
Requip dosages: 2 mg, 1 mg, 0.25 mg, 0.5 mg
Requip packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

2 mg requip order amex
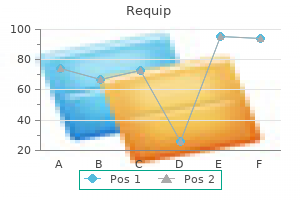
Prognostic worth of pinprick preservation in motor complete 300 medications for nclex requip 2 mg purchase fast delivery, sensory incomplete spinal cord damage treatment xanthelasma eyelid requip 0.5 mg otc. In: Their Primary Forms and in Their Modifications by Age, Sex, Constitution, Hereditary Disposition, Excesses, General Disorder, and Organic Disease. Synopsis of the Diastolic Nervous System: or the System of the Spinal Marrow, and Its Reflex Arc; as the Nervous Agent in All the Functions of Integration and of Egestion within the Animal Oeconomy. Recovery from spinal cord injury-underlying mechanisms and efficacy of rehabilitation. Neurological prognosis and the indications for treatment of paraplegia and tetraplegia, associated with fractures of the spine. Tendon reflexes for predicting movement recovery after acute spinal cord harm in humans. Prognostic significance of the delayed plantar reflex following spinal wire harm. Recovery is related to numerous degrees of autonomic dysreflexia typified by surges of hypertension, tachyarrhythmia, sweating, and hyperthermia which could be detrimental, inflicting intracerebral hematomas, seizures, and even death. The sensitivity and specificity of the digital rectal examination for detecting spinal wire harm in grownup sufferers with blunt trauma. Injury severity as major predictor of consequence in acute spinal twine damage: retrospective results from a big multicenter scientific trial. The international standards booklet for neurological and useful classification of spinal twine damage. Motor restoration following spinal twine harm related to cervical spondylosis: a collaborative examine. Spinal twine power metabolism following compression trauma to the feline spinal cord. Presented at the 2005 Annual Scientific Meeting of the American Association of Neurological Surgeons held in New Orleans, Louisiana. Pathophysiology of cerebral ischemia and mind trauma: similarities and variations. Correlation of the extracellular glutamate concentration with extent of blood flow discount after subdural hematoma within the rat. The relationships among the severity of spinal twine harm, motor and somatosensory evoked potentials and spinal wire blood flow. Focal microvascular occlusion after acute subdural haematoma in the rat: a mechanism for ischaemic damage and mind swelling The neurochemical and metabolic cascade following brain harm: moving from animal fashions to man. Brain oedema in focal ischaemia: molecular pathophysiology and theoretical implications. Spinal twine blood move as affected by adjustments in systemic arterial blood strain. Autoregulation of cerebral blood circulate after experimental fluid percussion damage of the mind. Loss of autoregulation and posttraumatic ischemia following experimental spinal cord trauma. Descending vasomotor pathways in people: correlation between axonal preservation and cardiovascular dysfunction after spinal twine injury. The clinical issues in cardiovascular control following spinal wire harm: an outline. The modifications in human spinal sympathetic preganglionic neurons after spinal cord injury. Tail arteries from chronically spinalized rats have potentiated responses to nerve stimulation in vitro. Autonomic dysreflexia: incidence in individuals with neurologically complete and incomplete tetraplegia. Relationship between serum dopamine-beta-hydroxylase activity, catecholamine metabolism, and hemodynamic modifications throughout paroxysmal hypertension in quadriplegia. J Neurosurg 1973;38:326�331 61 7 Emergency Room Evaluation Including Assessment of Spinal Shock 87. Experimental spinal wire injury: electrocardiographic abnormalities and fuchsinophilic myocardial degeneration. Studies of experimental cervical spinal wire transection, I: Hemodynamic adjustments after acute cervical spinal twine transection. The function of the sympathetic nervous system in pressor responses induced by spinal harm. Increased susceptibility of sufferers with cervical twine lesions to peptic gastrointestinal issues. Clinical and anatomical remark of a affected person with a complete lesion at C1 with maintenance of a normal blood pressure during forty minutes after the accident. Cardiovascular abnormalities accompanying acute spinal wire harm in people: incidence, time course and severity. The incidence of neurogenic shock in patients with isolated spinal twine injury in the emergency department. The motor examination is graded using a scale from zero to 5: 0-Total paralysis (no movement) 1-Palpable or seen muscular contraction 2-Full vary of motion with gravity eradicated 3-Full vary of motion towards gravity 4-Full vary of motion against gravity and partial extra resistance 5-Normal or full motor exercise the exam separates higher and lower limbs, which are additional subdivided into 5 major muscle groups, where every muscle group represents a specific spinal phase. For example, the C7 spinal segment is represented by the elbow extensors as a result of the first muscle is the triceps, which is innervated by a majority of C7 nerve fibers. In addition, the left and right sides are scored individually the place each limb gets a total maximum of 25, and a rating of a hundred represents an individual with no motor deficit. The sensory examination utilizes a numeric scale from zero to 2: 0-Absent sensation 1-Presence of sensation however "abnormal" 2-Normal or intact sensation. Limitations of the size and areas of enchancment had been identified, and it was then the system divides the sensory examination in a total of 28 dermatomes: seven cervical, 12 thoracic, 5 lumbar, and 4 sacral. Each sensory modality has a most bilateral whole of 112 points, thus making 224 for a patient without a sensory deficit. Based on both the motor and sensory assessments, a cumulative neurological evaluation is defined. This system in addition provides the ability to determine the level of where a spinal damage occurred primarily based on essentially the most caudal level with regular operate. An damage could be broadly categorized as full or incomplete based mostly on the presence of any motor or sensory operate distal to the world of damage. Frankel et al stratified the accidents into a five-letter grade (A to E) based mostly on decreasing severity. Grade A was described as a complete motor and sensory deficit below the extent of the lesion. Grades C and D had both motor and sensory functions beneath the level of harm; in grade C, motor operate was current however not useful for the patient, as opposed to grade D.
