
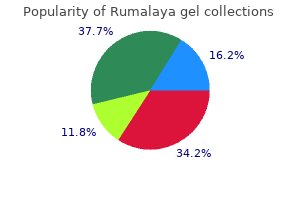
Rumalaya gel dosages: 30 gr
Rumalaya gel packs: 1 tubes, 2 tubes, 3 tubes, 4 tubes, 5 tubes, 6 tubes, 7 tubes, 8 tubes, 9 tubes, 10 tubes

30 gr rumalaya gel discount
A 5-mL syringe with a 25-gauge needle may be used to subcutaneously infiltrate 2 mL of tumescent anesthetic resolution (420 mL of regular saline muscle relaxant non-prescription rumalaya gel 30 gr discount with mastercard, 60 mL of 1% lidocaine with epinephrine spasms before falling asleep rumalaya gel 30 gr discount on-line, and 20 mL of sodium bicarbonate) over the access web site. This answer is delivered manually or with an infusion pump underneath ultrasound steerage, aiming to surround the vein section to be treated. Moderate ache along the handled vein and superficial thrombophlebitis happens in as much as 50% and 12% of the limbs, respectively. Tumescent anesthesia is required, and a dilute combination of lidocaine in normal saline may be used (50 mL of 1% lidocaine with 1:200,000 epinephrine in 500 mL zero. The warmth generated in the vein wall (not in the catheter tip) is then dissipated and causes managed collagen contraction or whole thermocoagulation of the vein. The consequence is managed tissue destruction that ultimately seals the lumen with minimal thrombus or coagulum. For instance, with a temperature of eighty five �C to 90 �C and a pullback velocity of three to 4 cm/min, the thermal impact is adequate to cause collagen contraction and occlude the lumen. Complications include paresthesia, hematoma, pores and skin burns, an infection, bruising, and thrombophlebitis/thromboembolism. Transient paresthesia is reported in up to in 15%, hematoma in 5%, skin burns in 2. Ligation of the vein at the saphenofemoral junction at the aspect of removal of the thigh portion of the vein also can cut back venous reflux. Venous stripping could also be carried out at the facet of ligation of the saphenofemoral junction, phlebectomy, or chemical sclerotherapy. Saphenous vein stripping has a better initial value due to hospitalization and ends in more time misplaced from work compared with endovenous procedures. Saphenous vein tributaries are identified and ligated till reaching the saphenofemoral junction. In one research of 210 legs in 182 sufferers with major saphenofemoral junction incompetence, the recurrence price for saphenofemoral junction ligation was 5. The relative risk of recurrence after ligation of the saphenofemoral junction alone is 2. A mixture of saline and native anesthetic is infused in to the subcutaneous tissue to produce tumescence and transilluminate the vein. Robert Muller, a Swiss dermatologist from Neuch�tel, Switzerland, rediscovered this system in 1956. After tumescent anesthesia, with the patient in Trendelenburg position, cutaneous incisions are made with a #11 scalpel blade or 18-gauge needle, vertically oriented alongside the thigh and decrease leg following the skin strains at the knee or the ankle. Incompetent perforators may be dissected and eradicated with mild traction or torsion, but that is tougher. Ongoing compression remedy with elastic bandages or compression stockings is really helpful for up to three weeks. Complementary chemical sclerotherapy could also be used a quantity of weeks after the initial procedure. Periprocedurally, sufferers should avoid early sun exposure because hyperpigmentation might outcome at the puncture or incision websites. This is achieved through the use of venous ligatures guided by hemodynamic and duplex ultrasonography knowledge derived from the deep and superficial venous system. The current Society for Vascular Surgery and American Venous Forum guidelines do suggest remedy of so-called pathological perforating veins, outlined as those with outward flow of 500-ms duration, diameter of three. Similarly, efficiency of those procedures in patients with deep vein occlusion is related to poor outcomes. The initial incompetent perforator closure fee was 90%, but fell to 70% at a mean follow-up of 20 months. However, as a result of this entry site is normally made in compromised skin immediately over the perforator, there may be danger of an infection or exacerbation of the wound. Laser obliterates the vein by heating the hemoglobin (Hb) throughout the vessel and injuring the endothelium. New advances in laser know-how have allowed supply of enough energy to obtain pan-endothelial necrosis without affecting buildings in the epidermal layer. It differs from laser by emitting a spectrum of sunshine, quite than a wavelength, to obliterate the vein. The quantity of postcooling is dependent upon the size of the vessels to be handled, with smaller vessels requiring longer postcooling. The laser is utilized to the surface of the pores and skin and targets a wavelength of light to the Hb inside the vessel, leading to heating and obliteration of the vessel. Small (<1 mm) superficial vessels with larger oxygenated Hb content are handled with shorter wavelengths (580-1064 nm), shorter pulse durations (15-30 ms), higher fluences (350-600 J/cm2), and smaller spot sizes (<2 mm). Typically, one to three laser treatments are scheduled at 6- to 12-week intervals. The patient subjective satisfaction index, measuring cosmetics, elevated from 42. Objective enchancment in cosmetic look, measured with computerassessed medical photography, elevated from 57% at 6 months to 82. Other complications embody edema, erythema, bruising, vesiculation, hypo/hyperpigmentation, transient hemosiderin staining, telangiectatic matting, and scarring. This process is contraindicated during pregnancy and in those with tanned or dark pores and skin, history of photosensitivity dysfunction, or keloidal scarring. Patients are advised to keep away from tanning before the process to keep away from absorption of shorter wavelengths from the laser by sun-induced melanin, resulting in blistering and hyperpigmentation. Laser and light therapies are costlier than liquid sclerotherapy, owing to the worth of gear. To lower telangiectatic matting and postsclerosis hyperpigmentation, a lowered quantity of froth per injection (0. The chance of recurrence at 5 years is 5% to 30%, relying on the therapy administered and ongoing danger components. Obesity, multiple pregnancies, incompetent perforators, and saphenofemoral junction incompetence are a variety of the often-mentioned danger elements for recurrence. However, sufferers will generally return for repeated therapies over their lifetime. Nael R, Rathbun S: Treatment of varicose veins, Curr Treat Options Cardiovasc Med 11(2): 91�103, 2009. Miyazaki K, et al: Long-term outcomes of treatments for varicose veins due to larger saphenous vein insufficiency, Int Angiol 24(3):282�286, 2005. Marsh P, et al: Pelvic vein reflux in female patients with varicose veins: comparability of incidence between a specialist personal vein clinic and the vascular department of a National Health Service District General Hospital, Phlebology 24(3):108�113, 2009. Kachlik D, Pechacek V, Baca V, et al: the superficial venous system of the decrease extremity: new nomenclature, Phlebology 25:113�123, 2010. Chronic venous insufficiency and varicose veins, N Engl J Med 360(22):2319�2327, 2009.

