
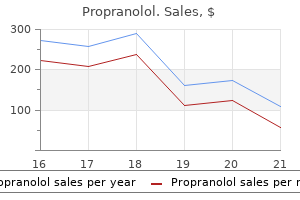
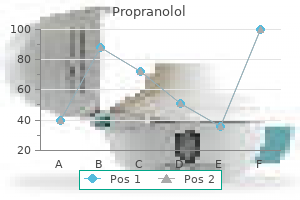
Propranolol dosages: 80 mg, 40 mg, 20 mg
Propranolol packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy propranolol 20 mg cheap
Inspect the mouth with a torch and spatula for angular stomatitis cardiovascular system labeled propranolol 40 mg free shipping, ulceration and atrophic glossitis blood vessels growing on cornea 20 mg propranolol cheap with mastercard. Ask the affected person to extend his arms and arms and look for evidence of hepatic flap. The arthropathy of haemochromatosis can also be current (a degenerative arthritis that notably involves the second and third metacarpophalangeal joints). Ask whether or not you could additional examine for hernias by asking the patient to stand and cough. If you discover a pulsatile liver, examine the cardiovascular system and significantly observe some other indicators of tricuspid regurgitation. If malignant disease is suspected, study all the node groups, the lungs and the breasts after an intensive abdominal examination. Non-haematological malignant disease that causes hepatomegaly hardly ever results in splenomegaly unless the portal vein is directly concerned. Look for bruising, pigmentation, cyanosis, jaundice, scratch marks (due to myeloproliferative disease or lymphoma) and leg ulceration (see below). Also note the presence of frontal bossing and the racial origin of the patient (thalassaemia is more frequent in folks of Asian or Greek background). Look on the nails for koilonychia (spoon-shaped nails, which are rarely seen today and which indicate iron deficiency) and the modifications of vasculitis. Pale palmar creases indicate anaemia (usually the haemoglobin level is < 90 g / L). The anterior conjunctiva ought to be distinctly redder in color except vital anaemia (<100 g / L) is current. Note any gum hypertrophy (the differential prognosis consists of acute myeloid leukaemia � especially monocytic � and scurvy), ulceration, an infection. Candida), haemorrhage, atrophic glossitis (secondary to iron, vitamin B12 or folate deficiency) and angular stomatitis. There are seven groups: submental, submandibular, jugular chain, posterior triangle, postauricular, preauricular and occipital. There are 4 major areas: central, lateral (above and lateral), pectoral (most medial) and subscapular (most inferior). Inspecting the eyes, note any jaundice, pallor or haemorrhage of the sclera, or the injected sclera of polycythaemia. Tap the backbone along with your fist for bony tenderness (which may be brought on by an enlarging marrow �. Ask to look at the legs from a neurological aspect for evidence of vitamin B12 deficiency. Remember, hypothyroidism and lead poisoning can cause anaemia and peripheral neuropathy. Finally, ask to look at the fundi (for engorged retinal vessels, papilloedema, haemorrhages, etc. Take time first to have a glance at the face for signs of thyrotoxicosis or myxoedema (see point 7 below). With the affected person sitting up and the neck totally exposed, examine for scars, swelling and prominent veins. Palpate gently from behind, with the neck flexed, feeling for any thyroid mass (Table sixteen. If a nodule is palpable, decide whether this is single or part of a multinodular goitre. Ask the patient whether or not the gland is tender (a clue to subacute thyroiditis) and notice any hoarseness of the voice (which could also be brought on by recurrent laryngeal nerve palsy). Test the sternocleidomastoid perform, as malignant disease might infiltrate this muscle. Percuss over the higher part of the manubrium from one side to the other, proper across the bone, and notice any change from resonant to boring (a signal of retrosternal extension). Auscultate over the thyroid gland for bruits (a sign of energetic thyrotoxicosis) and in addition over the carotid arteries. Examine the eyes for exophthalmos by noting the presence of sclera beneath the cornea when the affected person is trying straight ahead. Then take a look at for lid lag by asking the patient to follow your finger descending at a reasonable price. Iodine-induced (after previous iodine deficiency) � termed the Jod-Basedow phenomenon 5. Hydatidiform mole or choriocarcinoma (human chorionic gonadotrophin secretion � rare) three. In thyrotoxicosis the inferior indirect muscle energy is misplaced first, then convergence is affected, adopted by the opposite muscular tissues. Feel the radial pulse for sinus tachycardia, atrial fibrillation or a collapsing pulse. Ask to study the chest for proof of gynaecomastia (in men) and the guts for an ejection systolic murmur and signs of congestive cardiac failure. It is examined by tapping over the facial nerve 3�5 cm below and in entrance of the ear. Chronic illness (direct or erythropoietin-mediated depressive effect on bone marrow) Folate deficiency secondary to bacterial overgrowth Pernicious anaemia related to myxoedema Iron deficiency in girls owing to menorrhagia Haemolysis secondary to hypercholesterolaemia-induced spur-cell anaemia ht Test for delayed leisure of the biceps jerk. Look at the tongue, which can be swollen, then ask the affected person to let you know his or her name and tackle, and notice any hoarseness or slowness of speech. Examine them neurologically, starting with the ankle jerks, noting notably any evidence of gradual relaxation, which is greatest seen with the patient kneeling on a chair. Then examine for peripheral neuropathy and look for different uncommon neurological abnormalities (Table 16. The patient may be of brief stature (failure of development hormone secretion before development is complete) with no secondary sexual traits (gonadotrophin failure before puberty). Multiple fantastic skin wrinkles across the eyes and mouth are characteristic of progress hormone deficiency. Look carefully for a hypophysectomy scar on the forehead near the inner canthus of the attention. Lay the patient down and search for loss of pubic hair and testicular atrophy (in males testes are small and gentle � the normal dimension is 15�25 mL in volume). Note central weight problems with peripheral sparing and have a glance at the pores and skin for bruising, atrophy and pigmentation of extensor areas. Test for proximal myopathy of the arms and also of the legs (initially by getting the affected person to squat). Look for kyphoscoliosis and tap the spine for bony tenderness as a end result of osteoporotic vertebral crush fractures.