0.5 mg requip purchase visa
Rowland and Darryl Baptiste for their help and recommendation in getting ready this chapter treatment bronchitis discount 2 mg requip free shipping. Geron has reportedly developed assays to ensure excessive purity of their cell isolates treatment xdr tb guidelines requip 0.25 mg buy generic, in addition to techniques for culturing these cells without the need for feeder cells that would theoretically lead to viral contamination or nonhuman polysaccharide epitopes on the surface of transplanted cells. Review of remedy trials in human spinal wire damage: issues, difficulties, and suggestions. Spine J 2004; four:451�464 549 fifty six Translational Clinical Research in Acute Spinal Cord Injury Summary 550 8. Beneficial effects of methylprednisolone sodium succinate within the remedy of acute spinal twine harm. High dose methylprednisolone in the management of acute spinal cord harm - a scientific review from a scientific perspective. Questionnaire survey of backbone surgeons on the use of methylprednisolone for acute spinal wire injury. Ganglioside-induced regeneration and reestablishment of axonal continuity in spinal cord-transected rats. Effect of thyrotropin-releasing hormone on the neurologic impairment in rats with spinal twine damage: therapy beginning 24 h and 7 days after injury. Gacyclidine: a new neuroprotective agent acting on the N-methyl-D-aspartate receptor. Acute spinal wire injury: early care and therapy in a multicenter study with gacyclidine. Neuroprotective effect of gacyclidine: a multicenter double-blind pilot trial in sufferers with acute traumatic brain damage. The effect of nimodipine and dextran on axonal perform and blood flow following experimental spinal twine injury. Intrathecal dynorphin A (1-13) and (3-13) cut back spinal twine blood flow by nonopioid mechanisms. The effect of long-term high-dose naloxone infusion in experimental blunt spinal wire damage. Naloxone reduces alterations in evoked potentials and edema in trauma to the rat spinal twine. A novel impact of an opioid receptor antagonist, naloxone, on the manufacturing of reactive oxygen species by microglia: a research by electron paramagnetic resonance spectroscopy. Naloxone lowers cerebrospinal fluid ranges of excitatory amino acids after thoracoabdominal aortic surgery. The design of scientific trials for cell transplantation into the central nervous system. Experimental Treatments for Spinal Cord Injury: What You Should Know If You Are Considering Participation in a Clinical Trial. Factors predicting motor recovery and useful end result after traumatic central cord syndrome: a long-term follow-up. Cerebrospinal fluid drainage reduces paraplegia after thoracoabdominal aortic aneurysm restore: outcomes of a randomized medical trial. Postischemic gentle hypothermia reduces neurotransmitter launch and astroglial cell proliferation during reperfusion after asphyxial cardiac arrest in rats. Inhibition of glutamate launch: a possible mechanism of hypothermic neuroprotection. Biphasic opening of the blood-brain barrier following transient focal ischemia: effects of hypothermia. Prolonged hypothermia protects neonatal rat brain towards hypoxic-ischemia by reducing each apoptosis and necrosis. Post-ischemic hypothermia delayed neutrophil accumulation and microglial activation following transient focal ischemia in rats. Glutamate launch and free radical manufacturing following brain injury: results of posttraumatic hypothermia. Effect of reasonable hypothermia on lipid peroxidation in canine brain tissue after cardiac arrest and resuscitation. Current status of spinal twine cooling within the treatment of acute spinal wire damage. The direction of development of differentiating neurones and myoblasts from frog embryos in an applied electrical subject. Oscillating area stimulation for full spinal cord harm in humans: a section 1 trial. Neuroprotection by minocycline facilitates important recovery from spinal wire injury in mice. Minocycline remedy reduces delayed oligodendrocyte death, attenuates axonal dieback, and improves functional outcome after spinal cord damage. Minocycline inhibits contusion-triggered mitochondrial cytochrome c release and mitigates practical deficits after spinal cord injury. Minocycline reduces cell demise and improves functional restoration after traumatic spinal wire damage in the rat. Tetracyclines inhibit microglial activation and are neuroprotective in world brain ischemia. Minocycline inhibits microglial activation and protects nigral cells after 6-hydroxydopamine injection into mouse striatum. Minocycline neuroprotects, reduces microgliosis, and inhibits caspase protease expression early after spinal twine harm. Minocycline supplies neuroprotection towards N-methyl-D-aspartate neurotoxicity by inhibiting microglia. Minocycline alleviates death of oligodendrocytes by inhibiting pro-nerve progress issue production in microglia after spinal cord injury. Riluzole and methylprednisolone combined treatment improves useful recovery in traumatic spinal wire harm. Evaluation of the neuroprotective effects of sodium channel blockers after spinal twine injury: improved behavioral and neuroanatomical restoration with riluzole. Mechanisms underlying the riluzole inhibition of glutamate launch from rat cerebral cortex nerve terminals (synaptosomes). Effects of the sodium channel blocker tetrodotoxin on acute white matter pathology after experimental contusive spinal cord injury. Riluzole promotes cell survival and neurite outgrowth in rat sensory neurones in vitro. Nogo-A and myelin-associated glycoprotein mediate neurite development inhibition by antagonistic regulation of RhoA and Rac1. Myelin-associated glycoprotein interacts with the Nogo66 receptor to inhibit neurite outgrowth.
Requip 0.5 mg purchase on line
This line is then closely checked for its position relative to the sigmoid notch medications excessive sweating order 2 mg requip free shipping, posterior border symptoms 3 days before period requip 2 mg buy low price, and angle. The use of the so-called antilingula has been proposed as the landmark for the mandibular foramen, however has typically fallen into disfavor, because of each the difficulties with its identification and its lack of predictable relation to the foramen. In considering the three locations of the osteotomy minimize, the vascular hazards should be acknowledged, together with the maxillary artery superiorly, the inferior alveolar artery within the middle, and the facial artery inferiorly. Therefore, the surgical capability to management a bleed from one of these three sources ought to factor into the decision regarding the place to start and the place to finish the osteotomy. As the minimize is accomplished, anterolateral rigidity is maintained on the Merril-Levaseur retractor in order that the proximal fragment shall be introduced out laterally and prevent medial displacement. Preoperative submentovertex radiographs have been really helpful to establish divergence of the posterior border. The use of this radiograph as a criterion for selecting this method has been questioned, however some nonetheless imagine that it may be used to identify the harder cases. Oblique versions, with the cut ending above the angle, have been described by many clinicians, with the only obvious benefit being the relative ease in performing the technique. Interestingly, the one potential disadvantage, that of decreased skeletal stability, additionally appears to be difficult to reveal. The mandibular dentition is brought into its new place after the completion of both osteotomies, as established by a preformed occlusal splint and stabilized with maxillomandibular fixation. Attention is directed back into the wound and towards placement, or discount, and stabilization of the proximal fragment. Wire osseous fixation is usually not needed, though advocated by some surgeons. Most essential is achieving as broad a bone contact space as attainable, with out displacing or rotating the condyle. Adjustment of the lateral cortex of the distal fragment may be carried out with a straight fissure bur or small acrylic bur to permit the proximal fragment to lie as flat as possible against the vertical ramus. After an intensive irrigation of the wound, the mucosa is closed with a running stitch, using a resorbable suture. The use of osseous wire fixation has been advocated to ensure the seating of the condyle. Again, no examine evaluating wire osseous fixation with no fixation has proven any benefit for the use of the wire. The effect of the temporalis pull on relapse has led to other suggestions that embrace both stripping the temporalis attachment completely off of the coronoid process or coronoidotomy. The use of coronoidotomy has been recommended by some clinicians for large setbacks, with a couple of utilizing this modification routinely. A further modification of the inverted-L osteotomy has been using rigid inside fixation. A combination of sharp and blunt dissection is used to access the inferior border of the mandible. Care is taken to avoid damaging the marginal mandibular branch of the facial nerve. The exterior strategy has been advocated for large mandibular setbacks of larger than 10 mm, troublesome asymmetries, or large vertical strikes in patients with uncommon facial structure. Except for the danger of the scar, the risks of this system have been reported as being comparable with the intraoral method. These have included numerous radiographic research documenting positional change of the condyle relative to the fossa. The maintenance of some muscle attachment to the angles makes this chance unlikely. Goldstein81 was the first to use serial cephalograms to consider the postoperative change of the mandible after surgical correction of the mandibular prognathism. Poulton and colleagues82 beneficial overcorrecting the mandibular setback by 2 mm to present for the relapse that they noted. This quantity of common relapse has, surprisingly, remained pretty constant throughout the history of this method, even though technical modifications in procedures have been made. This problem was initially attributed to the "condylar sag" seen on x-ray films taken soon after surgery. In Scandinavian international locations, however, this surgical procedure has been successfully used for sufferers with mandibular horizontal extra and anterior open chew. This concern, nevertheless, seems to be unsubstantiated, in that nearly all of the clinicians reporting on the outcomes of this strategy have famous little or no, if any, motor nerve damage. The horizontal osteotomy of