Order rumalaya gel 30 gr on line
For these girls with recurrent being pregnant loss with out aneuploidy infantile spasms 2012 rumalaya gel 30 gr with amex, the data is less clear muscle relaxant without aspirin rumalaya gel 30 gr with mastercard. It has been difficult to evaluate studies because of broad variation in definition and molecular method used for screening. Paracentric inversions solely yield 50% viable gametes but these are balanced whereas pericentric inversions produce 100% viable gametes with 50% of them unbalanced. The threat of unbalanced offspring in Robertsonian translocations (those involving acrocentric chromosomes) depends on the sex of the provider father or mother and the chromosomes involved. Unique situations involving nondisclosure of parental genotype might happen if a parent at threat of an adult-onset disorder needs unaffected offspring with out figuring out his/her provider standing. Longer survival and improved high quality of life for these sufferers translate in to practical expectations to turn into parents. Patients who may have or carry single-gene defects might have a history of genetic disease in a member of the family or a family historical past of unexplained being pregnant losses or neonatal deaths. Those couples who desire preimplantation testing should also be made conscious of the inherent limitations of the testing due to a baseline error rate relying on the molecular approach used, the contribution of embryonic mosaicism, and the chance of a decreased general embryo yield per cycle. Preimplantation genetic analysis reduces pregnancy loss in women aged 35 years and older with a history of recurrent miscarriage. Comparison of blastocyst switch with or without preimplantation genetic analysis for aneuploidy screening in couples with superior maternal age: a prospective randomized managed trial. Depending on the standards used for prognosis, the prevalence ranges from 9% to 18% (1). Diagnostic criteria, clinical presentation, potential pathophysiology, and evidence-based therapies are summarized right here. For the Rotterdam standards, two out of the following three symptoms are required: oligo-ovulation and/or anovulation, medical and/or biochemical signs of hyperandrogenism, and polycystic ovaries (3). Importantly, all three diagnostic standards require the exclusion of other etiologies of menstrual irregularities and hyperandrogenism. Virilization (clitoromegaly, male-pattern frontal balding, or increased musculature) may also recommend tumor development. The type of menstrual dysfunction can range, but the underlying etiology is similar, anovulatory cycles. Most patients current with oligoovulation or anovulation leading to oligomenorrhea or amenorrhea. This extreme bleeding could be the end result of an absent luteal section inflicting heavy, prolonged bleeding as a outcome of unopposed effects of estrogen. Additional testing, such as a luteal progesterone level, can help to determine if cycles are anovulatory. Therefore, it is necessary to correlate the presence of polycystic ovaries with different scientific findings. Hirsutism (excessive hair growth) is the primary medical indicator of hyperandrogenism however its prognosis is subjective and ethnicity-dependent (6,7). This scale assesses the density and distribution of hair progress on multiple areas of the body. Other, much less particular, clinical options of hyperandrogenism include pimples, oily skin, and male-pattern alopecia. The exact dangers of infertility and spontaneous abortion charges are controversial with varying degrees of risk reported in a number of studies. Some elevated risk is probably going, particularly among overweight patients, manifesting as increased time to conception, reduced efficacy of infertility remedies, and elevated danger of miscarriage. Pathology evaluation of the endometrium is warranted in anovulatory patients regardless of age. The feminine identification and body image are primarily affected, as patients undergo from weight problems, zits, oily skin, excess hair progress, to not mention infertility and several other health care issues. As a result, patients whose lives and moods are significantly affected by the syndrome may also have a harder time complying with way of life and remedy suggestions, all issues that must be recognized and explored by clinicians. They also manifest varied metabolic abnormalities, corresponding to dyslipidemia (15), prothrombotic tendency, and increased proinflammatory markers. Often their diagnosis is delayed because of the assumption of the normalcy of irregular cycles after menarche and decreased severity of hirsutism. However, adolescents still have significant dangers of metabolic comorbidities that might be mediated by early intervention and prevention methods. Several theories have been proposed, two of which have vital supporting analysis. Alternatively, they might characterize parts of the identical complicated physiologic pathway. Anovulation results from insufficient number of a dominant follicle within the setting of hyperthecosis. Other research suggests hyperinsulinemia as the first insult via direct and oblique effects (15). Given the multifaceted approach to administration, a multidisciplinary team is normally needed for best outcomes. Most importantly, lifestyle intervention should address weight reduction or prevention of weight achieve by way of dietary modifications and regular exercise. A physique weight reduction of 5% to 10% has been shown to exert a big profit on major psychological, reproductive (menstrual regulation, ovulation, fertility), and metabolic (hirsutism, insulin resistance, risk components for diabetes and cardiovascular disease) outcomes (20). Medical therapies are sometimes optimal when combined with way of life interventions or nonmedical therapies. The maximal benefit is achieved with mixed estrogen-progestin pills, since these formulations benefit from the first-pass effect in the liver. An different routine is progesterone administration alone for a minimum of 10 days per thirty days. Hirsutism medical therapies include spironolactone, flutamide, finasteride, ketoconazole, and eflornithine. Spironolactone (25�100 mg twice daily) acts as an androgen receptor blocker, stopping the motion of androgens on the hair follicle. It can additionally be a diuretic and ought to be avoided in sufferers with renal impairment as a outcome of increased danger of hyperkalemia. Flutamide (125�250 mg/day) is a nonsteroidal antiandrogen that may be a teratogen and has been associated with hepatotoxicity not often. Finasteride is also a teratogen, however is related to much less renal or hepatic toxicity. Optimal outcomes are achieved when mixed with mechanical removal of hair (see below). The above remedies for hirsutism provide average results over a long term of remedy.
Syndromes
- Alcohol intoxication
- MRI of the chest
- Swollen or tender kidneys
- Progressive muscle weakness
- Paint thinner
- Fibrous dysplasia
- MRI
Generic 30 gr rumalaya gel free shipping
I attempt to muscle relaxant home remedy rumalaya gel 30 gr line send frequent letters to referring physicians to keep them abreast of the progress muscle relaxant safe in pregnancy buy 30 gr rumalaya gel with amex. The specialty is ethically charged to begin with, since its primary focus is on copy. In the normal sense, the act of replica is a personal, pure, and conjugal act between two individuals. However, treatment with the available applied sciences does everything but meet these standards. I will observe that system of regimen which, according to my capacity and judgment, I contemplate for the profit of my patients, and abstain from whatever is deleterious and mischievous. It is complicated within the field of reproductive drugs contemplating that there can be many individuals concerned within the treatment. As providers, we must also decide the impact of our selections on the yet unborn child. To further complicate issues, there are different participants to be considered in instances of egg donation and gestational surrogacy. To this end, there are four key parts that must be in place, including open dialogue, an ethics committee, out there assets, and moral analysis. Open Dialogue When in comparison with most other medical issues, the remedy of the infertile couple is exclusive as a result of it might possibly only be completed via the coordinated effort of a staff made up of physicians, nurses, scientists, psychological health professionals, and different key personnel. Ethics Committee Every heart should have a committee in place and a discussion board to discuss ethical issues. The committee can simply include a doctor, nurse, psychological well being professional, and a representative from the laboratory. One role of the committee is to evaluation the moral points regarding a particular treatment. If a decision is made to supply the therapy, the next step is to develop a complete coverage detailing how the remedy shall be administered. A ultimate position of the committee is to focus on moral points concerning particular person circumstances. Available Resources An essential part of an moral evaluation is utilization of available assets. The resources come from the information of particular person committee members and from exterior sources, as well. They have printed stories and statements titled "Ethical Considerations of Assisted Reproductive Technologies" as supplements to the journal Fertility and Sterility. These principles are used when performing a proper ethical evaluation and used by the doctor in day-to-day affected person care. Before an ethical analysis can be carried out, one should first have underlying values and the proper perspective. John Gregory (1724�1773) was instrumental in advancing the concept of medical ethics through his invention of "professionalism," which changed the main focus of medical ethics from being physician-based to patient-based. He described virtues that a doctor should exhibit to provide moral care of patients. Self-effacement: putting apart and never acting on irrelevant variations between oneself and the patient. Therefore, an moral evaluation must be accomplished with compassion, integrity, and devoid of any bias or prejudice. The necessary moral ideas and ideas which are used to perform an moral evaluation are mentioned beneath. Principle of Respect for Patient Autonomy Patient autonomy is doubtless considered one of the strongest and prevailing ethical ideas. The Principle of Double Effect the principle of double impact is in essence a compromise of two different necessary moral principles: beneficence and nonmaleficence. This precept refers to the ultimate goal of any treatment, which is to do something good for the affected person. Principle of Distributive Justice/Public Stewardship the precept of justice mandates fair and equitable treatment for all. Therefore, there ought to be no prejudice within the administration of therapy to the populace and equal entry for all. Paternalism Paternalism refers to the action of a physician who in an authoritative and directive fashion influences the decision-making process. Standard of Care When analyzing any remedy, you will want to determine whether or not this treatment falls inside the standard of take care of the neighborhood. This might hold special importance if this treatment has by no means been offered-a scenario where more important evaluation of all potential outcomes should be mentioned earlier than the therapy is offered. Impact on the Community While any therapy could additionally be ethically sound, it is necessary to step again and assess the influence of its potential effect on the group. For occasion, after cautious evaluation and deliberation, it might be decided that gender choice is ethical. However, if group members are uncomfortable with this process, then there ought to be reconsideration whether to supply gender choice in any respect or solely offer it under certain conditions. The pursuit of human cloning by a small group of scientists a number of years ago drew worldwide attention. There was public outcry that cloning crosses moral boundaries and some countries enacted laws in opposition to this follow. Case Presentations Case 1 A 35-year-old G0 P0 feminine presents with a historical past of infertility. Prenatal genetic testing was again discussed however the patient was uncertain if she could undergo a termination of the pregnancy. At this level, it was concluded that the couple had been adequately knowledgeable and treatment was offered. This case highlights the necessary ethical principle of respect for patient autonomy which is founded on informed consent. While it might have been the right choice to offer remedy in this case, if the female and male had been carriers of a more severe or fatal disease. Case 2 A 40-year-old G1 P0010 woman presents with a five-year history of unexplained infertility. She was recognized with cerebral palsy at delivery and is a paraplegic confined to a wheelchair. At one other center, she underwent therapy with clomiphene citrate plus intrauterine inseminations, which had been unsuccessful. Because of her medical state, she was sent to a high-risk obstetrician for counseling about the dangers and problems related to a future pregnancy. There was added concern that the therapy might end in a a number of pregnancy that could further heighten any risks. During the workup, a hysterosalpingogram confirmed the presence of multiple filling defects in the uterine cavity. The Cystic fibrosis is amongst the most commonly inherited ailments within the Caucasian population.