40 mg propranolol purchase otc
It projects to the dorsal and ventral premotor cortices and to the medial motor space cardiovascular disease and obesity 80 mg propranolol trusted, in all probability to the supplementary eye subject adjacent to the supplementary motor space proper cardiovascular accident cheap 80 mg propranolol mastercard. It initiatives prominently to the superior colliculus, the pontine gaze centre inside the pontine reticular formation and other oculomotor-related nuclei in the brain stem. Destructive lesions of the frontal eye subject cause ipsilateral conjugate deviation of the eyes, whereas stimulation, corresponding to with an epileptic discharge, induces contralateral deviation. A 75-year-old, right-handed man with a long historical past of hypertension and hypercholesterolemia is admitted to the hospital after awakening with left-sided weakness. Head and eyes are deviated to the best, and he has a left hemiplegia and left hemihypaesthesia. Subsequent examinations continue to doc head and eye deviations to the proper. Four days after admission, the head deviation has improved considerably, as has spontaneous eye movement to the left of the midline. Over a period of several days, the gaze deviation usually improves and ultimately resolves. Area 24 within the cingulate gyrus adjoining to area 6 incorporates several motor areas, that are termed cingulate motor areas. An additional useful subdivision, the pre�supplementary motor area, lies anterior to the supplementary motor area on the medial floor of the cortex. For purposes of this discussion, these further medial motor areas are included with the supplementary motor cortex. The supplementary motor area receives its major thalamic enter from the anterior a part of the ventral lateral nucleus, which in turn is the major recipient of fibres from the internal segment of the globus pallidus. Additional thalamic afferents are from the ventral anterior nucleus; the intralaminar nuclei, notably the centrolateral and centromedial nuclei; and the mediodorsal nucleus. The supplementary motor cortex receives connections from widespread regions of the ipsilateral frontal lobe, including the first motor cortex; the dorsal premotor space; the dorsolateral and ventrolateral prefrontal, medial prefrontal and orbitofrontal cortex; and the frontal eye subject. These connections are reciprocal, however the main ipsilateral efferent pathway is to the motor cortex. Parietal lobe connections of the supplementary motor cortex are with superior parietal area 5 and presumably inferior parietal space 7b. Contralateral connections are with the supplementary motor area and motor and premotor cortices of the contralateral hemisphere. Subcortical connections, apart from with the thalamus, cross to the striatum, subthalamic nucleus, pontine nuclei, brain stem reticular formation and inferior olivary nucleus. The supplementary motor space makes a considerable contribution to the corticospinal tract, contributing as a lot as 40% of the fibres from the frontal lobe. The supplementary motor space contains a illustration of the body in which the leg is posterior and the face anterior, with the upper limb between them. Its role in the control of movement includes primarily complex duties, 289 Chapter 16 Section V / the Cerebrum which require temporal organization of sequential actions and retrieval of motor memory. The penalties of injury to the supplementary motor space bear some putting similarities to the results of basal ganglia dysfunction; akinesia is common, and there could additionally be issues with the efficiency of sequential, complex movements. Stimulation of the supplementary motor area in conscious sufferers has been reported to elicit the feeling of an urge to move or the sensation that a movement is about to occur. A region anterior to the supplementary motor area for face representation is important in vocalization and speech manufacturing. In non-human primates, two subdivisions of the lateral prefrontal cortex are recognized: a dorsal space equal to space 9 and maybe together with the superior a part of area forty six, and a ventral area consisting of the inferior part of space forty six and space 45. Both the dorsolateral and ventrolateral prefrontal areas obtain their main thalamic afferents from the mediodorsal nucleus, and there are extra contributions from the medial pulvinar, the ventral anterior nucleus and the paracentral nucleus of the anterior intralaminar group. The dorsolateral area receives long affiliation fibres from the posterior and center superior temporal gyrus, together with auditory association areas; from parietal area 7a; and from much of the middle temporal cortex. From within the frontal lobe it also receives projections from the frontal pole (area 10) and from the medial prefrontal cortex (area 32) on the medial floor of the hemisphere. It tasks to the supplementary motor area, the dorsal premotor cortex and the frontal eye subject. Commissural connections are with the homologous area and with the contralateral inferior parietal cortex. The ventrolateral prefrontal area receives lengthy affiliation fibres from areas 7a and 7b of the parietal lobe, auditory affiliation areas of the temporal operculum, the insula and the anterior part of the lower financial institution of the superior temporal sulcus. From inside the frontal lobe it receives fibres from the anterior orbitofrontal cortex and initiatives to the frontal eye subject and the ventral premotor cortex. The cortex of the frontal pole (area 10) receives thalamic input from the mediodorsal nucleus, the medial pulvinar and the paracentral nucleus. It is reciprocally related with the cortex of the temporal pole, the anterior orbitofrontal cortex and the dorsolateral prefrontal cortex. The orbitofrontal cortex connects with the mediodorsal, anteromedial, ventral anterior, medial pulvinar, paracentral and midline nuclei of the thalamus. Cortical affiliation pathways come from the inferotemporal cortex, the anterior superior temporal gyrus and the temporal pole. Within the frontal lobe, it has connections with the medial prefrontal cortex, the ventrolateral prefrontal cortex and medial motor areas. Commissural and different connections observe the final sample for all neocortical areas. The medial prefrontal cortex is linked with the mediodorsal, ventral anterior, anterior medial pulvinar, paracentral, midline and suprageniculate� limitans nuclei of the thalamus. Within the frontal lobe, it has connections with the orbitofrontal cortex and the medial motor areas of the dorsolateral prefrontal cortex. Information on the detailed functions of the subregions of the prefrontal cortex is sparse. The dorsolateral prefrontal cortex is necessary for spatial processing of afferent data and for the organization of self-ordered working memory duties, including verbal working memory. The ventrolateral prefrontal cortex is concerned with the mnemonic processing of objects. Evidence from surgical lesions (prefrontal lobotomy) or pathological harm suggests a task for the prefrontal cortex within the appreciation or understanding of time, the normal expression of feelings (affect) and the ability to predict the consequences of actions. Both hemispheres interact in these features, so deficits following unilateral harm could additionally be relatively slight. The medial prefrontal cortex as a complete is essential in auditory and visual associations, and widespread changes in prefrontal activation are associated with calculating, considering and choice making. On the medial side of the hemisphere, its boundary with the occipital lobe is clearly demarcated by the deep parieto-occipital sulcus. On the lateral facet of the hemisphere, its boundaries with the occipital and temporal lobes are much less distinct and somewhat arbitrary. The inferior boundary is the posterior ramus of the lateral fissure and its imaginary posterior prolongation. Although he denies any problems, his spouse indicates that he has modified in a selection of respects prior to now year. On examination, he seems matted, apathetic and disinhibited and has marked difficulty with government capabilities.
Generic 20 mg propranolol
