
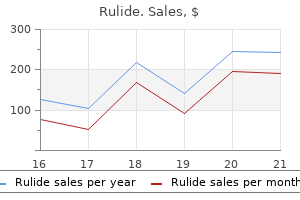
Rulide dosages: 150 mg
Rulide packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

150mg rulide order mastercard
A radiolucent sponge is placed anterior to the spine to protect the aorta in the course of the remainder of the surgical process severe withdrawal symptoms 150mg rulide discount otc. Posterior Midline Approach to the Thoracolumbar Spine the posterior midline method is probably the commonest approach used by spine surgeons in routine practice medicine 6 times a day buy 150 mg rulide. This method provides direct visualization of the spinous course of, laminae, pars interarticularis, side joints, transverse process, and pedicles. It can be used to perform diskectomy, direct decompression, osteotomies, and posterior interbody fusion and to place pedicle screws and cortical screws. Patient Position the posterior midline approach is carried out with the affected person prone on a spinal frame, with the stomach hanging freely to lower blood loss. Fluoroscopy can be used to mark the goal stage earlier than the pores and skin incision is made. The skin and subcutaneous tissue are infiltrated with 1:500,000 epinephrine, which can help in hemostasis. Surgical Steps A midline skin incision similar to the goal vertebrae is performed, and further dissection down the midline is accomplished using electrocautery to attain thoracolumbar fascia, which are incised according to the pores and skin incision. Cerebellar or Gelpi retractors are used to help maintain adequate tissue pressure during exposure. The tendinous attachments of muscles over the spinous course of are launched, followed by subperiosteal publicity of the lamina of curiosity utilizing a Cobb elevator. This procedure may be carried out unilaterally or bilaterally, depending on surgical indications. At this point in the procedure, the paraspinal muscle tissue may be held laterally with self-retaining retractors. Exposure lateral to the side joints could be completed if pedicle screws are planned or entry to the intertransverse area is desired for bone graft placement. When using standard pedicle screws, the multifidus tendons can be released from the lateral facet capsule with electrocautery. This facilitates mild retraction of the muscular tissues mendacity over the transverse processes, which could be elevated rather simply with a Cobb elevator. Care must be taken around the superior and inferior margins of the aspect because arterial perforators can be a nuisance if not acknowledged and cauterized. For pedicle screw placement via the cortical bone trajectory, the publicity solely needs to reach the lateral facet of the pars interarticularis. This spares the muscle attachments alongside the lateral side joint, which aids in achieving a minimally invasive midline dissection. After the desired process is completed, the muscle, fascia, subcutaneous tissue, and pores and skin are closed in individual layers. Advantages and Limitations Advantages of the posterior midline approach are surgeon familiarity, clear appreciation of the anatomy, and little or no threat of neurovascular damage. Limitations embody potential extreme blood loss, extensive soft-tissue injury, and extreme postoperative pain. Some authors report that L4-L5 may be approached through increased lateral flexion of the affected person, but the risk of L4 nerve injury also needs to be thought-about in preoperative planning and intraoperative execution. In addition, the diaphragmatic crus or diaphragm itself may inhibit access on this region. Transdiaphragmatic access is feasible; nevertheless, the surgeon ought to be ready to place a chest tube on this setting. The use of an adjustable table with a break positioned on the disk area of curiosity (especially at lower lumbar ranges and thoracolumbar levels) could facilitate safe access. Care ought to be taken to flex the ipsilateral hip, which can assist in mobilization of the psoas with out placing unnecessary strain on the lumbar plexus throughout retractor placement. A 3-cm incision is positioned on the left flank, and electrocautery is then used to reduce through the external oblique fascia. Blunt dissection with a finger or peanut is used to reach the retroperitoneum via the external indirect, inner indirect, and transverse abdominis muscular tissues. Branches of the subcostal iliohypogastric and ilioinguinal nerves may be encountered both running freely in the retroperitoneum or, extra generally, between the inner indirect and transversus abdominus. To reach the psoas, dorsal to ventral blunt dissection is used to move the peritoneum away from the surgical plane. Before passing via the psoas, the anterior vessels and posterior lumbar plexus are checked. To guarantee their security, the psoas must be separated between the middle and anterior third of the muscle, and the stomach contents together with peritoneum are protected by placing handheld retractors. After the psoas muscle is visualized, sequential tubular dilators are handed via the muscle to reach the disk area. A retroperitoneal approach to the lumbar backbone from L5-S1 to L1-L2 is achieved through a single pores and skin incision. For multilevel procedures, an indirect skin incision of 5 to 10 cm is created consistent with the fibers of the exterior oblique muscle alongside the lateral wall of the abdomen. Abdominal muscle tissue may be bluntly separated with minimal cautery after dividing their fascia. The peritoneum is separated from underlying retroperitoneal buildings by blunt finger dissection, and the belly contents are retracted anteriorly. The psoas muscle and the genitofemoral nerve are visualized, and the focused disk space is then approached between the left psoas and the aorta. A spinal needle or Kirschner wire is positioned in the disk house to confirm the surgical level fluoroscopically. Importantly, when approaching the L5-S1 degree, the disk is eliminated lateral to the frequent iliac vessels quite than within the bifurcation. Guidewires are inserted into the pedicles through 1- to 2-cm paramedian incisions, and cannulated pedicle screws are positioned over the guidewire. If substantial symptoms are present bilaterally, the contralateral aspect may be immediately decompressed by depressing the thecal sac anteriorly and "crossing over" to the other side and performing the decompression. Sequential soft-tissue dilators are then docked on the intervening side and expanded to a desired working diameter of roughly 24 to 28 mm. Various further retractors could be inserted over the tubular retractors to permit even higher visibility. The decompression of the lateral recess and foramen is carried out by way of the ipsilateral facet and pars interarticularis. Contralateral decompression of the spinal canal could be performed by angling the retractor blades to the opposite aspect or by inserting the retractor on the contralateral aspect and repeating this step. Pedicle screws are placed in a percutaneous fashion on the contralateral aspect to full the construct. A, With the patient in the lateral decubitus place, the pores and skin is incised in diagonal fashion just proximal to the iliac crest. Below the subcutaneous fats, the external oblique muscle is encountered and could be divided parallel to the muscle fibers (dotted line).