the vertical ramus has typically fallen into disuse due to the substantial relapse potential, however most of the remaining suggested variations continue to have remedy value. The two procedures that appear to be the most popular are the invertedL and the C osteotomites. Both are usually approached extraorally, although intraoral variants are possible. Indications the C osteotomy is generally reserved for therapy of horizontal mandibular deficiency, with some authors suggesting that it might be used to shut an anterior open chunk. The inverted-L, nonetheless, has been used for the correction of most types of mandibular horizontal discrepancies, together with an anterior open chunk. Generally, advancements of the distal phase with both approach require bone grafting to guarantee adequate bone union. For that purpose, the inverted-L is described first, with various modifications of the C mentioned later. This may be completed in quite a lot of methods, but most surgeons use a plastic drape with adhesive on one edge to separate the 2 areas. The external drapes ought to be arranged in order that they allow turning of the top for entry to the submandibular wounds in addition to access to the mouth. The submandibular incision is made 2 cm below the angle and inferior border of the mandible. The posterior portion is curved superiorly to comply with the cervical pores and skin line in addition to to enhance the entry to the whole vertical ramus. Sharp dissection is used down via the platysma, and then blunt dissection is begun to reduce threat to the marginal mandibular department of the facial nerve. The incision by way of the pterygomandibular sling and periosteum is made along the inferior border and is carried around the angle and up the posterior border about 2 cm. Periosteum and attachments for the masseter are fully stripped off the lateral cortex of the vertical ramus up to the level of the sigmoid notch. Very little periosteum is stripped off the medial side, particularly on the angle, to retain as a lot blood provide as possible to the proximal fragment. The posterior vertical osteotomy is made a minimum of 7 mm in front of the posterior border and extends to a degree of the inferior border simply in entrance of the angle. It is helpful to review the research by Reitzik and associates72 of the position of the foramen relative to the lateral landmarks to reduce trauma to the neurovascular bundle. Once the cuts are made, the medial periosteum may should be elevated from some of the distal fragment to allow its advancement. Moist gauze is positioned in the wound, and a similar process is completed on the alternative side. The subsequent step varies depending on the sort of mandibular motion that occurred; however, the importance of sustaining the proximal fragment near its preoperative place stays.
Discount 0.25 mg requip
Beveling the reduce from anterior to posteroinferior will reduce the amount of bone to be eliminated and increase the size of the lingual delicate tissue pedicle symptoms neck pain cheap requip 0.25 mg otc. Usually medications after stroke generic requip 0.25 mg on-line, when attempting to reposition the mobile dentoalveolar segment to the the rest of the mandible, further bony interferences are encountered. These exist primarily on the lingual cortex of the vertical cuts, and care must be used within the rotation of the mobile phase to access this cortex. As talked about earlier for the step osteotomy, when possible, a retractor should be placed between the bone and the skinny lingual mucosa to decrease iatrogenic delicate tissue trauma. Osseous wires or plates with monocortical screws are hardly ever needed for stability, however can be utilized if desired. Bone gaps attributable to movement of the phase, especially by vertical motion essential for the closure of an anterior open chunk, ought to be grafted. As has been noted earlier, the potential for this occurring in midline osteotomies is low, however whether this might be associated to different parts of the dental alveolus is uncertain. Whereas these techniques have fallen out of favor as primary remedy options, every has a small place in orthognathic surgery; due to this fact, the indications and techniques of each are described individually, and because the issues are similar, these are discussed together as nicely. The biggest concern in this process is the potential for damaging tooth, and due to this fact, house should be current or created to permit secure vertical cuts in the dental alveolus. The surgical site is then irrigated completely and closed with resorbable sutures. Primarily, it might be used as an aid in the correction of supereruption of posterior mandibular teeth or ankylosis of one or more posterior enamel. An incision begins 3 to 4 mm lateral to the attached gingiva, beginning on the anterior border of the vertical ramus. The osteotomy is printed with a bur, based on the preoperative radiographic evaluation of the size of the roots and the position of the inferior alveolar canal. The horizontal reduce is carried solely via the buccal cortex, and a thick splitting osteotome is used to complete the osteotomy. Grafting is used if a bone gap is important, and the mucosa is closed with a operating resorbable suture. Periapical radiographs taken intraoperatively after the buccal horizontal minimize will ensure that the osteotomies are made at a safe distance from the teeth and canal. This latter approach has been discovered to be helpful as a outcome of enough visualization is difficult with the presence of posterior enamel. Also, with either of those strategies, the horizontal cut could be made safely via the lingual cortex, which eliminates the dearth of predictability of the induced lingual cortical fracture. It has also been advocated for closure of an anterior open chunk when used with a bone graft. Technique An incision begins on the exterior oblique ridge of the base of the vertical ramus. The incision is carried all the way down to bone and extends ahead 4 to 5 mm under the hooked up gingiva. The incision could be positioned inferiorly in the region of the canine and forward the place it meets the contralateral incision on the midline. The periosteum is elevated to expose the lateral cortex, with care taken across the mental nerve, in addition to leaving some attachment on the inferior border of the symphysis for the soft tissue chin. The vertical cut posterior to the terminal molar is made first and carried right down to the extent of the deliberate horizontal osteotomy. As with the step osteotomies, the horizontal reduce must be placed appropriately, primarily based upon preoperative periapical radiographs. The horizontal reduce can then be positioned low sufficient to be at a protected distance from the dental root apices, in addition to sustaining an sufficient vascular pedicle to the dental alveolus. The angle of the horizontal cut should be made to facilitate phase movement; for example, a flat cut paralleling the maxillary occlusal airplane permits the straight development of the segment with out considerably altering mandibular vertical peak while at the similar time maintaining a large space of bone contact. However, the speed of restoration of sensory loss seems to give some measure of the iatrogenic trauma to the tooth. Early scientific research appear to show that enamel in mandibular alveolar osteotomies fare higher than their maxillary counterparts. The enamel at biggest danger for harm are those within the mobile phase directly adjacent to the vertical osteotomies. The tooth instantly posterior to the vertical cut are approximately equal in danger to the enamel within the middle of the cellular phase. Periodontal issues have been talked about by authors reviewing mandibular alveolar osteotomies. Periodontal issues are seen less incessantly when the vertical cuts are made in extraction websites than when the cuts are tried between teeth with out extraction. As with correction of an anterior open bite, any important bone gaps created may be full of graft materials. Also, the sagittal a half of the osteotomy permits a larger bone contact space to help in bony healing. The complete mandibular alveolar osteotomy can additionally be divided into interdental segments to appropriate axial inclination of tooth or close edentulous websites. Complications the problems of all mandibular subapical alveolar osteotomies are considered together owing to their similarities. Stability is usually mentioned as one of many benefits of the alveolar osteotomies due to the minimal delicate tissue forces appearing on these areas. Unfortunately, there have been very few research to document this declare, and the approach has limited use. Theisen and Guernsey220 evaluated six patients who had anterior subapical osteotomies. In distinction, Kloosterman48 evaluated a much larger group and found a 30% recurrence of an open chew after anterior maxillary osteotomies. Interestingly, the most important difference between the two groups was at delicate tissue "B" level, with the subapical osteotomy leading to a significant lower in the labiomental angle. Unlike segment stability, neurologic and vascular problems of segmental osteotomies have received quite lots of attention. The versatility of this process for correction of skeletal deformities of the chin is spectacular, and the results are superior to those of synthetic implant placement generally. The indications, therefore, are sometimes made apparent by comprehensive presurgical treatment planning. Technique the horizontal osteotomy of the symphysis is usually carried out along side other major osteotomies and, thus, is incessantly accomplished underneath basic anesthesia. However, it may be carried out as a separate procedure on an outpatient basis with sedation and local anesthesia. The mucosal incision is made on the labial facet of the vestibule at roughly 1 cm above its depth and extends posteriorly to the primary bicuspid region. The periosteum is elevated inferiorly to a degree slightly below the meant stage of the osteotomy. Laterally, the periosteum is elevated to the mental foramen after which extended posteroinferiorly to the mandibular inferior border beneath the psychological foramen bilaterally. The extent of the posterior cortical publicity is generally determined by the place of the mental foramen and the vertical top of the mandible on this area. In basic, no try is made to expose the mental nerve by releasing the soft tissue round it, primarily as a result of the nerve may be small and friable, making inadvertent severing a possibility.