The major afferent projections to the striatum are shown on the left cardiovascular system for nurses discount 40 mg propranolol mastercard, and the major efferent projections from the striatum are shown on the best cardiovascular system introduction purchase propranolol 40 mg without a prescription. This name refers to the fact that these striatal neurones affect the exercise of basal ganglia output neurones within the medial pallidum by way of the intermediary of the subthalamic nucleus. Pars lateralis (A9) Mesostriatal axons to dorsal striatum To: superior colliculus and thalamus Crus cerebri Mesostriatal axons to dorsal striatum Mesolimbic axons to ventral striatum, and prefrontal and limbic cortices Paranigral nucleus (ventral tegmental group A10) Pars compacta (A9) Pars reticulata Striatonigral (comb) fibres. A second outflow is established from the striatum to the pars reticulata of the substantia nigra. This also has each direct and oblique elements, via the lateral pallidum and subthalamic nucleus. The ventral striatum is the primary target of cortical afferents from limbic cortices, including allocortex, and from limbic-associated areas. Thus, the hippocampus (through the fornix) and the orbitofrontal cortex (through the inner capsule) project to the nucleus accumbens, and the olfactory, entorhinal, anterior cingulate and temporal visual cortices project 252 Chapter 14 / Basal Ganglia Reticular nucleus Caudate nucleus Centromedian nucleus Stria medullaris Internal capsule Third ventricle Thalamostriatal fibres Thalamic fasciculus H1 Lenticular fasciculus H2 Fornix Putamen Lateral Optic tract Subthalamic nucleus Ansa lenticularis Medial Subthalamic fasciculus Globus pallidus. The contiguities of the cortical areas, which project to the ventral striatum and neighbouring dorsal striatum, emphasize the imprecise nature of the boundaries between the 2 divisions. All the cortical regions overlap and abut each other, they usually project to neighbouring components of the dorsal striatum in addition to to the ventral striatum. The fundus striati and ventromedial caudate nucleus abut the olfactory tubercle and nucleus accumbens. This continuity of the ventral and dorsal striata, as revealed by the preparations of corticostriate projections, is reinforced by consideration of the aminergic inputs to the ventral striatum. The dopamine projections represent the so-called mesolimbic dopamine pathway, which additionally initiatives to the septal nuclei, hippocampus, amygdala and prefrontal and cingulate cortices through the medial forebrain bundle. In the latter case, the connection is each direct and indirect via the subthalamic nucleus. The projections from the pars reticulata are as described for the dorsal system, however axons from the ventral pallidum attain the thalamic mediodorsal nucleus (which projects to the cingulate and prefrontal association cortex) and midline nuclei (which project to the hippocampus). The brain areas beyond the basal nuclei, substantia nigra and subthalamic nucleus, to which both ventral and dorsal techniques seem to project, are due to this fact the prefrontal affiliation and cingulate cortices and the deep superior colliculus. The nucleus accumbens receives a dopaminergic innervation from the midbrain ventral tegmental space (cell group A10). It is believed to represent the neural substrate for the rewarding effects of a number of classes of medication of abuse and is therefore a major determinant of their addictive potential. The experimental remark that the locomotor-activating effects of psychomotor stimulant medicine such as amphetamine and cocaine (which act presynaptically on dopaminergic neurones to improve dopamine launch or block its reuptake, respectively) are depending on dopamine transmission within the nucleus accumbens led to the hypothesis that the reinforcing or rewarding properties of these drugs are mediated by the mesolimbic dopamine system. The globus pallidus lies medial to the putamen and lateral to the internal capsule. It consists of two segments, lateral (external) and medial (internal), that are separated by an inner medullary lamina and have considerably different connections. Both segments obtain large numbers of fibres from the striatum and subthalamic nucleus. The lateral section projects reciprocally to the subthalamic nucleus as a part of the indirect pathway. The medial segment is taken into account to be a homologue of the pars reticulata of the substantia nigra, with which it shares comparable mobile and connectional properties. Together, these segments represent the main output of the basal ganglia to different ranges of the neuraxis, principally to the thalamus and superior colliculus. The cell density of the globus pallidus is less than one-twentieth that of the striatum. The dendritic fields are discoid, with planes at proper angles to incoming striatopallidal axons, every of which potentially contacts many pallidal dendrites en passant. This association, coupled with the diameters of the dendritic fields (>500 �m), means that a precise topographical group is unlikely throughout the pallidum. Those projecting to the lateral segment represent the beginning of the so-called indirect pathway. Efferent axons from neurones within the lateral section cross through the interior capsule in the subthalamic fasciculus and journey to the subthalamic nucleus. Striatopallidal axons destined for the medial pallidum represent the socalled direct pathway. In every case, pathways established by way of the pallidum are distinguished from those passing by way of the substantia nigra pars reticulata. The former runs across the anterior border of the internal capsule, and the latter penetrates the capsule directly. Having traversed the interior capsule, each pathways unite in the subthalamic region, where they follow a horizontal hairpin trajectory and turn upward to enter the thalamus as the thalamic fasciculus. Within the thalamus, pallidothalamic fibres end within the ventral anterior and ventral lateral nuclei and within the intralaminar centromedian nucleus. These, in turn, project excitatory (presumed glutamatergic) fibres primarily to the frontal cortex, including the first and supplementary motor areas. The medial pallidum additionally initiatives fibres caudally to the pedunculopontine nucleus. This lies on the junction of the midbrain and the pons, near the superior cerebellar peduncle, and corresponds approximately to the physiologically identified mesencephalic locomotor region. The substantia nigra is a nuclear complex deep to the crus cerebri in each cerebral peduncle of the midbrain. The pars compacta, along with the smaller pars lateralis, corresponds to dopaminergic cell group A9. With the retrorubral nucleus (group A8), it makes up a lot of the dopaminergic neurone population of the midbrain and is the supply of the mesostriatal dopamine system that tasks to the striatum. The pars compacta of each aspect is steady with its reverse counterpart by way of the ventral tegmental dopamine group A10, which is sometimes generally recognized as the paranigral nucleus. This is the source of the mesolimbic dopamine system, which provides the ventral striatum and neighbouring components of the dorsal striatum, as properly as the prefrontal and anterior cingulate cortices. The dopaminergic neurones of the pars compacta (group A9) and paranigral nucleus (ventral tegmental group A10) also comprise cholecystokinin or somatostatin. Examination demonstrates a moderately demented lady who displays facial grimacing and random choreic actions of her limbs and trunk. She displays motor impersistence, exemplified, for instance, by a so-called serpentine tongue. Cortical atrophy may be superior, and ventriculomegaly is at times putting, reflecting both cortical and caudate atrophy. Late in the midst of the disease, because the striatum is severely affected, the chorea becomes less apparent and the affected person could develop a relatively akinetic state. Section through the cerebral hemisphere demonstrating marked atrophy of the caudate nuclei (arrows), with compensatory enlargement of the lateral ventricles. Family members describe psychiatric symptoms such as despair and emotional lability previous the onset of neurological symptoms; he has additionally exhibited frankly psychotic behaviour. Imaging demonstrates symmetric ventricular enlargement with widespread atrophic adjustments, most pronounced within the basal ganglia and thalamus; the putamen is very involved, with striking vacuolization.
Purchase propranolol 40 mg on-line
It additionally provides tibialis posterior cardiovascular workout plan propranolol 20 mg generic with visa, the proximal tibiofibular joint and the tibia and provides off an interosseous department that descends close to the fibula to attain the distal tibiofibular joint capillaries under tongue purchase propranolol 80 mg on-line. Muscular branches in the leg, both independently or by a typical trunk, supply soleus (on its deep surface), tibialis posterior, flexor digitorum longus. The course of the common peroneal nerve can be indicated by a line from the apex of the popliteal fossa, passing distally, medial to the biceps tendon, to the again of the head of the fibula, the place the nerve may be rolled against the bone. Two accompany the superior and inferior lateral genicular arteries and will arise in frequent. The third, the recurrent articular nerve, arises close to the termination of the widespread peroneal nerve. It ascends with the anterior recurrent tibial artery through tibialis anterior and supplies the anterolateral part of the knee joint capsule and the proximal tibiofibular joint. Cutaneous Branches - the two cutaneous branches, often from a common trunk, are the lateral sural and sural speaking nerves. The lateral sural nerve (lateral cutaneous nerve of the calf) supplies the skin on the anterior, posterior and lateral surfaces of the proximal leg. The sural speaking nerve arises close to the pinnacle of the fibula and crosses the lateral head of gastrocnemius to join the sural nerve. The frequent peroneal nerve is comparatively unprotected as it traverses the lateral side of the neck of the fibula and is definitely compressed at this site. The nerve may also turn into entrapped between the attachments of peroneus longus to the head and shaft of the fibula. Traction lesions can accompany dislocations of the lateral compartment of the knee and are most probably to happen if the distal attachments of biceps and the ligaments that insert into the fibular head are avulsed, probably with a small a half of the fibular head. Examination reveals weakness of ankle dorsiflexion and extensor hallucis longus and eversion of the foot; nonetheless, inversion and plantar flexion are regular, and the ankle reflex is preserved. Because the nerve divides at the fibular neck into the superficial and deep peroneal nerves, lesions