Buy rulide 150mg amex
The juvenile kind presents between 5-10 years medications mitral valve prolapse cheap rulide 150mg overnight delivery, usually with deteriorating school performance medications 122 rulide 150 mg cheap free shipping. Therapies such as enzyme alternative and gene remedy with oligodendroglial or neural progenitor cells are nonetheless experimental. Depending on the clinical form of disease, the imaging adjustments could also be rapidly progressive. The subcortical Ufibers and cerebellum are sometimes spared until late within the illness. Eventually, the progressive subcortical demyelination involves the subcortical U-fibers. Additional websites of late involvement embrace the corpus callosum, pyramidal tracts, and internal capsules. Regions of "burnt-out," getting older, or chronic demyelination show elevated diffusivity. Nonspecific elevation of choline and myoinositol may be seen in early and lively illness (31-6) (31-8). It was traditionally known as "bronze" Schilder disease and "melanodermic kind leukodystrophy" before its adrenal involvement was recognized. Axonal degeneration within the posterior fossa and spinal twine are also typical of the illness. The first is axonal degeneration that predominates within the posterior fossa and spinal cord, and the second is a extreme inflammatory demyelination. The innermost zone consists of a necrotic core of demyelination with astrogliosis, � Ca++. An intermediate zone of lively demyelination and perivascular inflammation lies just outdoors the necrotic, "burned out" core of the lesion. The most peripheral zone consists of ongoing demyelination with out inflammatory changes (31-12). Approximately 10% of affected patients present acutely with seizures, adrenal disaster, acute encephalopathy, or coma. There is periatrial T2 hyperintensity and diffusion restriction within the actively demyelinating, inflammatory regions. Relentless development with spastic quadriparesis, blindness, deafness, and vegetative state is typical. Dietary intake of Lorenzo oil (a combination of triolein and trierucin) has helped mitigate signs in some patients. Early bone marrow transplantation or hematopoietic stem cell gene remedy has improved scientific outcome for others. As the illness progresses, hyperintensity spreads from posterior to anterior and from the center to the periphery. The intermediate zone of lively inflammatory demyelination usually enhances T1 C+. Each region is scored for the presence (1) or absence (0) of atrophy, and each subregion is assessed as regular (0), unilateral abnormality (0. Most peripheral, vanguard zone reveals ongoing demyelination without inflammatory modifications. The inside core and outer perimeter of illness show increased diffusivity (hyperintensity). Faulty galactose cleavage leads to progressive psychosine accumulation in large ("globoid") multinucleated epithelioid cells. The childish kind is the commonest, sometimes presenting between 3 and 6 months with excessive irritability and feeding difficulties. The presence of globoid and Ca++ accumulation in the thalami and basal ganglia might lead to T1 shortening or hyperintensity. Krabbe disease is certainly one of the few leukodystrophies in which cerebellar findings appear early in the disease course. Learning disabilities with insidious, protracted cognitive impairment are typical. The illness is initially periventricular however later spreads to involve the subcortical arcuate fibers. This ends in poor protein recycling and intracellular accumulation of denatured proteins. The basal ganglia, corpus callosum, anterior commissure, and internal capsules are characteristically spared. Microscopic findings embody myelin pallor, thinned myelin sheaths, vacuolation, a limited number of reactive astrocytes with atypical features, and cystic modifications. Paradoxical improve in oligodendrocytes may be seen in some areas with marked loss in others. At post-mortem, a cystic leukoencephalopathy is observed with each axons and myelin sheaths absent. Development is initially regular, however progressive motor and cognitive impairment with cerebellar and pyramidal indicators follows. Note the symmetric periventricular disease, spared U-fibers, and early cyst formation. Nonspecific signs and signs including eczema, developmental delay, seizures, and hyperactivity may herald the disease. With adherence to dietary protein restriction, mitigation of the ravages of this illness occurs. Diffusion can be current and, when followed serially, might reflect a development of illness or poor dietary control (31-23). Decreased activity of the branched chain -keto acid dehydrogenase complicated disrupts the Krebs cycle and ends in elevated mind ranges of leucine and other leukotoxic metabolites. In turn, these induce cytotoxic or intramyelinic edema and spongiform degeneration. The overall prevalence is 1:850,000 reside births with a higher frequency among Mennonites, people of Middle Eastern descent, and Ashkenazi Jews. Within days after start, poor feeding, lethargy, vomiting, seizures, and encephalopathy may occur. Margins of parenchymal hyperintensity are most likely to turn out to be sharp in the course of the subacute part of illness. Imaging abnormalities are far more conspicuous infratentorially than supratentorially. Glycine is often metabolized to the final end-products of ammonia and carbon dioxide. Hypoxic ischemic injury has a relevant well being history and characteristic striatal, thalamic, and corticospinal tract involvement. Upward dislocation of the lens develops early and affects the majority of patients. Endothelial injury and hypercoagulability result in a excessive incidence of both arterial and venous occlusions, which happen at all ages.
Syndromes
- Extreme drowsiness or sleepiness
- Spreads with a knife
- Difficulty completely straightening joints
- Bronchoscopy -- camera down the throat to see burns in the airways and lungs
- Scarring of the lung
- Wear light-colored clothing. Light colors are less attractive than dark colors to biting insects. It also makes it easier to spot ticks or insects that have landed.
- Chest pain
- Coughing up blood
- Peripheral neuropathy
Rulide 150mg cheap on-line
Establishing proof in interventional ache remedy and manual therapy is tough because of confounding variables medications ranitidine rulide 150mg generic otc. Essentially medications jokes 150mg rulide order with amex, the categorization of these patients becomes vaguer, which ends up in inconclusive proof. Similarly, every intervention have to be carried out by a clinician, who may have his or her own processes, methods, and approaches, all of which are counterproductive for achieving a profitable, repeatable investigation resulting in stage I evidence. The cheap conclusion that could be drawn from the obtainable proof is that manipulation could additionally be one of many instruments used against the vagaries of musculoskeletal axial spine complaints, and though a balanced strategy is critical, manipulation may be included as a worthwhile therapy for patients with acute and chronic neck- and backrelated problems. Manual practitioners ought to choose their methods and focus areas based on the appropriate analysis of an damage. In osteopathic medicine, the issues being handled are referred to as somatic dysfunction, which means disrupted function of the body, sometimes at the native stage. These disruptions most regularly happen in articular areas (such as facet joints), in muscular tissues, and throughout the high-tension zones of the gentle tissues. Although some practitioners use generic, universal remedy routines for all sufferers with related problems, this method is much like providing an epidural steroid injection for each affected person who stories back ache: some patients will enhance, however establishing a clear prognosis earlier than remedy is begun should end in a greater, more environment friendly, and extra economical end result. Evaluation for somatic dysfunction relies largely on asymmetry (both static and with movement) and restriction of motion. Rather, freedom of movement and full vary of motion throughout the anatomic limits is the objective; subsequently, any restriction is primarily thought-about the place to begin. In the axial spine, vertebral segments are first assessed as a bunch and then individually, considering the changing mechanics because the backbone enters lordosis, transitions to kyphosis, eases by way of impartial, after which returns to lordosis. Tissue texture adjustments also are necessary clues (particularly in soft-tissue issues and acute signs within the axial spine) and tenderness of the area additionally can be of value in making a prognosis. In delicate tissues, significantly the layers from the floor to the outer muscle layers, tissue texture modifications (the so-called lumps and bumps) typically are evidence of somatic dysfunction. The extra acute the dysfunction or damage, the more acute the findings, together with redness, local microedema, tautness, and heat. Indications for Treatment Although practitioners who primarily concentrate on manipulation probably can find some type of subacute dysfunction to deal with in almost any affected person, certain sufferers and diagnoses are extra acceptable for a handbook remedy plan. The objective of therapy for all conditions is to improve perform, and in the end, high quality of life, via remedy to relieve movement restrictions. This objective is accomplished by way of proper prognosis of areas of restriction within the neuromusculoskeletal system and by restoring optimal tissue texture, physique symmetry, and range of movement. Most spinal pain outcomes from the advanced interactions between the backbone with regular age-related degeneration and the sensitivity and responsiveness of the nervous system, which regulates the consciousness of pain. These patterns also are identified as somatic dysfunction and may affectively be improved with osteopathic manipulative remedy ensuing within the normalization of physiologic movement and decreased pain. Osteopathic manipulative remedy also ought to be considered in sufferers with ache resulting from muscle strains/sprains or myofascial pain such as in athletic injuries, whiplash injuries, and even from performing home tasks. By making use of osteopathic manipulative treatment methods to the restricted joint, muscular and/or fascial movement can be restored more effectively, facilitating a return to normal mechanics, improvement in pain, and lowered use of oral medicine. In circumstances corresponding to spinal stenosis, disk herniations, radiculopathy, or scoliosis, osteopathic manipulative therapy can alleviate continual somatic signs and doubtlessly optimize tissue mechanics to enhance again ache over time. In sure patients (specifically, patients with a historical past of cancer, acute fracture, osteomyelitis, discitis, extreme osteoporosis, or rheumatoid arthritis), manipulation must be used with caution to forestall trauma or worsening dysfunction. High velocity�low amplitude thrust strategies should be averted because of the chance of fracture. In the setting of rheumatoid arthritis, a danger of spinal twine compromise exists with cervical manipulation if the cruciform ligament has sustained injury. During osteopathic manipulative therapy, if progressive neurologic decline