Purchase rumalaya gel 30 gr on-line
Strength and orientation of the applied magnetic area are varied to encode completely different part shifts for flowing pro tons relative to stationary protons muscle relaxant herbs generic 30 gr rumalaya gel with amex. The faster the spins are moving quinine muscle relaxant mechanism 30 gr rumalaya gel discount amex, the greater their part shift, and protons of flowing blood may be discriminated from stationary protons. Pairs of photographs are acquired which have totally different sensitivities to flow and are then subtracted to cancel background signal, leaving solely the signal from flowing blood. Phase shift is proportional to velocity, permitting move quantification with this modality. Phasecontrast acquisitions could additionally be acquired in two or three dimensions; though used rarely in angiography right now, Phasecontrast provides a reliable method to quantify quantity and course of circulate. It requires long imaging occasions: two knowledge sets in every direction are acquired through the use of flowencoding gradients of opposite polarity, and as a lot as three measurements within the orthogonal planes are wanted to picture circulate in all instructions. Acquisition times can be lengthy and stop imaging within the time span of a single breathhold. Some of the restrictions are caused by flowrelated artifacts corresponding to inplane saturation and phase dispersion. Overgrading of stenotic lesions is most commonly a manifestation of signal loss within the areas of complicated flow. Complex turbulent circulate patterns in areas of stenoses can create signal loss and mimic a important lesion. In the smallest volume element, a "voxel" of the image, this distribution of phases can outcome in cancellation quite than coherent addition of indicators, accounting for the presence of signal voids at the site of stenosis. Phase dispersion is additional decreased when voxel size is minimized utilizing thin sections. The biggest disadvantage of the thick volumes used with 3D techniques is that sluggish or recir culating circulate can turn out to be saturated. However, the need for substan tial overlap of adjacent slabs increases acquisition time. Contrast transit time can be affected by low cardiac output, valvular regurgitation, giant abdom inal aneurysms, and flowlimiting stenoses. Alternatively, with automated trig thirteen gering, a pulse sequence may be designed to sense the arrival of distinction and mechanically trigger image acquisition. Magnetic resonance fluoroscopy allows the user to visualize arrival of the contrast bolus immediately on the picture and manually trigger the start of the scan. Areas that require greater spatial resolution, such as the decrease extremities, also need bigger doses of contrast for longer acquisition occasions. It is important to time the contrast bolus to obtain maximum arterial gadolinium concentration throughout acquisition of central kspace knowledge. Contrast media not solely passes in to venous constructions, depen dent on the arteriovenous transit time of the tissue, but in addition rap idly leaks out of the vascular compartment, creating vital tissue enhancement. These use either gadolinium compounds that bind to albumin, or are large sufficient to stay throughout the vascular house or ultrasmall iron particle. Another agent, gadobenate, has the next T1 rest time due to its capacity for weak and transient interplay with serum albumin. This might improve vascular signal intensity and thus enhance diagnostic efficacy at doses corresponding to these used for present gadolinium agents. It is approved for imaging use in Europe however is beneath scientific investigation in the United States. For sufferers with beneath lying persistent renal insufficiency, gadolinium chelates may cause acute renal failure. It is decided by the focus of distinction agent within the arterial system while imaging information are being col lected. Reliable photographs may be acquired no matter whether circulate is laminar, turbulent, or stagnant. This technique acquires largevolume data units in coronal or sagittal orientation within a single breathhold in the course of the first move of the distinction materials. The distinction agent, gadolinium, is a heavy metallic however becomes inert when bound to a chelator. Administration of agents shortening T1 permits selective visualization of contrastcontaining constructions and better visualization of circuitous collaterals. Digital subtraction, spoiling, and fat saturation strategies suppress back ground sign and enhance sign from the distinction agent in the vessels. Optimal images are generated when gadolinium focus is highest within the vessel of curiosity. To make blood bright in comparison with background tissues, the gadolinium bolus have to be adminis tered in a method that ensures the vast majority of the distinction to be pres ent in the arterial tree. Acquisition prior to distinction arrival creates a hundred and seventy Postprocessing Techniques Magnetic resonance data may be seen as source photographs or be displayed in projections with any orientation. Image postprocess ing allows reformation in any desired plane to enhance conspi cuity of overlapping vessels (Table 133). By performing the projections of all angles around the zaxis of the affected person, the information sets can be considered in cine. Clinical Applications Extracranial Carotid and Vertebral Arteries Atherosclerosis, dissection, and inflammatory diseases have an result on the extracranial carotid and vertebral arteries. Phasecontrast sequences can supple ment anatomical data for flow path or quantification. Transcranial circulate has a rapid arteriovenous transit time, and thus venous contamination can restrict picture quality; due to this fact, time resolved imaging could also be required. Cine pictures of the proximal aorta can establish aortic regurgitation complicating kind A dissection. Delayed part pictures enable identifica tion of intramural hematoma, ulceration, and complications includ ing rupture. Magnetic resonance angiography can reveal the situation and dimension of an aneurysm, presence of a mural throm bus, and the connection of the aneurysm to the department vessels. Aortic coarctation appears as a discrete narrowing of the aorta distal to the left sub clavian artery. Magnetic resonance angiography depicts the stenosis, tortuosity of the aorta, and associated collateral ves sels. Magnetic resonance angiography is used after intervention to exclude issues similar to stenosis or aneurysm formation. Pseudocoarctation is a uncommon asymptomatic anomaly in the descending thoracic aorta and is characterised by an elongated redundant thoracic aorta with buckling distal to the origin of the left subclavian artery. It is thought to be a benign condition, though several reports reveal that problems could happen. Symptoms are typically from nerve compres sion; the brachial plexus is concerned in as much as 98% of cases. Magnetic resonance imaging can show obstruction/compression of the fats surrounding the brachial plexus, and of the subclavian vein and artery. Magnetic resonance angiography is performed throughout abduction and adduction maneuvers of the arm to simulate physiological compres sion of the veins and/or arteries to affirm the analysis. Pulmonary Vessels Radiofrequency ablation for atrial fibrillation has increased the function of noninvasive pulmonary vein mapping before intervention and for postprocedural surveillance for issues.