damaging the nerve at this stage could harm the main trunk of the nerve or either of its branches. A lesion of the superficial branch causes weakness of foot eversion with sensory loss on the lateral side of the leg, which extends onto the dorsum of the foot. The superficial peroneal nerve (superficial fibular nerve) begins at the common peroneal bifurcation. It is at first deep to peroneus longus and passes anteroinferiorly between the peronei and extensor digitorum longus to pierce the deep fascia in the distal third of the leg, the place it divides into medial and lateral branches. Between the muscle tissue it supplies peroneus longus, peroneus brevis and the skin of the lower leg. The medial branch passes anterior to the ankle and divides into two dorsal digital nerves: one provides the medial facet of the nice toe, and the other provides the adjoining sides of the second and third toes. It divides into dorsal digital branches that offer the contiguous sides of the third to fifth toes and the skin of the lateral side of the ankle, the place it connects with the sural nerve. Both branches, particularly the lateral, are at risk through the placement of portal incisions for arthroscopy. Branches of the superficial peroneal nerve provide the dorsal skin of all the toes besides that of the lateral side of the fifth toe (supplied by the sural nerve) and the adjoining sides of the good and second toes (supplied by the medial terminal department of the deep peroneal nerve). Some of the lateral branches of the superficial peroneal nerve are regularly absent and are replaced by sural branches. The superficial peroneal nerve may be subject to entrapment as it penetrates the deep fascia of the leg. It may also be involved in compartment syndrome affecting the lateral compartment. The deep peroneal nerve (deep fibular nerve) begins at the common peroneal bifurcation, between the fibula and the proximal part of peroneus longus. It passes obliquely ahead, deep to extensor digitorum longus, to the entrance of the interosseous membrane and reaches the anterior tibial artery within the proximal third of the leg. It descends with the artery to the ankle, dividing there Lesions of the Tibial Nerve the tibial nerve is vulnerable to direct injury within the popliteal fossa, where it lies superficial to the vessels at the degree of the knee. It may be broken in compartment syndrome affecting the deep flexor compartment of the calf. The nerve could also be entrapped beneath the flexor retinaculum at the ankle, resulting in tarsal tunnel syndrome. She has paraesthesia of the complete sole of the foot, along with medial ankle ache. On examination, she displays decreased sensation to pinprick on the sole, excluding the heel and the balls of all of the toes. Discussion: Symptoms consisting of ankle pain, foot ache or each, with or without paraesthesia of the sole of the foot, are the outcome of damage to the tibial nerve or its branches throughout the tarsal tunnel. The tibial nerve passes under the flexor retinaculum under the medial malleolus and divides into the calcaneal and plantar nerves. The distal branches of the nerve-the medial and lateral plantar nerves-travel beneath the flexor retinaculum on the ankle and may be entrapped there. The medial plantar nerve is the bigger department, supplying sensation to the anterior two-thirds of the medial sole of the foot and between the balls of all however the lateral fourth toe and the fifth toe, and together with the pores and skin across the toenails. It also gives branches to abductor hallucis, flexor digitorum brevis, flexor hallucis brevis and first lumbrical muscle. If the entrapment or harm is excessive sufficient, the calcaneal nerve can also be entrapped, inflicting numbness and paraesthesia of the medial sole and heel. Tarsal tunnel syndrome is an uncommon explanation for foot pain, usually caused by exterior compression (tight footwear, a decent cast) or trauma. Thickening of the flexor retinaculum or fibrosis around the nerve can also trigger the dysfunction, as can a variety of mass lesions in the tarsal tunnel, including synovial cysts, schwannomas or lipomas, or muscular hypertrophy. Lesions of the Common Peroneal Nerve Superficial Peroneal Nerve Branches Common Peroneal Nerve Lesions of the Superficial Peroneal Nerve the frequent peroneal nerve (common fibular nerve) is roughly half the size of the tibial nerve and is derived from the dorsal branches of the fourth and fifth lumbar and first and second sacral ventral rami. It descends obliquely alongside the lateral aspect of the popliteal fossa to the fibular head, medial to biceps femoris. The nerve then passes into the anterolateral muscle compartment through a decent opening in the thick fascia overlying tibialis anterior. It curves lateral to the fibular neck, deep to peroneus longus, and divides into superficial and deep peroneal nerves. Deep Peroneal Nerve 362 Chapter 20 / Lumbar Plexus and Sacral Plexus into lateral and medial terminal branches. It then passes distal to the lateral malleolus alongside the lateral side of the foot and little toe, supplying the overlying skin. It connects with the posterior femoral cutaneous nerve within the leg and with the superficial peroneal nerve on the dorsum of the foot. The floor marking on the ankle is a line parallel to the calcaneal tendon halfway between the tendon and the lateral malleolus. Rather just like the radial nerve on the wrist, the sural nerve tends to type painful neuromas. Branches the deep peroneal nerve supplies muscular branches to tibialis anterior, extensor hallucis longus, extensor digitorum longus and peroneus tertius, as properly as an articular department to the ankle joint. The lateral terminal branch crosses the ankle deep to extensor digitorum brevis, enlarges as a pseudoganglion and provides extensor digitorum brevis. From the enlargement, three minute interosseous branches supply the tarsal and metatarsophalangeal joints of the center three toes; the primary branch additionally supplies the second dorsal interosseous.
Propranolol 40 mg order overnight delivery
Transoral endoscopy is mainly a postrhinoscopic approach that offers the examiner with a wonderful overview of the nasopharynx cardiovascular disease youth risk factors purchase propranolol 40 mg with visa. Transoral endoscopic technique: With the tongue pulled ahead (to enlarge the area between the taste bud and posterior pharyngeal wall) arteries 60 blocked purchase propranolol 80 mg overnight delivery, the endoscope is introduced into the oral cavity over the left mandib- ular enamel and superior past the uvula to the posterior wall of the pharynx. Oropharynx Most structures of the oropharynx can be evaluated through the examination of the oral cavity. The palatine tonsils are evaluated for their symmetry, mobility, and for the presence of any coatings or ulcerations. Hypopharynx Clinical examination of the hypopharynx (mirror examination, endoscopy) is carried out concurrently with the examination of the larynx (see pp. Flexible esophagoscopy may be performed beneath local anesthesia, is usually nicely tolerated, and permits for concomitant examination of the abdomen and duode-. Posterior rhinoscopy the tongue is fastidiously depressed with a tongue blade, and then a small, prewarmed mirror is launched between the soft palate and posterior pharyngeal wall. Structures that might be evaluated with this system embrace the posterior ends of the turbinates, the choanae, the posterior margin of the vomer, and the assorted constructions of the nasopharynx. Rigid esophagoscopy provides a greater overview, significantly when on the lookout for overseas our bodies, as a end result of the advancing rigid scope tends to flatten out the mucosal lining, making it simpler to detect trapped overseas objects. Another conventional radiographic approach, used primarily in patients with equivocal swallowing disorders, is high-speed cineradiography. This approach can be utilized to consider the different phases of swallowing with high temporal resolution (approximately 50 images per second). Modern endoscopic strategies using a high-intensity gentle source, together with the brand new sectional imaging modalities, have introduced significant enhancements, significantly in the early detection of nasopharyngeal lesions. Diseases of the nasopharynx can have strikingly completely different causes at totally different ages. Because lesions of the nasopharynx are troublesome to study and should produce nonspecific symptoms, malignant tumors in particular are apt to go undetected Adenoids Synonyms: polyps, adenoid vegetations "Adenoids," the common term for hyperplasia of the pharyngeal tonsil, is a very widespread condition in children 3�6 years of age. The proliferation of lymphatic tissue on this region is so widespread in youngsters that it could possibly hardly be thought of an abnormal condition, and practically all children have a point of adenoid hypertrophy due to the immunologic exercise of that tissue. Not occasionally, the presence and severity of adenoidal symptoms depend on the relationship between the size of the nasopharynx and that of the adenoids. Clinical manifestations: Common symptoms of adenoids are persistent nasal airway obstruction ("mouth breathing,". Also, many small sufferers have frequently recurring infections of the nose and paranasal sinuses with otitis media and persistent impairment of eustachian tube ventilation, brought on for example by adenoid tissue obstructing the tubal orifices. Finally, chronic mouth