develops in a affected person or associated constitutional symptoms corresponding to night time pain, fever, or bowel/bladder dysfunction occur, the appropriate workup with additional diagnostic tests must be carried out to determine the correct remedy course. Technique Many classes of strategies have been developed, with some focusing on particular types of dysfunction and others offering multiple approaches for managing the identical sort of dysfunction. The osteopathic model has two major technique sorts: direct strategies that engage the restriction and oblique strategies that work away from the restrictive barrier to relieve rigidity and stress. Information concerning osteopathic rules and techniques is abundantly out there. The focused somatic dysfunction may be in the muscle belly itself, or may be an articulating joint spanned by the muscle; in either case, the restrictive barrier is engaged, most regularly by stretching the muscle to the edge of tolerable range of motion and maintaining it in a static place. The contraction is held for three to 5 seconds, and the muscle is then allowed to chill out. After a few seconds of elapse to allow complete relaxation of the muscle, the muscle is stretched further to the model new fringe of its vary of motion. This is repeated till the restriction is gone or until no further improvement is obtained. High Velocity�Low Amplitude High velocity�low amplitude strategies are the thrust strategies most individuals think of in a discussion of manipulation. This is just like cracking a stiff proximal interphalangeal joint, and must be no extra forceful or painful when applied appropriately. Some people use broad-range, high velocity�high amplitude strategies for the general therapy of a complete region, corresponding to the whole cervical or lumbar spine, with a single method. These shotgun strategies are fast and could be comparatively successful in young sufferers, but the potential exists for unintended harm, so a more targeted strategy is greatest. The cervical backbone is positioned with careful localization to a C5 somatic dysfunction. Soft-Tissue Techniques Soft-tissue methods are most appropriately in contrast with therapeutic massage both in appearance and effect. The strategies are sometimes direct (working into the restrictive barriers) but can be indirect (working with and away from the restriction) and are sometimes alternating mixtures of both. Often, a common space surrounding the particular somatic dysfunction is handled to cut back exterior tension forces on the focused somatic dysfunction. As the restrictions are launched, other methods may be applied to treat the deeper dysfunction. Counterstrain Technique Counterstrain techniques, also referred to as strain-counterstrain, is a considerably broad category that focuses on treating particular person areas of somatic dysfunction in the stomach of individual muscular tissues referred to simply as tender factors. Most commonly, patient suggestions is elicited while a position of biggest comfort is attempted and held for a varied amount of time (novices are taught to hold this position for approximately ninety seconds). The concept of this technique is to reduce as a lot rigidity as possible from the fibers surrounding the tender space to fully reset muscle fiber size to baseline levels. Facilitated Positional Release Facilitated positional release methods are much like counterstrain techniques in most ways. The area is arranged in a quantity of planes to discover a position of comfort, whether subjectively for the patient or relative to a balance point of neutral tension for the practitioner. The use of this facilitating force usually requires management of both ends of the joint, which makes this maneuver easily executable for the cervical spine, wrists, and ankles, but tougher for the lumbar spine and hips. This position creates an axial load down the cervical spine to facilitate remedy.
Rulide 150mg purchase overnight delivery
Ito M treatment vertigo purchase rulide 150 mg on-line, Sudo H symptoms blood clot leg generic rulide 150 mg line, Abumi K, et al: Minimally invasive surgical remedy for tuberculous spondylodiscitis. In this retrospective study, 128 patients who underwent early surgical procedure for spinal epidural abscesses had improved neurologic outcomes. The authors report on the outbreak of fungal infection from contaminated methylprednisolone acetate injections. Hawkins M, Bolton M: Pediatric spinal epidural abscess: A 9-year institutional review and evaluation of the literature. This retrospective examine reported on nine pediatric patients with spinal epidural abscess. This retrospective cohort study identified risk factors for sufferers to have concurrent noncontiguous spinal epidural abscess. Risk factors for failure of nonsurgical administration of spinal epidural abscesses embody diabetes in a affected person older than sixty five years, an infection with methicillin-resistant S aureus, and neurologic compromise. This literature review of 28 case series with a minimal of 30 patients every introduced an algorithm for selecting sufferers who may be safe candidates for nonsurgical administration of spinal epidural abscess. Reihsaus E, Waldbaur H, Seeling W: Spinal epidural abscess: A meta-analysis of 915 sufferers. This case cohort study in contrast mortality charges in sufferers with infectious spondylodiscitis with a reference population based on knowledge from Funen County, Denmark. This evaluation article supplies information about the latest achievements in prevention, analysis, microbiology, and therapy of postoperative spinal wound infections. Rubinstein E, Findler G, Amit P, Shaked I: Perioperative prophylactic cephazolin in spinal surgery: A double-blind placebo-controlled trial. The authors report on the local placement of vancomycin powder in surgical backbone wounds prior to fascial closing. This retrospective cohort study of all patients who underwent instrumented spine surgical procedure at a single establishment compared surgical site infections in wounds handled with vancomycin energy and people not handled with vancomycin powder. The authors concluded the native use of vancomycin powder decreased the an infection fee. The joints, bones, ligaments, tendons, and synovial tissues of the the backbone are affected by these disorders. Early medical intervention can stop illness progression, which might find yourself in spinal instability. Other spondyloarthropathies equally reply to medical management; nonetheless, fracture and deformity can develop in sufferers with advanced disease. Keywords: ankylosing spondylitis; inflammatory arthritides; rheumatoid arthritis Dr. Passias or an immediate family member serves as a paid marketing consultant to Zimmer; serves as an unpaid advisor to Medicrea; and has obtained research or institutional help from the Cervical Scoliosis Research Society. None of the following authors or any immediate member of the family has acquired something of value from or has inventory or inventory options held in a business firm or establishment related directly or indirectly to the subject of this chapter: Mr. Introduction Inflammatory arthritides are categorized individually from osteoarthritis, which is the most common form of spinal arthritis. These entities symbolize systemic autoimmune diseases that induce the physique to kind antibodies that assault a number of physique techniques, together with the backbone. Inflammatory arthritides affect joints, bones, ligaments, tendons, and synovial tissues all through the skeleton. Ankylosing spondylitis characteristically targets the sacroiliac joints and anterior longitudinal ligament. Other inflammatory arthritides embody psoriatic arthritis, reactive arthritis, gout, polymyalgia rheumatica, and enteropathic arthritis. Recognizing the features that differentiate these conditions is crucial for tailoring a treatment plan. However, surgical intervention is still incessantly indicated to handle compression of neural components, spinal instability, and spinal deformity. This disorder may current at any age, however mostly occurs between the ages of 40 and 60 years. Neurologic signs severe sufficient to require surgical session develop in solely 7% to 34% of those patients. The prevalence of involvement of the atlantoaxial spine is approximately 19% to 70%, with or with out the involvement of the craniocervical junction. A complex interaction between the adaptive and innate immune methods leads to an erosive and hypertrophic synovitis, often described as pannus. Dendritic cells, mast cells, macrophages, and neutrophils all play an necessary role. T and B cells produce cytokines and autoantibodies in response to currently unknown antigens expressed on synovial cells. T cell� and B cell�associated phosphoinositide-3-kinases delta and gamma recruit neutrophils and mast cells. Synovial cells release procollagenase, progelatinase, and different metalloproteinases, which promote destruction of the synovium, cartilage, bone, joint, and the encircling tissue. Etiology of Spine Instability Atlantoaxial instability begins with erosive pannus formation at the C1-C2 joints, bone destruction, and subsequent laxity of the transverse atlantal ligament. In sufferers with atlantoaxial instability, this worth increases and the value of the posterior atlantodental interval decreases, which will increase the risk of compression of the upper section of the cervical spinal twine. Posterior or lateral subluxation is rare, and usually occurs secondary to a rotational or a traction damage resulting in fractures of the axial spine. The cranium could settle caudally, concurrent with pannus development, and ventral brain stem compression may occur via pannus formation around the dens. Asymmetric bone loss from the occipital condyles and C1 lateral lots might contribute to a torticollis deformity. Neck ache is the most typical presentation, with delicate and progressive instability as the underlying pathophysiology. Joint arthropathy, muscle wasting, decreased vary of movement, neurologic symptoms, and altered mental status could also be present. Early recognition of cervical symptomology and intervention with treatment could spare the cervical spine and gradual illness development. In sufferers with atlantoaxial subluxation, the C2 spinous course of could turn out to be prominent with neck flexion. Asymmetric destruction of the lateral atlantoaxial joints can induce the top to be held downward with a lateral tilt. Instability might trigger secondary impingement of the higher and/or lesser occipital nerves (medial divisions of dorsal rami of C2 and C3 nerve roots, respectively), leading to occipital headaches. Patients with C1-C2 instability may report signs of vertigo, syncope, nystagmus, dysarthria, sleep apnea, swallowing issue, or facial paresthesia. The radiation of pain to the clavicles from C3-C4 or the scapulae from C5-C6 or C6-C7 is commonly described. Muscle weakness, atrophy, numbness, tingling or paresthesia, bowel or bladder incontinence, hyperreflexia, lack of proprioception, and/or gait instability might indicate myelopathy. Inflammatory markers include an elevated erythrocyte sedimentation rate, C-reactive protein level, and serum globulin degree. The C-reactive protein level has been shown to predict the chance of joint deterioration and must be monitored.