Rumalaya gel 30 gr generic with amex
It was stopped after 189 sufferers were entered as the results of the North American and European trials were reported gas spasms in stomach rumalaya gel 30 gr buy amex. Patients with expanding hematomas should return to the operating room for evacuation and restitution of hemostasis muscle relaxant pregnancy category purchase 30 gr rumalaya gel with mastercard. Judicious use of heparin, notably if the affected person is on a couple of antiplatelet agent, is essential. Carotid Endarterectomy Compared to Carotid Angioplasty/Stenting Carotid artery angiography and stenting is described intimately in Chapter 32. These differences endured for 1 year, however by 4 years, there was no distinction between the two teams concerning eventfree survival. The research patients have been adopted for 4 years, at which era the death and stroke charges have been 6. It involved 50 academic centers in the United Kingdom, Europe, Australia, New Zealand, and Canada. Between the years 2000 and 2008, 2502 sufferers have been randomized; 47% had been asymptomatic, and 53% had been symptomatic. The initial evaluation occurred after the last group of sufferers had no much less than 1 12 months of followup, and median comply with up was 2. Hunt J: the function of the carotid arteries in the causation of vascular lesions of the mind, with remarks on sure special features of symptomatology, Am J Med Sci 147:704�713, 1914. Carrea R, Molins M, Murphy G: Surgical treatment of spontaneous thrombosis of the interior carotid artery in the neck: carotid-carotidal anastomosis. An index of tolerance to momentary carotid occlusion, Arch Surg 106:521�523, 1973. Halliday A, Mansfield A, Marro J, et al: Prevention of disabling and deadly strokes by successful carotid endarterectomy in patients without current neurological symptoms: randomised managed trial, Lancet 363:1491�1502, 2004. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery, Circulation 124:e54�e130, 2011. North American Symptomatic Carotid Endarterectomy Trial Collaborators: Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis, N Engl J Med 325:445�453, 1991. Gowers W: On a case of simultaneous embolism of central retinal and center cerebral arteries, Lancet 2:794, 1875. The phrases speaking and noncommunicating check with the presence or absence, respectively, of blood circulate between the true and false lumens of the aorta. Aortic dissection is acute if presentation occurs inside 14 days of the onset of symptoms and persistent if greater than 2 weeks have elapsed. In practice, diagnosis of aortic dissection is dependent upon demonstration with imaging of an intimal flap with separation of true and false lumens. In sort A dissection, the true lumen is often displaced along the inside curvature of the aortic arch and continues caudally along the medial side of the descending thoracic aorta. Aortic department vessel blood circulate might derive from both the true or false lumen; alternatively, move could also be sluggish or absent throughout the false lumen, or branch vessels could additionally be completely occluded at or close to their origins. Acute aortic dissection is an unusual but life-threatening emergency that requires immediate prognosis, rapid triage, and quick medical, endovascular, or surgical therapy. A unified effort across several worldwide facilities over the previous 15 years has led to the establishment of an in depth registry that describes major aspects of presentation, management, and outcomes of sufferers with acute aortic dissection. Although features have been made in the supply of life-saving care to patients with acute aortic dissection, hospital mortality charges stay distressingly excessive. Enhanced awareness of danger factors for aortic dissection, presentation features, diagnostic pathways, and medical, endovascular, and surgical therapy strategies is a critical first step towards bettering outcomes. Analysis of the Swedish National Cause of Death Register between 1987 and 2002 estimated the incidence of thoracic aortic aneurysm or dissection to be sixteen. In traditional acute aortic dissection, the initiating occasion is an intimal tear by way of which blood quickly surges distally in to the media underneath systolic strain, splitting the layers of the aortic wall and creating an intimal flap that separates the true from the false lumen. Classification Classifying aortic dissection in accordance with anatomical location and time from onset of symptoms helps stratify risk and guide selection of initial therapy strategy. The Stanford classification system designates dissections that contain the aorta proximal to the brachiocephalic artery. In the older DeBakey classification scheme, a type I dissection originates within the ascending aorta and extends for a variable distance beyond the take-off the innominate artery. It is most frequently positioned a number of centimeters above the extent of the aortic valve along the higher curvature of the aorta in circumstances of type A dissection and accounts for nearly 60% of all circumstances. Compared with different locations in the ascending aorta, the proximal few centimeters of the greater curvature are uncovered to relatively higher hemodynamic, shear, and torsional force. By this mechanism, as many as 20% of dissections that originate in the distal arch or descending thoracic aorta could involve the ascending aorta. Blood inside the false lumen could reenter the true lumen anywhere along the size of the dissection. Reentry may be protective because of spontaneous decompression of the false lumen that will reduce the risks of rupture and/or growth of malperfusion syndromes. Acquired Aortic Rupture and End-Organ Malperfusion Aortic rupture, defined as tearing within the vessel wall that leads to extravascular hemorrhage, most commonly occurs with trauma. Dissection-mediated end-organ ischemia or infarction happens from (1) mechanical compression of aortic department vessels by false lumen hematoma, (2) extension of the dissection plane throughout the ostium of the department vessel, or (3) dynamic vessel inlet obstruction attributable to an oscillating intimal flap. The abdominal aorta is the least widespread website for entry (3% of cases), regardless of the excessive prevalence of intima media ulcers in sufferers with atherosclerotic illness on this section. A, Computed tomographic picture demonstrates three-channel descending aortic dissection in Marfan syndrome affected person. B, Schematic representation of dissection is provided: region 1 represents thrombosed false lumen, area 2 is true lumen considerably diminished in size, and region three designates contrast-enhanced false lumen. False Lumen Thrombosis Thrombosis of blood inside the false lumen might seal the entry tear, thus eliminating communication with the true lumen and interruption of false lumen enlargement. Partial thrombosis of the false lumen, however, has been recognized as a danger factor for long-term death in patients with sort B dissection. Alternatively, it has been proposed that partial thrombosis of the false lumen is associated with worse clinical outcomes by promoting vascular irritation, hypoxia, and/or neovascularization with weakening of adjacent vascular constructions and an increased threat for aortic rupture. A, Hematoxylin and eosin microscopic part of aorta reveals fragmentation and lack of elastin fibers with cyst-like buildings present inside media. This phenotype is felt to be associated with aortic wall weakening and elevated predisposition to dissection. Deceleration injury from high-speed accidents results in aortic transection with false aneurysm formation and rupture, mostly in the area of the aortic isthmus just beyond the origin of the left subclavian artery. In many instances, pregnancy unmasks main circumstances that predispose to aortic dissection. Decreased aortic compliance and vulnerability to pulsatile forces predispose to harm and create a substrate for dissection. Drug Use and Other Acquired Conditions Recent cocaine use, significantly amongst younger men who smoke tobacco, is an extra danger factor for aortic dissection.