Order 2 mg requip with visa
Difficulties arise if the deliberate osteotomy consists of extraction of the first bicuspid or if the reduce is planned behind this space medicine hollywood undead requip 0.25 mg generic online. Not solely is the vitality of the tooth doubtlessly compromised medications management requip 1 mg without prescription, however the whole dentoosseous segment may be affected by the level of the horizontal cut. If parallel horizontal cuts are planned to transfer the anterior section apically, the superior reduce is made first. The periosteal elevation posterior to the mental foramen is minimized to solely what is important for placement of a slender channel retractor and the reciprocating noticed blade or bur. It is useful at this level to inscribe a vertical mark (or two or three marks) into the bone throughout the planned osteotomy website in the anterior mandible so that the transverse position of the inferior fragment can be more easily reoriented after completion of the osteotomy. The length and angle of the horizontal cut might have profound results on positioning of the mobilized phase as properly as the ultimate postsurgical outcomes. Further osteotomies or osteoplasties of the chin are made after mobilization of the inferior section. The stabilization of the section in its new position could be accomplished with cortical wires, circumandibular wires, or plates and screws; prebent chin plates can be found with various levels of advancement in millimeters, and these may be used in a reverse style for setback procedures of the chin. For vertical augmentation or reduction, commonplace four-hole plates with screws could also be used, probably utilizing a bone graft, if essential. The wound is irrigated and closed in two layers, mentalis muscle and mucosa, with resorbable suture. The use of wires, pins, screws, or plate and screws for the fixation of the inferior section is widespread. Precious and associates230 evaluated the adjustments that occur as the bone remodels after a horizontal osteotomy. They beneficial that the fixation keep in mind these adjustments, especially the positioning of rigid fixation units. Plates placed along the superior border of the inferior fragment could turn into noticeable to the affected person because the bone remodels. This could also be because genioplasties are frequently accomplished at the side of other osteotomies, which makes the designation of varied complications to one explicit portion of the surgical procedure difficult. The risk of sensory loss from genioplasty alone has not been adequately evaluated, although in a single examine, it was noted that postsurgical sensory loss was found in all patients, but it was temporary, with regular sensation returning inside 12 months. Most of the literature regarding genioplasties concentrates on the soft tissue response to the skeletal motion. Two different research with follow-up of at least 1 12 months do appear to present some instability of the skeletal chin advancement. As with stability research of different osteotomies, there exists a big variation in individual relapse, and no try has been made to establish the particular etiologies. However, there are most likely many elements involved, including affected person age and the magnitude of development. There have been no research on the stability of this surgical procedure in correction not to pull on their lip in order to minimize the potential for wound dehiscence. The size of the reduce posteriorly has essential aesthetic penalties, and anegonial notching may be unaesthetic when it occurs at the junction of the distal portion of the advanced genial section and native mandible and subsequent bony remodeling that occurs in that region. Most notably, larger advancements require a larger cut to the primary or second molar area. Martinez and colleagues234 discovered that regeneration of the cortical thickness of the symphysis was considerably better in sufferers youthful than 15 years of age. They instructed that this can be useful if further surgical development of the chin is to be thought-about. Other issues, such as bone loss and an infection, have been reported, but small samples preclude any definitive conclusions regarding exact incidence. Case of elongation of the underneath jaw and distortion of the face and neck, caused by a burn, successfully treated. Report of a case of double resection for the correction of protrusion of the mandible. Treatment of open-bite by means of plastic indirect osteotomy of the ascending rami of the mandible. Surgical correction of mandibular prognathism by intra-oral subcondylar osteotomy. Oblique osteotomy of mandibular ramus-speical approach for correction of assorted kinds of facial defects and malocclusion. Correction of retrognathia by modified "C" osteotomy of the ramus and sagittal osteotomy of the mandibular physique. Ein beitrag zur chirurgischen kieferorthopadie unter berucksichtigung ihrer bedeutung fur die behandlung ang-eborener and erworbener kieferdeformitaten Uei soldaten. Modified intraoral sagittal splitting technique for correction of mandibular prognathism. Die vertikale osteotomie zur verlangerung des einseitig verkurzten aufsteigenden unterkieferastes. Total mandibular alveolar osteotomy: encouraging experiences with an infrequently indicated procedure. Histologic investigation of pulpal modifications following maxillary and mandibular alveolar osteotomies in the canine. Biological basis for vertical ramus osteotomies-a study of bone healing and revascularization in grownup rhesus monkeys. A radioisotope study of the vascular response to sagittal cut up osteotomy of the mandibular ramus. A quantitative histologic study of tissue responses to ramal sagittal splitting procedures. Revascularization and bone therapeutic after anterior maxillary osteotomy: a research utilizing grownup rhesus monkeys. Positional changes of the mandible after surgical correction of mandibular protrusion by horizontal osteotomy of the rami. Positional changes of the mandible and upper and lower anterior tooth after indirect sliding osteotomy of the mandibular rami. Mandibular development surgery: a examine of the decrease border wiring technique for osteosynthesis. Muscular and mandibular adaptation after lengthening, detachment, and reattachment of the masseter muscle. Stability two years after mandibular advancement with and without suprahyoid myotomy: an experimental examine. Vertical osteotomy vs sagittal split osteotomy of the mandibular ramus: comparability of operative and postoperative elements. Radiography of the temporomandibular joint after indirect sliding osteotomy of the mandibular rami. Treatment of temporomandibular joint dysfunction by intraoral vertical ramus osteotomy.