Order rulide 150 mg with visa
The craniopharyngeal canal is often obliterated by the twelfth gestational week symptoms heart attack women 150 mg rulide buy fast delivery. It is changed by the transient intersphenoidal synchondrosis medications hypothyroidism rulide 150 mg visa, which usually closes around three postnatal months. The posterior cranium base consists primarily of the occipital bone, which has four major ossification centers situated across the foramen magnum. In distinction to the anterior and central skull base segments, the posterior cranium base is almost fully ossified by birth. The petrooccipital and occipitomastoid sutures are among the many last of all of the cranial sutures to close (15-17 years). Anomalies of the Skull and Meninges (41-3) Endocranial view of the grownup skull shows the following: foramen cecum (1), crista galli (2), cribriform plate (3), planum sphenoidale (4), lesser sphenoid wing and optic canal (5), superior orbital fissure (6), endocranial openings of carotid canal (7, 12), foramen rotundum (8), foramen ovale (9), foramen spinosum (10), foramen lacerum (11), clivus (13), petrooccipital fissure (14), inside auditory canal (15), jugular foramen (16), jugular tubercle overlying hypoglossal canal (17), and the foramen magnum (18). A detailed description of cranial nerves-their origins, programs, and imaging appearances-is included in Chapter 23. The endocranial floor consists of the orbital plates of the frontal bones, the ethmoid bone with its cribriform plate and sinus roof, and the lesser sphenoid wing. In this specimen, the foramen cecum (1) persists as a small bony midline pit instantly in front of the crista galli (2). The olfactory recesses with the sieve-like cribriform plate (3) lie on either side of the crista galli. A flat bony surface, the planum sphenoidale (4), extends posteriorly from the cribriform plate of the ethmoid bone to the sella turcica. It is composed of the higher sphenoid wing, the basisphenoid, and the temporal bone anterior to the petrous ridge. A central despair, the sella turcica, is bordered anteriorly by the tuberculum sellae and anterior clinoid processes. The posterior border of the sella is fashioned by the dorsum sellae, a prominent bony projection that lies anteromedial to the petrous apices. The middle meningeal artery enters the cranial cavity through the foramen spinosum. Congenital Malformations of the Skull and Brain 1298 (41-4) (Top) Autopsy exhibits occipital cephalocele, mind with pachy-/polymicrogyria. The foramen lacerum (11) is an irregular cartilage-filled aperture that lies between the sphenoid bone and petrous apex. The internal carotid arteries exit the petrous temporal bone at the endocranial carotid canal (12). The dorsum sellae continues posteroinferiorly as the upper a part of a easy concavity, the clivus (13). An atretic cephalocele is a small defect that incorporates just dura, fibrous tissue, and degenerated mind tissue. Atretic cephaloceles mostly occur on the obelion (along the sagittal suture on a level with the parietal foramina). They are typically classified by location and are named based on the roof and flooring of the bone(s) by way of which they herniate. Most congenital cephaloceles have coexisting intracranial abnormalities of various severity. Cephalocele prevalence and type differ considerably with geographic location and ethnicity. Cephalocele imaging has 4 goals: (1) depict the osseous defect, (2) delineate the sac and define its contents, (3) map the course of adjacent arteries and determine the integrity of the dural venous sinuses, and (4) identify any coexisting anomalies. This helps scale back both false optimistic and false adverse examinations during a time of active ossification. We now discuss four of the commonest forms of cephalocele: occipital, frontoethmoidal, parietal, and cranium base cephaloceles. The petrooccipital fissure (14) lies between the petrous apex and the occipital bone. Cephaloceles "Cephalocele" is a generic term for the protrusion of intracranial contents through a calvarial or skull base defect. If the Anomalies of the Skull and Meninges 1299 (41-6) Graphic depicts frontonasal cephalocele with mind herniating by way of a patent fonticulus frontalis between the frontal bone above and nasal bone under. Occipital Cephaloceles Terminology and Classification Three subtypes of occipital cephalocele are acknowledged and identified based on the concerned bone(s). In addition to delineating the sac and its contents, figuring out the course and integrity of the dural venous sinuses is crucial for preoperative planning. At least half of all sufferers with occipital cephaloceles have associated abnormalities such as callosal dysgenesis, cerebellar malformations (including Chiari 2 and DandyWalker spectrum disorders), and grey matter heterotopias. Clinical Issues Occipital cephaloceles account for 75% of cephaloceles in European and North American Caucasians. Occipital cephaloceles are nearly all the time recognized at start as a variably sized occipital or suboccipital delicate tissue mass. The affected toddler is often microcephalic with seen craniofacial disproportion. Neurodevelopmental end result is expounded to cephalocele dimension and contents as properly as the presence and type of associated abnormalities. Frontoethmoidal Cephaloceles Terminology and Classification Frontoethmoidal cephaloceles are also referred to as sincipital cephaloceles. In frontoethmoidal cephaloceles, mind parenchyma herniates by way of a persisting dural projection into the midface, usually the forehead, dorsum of the nose, or orbit. The frontonasal subtype is most typical, representing 4060% of frontoethmoidal cephaloceles. In the nasoethmoidal subtype (30%), the sac herniates via a midline foramen cecum defect into the prenasal house. Here the cephalocele herniates by way of the maxilla and lacrimal bone into the inferomedial orbit. The herniated brain-which can derive from both supra- and infratentorial structures-is always irregular, showing dysmorphic, disorganized, and dysplastic (41-5). Depending on the size of the cephalocele, severe traction and distortion of the brainstem and supratentorial buildings may be present. Congenital Malformations of the Skull and Brain 1300 Etiology Frontonasal cephaloceles protrude via an unobliterated fonticulus frontalis into the anterior forehead at the glabella/dorsum of nostril (41-6). Nasoethmoidal cephaloceles herniate into the nasal cavity via a patent foramen cecum (41-7). Developmental defects within the lacrimal bones and frontal processes of the maxillary bones lead to a nasoorbital cephalocele, which herniates into the orbit. Associated abnormalities are current in 80% of sufferers with frontoethmoidal cephaloceles. These embody hypertelorism and eye anomalies, corpus callosum dysgenesis, interhemispheric lipomas, hydrocephalus, seizures, neuronal migration anomalies, and microcephaly. In a frontonasal cephalocele, brain herniates into the brow between the frontal bones above and the nasal bones beneath (41-8).