30 gr rumalaya gel buy
In most patients and nearly all sufferers operated on for aortic aneurysmal disease muscle relaxant 800 mg cheap rumalaya gel 30 gr fast delivery, graft excision without revascularization may be anticipated to lead to lower-extremity amputation muscle relaxant johnny english generic rumalaya gel 30 gr online. Total Graft Excision with In Situ Replacement Using Prosthetic Graft In situ replacement of an infected graft with a model new prosthetic graft is technically the only method of revascularization and avoids the potential for aortic stump blowout. However, changing an infected prosthetic graft with a new prosthesis poses the very real potential for recurrent graft an infection. In situ prosthetic replacement may be finest used as a salvage operation for unstable sufferers with either aortoenteric fistula or ruptured proximal pseudoaneurysms. Fortunately, the reported charges of clinically apparent reinfection following in situ substitute for aortoenteric fistula is surprisingly low (<15%). Recurrent infection in the setting of gross graft an infection has been disappointing. The authors use in situ substitute with prostheses as a bridge to definitive remedy with autogenous alternative at a later operation. The introduction of antibiotic-bonded Dacron grafts appeared to offer improved results for in situ prosthetic substitute. This modality seems to be most acceptable for remedy of graft infections with biofilm-producing S. Similar findings have recently been reported using silver-coated polyester grafts for in situ alternative. In a sequence of 24 patients with a selection of polymicrobial graft infections, Batt et al. In our expertise, subtotal graft excision may be attempted if the physique of the graft is found to be integrated at the time of surgical exploration. The body of the graft could be explored prior to violating the clearly infected portion. The wound is closed, the contaminated portion of the graft is removed, and the reconstruction accomplished. Subtotal graft excision should only be considered in high-risk sufferers with late-occurring graft infections. Such patients should be adopted closely, and infection of the residual graft ought to be anticipated. Animal research have demonstrated the allograft is comparatively immune to infection when antibiotic loaded. In three patients, allograft side branch rupture resulted in three aortoenteric fistulas that have been uniformly deadly. In a latest study of 110 consecutive patients with aortic infections, Bisdas et al. During a imply follow-up of 36 months, 6% required reoperation for graft deterioration, but no recurrence of an infection was famous. Graft Infection Following Endovascular Repair Graft infection following stent graft repair of aneurysm is changing into more incessantly reported. As of 2010, there have been 102 stories of stomach endograft infections within the literature. Infected grafts have been related to highly virulent organisms together with Propionobacterium, Staphylococcus, Streptococcus, and Enterobacter. On the other hand, remedy of contaminated thoracic endografts ought to embody graft excision and bypass with antibiotic-soaked prosthetic graft or cryopreserved allograft if extra virulent organisms are current. This conduit has proven to be the most resistant conduit to infection, has unchallenged patency rates, avoids the danger of aortic stump blowout, and infrequently degenerates. Patients with overwhelming sepsis may be higher served by extra-anatomical bypass and graft excision. The solely downside to this administration strategy is the length of the operative process. Treatment of Peripheral Graft Infections the incidence of graft an infection following infrainguinal peripheral arterial reconstruction ranges from 2%-5%. Late infections of autogenous grafts are very uncommon and most regularly happen in thrombosed grafts. In a sequence of 68 sufferers with contaminated infrainguinal autogenous grafts, Treiman et al. A patient presenting with bleeding from the location of an infrainguinal arterial reconstruction should be thought of to have a graft infection, and operative exploration is necessary. In less apparent cases, the prognosis of such infections is much like that of aortic graft infections. Computed tomography scanning is most helpful, and can show perigraft fluid collections and inflammation. Magnetic resonance imaging can successfully diagnose contaminated prosthetic grafts which have surrounding perigraft fluid. The grafts are simply accessible, and ultrasound is particularly good at identifying perigraft fluid. The mainstay of therapy is arterial reconstruction through uninfected fields and graft removing. However, sufferers who have been operated on for limb-threatening ischemia who endure graft excision can be anticipated to need revascularization or face inevitable amputation. In sufferers who would require concurrent revascularization at the time of contaminated graft excision, the administration choices are different for prosthetic grafts versus autogenous graft. In nearly all instances of prosthetic graft infection, the entire graft is concerned within the infectious process. This requires whole graft excision with revascularization via uninfected tissues. Careful planning and ingenious tunneling are required if cross-contamination is to be avoided. If the graft originates from the femoral artery, the profunda femoris artery, approached lateral to the sartorius muscle, can be utilized as the positioning of the proximal anastomosis. If the profunda femoris artery is diseased, the iliac vessels can be used, and the graft can be tunneled via the obturator foramen in to the thigh. The recipient artery or run off artery must be one stage below the infective course of. If the popliteal artery above the knee is involved in the infective course of, the model new runoff vessel should be the below-the-knee popliteal artery or the tibial vessels. More distal reconstruction to uninvolved tibial vessels shall be required if the contaminated graft terminates at the popliteal vessel beneath the knee or more distal. Often the graft will have to be tunneled via the lateral thigh to keep away from the previously violated medial thigh. The below-the-knee popliteal artery, peroneal artery, and the anterior tibial artery can all be approached by way of lateral leg incisions. After reestablishing circulate and closing the wounds, the prosthetic graft is excised by way of a separate incision. If potential, the entire graft must be excised with autogenous patching of the donor and recipient arteries to keep away from late issues from infected graft remnants.
Macrotys (Black Cohosh). Rumalaya gel.
- What other names is Black Cohosh known by?
- Is Black Cohosh effective?
- Dosing considerations for Black Cohosh.
- Menopausal symptoms such as hot flashes.
- How does Black Cohosh work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96830
Rumalaya gel 30 gr buy with amex
Absent an appreciation for the cardinal options of dissection spasms vs spasticity 30 gr rumalaya gel order overnight delivery, the diagnosis may be missed in a substantial variety of sufferers spasms and cramps buy rumalaya gel 30 gr online. Simple medical prediction rules have been developed to estimate probability of acute aortic dissection. These markers, assessed at bedside, were divided in to three distinct classes: predisposing components, traits of the pain at time of presentation, and key bodily examination findings. Visceral discomfort or limb pain may be indicative of aortic branch vessel ischemia from malperfusion. Syncope is a particularly ominous presenting symptom and should replicate cardiac tamponade from intrapericardial aortic rupture, cerebral malperfusion, and/or neurally mediated hypotension in response to the intense ache of the dissection. For example, paraplegia might develop when important impairment of flow to the anterior spinal artery, thoracic intercostals, or the artery of Adamkiewicz occurs. A retrospective evaluation of the International Registry of Acute Aortic Dissection decided that amongst 2538 patients with acute aortic dissection, ninety five. Hypertension is current in more than two thirds of kind B dissection patients and in roughly one third of type A sufferers. Additional auscultatory findings include a delicate first heart sound and a grade 1 or 2 midsystolic murmur at the base or alongside the left sternal border. An inverse correlation between the presence of pulse deficits and mortality is noticed in acute aortic dissection. Thus, invasive intraarterial monitoring may be essential in aortic dissection sufferers. Elevation of jugular venous stress, particularly with pulsus paradoxus, may indicate pericardial involvement with tamponade. Superior vena cava syndrome can rarely happen with compression by an expanding false aneurysm along the larger curvature of the ascending aorta. Sensitivity and specificity of these three noninvasive techniques are basically equal and exceed 90% in most sequence. Regardless of the diag- 34 nostic sequence employed, an institutional commitment to rapid imaging of critically unwell sufferers is critical. Essential options to be defined for both remedy and prognosis include presence or absence of ascending aortic involvement, entry and reentry sites, pericardial and aortic valve involvement, extent of the dissection, major department vessel compromise, and the anatomical substrate for potential malperfusion syndrome(s). Oropharyngeal anesthesia and aware sedation are required, with simultaneous monitoring of heart rate and rhythm, blood pressure, and oxygen saturation. In most circumstances, the true lumen is differentiated from the false lumen by observing systolic expansion and diastolic collapse, absence or minimal spontaneous echo contrast, and/or an antegrade Doppler sign. In one examine of ninety five sufferers with acute aortic dissection, elevated levels of circulating clean muscle myosin heavy chain protein (>2. Consistent with these knowledge, findings from one massive meta-analysis of 734 sufferers demonstrated that an elevated D-dimer degree had a 97% sensitivity and 96% adverse predictive worth for identifying acute aortic dissection. Conversely, an elevated D-dimer is less effective at "ruling-in" aortic dissection, with a specificity of 56% and constructive predictive worth of 60%. Associated findings could embody cardiomegaly (pericardial effusion) and pleural effusion (left > right). Effusions that