respiration can result in maxillary deformity and dental malalignment. Many of these small sufferers also have enlarged tonsillar lymph nodes at the mandibular angle. Often it will show retraction of the tympanic membrane or a middle ear effusion ensuing from continual impairment of eustachian tube ventilation, with adverse stress within the center ear. Additionally, hearing should be examined in adenoid patients (pure-tone audiogram, see p. Treatment: the treatment of abnormally enlarged adenoids mainly consists of surgical elimination of the adenoids underneath common endotracheal anesthesia (adenotomy, adenoidectomy). In patients with concomitant middle ear effusion, paracentesis must be performed in the same sitting or a ventilation tube must be inserted for drainage (see p. Benign Tumors Juvenile Angiofibroma Epidemiology: Benign tumors of the nasopharynx are uncommon. The most common of these is juvenile angiofibroma, which accounts for lower than zero. Symptoms: Typical signs are obstructed nasal respiratory, recurrent epistaxis, headache, impaired eustachian tube air flow with center ear effusion, and conductive hearing loss due to obstruction of the eustachian tube orifice. Diagnosis: the typical endoscopic appearance is that of a well-circumscribed, vascularized mass. Preoperative embolization of the feeding vessels (usually the maxillary artery) ought to be carried out to reduce the depth of intraoperative bleeding. Symptoms: Early symptoms of nasopharyngeal malignancies are unilateral conductive hearing loss with center ear effusion. Any persistent center ear effusion of long duration in an adult patient with no prior history of middle ear illness is suspicious for a tumor and must be investigated accordingly. Cervical lymph-node metastasis, usually involving the nodes at the mandibular angle, is one other frequent initial discovering. Features of advanced illness include nasal airway obstruction, recurrent epistaxis, headaches, and cranial nerve palsies. Malignant Tumors Epidemiology: Carcinomas of squamous-cell origin account for the nice majority of malignant nasopharyngeal tumors. A fundamental distinction is drawn between squamous cell carcinomas and lymphoepithelial carcinomas (Schmincke tumor). Much much less widespread tumors of this region are adenocarcinoma, adenoid cystic carcinoma, malignant melanoma. Nasopharyngeal malignancies can have a selection of appearances ranging from a easy, well-circumscribed tumor floor to mucosal ulcerations. Otomicroscopy reveals unilateral tympanic membrane retraction and a center ear effusion because of impaired eustachian tube air flow. Treatment: the therapy of alternative for many nasopharyngeal carcinomas is main high-voltage radiotherapy, because most of those tumors are very radiosensitive and the unfavorable tumor location and rapid invasion of the cranium base preclude healing surgery in lots of cases. Nasal flooring c Tumor a Postrhinoscopic endoscopy demonstrates a mass that has obstructed the nasopharynx. Lesions of the oropharynx also can contribute to the development of sleep-related respiratory disorders, notably obstructive sleep apnea. Tumors, particularly malignancies, are far much less frequent on this area however should still be considered within the differential prognosis, particularly when certain threat components are present (heavy smoking, Injuries and Foreign Bodies Scalds and Corrosive Injuries Etiology: the unintentional consuming of hot liquids by kids can cause severe scalding of the lips, oral cavity, and oropharynx. Corrosive accidents are more frequent in adults due to the ingestion of caustic liquids with suicidal intent. Symptoms: the dominant scientific signs are severe ache, particularly on swallowing, and elevated salivation. Subsequent blistering could happen, followed by the formation of a whitish fibrin coating. Further exams are aimed toward excluding injuries at decrease levels of the alimentary tract and within the mediastinum. A chest radiograph ought to at all times be obtained (to check for mediastinal widening due to esophageal perforation). An early, cautious endoscopic examination may be performed in order that the extent of the esophageal injury may be precisely assessed. Treatment: the preliminary therapy for scalds and corrosive injuries is to rinse the oral cavity with cold water. If the lips are affected, they want to be handled with a corticosteroid-containing ointment. Patients with more extreme accidents can additionally be treated with systemic corticosteroids, antibiotics, and analgesics. Foreign Bodies Foreign our bodies in the oropharynx are mostly positioned in the tonsils and on the tongue base.
Cuckoo Pint (Arum). Propranolol.
- Colds, throat swelling (inflammation), cough, and stimulating sweating.
- How does Arum work?
- Are there safety concerns?
- What is Arum?
- Dosing considerations for Arum.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96242
Propranolol 40 mg overnight delivery
Medial branches of the lower six thoracic dorsal rami are distributed primarily to multifidus and longissimus thoracis; occasionally they give filaments to the skin in the median region cardiovascular system equations 40 mg propranolol buy fast delivery. They run by way of or deep to longissimus thoracis to the interval between it and iliocostalis cervicis blood vessels close to skin generic propranolol 20 mg visa, supplying these muscle tissue and levatores costarum; the decrease five or six additionally give off cutaneous branches that pierce serratus posterior inferior and latissimus dorsi according to the costal angles. The lateral branches of a variable number of upper thoracic rami also supply the pores and skin. The lateral department of the twelfth sends a filament medially alongside the iliac crest, then passes all the method down to the pores and skin of the anterior part of the gluteal area. Medial cutaneous branches of the thoracic dorsal rami descend for a lengthy way close to the vertebral spines earlier than reaching the pores and skin. Lateral branches descend for a considerable distance-as much because the breadth of four ribs-before they become superficial; for instance, the department of the twelfth thoracic reaches the skin only slightly above the iliac crest. Subluxation of the interchondral joints between the decrease costal cartilages may lure the intercostal nerves, causing referred abdominal ache. The dorsal cutaneous branch of an intercostal nerve can become entrapped because it penetrates the fascia of erector spinae. In the emergency room, her electrocardiogram and cardiac enzymes are regular, however she is admitted for remark. Pain persists in the identical distribution the subsequent morning, but a number of raised vesicular lesions are now famous within the left thoracic area within the distribution of the T6 dermatome, and the affected person is exquisitely sensitive to delicate cutaneous stimulation there. Herpes zoster virus stays dormant in dorsal root ganglia following an infection with chickenpox, generally for a few years; it could be reactivated in immunocompromised individuals or within the non-immunocompromised elderly. Pain usually precedes the skin lesions and follows a dermatomal distribution in one or several adjacent dermatomes. The appearance of vesicular lesions in the identical distribution clearly identifies the cause. The motor nerve and even the spinal cord may be involved, resulting in the appearance of an acute radiculopathy, typically leaving the affected person with weak point and atrophy in that nerve root distribution. In some patients, severe and incapacitating ache lingers-so-called postherpetic neuralgia. The lumbar plexus lies deep inside psoas major, anterior to the transverse processes of the primary three lumbar vertebrae. The sacral plexus lies within the pelvis on the anterior floor of piriformis, deep to the pelvic fascia, which separates it from the inferior gluteal and pudendal vessels. The lumbosacral trunk (L4 and L5) emerges medial to psoas main and lies on the ala of the sacrum earlier than crossing the pelvic brim to be part of the anterior main ramus of S1. It ends beneath the flexor retinaculum by dividing into the medial and lateral plantar nerves. Its cutaneous space of provide, including its terminal branches, consists of the back of the calf, the whole of the only, the lateral border of the foot and the medial and lateral sides of the heel. It arises from the posterior divisions of the second to fourth lumbar ventral rami, descends through psoas major and emerges on its lateral border to cross between psoas and iliacus and enter the thigh behind the inguinal ligament and lateral to the femoral sheath. Its terminal branches kind in the femoral triangle roughly 2 cm distal to the inguinal ligament. In the abdomen the nerve provides small branches to iliacus and a department to the proximal part of the femoral artery. It subsequently supplies a large cutaneous space on the anterior and medial thigh and medial leg and foot and provides articular branches to the hip and knee. It arises from the anterior divisions of the second to fourth lumbar ventral rami, descends through psoas major and emerges from its medial border at the pelvic brim. It crosses the sacroiliac joint behind the common iliac artery and lateral to the interior iliac vessels, runs alongside the lateral pelvic wall on obturator internus and enters the thigh through the higher part of the obturator foramen. Near the foramen it divides into anterior and posterior branches, separated at first by a half