Rulide 150mg amex
Transdisciplinary Care for Cervical Spine Disorders Implicit in transdisciplinary care is an understanding that the needs of sufferers exceed the data schedule 6 medications discount 150 mg rulide, coaching 4 medications list 150mg rulide overnight delivery, and abilities of any single provider. Committing to this course of could be uncomfortable to those cultured within the biomedical hierarchy of command and management biomedical administration. The transdisciplinary care model requires dynamic interaction among quite lots of disciplines, thus enabling the exchange of data, knowledge, expertise, and clinical skills essential to team-based downside fixing. This strategy is gaining traction in different healthcare milieus such as oncology and nursing. Although more research regarding its implementation are wanted, transdisciplinary care has been shown to contribute to each clinician satisfaction and a favorable affected person expertise in a biopsychosocial practical restoration program. At the same time, nevertheless, a transdisciplinary milieu is self-policing by way of interprovider accountability. Importantly, this requires clear prospective group agreement regarding the generally difficult process of conflict resolution. For example, sufferers might freely make feedback to nonprovider workers members that could prove crucial in ways that exceed the traditional boundaries of patient-provider interplay. A systemic method acknowledges the perceptions and enter of all individuals concerned in the strategy of scientific care, including administrative personnel such as receptionists and schedulers. Foundations of a Transdisciplinary Team the concept of transdisciplinarity has received considerable attention outdoors the realm of backbone care. It is noted that "the multidisciplinary model involves vertical communication from supervisor to subordinates, with every member contributing an assessment after making use of a discipline-specific skillset (with) little discussion between team members (that) the interdisciplinary mannequin acknowledges the overlap in data of (team) members and facilitates horizontal communication at many factors in the (evaluation and care process) and that the transdisciplinary mannequin of care takes collaboration to a still larger stage, incorporating ongoing cross-disciplinary training (and) regulated overlapping roles. Viable transdisciplinary teams require healthcare suppliers to work throughout historic boundaries and processes; with out doing so, care coordination will finally degrade. Without leadership devoted to these ideas, individual or discipline-specific agendas will invariably undermine an built-in care milieu. Transdisciplinarity in Biopsychosocial Care the training of medical students within the biopsychosocial care mannequin has lagged considerably behind that of biomedical interventions. Psychosocial elements are important to the affected person experience and could be addressed at nearly every degree of affected person interaction. When repeated throughout a number of patient-provider interactions through transdisciplinary group care, the impact of such advice is compounded and powerfully supports energetic care methods. Depression, anxiousness, catastrophizing, fear-avoidance behaviors, and different psychosocial stressors have a well-established correlation with axial ache and the progression to chronic pain and incapacity. Early threat recognition and psychosocial interventions are facilitated in an environment of cross-trained suppliers. Routine clinical interventions corresponding to addressing fear-avoidance behaviors throughout exercise and stability training, discussing emotional distress at medical reassessments, or talking about passive treatment dependency during chiropractic follow-ups can complement structured psychological health care. The Benefits of Transdisciplinary Triage and Care Access Accreditation and reimbursement are more and more tied to entry and affected person satisfaction. More than any single discipline, transdisciplinary care teams have larger flexibility to meet the preferences and medical wants of sufferers with neck problems. Purpose is a transparent statement that defines and binds the neighborhood in worthy pursuit. Principles are clear, commonly understood statements reflecting how participants conduct themselves in pursuit of purpose. Participants are the group that defines just, equitable, and efficient relationships that all can trust to achieve purpose in accordance with ideas. Organizing ideas are activities and course of trusted as equitable, effective, and in accordance with organizational objective and ideas. The constitution is the codification of participant rights, obligations, and relationships that forms an organizational entity. A small share of sufferers with acute or first-episode cervical spine disorders are prone to expertise chronicity; therefore, early identification of danger elements is critical. In a transdisciplinary mannequin, screening for prospective incapacity risks facilitates broader care coordination with employers and other stakeholders. Potentially severe pathology, including purple flags, psychosocial yellow flags, and patient preferences, normally can be identified initially through a skilled phone interview (conducted by a registered nurse or equal professional) and/or other preclinical mechanism. For patients with advanced issues (for example, severe comorbid health standing, third-party liability claims, debilitating pain with present work absence), preappointment phone triage carried out by a nurse can inform scientific assessment whereas lowering each the quantity of ready time before coming to the clinic and the length of the consultation session. Initial scientific analysis by well-trained nonmedical spine specialists is appropriate to patients. Early entry to providers of nonmedical spine care can reduce time to analysis and supply timely care. Nurse practitioners, physician assistants, chiropractors, and physical therapists can hasten the identification of sufferers with red flags that warrant early evaluation by a spine surgeon. Transdisciplinary Clinical Assessment the flexibleness of the transdisciplinary mannequin permits a spread of medical assessments from focused to complete. Most patients current with axial neck pain and stiffness together with dysfunctional stabilization mechanics, postural faults, and lifestyle factors warranting useful treatment and rehabilitation. Both commonplace and advanced radiographs show a high prevalence of age-consistent degenerative findings, which are poorly correlated with axial neck ache. Although medicine, interventional procedures, and handbook remedy have specific makes use of, unattended useful deficits corresponding to motor control and stability dysfunction or work exposures doubtless will result in recurrent or progressive neck problems. In a transdisciplinary care setting, functionally oriented bodily and occupational therapy evaluations are important to rehabilitation, and include behavioral modification, focused exercise (for motor control, flexibility, and power training), and positive lifestyle changes. Transdisciplinary Care Planning and Coordination Synthesizing a therapy plan requires communication. Based on discipline-specific coaching or experience, factors corresponding to new signs, findings, or affected person noncompliance might become apparent to sure clinicians before others, and the flexibility to confer and respond can be crucial. Because of a lack of superiority of any single therapy method, the transdisciplinary mannequin is well suited to communication and timing, and coverings may be uniquely tailor-made to meet the evolving needs or preferences of patients. Although additional research is required, concurrent treatments could additionally be complementary within the continuum of care. For example, neuromotor and stabilization training can be restricted by pain and stiffness, which may be reduced through handbook therapy and/or interventional ache procedures. With transdisciplinary care emphasizing medical interventions to assist useful rehabilitation, sufferers and providers should stay open to various choices in the absence of improvement, including cessation or alteration of treatment. In cases refractory to lively care, referral to a persistent medical and psychologic ache specialist may be essential; nonetheless, proof suggests that integrated care in a biopsychosocial model shows promise in reducing the incidence of disability from persistent ache and associated work absence. Case Example One A 39-year-old lady employed as an oncology nurse reported a historical past of neck pain and stiffness relationship back to childhood. Team analysis was initiated on the recommendation of her primary care doctor. Her work had not required annoying lifting or affected person switch, and she had no historical past of current or distant neck or shoulder damage.
Creeping Joan (Moneywort). Rulide.
- Dosing considerations for Moneywort.
- Skin problems such as eczema, killing bacteria, diarrhea, increasing saliva, cough, and other conditions.
- How does Moneywort work?