occupy greater than 50% of the chest cavity may be indicative of rupture with hemothorax. Additional findings include displacement of intimal calcium, delayed contrast enhancement of the false lumen, and aortic widening. Branch vessel involvement anywhere along the course of the aorta to the level of the iliac arteries may be exactly displayed. Motion artifact, mural thrombi, and picture artifacts may negatively have an result on study accuracy. B, 3D reconstruction imaging in identical affected person supplies enhanced spatial resolution after surgical repair of aortic dissection and surrounding anatomical structures. Intravascular ultrasound is infrequently used as a second imaging technique for diagnosis in patients for whom false-negative outcomes on invasive aortography are suspected, and femoral entry has been obtained. Intravascular ultrasound may also have a role during performance of endovascular procedures. Systematic preoperative coronary angiography for hemodynamically stable persistent sort A dissection sufferers is a subject of debate. Identification of high-grade atherosclerotic disease of native coronary arteries and/or coronary artery bypass graft(s) affords dedication of the optimum operation for patients requiring ascending aortic surgery. However, in these cases, the potential for incorporating additional surgical procedures past repairing the dissection must be evaluated on a case-by-case foundation. Surgery or endovascular stent grafting when possible could be undertaken for failed medical therapy, pseudoaneurysm, or rupture. Differential Diagnosis Other Acute Aortic Syndromes Aortic transection from deceleration harm and traumatic aortic valve disruption with acute extreme aortic regurgitation happen within the setting of high-speed vehicular accidents or vertical falls. The nontraumatic acute aortic syndromes, nonetheless, are often not distinguishable from classic dissection on medical grounds alone, but rather are delineated with cross-sectional imaging. Predicting evolution to dissection, rupture, aneurysm formation, or false aneurysm improvement is tough. Imaging research in the former illness states could reveal wall thickening and periaortic stranding or hematoma, as nicely as a measurable enhance in aortic dimensions when compared with out there past research. Rapid expansion of the Marfan aorta occurs for causes not related to irritation, however when present could also be much more worrisome. Esmolol Propranolol 1 (9 min) 1 2 (5-7 h) Initial Medical Treatment Patients with acute aortic syndromes ought to be treated with intravenous medicines to lower the arterial blood stress as expeditiously as attainable. In sufferers with a contraindication or intolerance to -adrenergic receptor antagonists, a coronary heart rate� slowing nondihydropyridine calcium channel blocker, corresponding to diltiazem or verapamil, may be an efficient substitute. Target systolic blood strain and heart rate are a hundred and ten mmHg and 60 beats/min or less, respectively, but medications could require titration based on medical evidence of impaired end-organ perfusion. In Step 1, a low index of scientific suspicion for acute aortic dissection ought to prompt early diagnostic testing whereas medical remedy is initiated. Step 2 involves willpower of ascending aortic involvement, which considerably influences importance of emergent surgical consultation. In Step three, sufferers with kind A aortic dissection are referred for surgical procedure, and patients with sophisticated kind B aortic dissection are referred for endovascular remedy or surgical procedure. Patients with uncomplicated kind B aortic dissection are continued on medical therapy and monitored for changes in medical standing. In Step four, a care plan is established that emphasizes significance of long-term medical remedy, radiological surveillance, and lifestyle modifications to decrease risk of postdissection complications. The starting dose is 25 g/min by continuous infusion, and adjustments are normally made in increments of 10 to 25 g. Alternative intravenous vasodilators obtainable to be used within the acute setting include enalaprilat, hydralazine, and nicardipine. For acute aortic dissection sufferers with hypotension, cardiogenic shock from hemopericardium must be thought-about.
Rumalaya gel 30 gr order line
Owing to the young common age of the affected person inhabitants muscle relaxant equipment order 30 gr rumalaya gel overnight delivery, there were few deaths or major macrovascular occasions in either therapy group spasms from overdosing buy 30 gr rumalaya gel overnight delivery. Nonetheless, randomization to intensive glycemic control was associated with a nonsignificant 42% reduction in peripheral vascular and coronary occasions. At a mean follow-up of 17 years, randomization to intensive glycemic control showed a persistent 42% reduction in danger for a major cardiovascular event. Despite this finding, the significant danger reduction in microvascular events among patients initially randomized to intensive therapy continued (24% reduction). There was no vital reduction in threat of stroke or peripheral vascular outcomes. There has been nice interest in use of the insulin-sensitizing agents, metformin and the thiazolidinediones (glitazones), for prevention of cardiovascular occasions in diabetic sufferers. In distinction to the sulfonylurea arm of the examine, there was a major 42% reduction in diabetes-related mortality and a 36% reduction in all-cause mortality among patients randomized to metformin therapy in contrast with sufferers randomized to food regimen. Use of thiazolidinediones for glycemic control and prevention of cardiovascular occasions amongst diabetic patients has been an space of latest study and significant controversy. However, it is recommended that much less stringent glycemic control be considered for patients with prior historical past of extreme hypoglycemic reaction, for these with extensive micro- and macrovascular illness, and for these with restricted life expectancy. Indeed, there was a trend toward increased threat of a fatal or nonfatal cardiovascular occasion amongst individuals randomized to triple-vitamin therapy compared to placebo. Treatment of Hyperhomocysteinemia Hyperhomocysteinemia is a dysfunction associated with derangements of the metabolic pathway concerned in metabolism of the important amino acid methionine. Homocystinuria is associated with psychological retardation, ectopia lentis, and premature coronary and peripheral atherosclerosis. Among heterozygotes for cystathionine -synthase deficiency, homocysteine levels are considerably lower (on the order of 20-40 mol/L vs. Among patients randomized to vitamins, fasting plasma homocysteine levels fell from 14. Among the sufferers randomized to aggressive vitamin therapy, there was a decrease in the incidence of an irregular stress check. Although the effectiveness of supplementation with folic acid and vitamin B12 for lowering plasma homocysteine levels has been established, few information show a good factor about vitamin supplementation to stop vascular events in sufferers with hyperhomocysteinemia or established vascular disease. A latest meta-analysis of six main prevention trials of 95,000 individuals at low to average cardiovascular threat (representing 660,000 person-years) found that aspirin lowered the risk of any vascular event by 12%. This meta-analysis additionally included sixteen secondary prevention trials of 17,000 individuals at high-average threat, representing 43,000 personyears. In the secondary prevention trials, aspirin lowered serious vascular events by 29%, including complete stroke and coronary events, and was associated with a borderline nonsignificant 9% reduction in vascular mortality. The preliminary meta-analysis decided that antiplatelet remedy considerably reduced the percentages of a major vascular event amongst high-risk sufferers with atherosclerosis by 27%. It can be noteworthy that not considered one of the trials on this meta-analysis investigated the advantage of aspirin alone. Aspirin was related to a 64% reduction within the relative threat of fatal and nonfatal vascular events and a 58% reduction in fatal and nonfatal vascular occasions or critical limb ischemia. There was no statistically vital distinction in prevalence of the first composite endpoint of fatal and nonfatal coronary occasions, stroke, or revascularization between aspirin- and placebo-treated sufferers. Large multicenter randomized medical trials have investigated the use of the antiplatelet agent clopidogrel for secondary prevention of cardiovascular occasions. Clopidogrel is a thienopyridine by-product that inhibits platelet aggregation by antagonism of the adenosine zero. Aspirin for prevention of cardiovascular events in a basic population screened for a low anklebrachial index: a randomized controlled trial. There was no enhance in minor or major bleeding episodes related to clopidogrel, although there was an elevated incidence of gastrointestinal hemorrhage amongst patients randomized to aspirin. These embody several small research that explored the potential impact of oral anticoagulation on limb-related outcomes. A evaluation of three small trials discovered that oral anticoagulation remedy had no benefit on walking capability or limb-related outcomes, nor on cardiovascular outcomes amongst patients with intermittent claudication. Subset analyses, however, demonstrated a big reduction (31%) within the rate of graft occlusion of venous conduit bypass grafts, but not prosthetic grafts, amongst patients randomized to warfarin. Over a follow-up interval of 35 months, there was no important benefit of oral anticoagulation therapy in both of the two co-primary endpoints. Relative danger discount for every subgroup of sufferers is displayed with 95% confidence intervals. In a submit hoc evaluation, twin antiplatelet remedy was associated with lower charges of graft occlusion and lower-extremity amputation among patients who had prosthetic (vs. Aspirin therapy is particularly important among sufferers undergoing surgical or percutaneous revascularization procedures, and must be continued perioperatively-or initiated as soon as attainable postoperatively- if it had not been prescribed previously. Care and Protection of the Feet Careful consideration to foot care is indicated to reduce the chance of skin breakdown and an infection, and is especially necessary in diabetic individuals with