acute assaults, and through assaults to relieve pain and pressure. Nitroglycerin is more practical than nitroprusside, an identical organic nitrate, in reducing venous return but is less efficient in increasing arteries. Ca2+ binds to calmodulin in smooth muscle and troponin in the coronary heart and affects muscle contraction. Results are adverse inotropic (force of contraction), chronotropic (rate), and dromotropic (conduction) effects. Systolic failure is the shortcoming of the ventricle to empty normally; diastolic dysfunction is the inability of the ventricle to fill correctly. Aging, smoking, weight problems, fat, cholesterol, inactivity, viruses, and genetic defects promote heart failure; risk is also elevated by hypertension and diabetes. Accumulation of fatty deposits in heart arteries results in coronary artery disease. The commonest types of heart failure-caused by damaged coronary heart muscle-are treated with medicine to enhance quality of life and survival. Glycosides improve coronary heart contractility and contraction force by activating Na+-K+ pumps on coronary heart cells. Blockers such as propranolol are particularly helpful for exertional angina but are ineffective in opposition to vasospastic angina. They are utilized in combination with calcium channel antagonists (eg, dihydropyridines, verapamil, diltiazem), natural nitrates, or both to treat cardiac signs that are resistant to a single drug. Dihydropyridines, but not diltiazem and verapamil, can be used in such a mixture. Digoxin is the commonest digitalis preparation; digitoxin is used when an extended halflife is needed (7 days versus 1-2 days for digoxin). After digitalis restores heart perform, its use is sustained to stop recurrence of heart failure. Digitalis may reduce the progression fee of coronary heart injury in some patients, especially these in whom an increase in end-diastolic pressure and volume will occur. Digitalis reduces sympathetic tone by directly blunting the baroreceptor response. Medical conditions (eg, anemia, fever, coronary heart failure, electrolyte imbalance) may cause arrhythmias. Synchronized electrical shock (defibrillation), electronic pacemakers, and radiofrequency ablation are nondrug therapies. If symptomatic and severe (rates 40/min) with nonreversible cause, consider permanent pacing. No intervention unless symptomatic Sinus bradycardia (60 bpm) If asymptomatic, no intervention. If symptomatic and extreme (rates 40/min) with nonreversible trigger, think about momentary pacing. Premature atrial complexes Premature ventricular complexes If asymptomatic, no intervention. Warfarin, an anticoagulant, is used for atrial fibrillation to stop strokeinducing blood clots. The commonest antagonistic effect of warfarin is bleeding, from gentle nosebleed to life-threatening hemorrhage. Antiarrhythmic medicine, such as amiodarone and sotalol, maintain the traditional rhythm of the heart. The selective blockers have fewer central antagonistic effects than nonselective blockers, corresponding to propanolol. Level of blood pressure is associated with cardiovascular occasions in a steady, graded, and apparently independent fashion. This pressure, or blood stress, is a measure of how much work is required by the heart to push blood via the arteries. The 2 numbers used to point out blood stress correspond to systole and diastole (eg, 120/80 mm Hg). The systolic (top) quantity reflects stress of blood in opposition to arterial walls that results from contraction of the heart. The diastolic quantity (bottom) displays arterial blood strain whereas the guts is filling and resting between beats. High blood pressure in adults is outlined as a persistently increased blood stress of 140/90 mm Hg or higher. Hypertension is known as the "silent killer" because it causes severe problems with out apparent symptoms. Liver Adrenal Medulla Cortex Hypertension Cortical tumor may improve aldosterone output. Renin substrate (angiotensinogen) Compression of extrarenal or intrarenal vessels promotes output of renin by juxtaglomerular cells. Diuretics have been the main antihypertensive medicine for decades and are still thought to be one of the best therapy for AfricanAmerican and aged sufferers and the best agents for preventing stroke. Thiazides (eg, chlorothiazide, chlorthalidone) are taken alone for reasonable hypertension or used in combination with different drug types. Potassium-sparing brokers (eg, amiloride, spironolactone) enhance potassium retention by kidneys and increase K+ levels within the physique. Na+ H2O Na+ K+ Compression of extrarenal or intrarenal vessels promotes output of renin by juxtaglomerular cells. Aldosterone promotes Na+ and H2O retention, K+ excretion, and arteriolar constriction. Most adverse results are gentle; renal failure and fetal/neonatal morbidity may happen. Hypertension and Blockers Intracranial strain could have an result on blood supply to brain, thus influencing neural mechanisms. Cortex Catecholamines from adrenal medulla affect tone of resistance in vessels as nicely as coronary heart rate and output. Blockers are prescribed together with other antihypertensive agents to deal with hypertension. They are glorious for patients with angina however ought to be averted by patients with bradycardia (low coronary heart rate), bronchial asthma, and persistent bronchitis.