- What is Moneywort?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96092
Cheap 150mg rulide otc
The hanging lack of practically all myelin in AxD is considered a secondary phenomenon that arises from severely disrupted astrocyte-derived myelination signaling treatment kidney cancer symptoms safe rulide 150 mg. Early in the illness course medicine 219 order rulide 150 mg online, the subcortical arcuate fibers are initially affected, and the gyri may appear swollen (31-62). As the illness progresses, diffuse quantity loss with ventricular and sulcal enlargement ensues. Clinical Issues AxD is uncommon, accounting for just 1-2% of childhood inherited leukodystrophies. In the infantile form, which is the most common, sufferers youthful than 2 years present with megalencephaly, progressive psychomotor retardation, and seizures. Juvenile AxD presents between ages 2-12 years and is characterized by bulbar and cerebellar indicators. Patients over the age of 12 years current with a selection of signs and signs, together with ataxia, bulbar indicators, and cognitive decline. Alexander Disease Terminology Alexander disease (AxD) is also called fibrinoid leukodystrophy, a misnomer given that it includes each white and grey matter. A classic finding is a T1 hypointense, T2 hyperintense rim around the frontal horns. A distinctive finding in AxD is enlargement of the caudate heads and fornices, which seem swollen and hyperintense. The thalami, globi pallidi, brainstem, and cerebellum are much less commonly affected (31-64B). In the juvenile and grownup forms, brainstem and cerebellar involvement may be striking and will even mimic a neoplasm. Differential Diagnosis the most important differential diagnoses of AxD are other inherited leukodystrophies with macrocephaly. Genetic defects that affect both peroxisomal formation or enzymatic operate cause a bunch of ailments referred to as peroxisomal issues. The commonest kind is brought on by single protein deficiencies inside intact (morphologically normal) peroxisomes. The second less widespread group of peroxisomal disorders attributable to abnormal formation of peroxisomes is discussed beneath. Hyperbilirubinemia may cause increased T1 signal depth within the globi pallidi of older sufferers. Mitochondrial Diseases (Respiratory Chain Disorders) the mitochondria are cellular organelles that are the "power plants" answerable for energy manufacturing. Although virtually every organ or tissue of the body may be affected, the nervous system and skeletal muscle are particularly susceptible because of their high power calls for. Mitochondrial disorders have vital medical and imaging overlap and are difficult to distinguish from each other. The commonest gross findings are cerebral neocortical and cerebellar abnormalities. Hepatointestinal dysfunction, hypotonia ("floppy toddler"), seizures, retinitis pigmentosa, and psychomotor retardation are frequent. The putamina (especially the posterior segments) are consistently affected, as are the caudate heads. The dorsomedial thalami can be involved, whereas the globi pallidi are less generally affected. Symmetric lesions within the cerebral peduncles are frequent, and the periaqueductal grey matter is frequently affected. The medical triad of lactic acidosis, seizures, and stroke-like episodes is the basic presentation, but different widespread signs embrace progressive sensorineural listening to loss, migraines, episodic vomiting, alternating hemiplegia, and progressive brain injury. Mean age at symptom onset is 15 years, although some sufferers might not turn into symptomatic till 40-50 years of age. The subcortical arcuate fibers, corticospinal tracts, cerebellum, and posterior brainstem are Kearns-Sayre Syndrome Terminology and Etiology. These episodic crises are sometimes triggered by febrile sickness, immunization, or surgery. Patients may develop an acute Reye-like encephalopathy with ketoacidosis and vomiting. Inherited Metabolic Disorders bilaterally symmetric basal ganglia lesions (31-73). Volume loss leads to tearing of cortical dural bridging veins that cross from the brain surface to the superior sagittal venous sinus, resulting in recurrent subdural hematomas (31-77). Other causes of macrocephaly and situations with center cranial fossa cystlike areas in infants and children must be thought-about within the differential prognosis. Three phenotypes are reported, together with neonatal onset with multiple associated congenital anomalies, neonatal onset without anomalies, and late-onset form. The neonatal onset form presents with overwhelming illness, together with metastatic acidosis and extreme hypoglycemia. The late-onset form presents with vomiting, hypoglycemia, and unexplained acidosis. The urea cycle normally prevents excess accumulation of toxic nitrogen products by incorporating nitrogen into urea, which is then excreted within the urine. Interruption of the urea cycle ends in elevated serum ammonia, which readily crosses the blood-brain barrier and causes diffuse cerebral edema. The globi pallidi, putamina, and thalami are affected with extended hyperammonemia and may show restricted diffusion (31-78D) (31-78E). A attribute sample of "crenulated" subcortical diffusion restriction and T2 prolongation strongly suggests urea cycle disorder (31-78E). Note the symmetrically enlarged basal ganglia and the bilateral "open" sylvian or lateral cerebral fissures. Central hypotonia with pyramidal tract signs and symptoms at the time of scientific disaster is seen. Neuroimaging findings range primarily based on the particular acidemia and the stage of brain maturation on the time of presentation. Manganese, Ca++, and myelin breakdown merchandise could contribute to decreased T2 sign. Adult-onset disease is characterized by slowly progressive dystonia and ataxia, as properly as extrapyramidal signs. In the most typical childish kind, initial psychomotor retardation and hypotonia are adopted by neurologic deterioration. Krabbe illness demonstrates hyperattenuating thalami, caudate, and dentate nuclei. Etiology and Pathology Fabry illness is an X-linked lysosomal storage dysfunction of glycosphingolipid metabolism. Mutation in -galactosidase leads to abnormal accumulation of glycosphingolipids in numerous tissues, especially within the vascular endothelium and smooth muscle cells. Clinical Issues Infants with Fabry illness typically present with diffuse angiokeratomas, however late-onset Fabry disease is rather more difficult to diagnose.