vascular disease and in patients with critical limb ischemia. Well-fitted sneakers are beneficial to scale back the risk of pressure-induced necrosis. The patient is suggested to inspect the skin of the ft incessantly so minor abrasions may be addressed promptly. In sufferers with ischemia at rest, conservative measures embrace placing the affected limb in a dependent position. Sheepskin must be placed beneath the heels of the ft to forestall pores and skin breakdown at these websites. A footboard should be used to cradle the blankets over the ft in a fashion that minimizes frictional trauma. Wisps of cotton or lambswool inserted between the toes help defend the digits from intertriginous friction and moisture. Gentle heat is really helpful to reduce vasoconstriction, however extreme heat must be prevented. Tinea pedis must be treated with appropriate antimicrobial preparations to cut back the danger of cutaneous breakdown resulting in bacterial superinfection. Caution is suggested in using topical drugs due to the risk of native inflammatory reactions. Open sores should be kept clean, and deep cultures must be obtained (also see Chapter 60). A latest examine, nevertheless, did observe comparable enchancment in walking time between home-based exercise coupled with activity monitoring and supervised exercise coaching. There was no impact of exercise training on resting calf blood flow in these studies. Exercise coaching enhances endothelium-dependent vasodilation in peripheral conduit arteries, and thereby may contribute to improved blood move and strolling time in claudicants. Prior to beginning train rehabilitation, sufferers should endure a complete cardiovascular threat assessment that features a historical past, bodily examination, and ascertainment of all relevant atherosclerotic danger components. It also could serve as a baseline evaluation of the time to onset of claudication, and maximal strolling time tolerated on the treadmill. During the training session, patients ought to be inspired to walk till signs of moderate severity develop.
Rumalaya gel 30 gr order overnight delivery
In 1977 muscle relaxant ibuprofen rumalaya gel 30 gr buy generic on line, Klaus Mathias muscle relaxant renal failure 30 gr rumalaya gel generic free shipping, an interventional radiologist, described a catheter system that might be used for performing balloon angioplasty of cervical carotid stenosis,12 and this was followed by a couple of case reports of profitable carotid angioplasty performed in the surgical suite. This early report represents the primary percutaneous intervention carried out with the profit of distal embolic protection. During the Nineteen Eighties, scientific stories of carotid angioplasty were sporadic and restricted to small 386 387 In 1996, Theron et al. Unfortunately, this early-generation distal safety balloon might only be used with balloon angioplasty (and not with stents). As increasing scientific information turned available, use of distal safety units was recognized and accepted by many (but not all25) as an integral if not mandatory part of carotid artery dilation and stenting. This research also demonstrated that endovascular methods have been superior to surgical procedure when contemplating different risks related to the incision in the neck and use of general anesthesia. Major groin or neck hematomas occurred much less often after endovascular therapy than after surgery (1. The results of this early clinical trial set the stage for investigation of carotid stenting. Revascularization is typically really helpful in this group if there are additional unfavorable angiographic options. An important, albeit controversial and unsettled, concern within the remedy of symptomatic sufferers pertains to the timing of the revascularization procedure after the index symptomatic event. Argue that the best risk of a recurrent event is throughout this early interval and any delay in treatment will considerably diminish its therapeutic worth, since a substantial portion of these sufferers would have already experienced a neurological event in the course of the ready period. Guideline on the Management of Patients with Extracranial Carotid and Vertebral Artery Disease32 and essentially rely upon symptomatic standing and severity (degree) of stenosis. Amaurosis fugax refers to transient monocular visual loss, usually described by the patient as a shade being drawn down or throughout the attention (amaurosis, Greek for "darkening," and fugax, Latin for "fleeting"). Dizziness and issues with balance are signs that usually outcome from ischemia or infarction within the vertebrobasilar system, and the presence of a carotid artery stenosis in a patient presenting with dizziness is nearly at all times incidental i. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery, developed in collaboration with the American Academy of Neurology and Society of Cardiovascular Computed Tomography. Realizing the potential of carotid artery stenting: proposed paradigms for patient selection and procedural method. Treatment of sufferers with asymptomatic carotid artery stenosis has turn out to be extremely controversial, with two main points fuelling this ongoing debate42�44: 1. This discount in stroke danger has been attributed to the advantages of risk-factor modification, use of antihypertensive medicines,forty six antiplatelet brokers,47 smoking cessation, and statin remedy. Hence, at present, degree of carotid diameter stenosis severity stays the predominant basis for clinically deciding whether or not to deal with patients with asymptomatic carotid stenosis. In up to date practice, most clinicians will (should) solely deal with an angiographically confirmed 80% or greater, unilateral, by the way found. Patients with stenosis less than 60% are managed medically, with periodic (usually annual) ultrasound surveillance to monitor stenosis development. Although stenosis severity between 60% and 80% is usually managed with conservative medical treatment, this recommendation could should be altered based mostly on particular person circumstances. Some examples include: l Contralateral carotid occlusion and a stenosis between 60% and 80% within the index carotid artery that also provides the territory of occluded carotid artery by way of collaterals. This nonnegotiable low tolerance for periprocedural complications constitutes what the authors have framed as the 3% Rule of Carotid Stenting. Similarly, a affected person with compromised brain function (diminished brain reserve) is extra more probably to clinically manifest neurological events associated to periprocedural embolization. Patients with prior giant strokes, multiple small strokes, or lacunar infarcts and those with dementia are examples of patients with compromised mind reserve. Some degree of calcification is almost ubiquitous in a diseased carotid bifurcation, but heavy concentric calcification in affiliation with a severe stenosis is a serious problem. Although the demonstration of carotid calcification is simple and requires solely fluoroscopy. The high grade of stenosis, 90-degree angle between the inner carotid artery and exterior carotid artery, and proximal calcification make passage of wires and gear hazardous. Subtraction imaging with out contrast reveals calcification of both the interior carotid artery and external carotid artery. Note the comparatively full filling of the exterior carotid artery vessels in comparison. This is due to the high diploma of tortuosity of the inner carotid artery distal to the lesion, stopping safe and effective positioning of a filter gadget. We arbitrarily define heavy calcification as calcification three mm or more in width, with concentricity defined by imaging in two orthogonal views. Inability to completely dilate and increase the deployed stent regardless of using bigger and/or high-pressure balloons (resulting in a stent with an hourglass appearance) is an intraprocedural nightmare. Excessive vascular tortuosity is defined as two or more bend factors that are 90 degrees or higher. Worsening grades of tortuosity improve the problem when attempting to cross the stenosis and should make device supply difficult or impossible. Straightening of the tortuous vessel segment by stiff wires or units might lead to vessel spasm and lowered antegrade flow. Additionally, sluggish flow increases the risk of fibrin deposition throughout the filter. Iatrogenic tortuosity may also be launched by placement of the sheath in a redundant carotid artery, so tortuosity should be assessed after the sheath is in place below the carotid bifurcation. Ulceration is often famous, even on angiograms from asymptomatic sufferers, and though not a contraindication, operators ought to be aware that the danger of embolization could be greater, particularly in the course of the phase of poststent balloon dilation. Note that both calcium and thrombus may appear as filling defects, and the differentiation is based on the clinical presentation. Whereas a filling defect in a symptomatic patient ought to be presumed to be thrombus. An occluded carotid artery is an absolute contraindication Durability of Carotid Artery Stenting Durability is defined by the flexibility to reduce the danger of a future stroke (the purpose why these procedures are performed) and by the frequency of in-stent restenosis (discussed later on this chapter. This is identified by the hazy appearance and is just visible following distinction injection. A comprehensive history and physical examination, including a detailed neurological examination, are necessary first steps when evaluating a affected person for a possible carotid intervention. Often, patients referred for treatment of "symptomatic" carotid artery stenosis have other reasons for their symptoms, including posterior circulation (vertebrobasilar) illness, cardiac arrhythmias, or a cardioembolic source. A formal neurological session and additional diagnostic imaging are sometimes useful in sorting out these patients. B, Result could be seen after remedy utilizing an Emboshield (Abbott Vascular, Santa Clara, Calif. Wire is independent of filter, and negotiating the unfavorable bifurcation and extreme eccentric stenosis is far simpler with a wire uncoupled from the filter element. Note that ulcer is excluded, not obliterated, and no try ought to be made to obliterate ulcer through the use of bigger balloons. This lesion was treated using a Percusurge GuardWire (Medtronic, Minneapolis, Minn.