of obturator externus and extra distally by adductor brevis. It offers articular branches to the hip and knee and may supply pores and skin on the medial thigh and leg. The sciatic nerve is the nerve of the posterior compartment of the thigh and, via its major branches, of all of the compartments of the lower leg and foot. It enters the lower limb via the larger sciatic foramen beneath piriformis and descends between the larger trochanter and the ischial tuberosity. The precise level of division could be very variable as a end result of the tibial and common peroneal nerves are structurally separate and solely loosely related all through their proximal course. The sciatic gives off articular branches that offer the hip joint by way of its posterior capsule (these are typically derived immediately from the sacral plexus) and the knee joint. All the hamstring muscle tissue, together with the ischial part of adductor magnus however not the quick head of biceps femoris, are provided by the medial (tibial) component of the sciatic nerve. It descends alongside the back of the thigh and popliteal fossa to the distal border of popliteus, then passes anterior to the arch of soleus with the popliteal artery and continues into the leg. In the popliteal fossa it lies lateral to the the widespread peroneal nerve (common fibular nerve) is derived from the posterior division of the sacral plexus. It descends obliquely along the lateral facet of the popliteal fossa to the fibular head, lying between the tendon of biceps femoris and the lateral head of gastrocnemius. It curves lateral to the neck of the fibula deep to peroneus longus and divides into superficial and deep peroneal (fibular) nerves; the frequent peroneal nerve is well injured on the fibular neck. Before it divides, it provides off articular branches to the knee and the superior tibiofibular joints and cutaneous branches. Its cutaneous space of provide, together with its terminal branches, consists of the anterolateral and lateral surfaces of the leg and many of the dorsum of the foot. The superior gluteal nerve (L4, L5, S1) leaves the pelvis through the higher sciatic notch above piriformis and provides gluteus medius, gluteus minimus, tensor fasciae latae and the hip joint. The inferior gluteal nerve (L5, S1, S2) passes through the larger sciatic notch beneath piriformis and supplies gluteus maximus. Obturator Nerve (L2�4) Gluteal Nerves Autonomic Innervation Sciatic Nerve (L4, L5, S1�3) the autonomic provide to the limbs is exclusively sympathetic. The preganglionic sympathetic influx to the decrease limb is derived from neurones within the lateral horn of the lower thoracic (T10, T11) and higher lumbar (L1, L2) spinal twine segments. Fibres cross in white rami communicantes to the sympathetic chain and synapse in the lumbar and sacral ganglia. Postganglionic fibres pass in gray rami communicantes to enter the lumbar and sacral plexuses, and heaps of are distributed by way of the cutaneous branches of the nerves derived from these plexuses. The blood vessels to the lower limb obtain their sympathetic provide by way of adjoining peripheral nerves. Postganglionic fibres accompanying the iliac arteries are destined mainly for the pelvis but may provide vessels within the upper thigh. The preaxial border starts close to the midpoint of the thigh and descends to the knee.
Syndromes
- School age test or procedure preparation (6 to 12 years)
- Flushing from niacin (vitamin B3)
- Inner ear (cochlear) implants
- Are you sensitive to light?
- Stroke
- Increased muscle tone (spasticity)
- Bladder cancer
- Cyclophosphamide (Cytoxan)
Purchase 20 mg propranolol with mastercard
Unlike most iatrogenic strictures cardiovascular disease icd 9 40 mg propranolol buy visa, malignant strictures have an irregular appearance heart disease japan propranolol 80 mg order fast delivery. This had caused bladder outlet obstruction and dysuria; observe the bladder catheter. Oblique retrograde urethrogram shows a decent stricture of the bulbar urethra following gonococcal infection in a 25-year-old man. The overwhelming majority of solid testicular masses on this age group are either seminomas or mixed germ cell tumors. The testis was totally necrotic despite emergent exploration and an orchiectomy was performed. Elongated testicular hypoechogenicity is typically the only grayscale manifestation of secondary orchitis. Symptoms and hypoechogenicity resolved after steroid treatment of drug-induced vasculitis. The look may counsel primary (mumps) orchitis, but medical history indicates detorsion, and hypoechogenicity resolved at follow-up. Its attribute onion pores and skin look is sort of pathognomic of an epidermoid cyst, which was successfully enucleated. Bilaterality may suggest multifocal germ cell tumor or lymphoma, however demographics and a scientific historical past of longstanding sarcoidosis point out granulomatous orchitis (subsequently biopsy confirmed). This was a calcifying Sertoli cell tumor, which regularly have intensive calcifications. Segmental testicular infarction, an underdiagnosed entity: case report with histopathologic correlation and evaluation of the diagnostic options. Testicular adrenal rests in congenital adrenal hyperplasia: a rare presentation of testicular masses. Segmental testicular infarction: report of seven new instances and literature review Emerg Radiol. Sonography of the pediatric scrotum: emphasis on the Ts-torsion, trauma, and tumors. Copious gel and patient-directed ultrasound aids identification of those small, superficial benign cysts. Location, affected person age, and ultrasound options distinguish this benign entity from cystic testicular tumors. Configuration and clinical historical past advised intratumoral hemorrhage rather than testicular trauma. Simultaneous color Doppler confirms a combined intra- and extratesticular varicocele. Such an ultrasound look might immediate testis-sparing resection (as on this case). The presence of cystic areas means that this tumor contains teratomatous elements. Differentiation between giant epididymal cysts/spermatoceles and complicated hydroceles may be tough, but cysts displace, somewhat than envelop, the testis. Location inside the head may suggest a spermatocele, but differentiation between spermatoceles and epididymal cysts is usually not clinically important. The herniorrhaphy was difficult by hemorrhage that prolonged along the inguinal ring. Color Doppler (not shown) carried out throughout a Valsalva confirmed move within dilated peritesticular veins. A affected person history of von Hippel-Lindau instructed an epididymal papillary cystadenoma, a rare benign epididymal lesion. The scan was performed through the Valsalva maneuver, which triggered retrograde filling from incompetent valves. Papillary cystadenoma of epididymis: is there a necessity for additional investigation in unilateral instances Polyorchidism is a particularly rare, typically inconsequential, congenital dysfunction, although most cancers threat has been suggested. Clinico-radiological and pathological evaluation of extra testicular scrotal lesions. Note the interior heterogeneity because of ill-defined, hypoechoic areas representing intraparenchymal hematoma in a patient with scrotal trauma. Testicular tumors: what radiologists have to know-differential prognosis, staging, and administration. No focal atrophy of the infarcted section may be seen, and the adjacent parenchyma seems homogeneous. Note the moderately atrophied anteriorly displaced testis as a outcome of persistent mass impact. Sagittal color Doppler ultrasound of the testis and epididymis demonstrates hyperemia according to epididymo-orchitis. Pathology confirmed a blended germ cell tumor with 75% embryonal cell, 15% teratoma, and 10% yolk cell parts. Pathology confirmed fibrosis with heterotopic ossification doubtless secondary to prior traumatic damage. Note the few small echogenic foci as a result of internal calcification, casting a posterior acoustic shadow. Note the welldefined echogenic focus of calcification adjacent to the abscess and its robust posterior acoustic shadow. This feature is frequent in young sufferers with chronic prostatitis due to calcium precipitation in obstructed acini. M�llerian duct cysts are usually midline and enormous, extending above the bottom of the prostate, and solely rarely talk with the urethra. The cyst is seen arising from the ejaculatory duct and lengthening beyond the prostatic base. To distinguish among ejaculatory duct cyst, utricle cyst, or M�llerian duct cyst, look at the relationship of the cyst with the urethra. Note the cystic lesion has an irregular wall and internal echoes with an appearance resembling an abscess. Prostatic stromal neoplasms: differential analysis of cystic and solid prostatic and periprostatic masses. Associated extreme bladder wall trabeculation is in maintaining with bladder outlet obstruction. Presence of a large jackstone throughout the bladder signifies bladder decompensation. Surgical pathology from surgical resection revealed prostate sarcoma, not otherwise specified. It is a uncommon presentation of prostatitis but is frequent in tuberculosis prostatitis. A small amount of simple free fluid inside the pelvis in a premenopausal lady is a typical finding that could be seen in all phases of the menstrual cycle. The fluid has high attenuation with the highest attenuation present around the left ovary (sentinel clot sign). The lesion surrounds each ovaries and insinuates itself between pelvic structures with out significant mass effect.