Buy rulide 150mg with mastercard
In a report from 2005 medicine zantac rulide 150 mg cheap overnight delivery, cheerleading injuries during practice medicine pictures rulide 150mg cheap line, sideline performances, and competitions have been found to account for approximately 50% of catastrophic backbone accidents in feminine highschool and collegiate athletes. For high-speed and collision sports activities, protecting tools for the top and face might have had unintentional results on the danger for spinal accidents. It has been suggested that the introduction of energy-absorbing helmets within the Nineteen Seventies may have contributed to an increased price of catastrophic cervical backbone injuries in American football because it fostered use of the crown of the pinnacle during tackling, also referred to as spear tackling. As such, rule modifications restricting doubtlessly harmful types of play have been one other essential side of injury prevention. Prohibiting checking from behind has probably contributed to a decreased incidence of extreme spinal accidents in ice hockey. Rule adjustments to eliminate spear tackling in American football even have resulted in a notable reduction in the incidence of catastrophic cervical injuries. Beyond enforcement of penalties for such infractions during video games, proper coaching in protected methods for tackling and checking in any respect ranges of participation are needed. Many sports-related injuries occur in unsupervised settings; thus, public consciousness is another essential part of injury prevention. Also, an American Academy of Pediatrics place statement recommends that pediatricians actively advise parents towards trampoline use by kids. Proper gear for immediate stabilization of an injured participant must be obtainable, together with a inflexible spine board and stretcher, cervical immobilization collars, instruments to take away facemasks, supplemental oxygen and airway administration units, and cardiopulmonary resuscitative equipment. Contingency plans must be in place for rapid transport to a predesignated hospital if wanted. The player may be logrolled to the supine position utilizing cervical spine precautions. Helmets and pads promote relative impartial alignment, so they should be left in place throughout this process. For injured gamers with airway compromise, the facemask ought to be removed with proper instruments or bolt cutters, if essential. Depending on the mechanism of damage, the examining doctor must preserve a excessive index of suspicion for spinal injury. A cervical collar must be applied and a rigid spine board used to transport the injured athlete from the sector. The addition of bolsters alongside the sides of the pinnacle and guide splinting by a chosen individual are precautions used to maintain impartial alignment throughout transport. Players who exit the taking half in field independently however who later notify the medical workers of a possible spinal injury should be examined on the sideline in a seated or supine place. For athletes whose signs and examination suggest a minor harm, monitoring their situation is sufficient. Table 1 Cervical Injury Fractures A number of cervical backbone fractures occur in the athletic setting (Table 1). Spinous process fractures are comparatively benign and often symbolize avulsion accidents resulting from forceful contraction of the trapezius and rhomboid muscle tissue. Compression fractures may be attributable to comparatively low-energy mechanisms of harm as properly. In higher-energy collisions, the position of the cervical spine and the course of loading affect harm patterns. When the neck is in impartial alignment, the cervical backbone is lordotic and energy inputs may be dissipated somewhat by the intervertebral disks and paraspinal muscular tissues. Biomechanical analysis has instructed that with flexion of approximately 30�, the straightened cervical spine assumes the bodily characteristics of a segmented column. When the edge of vertical compression is reached, the cervical backbone fails and buckles in a flexion mode with anterior column failure and attainable facet subluxation or dislocation. If an injured participant sustains an obvious or suspected spinal wire damage, the on-the-field management protocol previously described should be adopted for initial treatment. Efforts to keep oxygenation and blood strain to maximize spinal wire perfusion should be initiated throughout transport to the hospital. After preliminary resuscitation, the injured participant ought to be transported to a tertiary referral trauma middle the place immediate reestablishment of spinal alignment and neurologic decompression may be carried out by way of closed or open methods. Cervical twine neurapraxia, also referred to as transient quadriparesis, can happen on account of pressured hyperflexion or hyperextension in a stenotic canal. Symptoms, which final from a few minutes to 48 hours, range from mild paresthesias in a couple of extremity to transient quadriplegia. Neck ache is minimal to nonexistent within the absence of structural harm to the spinal column. Recurrence of cervical wire neurapraxia has been reported in up to 50% of instances, with the danger correlating to the extent of canal stenosis. Stingers Stingers or burners are caused by neurapraxia of one or more ipsilateral cervical nerve roots or the brachial plexus, resulting in pain, paresthesias, and weak point in a single upper extremity. The participant normally stories tingling and burning radiating from the neck into the arm. Physically immature athletes could maintain this damage by a mixture of lateral bending of the neck and melancholy of the contralateral shoulder, leading to traction to the upper cervical nerve roots or the brachial plexus trunk. Physically mature athletes can experience related signs caused by axial loading of an prolonged, rotated, or laterally bent cervical backbone causing neuroforaminal compression. This latter presentation is more common in athletes with preexisting degenerative changes and will end in extra severe symptoms. A stinger could be distinguished from cervical twine neurapraxia by its unilateral features and absence of long tract signs. If radiculopathy is suspected primarily based on clinical features, superior imaging research might help confirm the analysis. Persistent signs might recommend higher grade injury similar to axonotmesis or neurotmesis. The use of electrodiagnostic research and the involvement of a hand or microvascular specialist are helpful in these tough instances. Disk Herniation Although disk herniation ensuing from degenerative changes within the spine is widespread in the common population, axial loading of the neck during sports activities activities could contribute to disk herniation in athletes. Disk herniation may end in isolated neck ache, or it may be accompanied by radicular signs. The initial management of disk herniation in athletes is just like that for the general population for administration of axial ache and isolated root compression. Effacement of the spinal cord could be managed nonsurgically, but repeat imaging must be carried out to exclude cord compression in symptomatically improved athletes earlier than they return to sports activities. Musculoligamentous Injuries Muscular and ligamentous accidents are common sports-related injuries. Ligamentous sprain or muscular strain can occur after aggressive bending or rotational injuries to the neck. Pain is probably not instant; instead, it might manifest over the 24-hour interval after injury. Tenderness is usually seen on palpation, and range of motion may be limited by affected person guarding. If needed, a collar ought to be used till ligamentous injury is definitively ruled out.
Rulide 150mg purchase with amex
Because nerve conduction happens in each instructions following nerve depolarization symptoms mold exposure order 150mg rulide otc, sensory nerve conduction studies may be carried out utilizing both orthodromic (in the course of physiologic conduction) or antidromic (opposite of physiologic conduction) techniques 10 medications that cause memory loss rulide 150mg discount line. Although the antidromic method is usually most well-liked, significantly due to the upper amplitude compared with the orthodromic approach, both methods have advantages and disadvantages. Late response studies such because the F-wave and H-reflex studies are typically used to assess more proximal nerve segments. These research can present extra info within the analysis of radiculopathies, plexopathies, polyneuropathies, and proximal peripheral neuropathies. Taken altogether, the numeric values of the latency, amplitude, and conduction velocity of the various nerve conduction research can level to a focal nerve lesion such as an entrapment or a diffuse neurogenic process such as a peripheral polyneuropathy. Monopolar and concentric needles each have benefits and disadvantages, but each are widely used. The needle is inserted into each muscle of curiosity, and a number of other additional small, transient insertions are made to adequately sample every muscle. Insertional activity and spontaneous activity are assessed while the muscle is at rest. In a traditional muscle, there must be electrical silence shortly after needle movement. Increased insertional exercise is defined as any electrical activity that lasts longer than 300 ms after temporary needle movement, with the exception of end plate potentials, which can be seen if a needle is positioned near the motor finish plate. Spontaneous activity is defined as any electrical activity at rest that lasts longer than 3 seconds. Two kinds of spontaneous exercise commonly seen with denervation are fibrillations and positive sharp waves. These symbolize irregular electrical exercise generated from denervated single muscle fibers. Fibrillations and constructive sharp waves are graded primarily based on their distribution and intensity, ranging from 1+ (persistent single runs in two areas) up to 4+ (continuous discharges in all areas of the muscle). Amplitude is measured from essentially the most optimistic to essentially the most negative peak, and the conventional worth is often 1-2 mV. Amplitude can be elevated in the setting of reinnervation, usually indicating a continual neurogenic dysfunction. Duration is measured from the initial baseline departure to the final return to baseline, and the traditional value is often 5-15 ms. Duration may be increased within the setting of reinnervation, usually indicating a subacute neurogenic dysfunction. Increased phases, or polyphasicity, can be seen in the setting of reinnervation, usually indicating a subacute neurogenic dysfunction. Table 2 Electrodiagnostic Testing for Spine Disorders the timing of efficiency of electrodiagnostic testing is dependent on the medical differential analysis. Electrodiagnostic testing may be indicated within the assessment of any suspected nerve dysfunction. Patients with signs such as arm or leg pain, weakness, or numbness or tingling are generally referred for electrodiagnostic testing. Testing can confirm the presence of a radiculopathy; rule out peripheral nerve issues, which might affect similar anatomic distributions; and identify the presence of multiple coexistent nerve disorders. For instance, a patient may concurrently have a cervical radiculopathy, carpal tunnel syndrome, and a peripheral polyneuropathy. The timing or efficiency of electrodiagnostic testing also depends to some extent on the sort of data desired. This misconception is based on the idea that wallerian degeneration, which can take a number of days to weeks, must first occur earlier than significant information can be obtained. However, a considerable axonal damage could be seen immediately, and this info could assist in early localization of the damage. The major limitation to early performance of electrodiagnostic testing is the problem in differentiating a conduction block from an axonal damage immediately after a nerve damage. This is adopted by adjustments of denervation in the peripheral muscle tissue (proximal to distal) at approximately three weeks. Temperature is the most important physiologic issue affecting nerve conduction research. A lower in temperature can cause prolonged latency, increased amplitude, increased duration, and decreased conduction velocity. Normal temperature is approximately 32�C for the upper extremity and 30�C for the lower extremity. Other physiologic components that can affect nerve conduction research embrace age, peak, sex, edema, weight problems, and anomalous innervation. These embody improper electrode placement, suboptimal stimulation, inaccurate measurements, and failure to acknowledge artifacts. These elements can create inaccurate latency, amplitude, and conduction velocity measurements, which may finish up in incorrect conclusions. Recognition of potential technical elements is crucial when conducting nerve conduction studies. A 2011 study reported that when solely optimistic sharp waves or fibrillations were considered irregular, specificity ranged from 92% to 97% in lumbosacral radiculopathy. At least one motor nerve conduction research and one sensory nerve conduction examine ought to be carried out within the concerned limb. The sensory nerve conduction research ideally ought to be within the distribution of the suspected radiculopathy. The screening for a suspected radiculopathy ought to look at no much less than five to seven muscles, including the paraspinal muscular tissues. No consensus exists relating to which muscular tissues should be included within the preliminary screening. The optimum variety of muscle tissue tested for both cervical and lumbosacral radiculopathy screenings has been proposed to be six muscles and should include the paraspinal muscles. A diagnosis of a radiculopathy based on findings of fibrillations and optimistic sharp waves is considered extremely convincing. A prognosis of a radiculopathy based mostly on findings of decreased recruitment or increased polyphasicity is taken into account much less robust. Diagnostic Ultrasonography as an Adjunct to Electrodiagnostic Testing the use of neuromuscular ultrasonography has rapidly increased over the past decade and is a valuable adjunct to electrodiagnostic testing. Ultrasonography could also be considered in conditions during which peripheral nerve entrapment is a part of the differential analysis, but electrodiagnostic take a look at findings are adverse for evidence of any entrapment neuropathy. Iatrogenic harm to these constructions can happen from contusion, mechanical compression, vascular compromise, or a mixture of these elements. The first broadly used technique for intraoperative assessment of neurologic constructions was the Stagnara wake-up check. The Stagnara wake-up test also is associated with risks similar to recalling intraoperative occasions, extubation, and issue performing the check in sure affected person populations corresponding to those with cognitive deficits.