Cheap 100 mg solian with visa
The infant had no feeding difficulties symptoms narcolepsy order 100 mg solian with amex, and resection was delayed to 6 months of age symptoms 4 weeks generic solian 100 mg overnight delivery. Histology showed dilated lymphatic spaces with an endothelial lining typical of a mesenteric lymphangioma. This gallery of pictures reveals the variable appearance of a mesenteric lymphangioma from complex (more common) to unilocular, as on this case. It is troublesome to tell whether that is 1 stone or multiple small stones that are clumped collectively. Troyano-Luque J et al: Short and long run outcomes related to fetal cholelithiasis: a report of two cases with antenatal analysis and postnatal follow-up. This choledochal cyst grew all through the pregnancy and the new child developed jaundice and wanted surgical procedure by day 12 of life. Definitive therapy for type 1 choledochal cyst is cyst resection and biliary diversion. Cong X et al: Evaluation and screening ultrasonic indicators in the diagnosis of fetal biliary cystic malformation. Staging, Grading, & Classification � Todani modification of Alonso-Lej classification Type 1: Cystic, saccular, or fusiform extrahepatic biliary dilatation (80-90% of cases) Type 2: Common bile duct diverticulum Type 3: Choledochocele 5. A clue to the vascular nature of the mass on this grayscale image is the massive draining vein (Doppler confirmed flow). The fetus was followed carefully and began to show signs of hydrops at 38 weeks, which precipitated delivery. There is dramatic arteriovenous shunting inside the mass, typical of a congenital hepatic hemangioma. The differential consideration was both a mesenchymal hamartoma or a lymphangioma that concerned the liver capsule. Mesenchymal hamartomas are benign and surgical procedure is curative but will not be attainable if the tumor is extensive. Fetal instances often present speedy development and have a extra guarded prognosis than these diagnosed later in childhood. Harris K et al: Placental mesenchymal dysplasia with hepatic mesenchymal hamartoma: a case report and literature evaluation. A spoke-wheel appearance is used to describe the pattern of varying echogenicities within the mass. There is a light quantity of disorganized internal vascularity however no enlarged draining vessels as seen with a congenital hepatic hemangioma. Miura Y et al: Diagnosis and therapy of a preterm infant with inoperable congenital hepatoblastoma-a case report. There was marked hepatomegaly with the left lobe having a traditional homogeneous appearance, whereas the best has giant areas of irregular, heterogeneous, low sign depth. Metastases could both be diffusely infiltrating, as shown right here, or type discrete plenty. Small or infiltrating hepatic metastases could be troublesome to discern prenatally, but the liver ought to at all times be given cautious scrutiny as 25% of neuroblastoma instances have liver involvement. The abdomen was massive with hepatomegaly and a small quantity of ascites (compare the protuberant stomach to the normal-sized chest). A presumptive analysis of trisomy 21 with leukemia was made, which was confirmed at supply. The parents were subsequently found to be cystic fibrosis carriers, and the fetus was identified with cystic fibrosis at delivery. Meconium Peritonitis (Mimic) Fetal Growth Restriction (Left) Plaque-like calcifications scattered in the abdomen and outlining the serosal floor of the fetal abdomen are basic options of meconium peritonitis. In an oblique plane it appears like fluid but the place the beam is perpendicular the muscle layers could be seen. Note the hypoechoic stomach wall musculature positioned exterior the peritoneal cavity. Hydrops 560 Ascites Abdominal Wall and Gastrointestinal Tract Bowel Perforation Bowel Perforation (Left) this indirect picture via the abdomen reveals bowel dilation from jejunal atresia. The ascites is from bowel perforation and this constellation of findings is pathognomonic for meconium peritonitis. Urinary Ascites Urinary Ascites (Left) this midline sagittal image in a case of posterior urethral valves exhibits a massively dilated bladder and tortuous ureter. The bladder is thick-walled from chronic obstruction and partially decompressed following rupture. Infection Arrhythmia (Left) Hepatosplenomegaly is a outstanding feature of fetal infection. In this case of syphilis, ascites is seen surrounding the markedly enlarged spleen (calipers). When considering an infection, additionally look for intrahepatic and intracerebral calcifications. Most stomach cystic lots are from urinary tract Gastrointestinal tract subsequent most typical � Is it simple cyst or complicated cystic mass