Order requip 0.5 mg visa
The anterior vertebral height increased 4 mm and the kyphotic deformity decreased 5 medicine 035 requip 1 mg buy with visa. In another systematic review of 69 research treatment yeast uti generic requip 1 mg line, Hulme et al59 found comparable charges of extravasation for vertebroplasty (41%) and kyphoplasty (9%), with subsequent scientific problems occurring in three. An elevated fee of cement extravasation with vertebroplasty in contrast with kyphoplasty might have clinical penalties past an elevated risk of complications. Thus, if kyphoplasty results in a decrease incidence of cement extravasation, higher short-term medical outcomes could also be expected. Compression of neural components can lead to paralysis with involvement of the spinal cord61 or radiculopathy with compromise of a neural foramen,41,62 necessitating surgical decompression. Cement may also move into venous channels and in the end result in a pulmonary embolism,65�67 which is reported to happen in 0. The higher incidence of fractures within the early postoperative interval could probably be explained by increased affected person activity and better stress secondary to a diminished degree of ache. Furthermore, the presence of 1 osteoporotic fracture can improve the danger of growing one other fracture as a lot as 12. Other potential risk components for growing adjacent-level fractures embrace cement extravasation right into a disk76 and osteoporosis secondary to steroid use. Questions for Discussion What are the indications for vertebroplasty or kyphoplasty after a compression fracture of osteoporotic backbone Since vertebroplasty was first launched for the therapy of hemangiomas, the use of vertebroplasty and kyphoplasty has evolved to embody a wide spectrum of patients. Even inside the subset of patients with osteoporosis, these procedures have been utilized to patients with very heterogeneous clinical and radiographic characteristics. Regardless of the indication, the first end result for assessing the efficacy of these procedures is pain reduction. One of the most important variables among research of vertebroplasty and kyphoplasty is the length of signs previous to treatment or, as a correlate, the age of the fracture. Voormolen et al80 carried out a prospective, randomized, controlled trial with 34 sufferers during which they in contrast vertebroplasty with optimum ache treatment (control group) in the remedy of subacute and persistent painful osteoporotic fractures, defined as higher than 6 weeks but lower than 6 months old. Roland-Morris disability scores had been considerably higher for the treatment group at both time factors. This research was graded as moderate-quality proof, as an alternative of good high quality, for a number of points. First, there have been relatively few subjects, which raises considerations in regards to the examine design being underpowered. Third, defining the "gold normal" of remedy for osteoporotic compression fractures to be optimum ache medication with out different therapies such as bracing and physical therapy is debatable. Diamond et al28 offered moderate-quality proof with a potential, nonrandomized trial evaluating vertebroplasty with conservative administration in patients with signs ranging in period from 1 to 6 weeks and a imply follow-up of 215 days. At the 6-week and 6- to 12-month follow-up points, each groups had important improvement compared with preoperative ache scores, with no difference between groups. Physical operate (Barthel index) scores followed an identical pattern, with solely the vertebroplasty group enhancing at 24 hours however both teams recognizing comparable improvement at 6 weeks and 6 to 12 months. Nakano et al27 introduced more reasonable quality evidence with a matched case-control examine, comparing vertebroplasty with conservative treatment. This study consisted of 60 sufferers with symptoms of no less than 4 weeks length and a mean follow-up of 17 months. Compared with sufferers within the control group, pain scores for these within the vertebroplasty group were significantly lower at both postoperative time factors, though the medical significance is questionable because the difference between groups is small. Kasperk et al81 performed a potential, nonrandomized, controlled trial comparing kyphoplasty with standard medical management, which generated moderate-quality proof. A total of 60 sufferers were enrolled within the examine after a minimal of 12 months of symptoms, with follow-up at three and 6 months. Together, these four trials offer moderate-quality proof that vertebroplasty and kyphoplasty, in contrast with conservative remedy, can improve ache control when signs have been present from 1 week to higher than 12 months. The outcomes of the studies by Voormolen et al80 and Diamond et al28 demonstrated that pain scores improve in 24 hours after vertebroplasty, coinciding with several different studies that provide low or very low high quality evidence that ache scores considerably improve in the first 24 hours after vertebroplasty or kyphoplasty. Other studies provide low-quality evidence that the benefits of vertebroplasty can final even longer. Spinous course of tenderness on bodily examination is incessantly thought of an inclusion criterion when choosing vertebral ranges for therapy with vertebroplasty or kyphoplasty. However, in a retrospective cohort, Gaughen et al13 offered very low high quality proof suggesting the opposite. Overall, 91% of 100 patients famous no much less than a three-point reduction in ache with an 11-point scale. Several radiographic findings have been evaluated with regard to the efficacy of vertebroplasty. The authors of a retrospective cohort of forty five patients treated with vertebroplasty demonstrated that 100 percent of patients with elevated T2 signal on magnetic resonance imaging, indicative of bone edema on the handled degree had improvement in ache, whereas 80% of sufferers without increased T2 sign famous reduced pain. Very low quality evidence does counsel that osteoporotic compression fractures related to intravertebral clefts93 and intraosseous vacuum phenomena94,ninety five are amenable to remedy with vertebroplasty. In a cohort examine providing very low quality proof, Peh et al96 checked out whether vertebroplasty is helpful with extreme compression fractures. Thirty-seven patients were recognized with vertebrae collapsed to one third or less of their authentic height. Sixty-five percent of fractures were classified as gibbus, 27% as vertebra plana, and 8% as H-shaped. At a imply follow-up of 11 months, 97% of patients had full or partial pain aid. In abstract, moderate-quality evidence means that vertebroplasty or kyphoplasty is indicated for fractures with ages various from 1 week to higher than 12 months. Low and really low high quality evidence additionally means that vertebra plana fractures and fractures with clefts or intraosseous vacuum phenomena are candidates for these remedies. Are kyphoplasty and vertebroplasty equivalent treatments for osteoporotic compression fractures As with assessing the indications for these procedures, the first outcome of interest for evaluating vertebroplasty and kyphoplasty is pain control. Grohs et al55 provided moderate-quality evidence with a potential, nonrandomized trial immediately comparing vertebroplasty and kyphoplasty. This study included a complete of 51 patients with osteoporotic vertebral compression fractures and follow-up at 1 day, 4 months, and 2 years postoperatively. First, the vertebroplasty group had a major reduction in ache scores in any respect time points, displaying there was a long-lasting effect on pain. Second, there was no statistical analysis instantly evaluating vertebroplasty and kyphoplasty scores to help the statement that kyphoplasty is superior. Any further comparisons between vertebroplasty and kyphoplasty with respect to ache discount can only be accomplished not directly between totally different research. Several studies already described present moderate-quality proof suggesting that each vertebroplasty and kyphoplasty effectively cut back pain,27,28,80,81 although the length of efficacy is variable between research.