Cheap rulide 150 mg without prescription
Resnick S treatment yellow jacket sting rulide 150mg cheap mastercard, Inaba K medicine ball core exercises 150 mg rulide amex, Karamanos E, et al: Clinical relevance of magnetic resonance imaging in cervical backbone clearance: A prospective study. When screening for trauma sufferers susceptible to thoracolumbar spine harm, medical examination mixed with age older than 60 years and a high-risk mechanism resulted in a sensitivity of ninety eight. This retrospective cohort examine investigated the performance of scientific examination to clear thoracolumbar trauma in patients with distractive injuries. The sensitivity of medical analysis clearance was 75% for all thoracolumbar harm and 89% for important harm requiring surgical procedure or bracing. Inaba K, Munera F, McKenney M, et al: Visceral torso computed tomography for clearance of the thoracolumbar backbone in trauma: A review of the literature. This research presents a classification for exterior cervical immobilization that appeared clinically helpful and had nearly good intrarater and interrater settlement. This systematic literature review suggests an increased threat of strain ulcer development with external immobilization gadgets. This potential observational research on trauma patients within the emergency division found substantial grade 1 and a couple of pressure ulcers as nicely as shoulder and chest ache related to the utilization of extrication collars and headblocks. This review highlights the perfect traits of bracing for thoracolumbar accidents. This article evaluations the American Academy of Orthopaedic Surgeons clinical practice guideline on the remedy of osteoporotic spinal compression fractures. This review suggests no evidence exists for or towards using exterior orthoses for treatment of vertebral compression fracture. An association was found between shorter surgical timing and vital neurological recovery. Jug M, Kejzar N, Vesel M, et al: Neurological recovery after traumatic cervical spinal cord harm is superior if surgical decompression and instrumented fusion are carried out inside 8 hours versus 8 to 24 hours after harm: A single middle expertise. Grassner L, Wutte C, Klein B, et al: Early decompression (<8 h) after traumatic cervical spinal cord injury improves functional end result as assessed by spinal wire independence measure after one yr. This article evaluations the essential neuroprotective interventions at present applied in clinical follow, these underneath scientific investigation, and potential future neuroregenerative therapies. The number of accidents in the upper cervical spine is growing, mostly occurring in the geriatric inhabitants. Many new classification techniques provide extra actual differentiation of stability and will assist guide treatment. For atlas and axis fractures, a quantity of techniques of osteosynthesis have been proposed somewhat that atlantoaxial fusion. In the subaxial backbone, hyperextension injuries with spinal wire accidents and fractures via an ankylosed spine are increasing in frequency, and evidence suggests early surgery supplies optimum outcomes. Other widespread accidents are lateral mass and facet fractures, with newer proof suggesting that surgical therapy is best than nonsurgical therapy. Keywords: atlas fractures; axis fractures; craniocervical dissociation; decrease cervical spine injuries; occipital condyle fractures; upper cervical spine trauma Dr. Early identification and classification of damage patterns is important and potential by using crucial physical examination and trendy imaging. The use of protocols to identify substantial damage may end up in fewer delays and missed diagnoses. Most injuries have a number of treatment choices, and treatment should be individualized. Epidemiology Cervical backbone accidents occur in 3% to 5% of all blunt trauma sufferers; fewer than 25% of these patients sustain spinal twine accidents. Although the geriatric inhabitants is growing in number, the rate of backbone fractures in these sufferers appears to be increasing at a larger fee. Upper cervical accidents occur between the occiput and C2; subaxial injuries are found between C3 and T1. In all cervical injuries, 65% of fractures and 75% of dislocations happen in the subaxial cervical backbone. In a report of sixty nine people with cranial cervical disassociation in a single county in Washington state over a 5-year period, two-thirds of the individuals died at the scene and one-third survived to reach the hospital. C, Coronal scan shows how the occipital condyles lie within the C1 lateral masses. Diagnosis Protocols for the initial analysis of cervical spine accidents have been described beforehand. Thus, spinal column stability exists if gravity and the alar ligaments, which project laterally and slightly cranially from the dens to the anterior-medial edge of the foramen magnum, and the tectorial membrane ligaments maintain the occipital condyles downward. The tectorial membrane, which is the thickened continuation of the posterior longitudinal ligament spanning between the dens and the foramen magnum, is the other important restraining ligament. The atlas is a ring-like structure with giant lateral lots linked by a short anterior arch and a longer posterior arch. The posterior arch is notched on its superior floor by the vertebral artery, which could be considered a weak location where fractures can occur. The inferior floor of the atlantal lateral lots is semiconvex and situated instantly above a similar aspect articulation of the axis. Most conspicuous is the dens or odontoid process, which initiatives in a cranial path behind the atlantal anterior arch. Forward translation is prevented by the transverse ligament and secondarily by the alar ligaments. Biomechanically, the atlas acts as a bushing whereas the stabilizing ligaments prolong from the axis to the occiput. This structure thickens horizontally, creating the transverse ligament that spans behind the dens and attaches to tubercles on the atlas. The transverse ligament prevents anterior atlantoaxial subluxation by maintaining the dens in apposition to the atlantal anterior arch. The anterior atlantal ligament extends from the posterior side of the atlantal anterior arch to the ventral side of the dens. Subaxial Anatomy the subaxial cervical vertebrae have comparable morphology, though they turn into larger caudally. Short, obliquely oriented pedicles join the vertebral body to the lateral lots. The lateral plenty are rhomboid formed when viewed laterally and square shaped when seen dorsally. The upward and downward projections of the lateral plenty are the superior and inferior aspects, respectively. Posteriorly, the lateral plenty are linked by thin lamina that thickens in the midline. The anulus fibrosus has a strong collagenous construction and is important for stability. Two-paired synovial facet joints are oriented upward and assist stop anterior translation.