Thin-walled, thick-walled, calcified, intestine signature � Is it fixed or does it change look throughout examination, between exams Helpful Clues for Common Diagnoses � Multicystic Dysplastic Kidney Multiple cysts of varying sizes with no discernible renal parenchyma Reniform form is lost Variable in utero course: May involute, stay secure, or develop May be huge and cross midline � Ureteropelvic Junction Obstruction Look for communication with dilated calyces Ends abruptly at ureteropelvic junction, no ureteral or bladder dilation May present as large cyst with no remaining regular parenchyma if severe obstruction � Lower Urinary Tract Obstruction Posterior urethral valves commonest trigger � Look for keyhole look created by dilated posterior urethra Prune-belly syndrome and urethral atresia less frequent Ureteral dilation and hydronephrosis additionally commonly seen Helpful Clues for Rare Diagnoses � Choledochal Cyst Cystic dilatation of extrahepatic &/or intrahepatic bile ducts Unilocular, easy, right upper quadrant cyst is most common presentation in fetus � Round in axial aircraft and fusiform in longitudinal plane Following bile ducts into cyst confirms analysis � Urachal Anomaly Includes isolated cysts and patent urachus Communication with bladder confirms patent urachus Bladder might appear elongated with figure eight or waisted configuration May prolong into base of umbilical wire 562 Cystic Abdominal Mass Abdominal Wall and Gastrointestinal Tract � Associated with allantoic cord cysts May resolve as gestation progresses � Neuroblastoma Arises from adrenal gland ~ 50% are cystic Complex look with thick septations Cystic neuroblastoma has wonderful prognosis � Splenic Cyst Incidental discovering of no clinical significance If posterior to abdomen could seem as cystic suprarenal mass and be confused with cystic neuroblastoma Use high-frequency transducer to verify location in splenic parenchyma � Fetus-in-Fetu, Teratoma Overlapping features between these 2 entities � Fetus-in-fetu more developed and must have spinal parts Complex, with large strong part encapsulated within cyst Calcifications, together with well-formed bones, most specific finding Majority reported in higher retroperitoneum Fetus-in-fetu thought to end result from inclusion of monochorionic diamniotic twin within host twin � Hydrocolpos Cystic mass (distended vagina) posterior to bladder Vagina not septated as in cloacal malformation Normal external genitalia � Cloacal Malformation In basic cloaca the bladder, vagina, and rectum all talk with single perineal opening Vagina duplicated in share creating longitudinally septated mass Fluid-fluid levels from mixing of meconium, vaginal secretions, and urine Abnormal genitalia with lack of normal labial/clitoral formation; absent anal dimple Hydronephrosis and lumbosacral anomalies may also be present Ascites reported in some circumstances from retrograde move via fallopian tubes Multicystic Dysplastic Kidney Multicystic Dysplastic Kidney (Left) Multicystic dysplastic kidneys are often very large and filled with cysts of various measurement. A clue that these giant "cysts" are actually related to the kidneys is their posterior location adjoining to the spine. This can also be shown on the autopsy picture the place the ureter is seen "snaking" by way of the abdomen. There was a unilateral accumulating system rupture, partially decompressing the left amassing system. Note how the fluid is surrounding and compressing the kidney, traditional features of a urinoma. Surgery confirmed an ileal atresia with perforation, sophisticated by meconium peritonitis and pseudocyst formation. In this case, there are small peripheral cysts with an echogenic central stroma, a characteristic seen with torsion. The appearance of mesenteric lymphangiomas is sort of variable, starting from a unilocular cyst to a big complex mass. Use a high-frequency transducer to search for a trilaminar gut signature with a hyperechoic mucosa, hypoechoic muscular wall, and hyperechoic serosa. A small tubular construction, felt to be a bile duct, could presumably be seen contiguous with it. During real-time evaluation, the cyst may enhance in size when the bladder contracts during voiding, sending urine into the cyst. Urachal Anomaly Neuroblastoma (Left) Axial scan via the higher stomach shows a complex cystic mass. Given this cyst was suprarenal, an adrenal hemorrhage was additionally thought of in the differential, but it remained unchanged. Neuroblastoma Splenic Cyst (Left) this fetus offered at 22 weeks with a left-sided suprarenal cyst that was easy in appearance. This meets the strict criteria for a fetus-in-fetu, which is felt to outcome from an aberration in monochorionic twinning.