Diseases
- Lattice corneal dystrophy type 2
- Martsolf Reed Hunter syndrome
- Cholestatic jaundice renal tubular insufficiency
- Abdallat Davis Farrage syndrome
- Free sialic acid storage disease
- Genetic diseases, inborn
- Nerve sheath neoplasm
Requip 2 mg order without a prescription
It has an interrater validity and reliability which might be comparable to pure keratin treatment purchase 0.5 mg requip free shipping earlier scales medicine 666 cheap requip 2 mg visa, and a superior predictive value for practical consequence. It additionally showed a robust correlation with the advanced biomechanical motor score system. Chicago: American Spinal Injury Association/International Medical Society of Paraplegia; 1992 3. Chicago: American Spinal Injury Association/International Medical Society of Paraplegia; 2006 four. The value of postural discount within the initial administration of closed accidents of the backbone with paraplegia and tetraplegia, I. Classification of the severity of acute spinal wire damage: implications for administration. Motor classification of spinal wire accidents with mobility, morbidity and recovery indices. Methylprednisolone or naloxone treatment after acute spinal twine injury: 1-year follow-up information. Comparison of useful and medical evaluation within the classification of persons with spinal wire damage. Scoring acute spinal wire injury: a examine of the utility and limitations of five totally different grading systems. A check of the 1992 International Standards for Neurological and Functional Classification of Spinal Cord Injury. Inter-rater reliability of the 1992 international standards for neurological and functional classification of incomplete spinal twine harm. Inter-rater reliability of motor and sensory examinations performed in accordance with American Spinal Injury Association requirements. Prediction of ambulatory performance primarily based on motor scores derived from standards of the American Spinal Injury Association. The evolution of walking-related outcomes over the primary 12 weeks of rehabilitation for incomplete traumatic spinal wire harm: the multicenter randomized Spinal Cord Injury Locomotor Trial. Neurorehabil Neural Repair 2007;21:25�35 69 eight American Spinal Injury Association Neurological Examination 29. Superiority of motor stage over single neurological stage in categorizing tetraplegia. These members of the health care group make up the first line of protection in crucial care scenarios, yet their actions remain in the background to many physicians. Their many roles include initial protection towards pores and skin breakdown, respiratory problems (pneumonia, acute respiratory misery syndrome, etc. Early preventive measures can help decrease long-term prices and lower general mortality rates. The prices are less for lower lesions involving the thoracic or lumbar space however are still substantial: nearly $1,000,000. With aggressive measures initiated early in the midst of remedy, annual and lifetime financial savings may be considerably lowered. Because of earlier interventions by paramedics, nurses, and allied health professionals there was a 40% reduction in mortality within the first 2 years postinjury. Nurses start with an preliminary assessment and are very important in serving to to maintain an airway no matter whether intubation is indicated. They are key in immobilization of the cervical spine until clearance could be established. The objective of immobilization is prevention of further neurological harm in the presence of an unstable backbone. Measures generally used in spinal immobilization are the location of a rigid cervical collar, transportation on a spine board, and proper logrolling of patients. Although these could additionally be seemingly benign interventions, pain and impairment of chest wall mobility can occur in as much as 70% of patients. In Alberta, Canada, a multidisciplinary group of well being care providers developed regional insurance policies and procedures for logrolling with and with out cervical backbone injuries. Their aim was to consider regional practices and establish and implement constant logrolling practices Table 9. Review of rehabilitative administration in the acute care setting in addition to a review of the method for selecting an applicable rehab facility. Outlined the process required to set up and implement constant logrolling practices throughout Alberta, Canada. Described the procedure and policy development aspect as nicely as the method required to educate workers. Reviewed the implementation and evaluation thereafter in an evidence-based method to enhance patient safety via a single intervention. Conclusion is ongoing means of this evaluation with the development indicating success. Description of the implementation of a stress ulcer prevention protocol at a single institution as well as a scientific evaluation of literature describing the costliness of failing to stop strain ulcers. Concluded that inside three months of implementation their Pressure Ulcer Prevention Protocol Interventions and educational program lowered the incidence of strain ulcers at their institution more than one half. Enhanced mobility may assist physical remedy and more rapid restoration of ventilatory muscle energy. Retrospective evaluate of forty eight ventilated patients with nosocomial pneumonia and matched controls. Intent was to decide if nosocomial pneumonias acquired in ventilator-dependent patients elevated mortality of extended hospitalization. Used evidence-based strategies to review present literature on the analysis of ventilator-associated pneumonia attributable to bacterial pathogens. Concluded that present literature highlights the limitation of present knowledge of this disease and underscores the need for additional studies to study advantages, dangers, and prices of diagnostic procedures and to measure the effectiveness in terms of outcomes somewhat than sensitivity and specificity. The sufferers had been stress sore free at admission and the Braden Scale was in contrast with the present Norton Scale to precisely predict patients at risk for developing strain sores. The Braden Scale in contrast favorably with the Norton in sensitivity, and the Norton Scale had an inclination to overpredict threat with a better specificity, which could lead to a greater variety of patients receiving unnecessary and costly treatments utilizing the Norton Scale. Over 50 years, respiratory points had been the number one reason for death followed by urinary and cardiovascular issues, however trends have modified over time. Concluded that with different elements being equal, over the last three decades there has been a 40% decline in mortality through the critical first 2 years postinjury. However, the decline in mortality over time within the post-2-year interval is small and never statistically significant on this research. Additional objective was to determine the incidence of thrombosis in subgroups in accordance with website of damage or presence of a particular damage.
Requip 0.5 mg purchase with mastercard
In general medicine 751 generic 0.5 mg requip fast delivery, outpatient intravenous anesthesia with airway safety can be used for isolated posterior segmental procedures medications with pseudoephedrine requip 1 mg buy with amex. A excessive palatal vault permits access to the palatal osteotomy via a transantral strategy beneath the nasal floor. A mucoperiosteal dissection beneath the superior aspect of the incision exposes the lateral maxilla, and the pterygomaxillary area is exposed by way of delicate tissue retraction in a tunneling approach. At the anterior interdental osteotomy site, conservative tunneling of the periosteum exposes the total vertical extent of the dentoalveolar segments. After retraction of the delicate tissue with pores and skin hooks and right-angle retractors, the facial interdental osteotomy could also be outlined with a small fissure bur, or it can be accomplished instantly with a skinny cement-spatula osteotome. The palatal osteotomy is completed with a small, sharp, curved osteotome directed on the junction of the vertical alveolus and the horizontal palatal shelf. A, Transantral osteotomy is made at the junction of the horizontal palate and vertical alveolar process. Next, the pterygomaxillary junction is separated with a curved osteotome utilizing a technique much like that for a complete maxillary osteotomy. The posterior dentoalveolar segment is down-fractured utilizing digital stress, and any osseous interferences may be eliminated using a bur or rongeurs. Any beforehand inaccessible medial and posterior walls of the cellular section are addressed now after mobilization and displacement of the posterior phase. Final contouring is completed while holding the splint in the secure portion of the maxilla anteriorly, after which the mandible is rotated into its right occlusal place to make certain that no distortion of the splint has occurred. A splint modification should be considered that outcomes is a barely thicker splint with transpalatal acrylic or wire reinforcement that may add rigidity to prevent inadvertent distortion of the posterior extension of the splint and to help the osseous segments postsurgically. Once the segments are ligated to the splint, the repositioned posterior maxillary segment(s) could also be fixated with interosseous wires, suspension wires, secure pin fixation, or bone plates and screws. A midline palatal incision provides entry for the elimination of bone because the posterior maxillary segment is moved medially. Meticulous surgical dissection can ensure maintenance of the integrity of the descending palatine vessels. Surgically Assisted Rapid Palatal Expansion History the idea of maxillary transverse width discrepancy correction orthodontically originated within the United States in 1860 by G. Angell in Dental Cosmos,89 where he described widening of the maxillary dental arch by opening the midpalatal suture. Bone is removed at the perpendicular plate of the palatine bone utilizing a transantral method. Lines94 and Bell and Epker95 demonstrated that increased facial skeletal resistance to growth was positioned on the zygomaticotemporal, zygomaticofrontal, and zygomaticomaxillary sutures, whereas Wertz96 hypothesized that the resistance was attributable to the zygomatic arches. This controversy regarding the specific areas of resistance in the midfacial skeleton stimulated the development of a variety of maxillary osteotomy designs to broaden the maxilla utilizing orthodontic home equipment. The benefits of its use are gradual callous distraction that permits the soft tissues to accommodate to the bony actions thereby leading to improved long-term stability. Several components must be thought of when figuring out which methodology is preferable for