Propranolol 40 mg generic with amex
Another potential danger is perforation of the lateral sinus wall 4 main arteries propranolol 40 mg purchase on line, leading to a buccal abscess or perforation of the sinus roof inflicting infection of the orbital contents kidney arteries and veins propranolol 20 mg discount otc. There must be little hesitation in using this process, because the frontal sinus immediately borders the cranial cavity, posing a risk of meningoencephalitis or frontal brain abscess. Occipitofrontal sinus radiograph demonstrates a fluid level (arrow) within the left ethmoid labyrinth. Secretions and pus are aspirated from the frontal sinus, and the sinus is irrigated with decongestant nostril drops and an antibiotic answer. Chronic Sinusitis Etiopathogenesis: Besides intranasal anatomic adjustments such as septal deviation and septal spurs, a selection of different ailments of a persistent inflammatory, allergic, traumatic or neoplastic nature can result in continual sinusitis. The frequent pathogenic mechanism is impaired ventilation of the ostiomeatal unit (see 1. This hampers drainage of the dependent sinus methods, particularly the adjacent maxillary sinus and anterior ethmoid cells. As the mucosa turns into swollen, particularly within the slender anatomical passages of the ostiomeatal unit, a vicious cycle becomes established that initially leads to recurrent bouts of acute irritation and ultimately culminates in a persistent, chronic sinusitis. Chronic sinusitis frequently impacts the maxillary sinus and ethmoid cells, whereas the frontal and sphenoid sinuses are less commonly concerned. Symptoms: the character of the ache is variable and might vary from a sense of pressure to persistent or recurrent complications. Many sufferers also complain of nasopharyngeal drainage (postnasal drip), and some complain of obstructed nasal respiratory. Imaging studies: Today, computed tomography is considered the only acceptable modality for imaging the paranasal sinuses if persistent sinusitis ist suspected. Conventional sinus radiographs are of very limited worth in diagnosing continual sinusitis due to artifacts from superimposed structures. Treatment: Conservative remedy options embody decongestant nose drops (for no more than one week), heat remedy (electric light cabinet, microwaves, infrared), and broad-band antibiotics. With an allergic etiology, acceptable antiallergic remedy must also be offered (see p. Chronic sinusitis b Middle turbinate Septum Septal spur Inferior turbinate Septal deviation and ridges Left ethmoid labyrinth a Septal deviation with a distinguished septal spur have brought on narrowing of the left nasal cavity. The opacifica- tion of the left ethmoid labyrinth displays the chronic inflammation resulting from impaired ventilation and drainage of the center meatus and ostiomeatal unit. The precept of endoscopic sinus surgery is to enlarge the tight passages within the center meatus and ostiomeatal unit including the natural ostia of the maxillary sinus and, if needed, the frontal sinus. A preliminary septoplasty could additionally be needed in patients with functionally important septal deviation. The hazards of intranasal sinus surgical procedure are primarily based mainly on the close proximity of the sinuses to the anterior cranial fossa, optic nerve, and (in the case of the sphenoid sinus) to the internal carotid artery. The prerequisites for any sort of intranasal sinus surgical procedure, then, are a detailed data of sinonasal anatomy and technical proficiency in handling the endoscope or microscope, which must be gained in diagnostic procedures and by practice on anatomic specimens. The surgeon must also be nicely versed in the radiographic anatomy of this region. Middle turbinate Septum Polyp Inferior turbinate A nasal polyp has prolapsed from the center meatus into the principle part of the left nasal cavity. Nasal Polyposis Pathogenesis and morphology: Nasal polyposis is a really advanced situation that develops in response to a selection of noxious stimuli, appearing morphologically as edematous, polypoid hyperplasia of the sinus mucosa (usually within the anterior ethmoid cells and maxillary sinus) and projecting into the nasal cavity in the type of polyps. Etiology: Besides genetic causes, nasal polyps are attributed primarily to chronic irritation of the mucosa, like that occurring in chronic rhinitis or sinusitis. The functional anatomy of the ostiomeatal unit, with its slitlike passages, seems to have causal significance in nasal polyposis, as in chronic sinusitis, because it controls the air flow and drainage of the frontal and maxillary sinuses. The opposing mucosal surfaces in these areas are often separated by a distance of less than 1 mm. If they arrive into contact, this can impair the mucociliary clearance mechanism and hamper the traditional transport of dangerous substances toward the nasopharynx. Whether, when, and to what extent these pathologic changes lead to symptomatic polyposis varies in different individuals and should depend partly on the timing of diagnosis and remedy. Symptoms: the medical manifestations of nasal polyps depend on their extent and should encompass obstructed nasal breathing, hyposmia or anosmia (due to obstruction of the olfactory groove), headache (due to impaired air flow and drainage within the paranasal sinuses), snoring, rhinophonia clausa, and frequent throat clearing due to related postnasal drainage. Spread to the decrease airways can result in laryngitis with hoarseness and bronchitic signs. Diagnosis: As in chronic sinusitis, the diagnosis is established by cautious rhinoscopic or endoscopic analysis of the nasal cavity, giving explicit consideration to the lateral nasal wall. Treatment: Treatment might start with symptomatic conservative measures such as using corticoidcontaining nasal sprays and systemic antihistamines. A partial or even complete remission of nasal polyps can generally be achieved with these measures alone. Besides intranasal polypectomy, which is carried out primarily in older or higher-risk patients, an important current choice is intranasal sinus surgery using endoscopic or microsurgical approach (see also Treatment of Chronic Sinusitis, p. Primary ciliary dyskinesia is an autosomal-recessive illness characterized by morphologic modifications within the cilia (absence of dynein arms, transposition of microtubules), leading to a marked discount in beat frequency and dyskinetic ciliary actions which are ineffectual for mucus transport. The impaired function of the mucociliary apparatus is manifested by symptoms of primary ciliary dyskinesia, which consist primarily of recurrent sinusitis and nasal polyposis, eustachian tube catarrh, otitis, bronchitis, and bronchiectasis. Life expectancy in affected sufferers relies upon mainly on the severity of pulmonary involvement. Mucoceles and Pyoceles A mucocele is a cystlike, mucus-containing sac that may kind inside a paranasal sinus. A pyocele is a mucocele that accommodates purulent material because of superinfection. Pathogenesis: A mucocele may be brought on by adhesions (postinflammatory, post-traumatic, or postoperative) that impede drainage from the paranasal sinus system. Mass lesions (polyps, tumors) can also impede and obliterate the drainage tracts, leading to mucocele formation. The outflow obstruction causes the mucocele to exert growing strain on the encompassing sinus walls, resulting in progressive thinning of the bone. In this way the mass can erode into adjoining constructions such because the orbit and even the cranial cavity. The most typical site of prevalence is the frontal sinus, followed by the ethmoid cells, maxillary sinus, and sphenoid sinus. Symptoms: A frontal sinus mucocele often presents as an isolated, tense swelling over the anterior wall of the frontal sinus. It can also trigger inferolateral displacement of the orbital contents, particularly if it has eroded by way of the sinus flooring. On the opposite hand, swelling within the cheek area with upward displacement of the orbital contents is extra characteristic of a maxillary sinus mucocele. Proptosis, restricted ocular actions, and diplopia can also happen, relying on the placement of the mass. On the other hand, modern sectional imaging modalities (computed tomography and magnetic resonance imaging. Rhinosinogenic Complications There are numerous mechanisms by which severe and even life-threatening issues can come up from inflammatory diseases of the paranasal sinuses.