Purchase solian 100 mg overnight delivery
Its pathogenesis is unclear; nevertheless medicine ball chair solian 50 mg purchase with amex, the nephropathy of getting older seems to be categorically completely different from that of natural development because medicine rash purchase 100 mg solian with amex, not like natural progression, the nephropathy of getting older proceeds with out essential increases in proteinuria (see Chapter 67). The vicious cycle is entered when the hyperperfusion and metabolic dysfunctions are adequate to inflict kidney injury. Described herein are evidence-based therapies to prevent entry into the vicious cycle or to sluggish the cycle once it has been entered. If that might be reasonably excluded, it should then be decided whether another kidney disorder has been superimposed (see Chapter 71). Here we discuss the latter, that are probably the most sensible and commonly used strategies to monitor development. The threshold for natural progression attributable to proteinuria seems to be crossed when proteinuria exceeds 500 mg/day. For conditions 1 via 6, see Chapters 29, 33, forty four, fifty six, sixty two, and 65, respectively. The beneficial methods for monitoring proteinuria tendencies in particular person patients are shown in Table 80-1. The key points are as follows: the gold commonplace for monitoring proteinuria is the protein content of an precisely collected 24-hour urine specimen. Unfortunately, in follow, nominal 24-hour urine collections typically are largely undercollections or overcollections. For this reason we favor the time period "intended" 24-hour urine assortment when such collections are made. Comments Table 80-1 Recommended and nonrecommended strategies for monitoring proteinuria or albuminuria. Degree of completeness of an meant 24-hour urine assortment = measured creatinine content material (M)/expected creatinine content material (E). Recommended Kidney Protective Therapies According to Level of Recommendation Level 1 Recommendations 1. Box 80-3 Recommended kidney protecting therapies according to level of advice. This profit of having acquired the antihypertensive study drug in the course of the randomized trial was independent of the class of the antihypertensive examine drug. Administration of antihypertensive drugs at night might improve their efficacy in stopping cardiovascular events. However, in our experience such high-dose therapy has not been useful, even when combined with aldosterone antagonists, salt restriction, protein restriction, diuretic remedy, and statin therapy. Renin Inhibitor Therapy Aliskiren, a direct renin inhibitor, is an efficient antihypertensive agent and has been shown to scale back albuminuria in diabetic nephropathy and IgA nephropathy. Reducing dietary protein intake from the usual stage (in developed nations about 1 to 1. Panel C: Add aldosterone antagonist, especially if a number of of the following are present: � Pre�diabetes mellitus or diabetic mellitus � Serum K+ tends to be at the low finish of regular � Arrhythmia/cardiomyopathy considerations Start spironolactone 25 mg daily or eplerenone 50 mg daily. In this respect, carvedilol could additionally be an exception, particularly with regard to individuals with hyperglycemia. In addition edema formation, pericardial infusion and hirsutism are important problems. This drug has since lost favor, except as a drug to control the symptoms of prostatism. Men and those with glomerular illness could significantly benefit from the lowprotein diet. The threat of protein-energy wasting will increase with coexisting inflammatory disorders similar to diabetes, extreme atherosclerosis, or autoimmune diseases. Alkali therapy can mitigate protein-energy losing (see the discussion of alkali therapy). The mechanism of the superior effect of chlorthalidone may be related to its more practical suppression of carbonic anhydrase and its capacity to help regulate nitric oxide better than hydrochlorothiazide. Urine sodium should be measured each time 24-hour urine protein is measured (see the discussion of monitoring of proteinuria). Spironolactone and the extra selective aldosterone antagonist eplerenone have substantial antihypertensive, cardioprotective, and antiproteinuric effects even at low doses. These measures embody sodium bicarbonate therapy (see the dialogue of alkali therapy), the avoidance of potassium-rich meals, and consciousness of the symptoms of extreme hyperkalemia. These include the comparatively sudden onset of symmetric proximal muscle weak spot (difficulty climbing stairs or rising from a chair) or muscle stiffness. On arrival the affected person should immediately advise the medical personnel that severely elevated serum potassium may be the problem. Cigarette smoking promotes