each individual patient. Finally, problems with price, not only from a monetary standpoint but in addition together with day with no work from work or school in addition to the psychological influence of surgical procedure, must be considered. This concept appears valid in a twodimensional drawing; nonetheless, in three dimensions, if the osteotomy is flat from lateral to medial, as growth occurs, the bone on the piriform area slides laterally over the flat floor lateral to it, and the bone in the buttress region slides laterally over the flat floor lateral to this area. Separation of the hemimaxillae is carried out by driving a skinny spatula osteotome between the central incisors within the earlier than referral for a surgical choice and the dentition has reached a maximum restrict of movement, presumably with root resorption, which might make a single-stage segmental maxillary process extra fascinating. A, Bilateral horizontal mucoperiosteal incisions are made, followed by bilateral osteotomies from the piriform rims to pterygomaxillary junctions. B�D, Division of the hemimaxillae is achieved by inserting an osteotome within the midline. The activation period can begin after 5 days and the growth equipment is activated, or turned with a special "key," according to particular directions (usually a fee and rhythm of twice-daily activations of zero. After completion of the distraction section, a consolidation period should be allowed for bony healing with the system locked in place to forestall counterclockwise rotation, using a chrome steel wire via the activation gadget or composite resin, or another material, placed to forestall device deactivation. This is usually held in place for a interval of 8 to 12 weeks after completion of bony movement. The enlargement gadget is turned three or 4 activations (1/4 mm every activation, although some gadgets are 0. Both segments are mobilized until equal mobility is seen bilaterally in each hemimaxillary phase. Some authors suggest a subtotal Le Fort I osteotomy with a horizontal osteotomy, vertical midline osteotomy, and with pterygoid and nasal septal separation. It is unclear whether or not these findings could be as important with complete cuts from the piriform to the pterygomaxillary fissure. Need for separation of the pterygomaxillary junction is, subsequently, a topic of debate. In addition, nasal septal separation from the nasal crest of the maxilla will avoid postoperative nasal septal deviation because the septum could remain attached to one of many two maxillary segments. Also, two sources of potential hemorrhage, by way of manipulation of the pterygomaxillary junction and separation of the nasal septum from the nasal crest of the maxilla, should be averted if this procedure is performed as an officebased process or on an outpatient foundation under intravenous sedation. Steroids are used routinely, but systemic antibiotics Zygomatic Osteotomy and Modified Le Fort Osteotomies As discussed in the part on anterior maxillary repositioning, sufferers with extreme midface deficiency may benefit from enhancement of the prominence of the zygoma region. Numerous strategies have been developed to increase the malar eminences and the paranasal regions, mostly utilizing bone grafts or artificial implants. Autologous grafts, from the ramus, chin, or coronoid course of, are disappointing because of resorption and the donor website morbidity. Allogeneic transplants such as lyophilized cartilage have been used with some success however are prone to migration, irritation, and resorption. B, the horizontal osteotomy is accomplished in the identical manner as the bilateral osteotomy. If alloplasts are contraindicated or declined by the patient, the zygomatic osteotomy may be a useful various. This is performed as near the lateral orbital rim as potential, and the zygoma is out-fractured gently so that an inter- positional material may be positioned in the hole to hold the zygoma in a lateral position. The interpositional material (bone graft or synthetic implant) may be stabilized in a standard style in this area. B, With out-fracturing and placement of graft materials for transverse augmentation of the malar eminence. C, Mushroom-shaped graft placement for anteroposterior and transverse augmentation of the malar eminence. These methods or modifications to these procedures have been described previously115; however, this group of maxillary osteotomies is proscribed clinically almost about their use for maxillary expansion, rotation, and torque, or yaw, movements. Experience with functionally steady plate osteosynthesis after ahead displacement of the upper jaw. The stabilization of osteotomized maxillary segments with Luhr mini-plates in secondary cleft surgery.
Buy 1 mg requip with visa
Even complaints of paresthesia within the maxilla are reported that may be because of medicine keri hilson lyrics requip 0.25 mg online larger Le Fort advancements causing delayed infraorbital re-innervation and/or bigger defects within the lateral wall of the sinus associated with continual sinusitis medications and side effects 2 mg requip buy otc. Postoperative malocclusion of the posterior dentition as a result of a deep curve of Spee and an extensive prosthetic bridge. Periodontal illness, bone loss, and calculus can typically be the cause of surgical wound infections. The geniotomy incision is the most probably to dehisce and turn into contaminated, maybe owing to age-related periodontal elements. Skeletal relapse is a typical drawback in all surgical procedure, but in orthognathic surgical procedure, this is often corrected by the orthodontist. Up to 20% relapse is reported in orthognathic surgical procedure, which might be just one mm if the skeletal change was 5 mm. Therefore, the surgeon should use techniques that reduce relapse similar to bone grafting and bolstered plating materials. This may be worsened by the surgeon bending and work-hardening the plate to match an osteotomy gap. Bone grafting the lateral wall of the maxilla is advisable owing to the restricted bone contact and prevention of sentimental tissue ingrowth. Bicortical place screws are most likely the strongest, however after they fail, the entire construct is lost. Maxillomandibular development surgical procedure results for 71 obstructive sleep apnea syndrome patients categorized by polysomnography. The success of the chosen therapy ought to be evaluated each subjectively and objectively. However, all agree that the potentially important physiologic penalties that can be life-threatening result from hypoxemia. A more affordable strategy could be to outline the concept of success in phrases of "excellent," "good" "fair," and "poor" and to keep away from utilizing the term "cured" in assessing remedy outcomes. In managing patients with extreme sleep apnea, a "treatment" is seldom achieved with a single surgical or medical treatment (tracheostomies excluded). Further observations on the potential rhythms of the cerebral cortex throughout sleep. Regularly occurring periods of eye motility and concomitant phenomena during sleep. Polygraphic examine of the episodic diurnal and nocturnal (hypnic and respiratory) manifestations of the pickwick syndrome. Obstructive sleep apnea and cephalometric roentgenograms: the position of anatomic upper airway abnormalities within the definition of abnormal breathing during sleep. Palatopharyngoplasty failure, cephalometric roentgenograms, and obstructive sleep apnea. Maxillary, mandibular, and hyoid development for remedy of obstructive sleep apnea: a evaluation of forty sufferers. Home remedy of obstructive sleep apnea with continuous positive airway stress applied through a nose-mask. The quick results of steady positive airway strain therapy on sleep pattern in patients with obstructive sleep apnea syndrome. Relief of sleep-related oropharyngeal airway obstruction by continuous insufflation of the pharynx. Reversal of obstructive sleep apnea by steady constructive airway stress applied via the nares. Management of obstructive sleep apnea: comparison of varied remedy modalities. Surgical correction of anatomic abnormalities in obstructive sleep apnea syndrome: uvulopalatopharyngoplasty. The palataopharyngoplasty operation for snoring and sleep apnea: an interim report. The effect of mandibular osteotomy in three sufferers with hypersomnia sleep apnea. Mandibular advancement combined with horizontal development genioplasty for the, 29. Maxillary, mandibular, hyoid development: an alternative alternative to tracheostomy in obstructive sleep apnea syndrome. Acute and long-term ventilatory effects of hyperoxia within the grownup sleep apnea syndrome. Therapeutic use of progesterone in alveolar hypoventilation related to obesity. The results of a nonsurgical treatment for obstructive sleep apnea: the tongue-retaining device. Inferior mandibular osteotomy and hyoid myotomy suspension for obstructive sleep apnea: a review of 55 sufferers. Maxillomandibular ad, vancement surgical procedure in 23 patients with obstructive sleep apnea syndrome. Obstructive sleep apnea syndrome: a evaluation of 306 consecutively handled surgical patients. Maxillomandibular advancement surgical procedure in a sitespecific treatment approach for obstructive sleep apnea in 50 consecutive patients. Staged surgical therapy of obstructive sleep apnea syndrome: a evaluate of 35 patients. Obstructive sleep apnea syndrome fifty-one consecutive sufferers treated by maxillofacial surgical procedure. Obstructive sleep apnea syndrome: a surgical protocol for dynamic upper airway reconstruction. Long-term skeletal stability after inflexible fixation of Lefort I osteotomies with developments. Maxillomandibular advancement surgery in obstructive sleep apnea syndrome patients: long-term surgical stability. Transnasal jet air flow is a helpful adjunct to educate fibreoptic intubation: a preliminary report. Predictability of prebent development plates for use in maxillomandibular development surgery. According to a current survey, blepharoplasty of upper and lower lids was the third mostly carried out cosmetic procedure in United States in 2008, trailing body liposuction and breast enhancement. Discrepancies between what the practitioner needs to treat and what the affected person desires to have treated can lead to suboptimal outcomes. Based on the huge quantity of data out there on the internet, most patients can be quite centered about their concerns. Therefore, proper preoperative communication and treatment planning is completely essential in order to obtain passable outcomes and a "pleased" patient. The function of this chapter is to familiarize the reader with commonly used nomenclature, surgical anatomy, patient selection, surgical execution, and potential issues associated with higher and lower lid blepharoplasty.