Generic propranolol 20 mg with visa
Oncologic beads (chemotherapeutic-loaded drug-eluting beads or yttriumloaded radioembolic beads) may provide treatment choices cardiovascular system and circulatory system 80 mg propranolol generic fast delivery. Preoperatively earlier than nephrectomy coronary heart bridging propranolol 40 mg cheap on line, cheap Gelfoam and coils could also be appropriate. In a nonoperative scenario, particles and liquids could have one of the best consequence, however be cautious of shunting suspected on preembolization picture. Together, these embolic agents should scale back the danger of additional gastric variceal hemorrhage. Glue and Onyx Embolization of Extrasegmental Bile Duct Leak (Diagnostic Sinogram) Glue and Onyx Embolization of Extrasegmental Bile Duct Leak (During Embolization) (Left) Embolics have nonvascular utility [e. Contrast injected through a surgical drain tracks into a biliary duct, inadvertently surgically excluded from the biliary system. Slow Onyx injection, followed by fast "glue" injection and entry removing, successfully halted the leak. Stent Deployment (Fluoroscopic Appearance) sixty two Stents: Vascular General Principles Self-expanding: Sheathed in retractable delivery system; spontaneously expands after retraction � Most incessantly constructed from nitinol Alloy regains original shape when not compressed/constrained � Requires acceptable oversizing to achieve safe intravascular fixation � Typically more versatile � Conforms to changing vessel diameters Drug-eluting: Stent coated with medicine. Basavarajaiah S et al: Treatment of drug-eluting stent restenosis: comparison between drug-eluting balloon versus second-generation drug-eluting stents from a retrospective observational examine. Expected Outcomes � High preliminary technical success price Initial technical success is dependent upon � Anatomic location of lesion. Subclavian Steal (Left Subclavian Arteriogram) Subclavian Steal (Post Stent Deployment) (Left) Selective arteriogram of the left subclavian artery reveals a partially obstructive linear defect close to the subclavian artery origin. Contrast injected by way of the information sheath outlined the aneurysm throughout stent deployment. Healthy vascular tissue adjacent to the diseased phase is critical to lined stent exclusion of an aneurysm. The stentgraft excludes the aneurysm from circulation, eliminating the potential for aneurysm thrombosis or distal embolization. There are proximal and distal radiopaque markers that denote the stent margins for precise deployment. Once dilated, the high intrinsic radial drive of the stent maintains patency of the vessel. Renal Artery Balloon-Mounted Stent Deployment (Diagnostic Arteriogram) Renal Artery Balloon-Mounted Stent Deployment (Diagnostic Arteriogram) (Left) A diagnostic right renal arteriogram was obtained via a reverse curve catheter selectively engaged at the arterial takeoff. Emergent celiac arteriography revealed a bleeding proper hepatic artery pseudoaneurysm. Arteriobiliary Fistula (Placement of Balloon-Mounted Covered Stent) (Left) Due to the shut proximity of the bleed to the adjoining takeoff arteries and the quick out there landing zone, we opted to maximize stent position by placing a balloon-mounted stent. The naked metal portion of the stent is placed throughout the portal vein, allowing antegrade flow to proceed unobstructed by way of the portal vein. Central Venous Occlusion (Prestent) Central Venous Occlusion (Poststent) (Left) A affected person who had been receiving hemodialysis via a left arm graft complained of recently increased left arm swelling. Venous In-Stent Restenosis (Fractured Stent, Subclavian Vein) Venous In-Stent Restenosis (Hemodialysis Fistula Outflow) (Left) Stenting of the subclavian vein typically results in stent fracture and resultant instent stenosis. In this case, stenosis was associated with a high-flow hemodialysis fistula and quickly reoccurred despite repeated angioplasty. Treatment options that have been considered included putting a lined stent throughout the aneurysm neck to exclude the aneurysm vs. Contrast has been injected via the microcatheter, opacifying the aneurysm and confirming the catheter tip position. The stent prevents the coils from prolapsing into, and occluding, the splenic artery. Stent-Assisted Coil Embolization (Coil Deployment into Aneurysm) 72 Stents: Vascular General Principles In-Stent Intimal Hyperplasia (Diagnostic Aortogram) In-Stent Intimal Hyperplasia (Post Deployment of Balloon-Mounted Stent) (Left) High-grade proximal proper renal artery stenosis is seen in a patient with poorly controlled hypertension and mild renal insufficiency. In-Stent Intimal Hyperplasia (10-Month Follow-Up) In-Stent Intimal Hyperplasia (Restent) (Left) Hypertension was initially properly managed after stent placement, however the patient offered 10 months later with recurrent hypertension. Repeat angiography revealed a narrowed lumen inside the stent with a normal-caliber renal artery distally, findings in maintaining with instent intimal hyperplasia. It has many purposes, together with remedy of colonic, biliary, and vascular obstructions. Additional necessary but offlabel uses exist, together with emergent remedy of arterial bleeding when precise stent location is critical. The stent accommodates coated (above) and fenestrated (below) segments separated by a radiopaque band. Ureteral Stent Colorectal Stent (Left) A double J ureteral stent has been deployed in a patient with ureteral obstruction from peritoneal carcinomatosis. The proximal pigtail is in the renal pelvis, and the distal pigtail in the bladder. Subsequently, this cholangiogram revealed an obstructing stone in the left major biliary duct. This specific stent may be manipulated after deployment by greedy and pulling on the blue radiopaque band. A stent may be launched over the guidewire and any particles aspirated via the sheath. Contrast injection through the sheath is used to confirm an appropriate stent position prior to deployment. A guidewire placed via the sheath is advanced throughout the stenosis whereas the sheath is aspirated. Contrast injection shows the guidewire crossing the stenosis and a large calcified plaque at the proximal end of the stenosis. A 2nd filling defect, more cephalad within the popliteal artery, has not but been captured in the system. These were isolated varices that had been positioned mainly in the gastric fundus with no obvious esophageal varices seen. A balloon occlusion catheter was superior through the left renal vein, and the tip was positioned within the gastrorenal shunt. Various sclerosing brokers can be utilized, together with ethanolamine oleate iopamidol, sodium tetradecyl sulfate, and polidocanol, in either liquid or foam consistency. N-butylcyanoacrylate (glue) and absolute ethanol have also been used as liquid sclerosants. The entry needle is inserted perpendicular to the vessel and parallel to the airplane of scan. An entry needle is inserted from the facet of the vessel and seen in complete length. An access needle is inserted parallel to the vessel and perpendicular to the aircraft of scan. An access needle is inserted parallel to the vessel and parallel to the plane of scan. The entry needle is inserted parallel to the airplane of scan over the vessel and seen in complete length.