development of all types of kidney illness in a dose-dependent manner, perhaps extra in these of African American ancestry. There is ample experimental evidence that uric acid is proinflammatory and vasculotoxic1 and that allopurinol is anti-inflammatory and cardioprotective by a quantity of mechanisms. This is practical advice as a end result of the danger of extreme allopurinol reactions appears to be restricted to the first eight weeks of remedy, and immediate withdrawal of the offending drug is related to decreased mortality threat. StevensJohnson syndrome has been reported in postmarketing surveillance of febuxostat. If after 8 weeks that dose is well tolerated, it can then be increased till the uric acid degree is at aim (less than 7 mg/dl). Also, the patient must be strongly cautioned, when she or he begins allopurinol or when the dose is increased, to cease the allopurinol if rash, fever, or other signs of illness develop. However, there have been no high-quality randomized trials to take a look at that speculation. To achieve phosphorus control (see Chapter 85), the next are advised: Phosphorus control ought to begin earlier than the serum phosphorus is constantly greater than four. The first method is to scale back phosphorous intake with the precaution that severely decreasing meat and dairy merchandise might lead to protein malnutrition. If grains are substituted for meat and dairy merchandise, better management of serum phosphorous can be achieved. If dietary measures are ineffective, use of phosphate binders is generally really helpful. The proof favors the notion that calciumcontaining phosphorous binders are more probably to lead to vascular calcification and increase cardiovascular risk than noncalcium phosphate binders (see Chapter 85). Spot urine protein/creatinine ratios are unreliable estimates of 24 h proteinuria in most systemic lupus erythematosus nephritis flares. An method to validating standards for proteinuric flare in systemic lupus erythematosus glomerulonephritis. Systematic evaluation: Blood pressure target in persistent kidney disease and proteinuria as an impact modifier. Persistence of mortality discount after the end of randomized therapy in scientific trials of blood pressure-lowering drugs.
Buy 50 mg solian mastercard
Ischemic stroke because of treatment 3rd degree av block 100 mg solian purchase amex in situ Ischemic stroke due to treatment bipolar disorder solian 100 mg discount mastercard in situ thrombosis, usually triggered by thrombosis, usually triggered by plaque rupture within the carotid or plaque repture within the carotid or cerebral artery. Myocardial infarction and associated heart disease account for 70% of the mortality in folks with diabetes. In one principle that involves an autoimmune-mediated mechanism, predisposed sufferers react abnormally to environmental triggers by producing antibodies that are directed in opposition to cells. Patients require lifelong therapy with exogenous insulin to control blood glucose ranges and prevent short- and long-term macrovascular and microvascular problems corresponding to nephropathy, neuropathy, retinopathy, and heart problems. Protein O Glucose O Glucose Insulin receptor down-regulation Triglyceride Fatty acid Adipocyte Amino acids Glucose accumulates in blood. Before diabetes is recognized, sufferers, typically overweight, have hyperinsulinemia caused by extra dietary carbohydrates. Resistance develops in a quantity of attainable ways, eg, continual hyperinsulinemia causes insulin receptor down-regulation, which leads to defects in insulin binding and postreceptor insulin signaling pathways. Oral hypoglycemic brokers decrease plasma glucose ranges, improve insulin resistance, and cut back long-term complications. Exogenous insulin stimulates carbohydrate metabolism and helps with transfer of glucose into cardiac and skeletal muscle and adipose tissue. Insulin also aids in conversion of glucose to glycogen, stimulates lipogenesis and protein synthesis, and reduces serum potassium and magnesium ranges. Absorption of an insulin product could differ in a patient from one injection to the following, absorption being affected by site of injection, temperature, physical activity, and dose. Insulin preparations differ in dose, onset, length, and sources of origin, including biosynthetic and semisynthetic human (therapeutically equal), human insulin (least antigenic and most soluble), and beef and pork (replaced by human). Symptoms are autonomic (eg, sweating, trembling, feeling of warmth) or neuroglycopenic (eg, confusion, weak point, drowsiness). Elderly patients with neuropathy, sufferers with long-standing diabetes (>10 years), and sufferers taking blockers can have blunted symptoms. Insulin injection can also trigger