Requip 2 mg cheap visa
Retropharyngeal pseudomeningocele after atlanto-occipital dislocation: report of two instances medications vitamins order requip 0.25 mg on line. The lateral roentgenogram of the neck: with comments on the atlanto-odontoid-basion relationship medications you cant drink alcohol with order 2 mg requip with amex. Radiologic analysis of traumatic occipitovertebral dissociation, I: Normal occipitovertebral relationships on lateral radiographs of supine subjects. Atlanto-occipital dislocation, I: Normal occipital condyle�C1 interval in 89 kids. Transversal dislocation of the occipito-cervical joint: a explanation for cervico-occipital neuralgia [in Italian]. Severe posttraumatic craniocervical instability in the very younger affected person: report of three cases. Traumatic avulsion fracture of the occipital condyles and clivus with associated unilateral atlantooccipital distraction. Radiologic and clinical spectrum of occipital condyle fractures: retrospective review of 107 consecutive fractures in 95 patients. Type I fractures of the odontoid process: implications for atlanto-occipital instability: case report. Traumatic atlanto-occipital dislocation with survival: serial computerized tomography as an aid to analysis and reduction: a report of three circumstances. Magnetic resonance imaging of suspected atlanto-occipital dislocation: two case reports. Traumatic atlanto-occipital dislocation; with case report of a affected person who survived. Complete medulla/cervical spinal wire transection after atlanto-occipital dislocation: an extraordinary case. Posterior atlanto-occipital dislocation with fractures of the atlas and odontoid process. Dual-strap augmentation of a halo orthosis in the remedy of atlantooccipital dislocation in infants and young youngsters: technical observe. Atlanto-occipital fusion for dislocation in children with neurologic preservation: a case report. Survivors of occipitoatlantal dislocation accidents: imaging and medical correlates. Indications for surgical procedure and stabilization strategies of the occipito-cervical junction. Occipitocervical fusion: indications, technique, and long-term ends in 13 patients. Occipito-cervicothoracic backbone fusion in a patient with occipito-cervical dislocation and survival. Traumatic posterior atlantooccipital dislocation with Jefferson fracture and fracture-dislocation of C6�C7: a case report with survival. Posterior atlanto-occipital dislocation and concomitant discoligamentous C3-C4 instability with survival. Anterior C1�C2 screw fixation and bony fusion by way of an anterior retropharyngeal strategy. Atlanto-axial arthrodesis by anterior retropharyngeal intermaxillo-hyoidal method [in French]. Salvage anterior C1C2 screw fixation and arthrodesis via the lateral approach in a affected person with a symptomatic pseudoarthrosis. Biomechanical assessment of transoral plate fixation for atlantoaxial instability. Spine 2002;27:219�220 227 24 Craniocervical Disruption: Injuries of the Occiput�C1�C2 Region 123. One-stage posterior decompression and fusion utilizing a Luque rod for occipito-cervical instability and neural compression. Fusion of the craniocervical transition with "CerviFix" after survived atlanto-occipital dislocation [in German]. Cervico-occipital fusion for congenital and posttraumatic anomalies of the atlas and axis. Luxation traumatique occipitoatloidienne: interet de nouveaux signes radiologiques (a propos de deux cas). Occipitocervical fusion with posterior plate and screw instrumentation: a long-term follow-up examine. Occipitocervical arthrodesis utilizing contoured plate fixation: an early report on a flexible fixation technique. An anatomic study of the thickness of the occipital bone: implications for occipitocervical instrumentation. Biomechanical evaluation of a brand new modular rod�screw implant system for posterior instrumentation of the occipito-cervical spine: in-vitro comparison with two established implant techniques. A biomechanical evaluation of occipitocervical instrumentation: screw in contrast with wire fixation. Biomechanical analysis of five different occipito-atlanto-axial fixation strategies. Clinical experience with inflexible occipitocervical fusion in the administration of traumatic higher cervical spinal instability. Images in emergency medicine: long-term survival following full medulla/cervical spinal twine transection. Chiari I malformation related to atlanto-axial dislocation: specializing in the anterior cervicomedullary compression. Case reports: Atlantooccipital and atlantoaxial traumatic dislocation in a child who survived. Irreducible anterior atlantoaxial dislocation: one-stage treatment with a transoral atlantoaxial reduction plate fixation and fusion. Cranio-cervical stabilization of traumatic atlanto-occipital dislocation with minimal resultant neurological deficit. Novel therapy of basilar invagination resulting from an untreated C-1 fracture associated with transverse ligament avulsion. Atlantal lateral mass screws for posterior spinal reconstruction: technical notice and case sequence. Avulsion transverse ligament accidents in kids: successful treament with nonoperative management. Delayed decompression of chronic C1C2 subluxation in a pediatric patient with tetraplegia-is recovery attainable Coronally oriented vertical fracture of the axis physique: surgical therapy of a rare situation. A review of current choices and early analysis of rigid internal fixation methods. Lindsey and Zbigniew Gugala the axis is a unique second vertebra that performs a important function in upper cervical backbone movement and stability. The specialised anatomy and kinematics of the axis (in mixture with the atlas) topics it to biomechanical hundreds that can be various and considerable. These loads, when excessive, may find yourself in a selection of ligamentous and bony injuries, among which odontoid fractures are the most common. Fractures of the odontoid can account for as a lot as 20% of all cervical spine injuries.