30 gr rumalaya gel buy with visa
Compressibility and reflux following a Valsalva maneuver are decided in these veins spasms neck purchase 30 gr rumalaya gel visa. The posterior tibial and peroneal veins are assessed for reflux using the posteromedial and anterolateral views quick spasms in lower abdomen rumalaya gel 30 gr generic online. Plethysmographic Evaluation of Venous Reflux Duplex ultrasound identifies reflux in particular person veins, and plethysmographic strategies consider the volume of venous reflux within the limb. The air chamber is filled with air to 6 mmHg and linked to a strain transducer and recorder. Changes in the volume of the leg because of emptying or filling veins produce modifications within the strain of the air chamber. Recordings are made with the affected person supine, and the leg elevated at a 45-degree angle. The patient then stands with the leg flexed slightly and bearing weight on the nonstudy leg. The time till the quantity plateaus after the raised limb is dropped is the venous filling time. Calf ejection fractions beneath 40% indicate sufferers most likely to benefit from deep vein reconstruction. Vascular Laboratory Accreditation Laboratory accreditation is obtained via organizations such because the Intersocietal Commission for the Accreditation of Vascular Laboratories ( The accreditation process reviews the tutorial credentials of the interpreting physicians and sonographers, as well as laboratory procedures. It offers glorious requirements for organising examination protocols and high quality assurance applications. Aboyans V, Criqui M, Abraham P, et al: the measurement and interpretation of the ankle brachial index, Circulation In press. Stein R, Hrilajac I, Halperin J, et al: Limitation of resting ankle brachial index in symptomatic patients with peripheral artery disease, Vasc Med eleven:29�33, 2006. Logason K, Barlin T, Jonsson M, et al: the significance of Doppler angle of insonation on differentiation between 50-69% and 70-99% carotid artery stenosis, Eur J Endovasc Surg 21:311, 2001. American Society of Echocardiography; Society for Vascular Medicine and Biology, Vasc Med 11:183�200, 2006. Hong H, Yang Y, Liu B, et al: Imaging of the abdominal aortic aneurysm: the present and the longer term, Curr Vasc Pharmacol eight:808�819, 2010. Cao P, De Rango P, Verzini F, et al: Endoleak after endovascular aortic repair: classification, diagnosis and management, J Cardiovasc Surg (Torino) fifty one:53�69, 2010. Radermacher J, Chavan A, Bleck J, et al: Use of Doppler ultrasonography to predict the result of therapy for renal-artery stenosis, N Engl J Med 344:410, 2001. Collins R, Cranny G, Burch J, et al: A systematic evaluation of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the prognosis and assessment of symptomatic, lower limb peripheral arterial disease, Health Technol Assess 11:1�184, 2007. Begelman S, Jaff M: Noninvasive diagnostic methods for peripheral arterial disease, Cleve Clin J Med seventy three:22�29, 2006. Kucher N: Clinical follow: deep vein thrombosis of the higher extremities, N Engl J Med 3:861�869, 2011. Bounameaux H, Perrier A, Righini M: Diagnosis of venous thromboembolism: an update, Vasc Med 15:399�406, 2010. Miyazaki K, Nishibe T, Kudo F, et al: Hemodynamic adjustments in stripping operation or saphenofemoral ligation of the greater saphenous vein for primary varicose veins, Ann Vasc Surg 18:465�469, 2004. Cardiovascular Disease Educational and Research Trust; European Society of Vascular Surgery; the International Angiology Scientific Activity Congress Organization; International Union of Angiology; Union Internationale de Phlebologie on the Abbaye des Vaux de Cernay, Circulation 102:E126�E163, 2000. Longitudinal and transverse magnetizations occur simultane ously but are two completely different processes that replicate properties of vari ous tissues in the physique. Since T1 measures sign restoration, tissues with brief T1 are brilliant, whereas tissues with lengthy T1 are darkish. Exogenous distinction such as gadoliniumbased brokers are routinely used to alter this sue conspicuity. Magnetic resonance echoes are digitized and stored in "kspace" composed of either two axes (for 2D imaging) or three axes (for 3D imaging). Kspace represents frequency information and is related to picture area by Fourier transformation. An essential characteristic of kspace is that tissue contrast is determined by the center of kspace (cen tral part encoding lines), whereas the periphery of the kspace encodes the image detail. The order by which kspace traces are collected could be varied, strongly influencing tissue distinction. In addition to easy linebyline kspace acquisition schemes, more complex schemes have been described. In spiral imaging, data acquisition begins on the center of kspace and spirals to the periph ery. Those alongside the yaxis will yield coronal photographs, and the xaxis gradients will present sagittal photographs. Detailed comparability with other imaging technologies is past the scope of this chapter, but common benefits and dis advantages appear in Table 131. These turn into necessary for many purposes corresponding to aortography, where multiple modalities. Magnetic resonance imaging detects the magnetic second created by single protons in omni current hydrogen atoms. Because any moving electric cost pro duces a magnetic area, spinning protons produce small magnetic fields and could be regarded as little magnets or "spins. However, a slight excess of spins aligns with the sphere, inflicting web tissue magnetization. The time required for this align ment is denoted by the longitudinal relaxation time, T1. The internet magnetization vector ideas from the longitu dinal to the transverse airplane (transverse magnetization). The pace of wobbling is dependent upon the power of the magnetic subject every proton experiences. Some protons spin quicker whereas others spin slower, they usually quickly get out of phase relative to each other. In addition to the intrinsic T2 of tissue, inhomogeneity of B0 ends in fast lack of transverse magnetization. The relaxation time that displays the sum of those random defects with tissue T2 is Magnetic Resonance Angiography Techniques Magnetic resonance imaging depends on selective imaging of transferring blood where indicators from blood vessels are maximized, whereas signals from the stationary tissues are suppressed. Algorithms then enable reformatted photographs much like those found in typical xray angiography (Table 132). The approach makes use of two consecutive inversion pulses: the first nulls or blackens the blood everywhere within the coil, and the second restores magnetization in the slice being imaged. Between these pulses and picture manufacturing, blood throughout the slice is replaced by nulled blood from exterior. This produces more reliable black blood than standard approaches, making this sequence ideal for exam ining wall thickness, dissection flaps, and the presence of mural thrombus or inflammation. A, Cross-sectional T1-weighted picture of ascending and descending aorta; lumen appears black.