lipohypertrophy, which happens in sufferers who use only one site somewhat than rotating websites. Lipoatrophy, an immunologic reaction to insulin, is treated by changing to human insulin and injecting it into the affected area. Older medicine (eg, chlorpropamide, tolbutamide) have been replaced by new agents (eg, glimepiride, glipizide, glyburide), with higher potency, fewer drug interactions, and better pharmacokinetic profiles. If glucose control fails with long-term sulfonylurea use, different brokers may be added as a substitute of increasing sulfonylurea doses. Sulfonylureas are greatest for sufferers recognized after the age of 40 years or when disease duration is less than 5 years, physique weight is type of ideal, and fasting glucose ranges are less than one hundred eighty mg/dL. Metformin decreases blood glucose levels by lowering hepatic glucose production and glycogen metabolism and bettering insulin resistance via enhancing insulin-mediated glucose uptake. Hypoglycemia occurs solely when metformin is used with insulin or hypoglycemic medication. Similar to sulfonylureas, meglitinides trigger a rise in insulin secretion from pancreatic cells. Unlike sulfonylureas, meglitinides have a speedy onset and a shorter duration, which necessitates dosing within 30 minutes of every meal. These medication inhibit glucosidases within the small gut brush border that break down (hydrolyze) complicated polysaccharides and sucrose into absorbable monosaccharides. The price of carbohydrate digestion and glucose absorption is thus delayed, which finally ends up in decrease postprandial glucose spikes (by 25-50 mg/dL). These medication work best in sufferers with postprandial hyperglycemia and when taken with a meal containing advanced carbohydrates. Receptor activation modulates transcription of a number of insulinresponsive genes that control glucose and lipid metabolism. The liver, however, is resistant to that insulin and therefore continues to produce large quantities of glucose. Instead of stimulating the pancreas to produce extra insulin, sensitivity to present insulin ought to be increased to sluggish hepatic glucose production. Other functions are excretion of waste and secretion of hormones into the blood for delivery to distal targets. It is the normal route for water and salt consumption and a possible supply of fluid and electrolyte loss. During digestion, a big volume of digestive secretions is added to the ingested, chewed, and swallowed meals. Nearly all of this mixed combination have to be reabsorbed to avoid major disturbances in fluid-electrolyte and acid-base balance. The small gut provides a large floor space for the absorption of nutrients and drugs. Laxatives trigger emptying of the colon and defecation by stimulating peristalsis or by including extra bulk or water to the feces. Peptic ulcer illness is brought on by an erosion of the mucosal layer of the stomach or proximal small gut (duodenum). Peptic ulcer disease is finest handled by a mixture of way of life changes and medicines. These brokers embrace histamine antagonists, corticosteroids, phenothiazines, benzodiazepines, and serotonin receptor antagonists. Principal elements of the enteric nervous system are 2 networks or plexuses of neurons, each of which are embedded in the wall of the digestive tract and prolong from the esophagus to the anus. The myenteric (Auerbach) plexus is situated between the longitudinal and circular layers of muscle within the tunica muscularis and controls primarily digestive tract motility. Sensory neurons receive data from sensory receptors in the mucosa and muscle. Interneurons combine info from sensory neurons and transmit it to enteric motor neurons. A ring of muscle contraction appears on the oral side of a food bolus and strikes toward the anus, so the luminal contents are forced in that path. A stronger wave (B) is originating at incisure and is once more squeezing gastric contents in each instructions. Duodenal bulb might contract or might stay crammed as peristaltic wave originating simply past it empties second portion. Contents of duodenal bulb space pushed passively into second portion as extra gastric contents emerge. Mixing ensures that ingested materials are uncovered to digestive enzymes and correctly absorbed. Segmentation contractions are a common kind of mixing motility seen especially within the small gut; segmental rings of contraction break down and mix food. Alternating contraction and relaxation of longitudinal muscle in the gut wall additionally offers efficient mixing of its contents. Important peristaltic reflexes are the gastrocolic, in which stomach distension causes colonic exodus, and the enterogastric, by which small intestine distension or irritation reduces abdomen secretion and motor exercise.