
Periactin dosages: 4 mg
Periactin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Periactin 4 mg cheap line
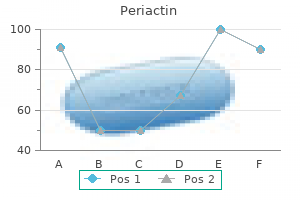
Late oligodendrocyte progenitors coincide with the developmental window of vulnerability for human perinatal white matter harm allergy forecast galveston generic periactin 4 mg otc. Maternal an infection allergy symptoms yahoo purchase 4 mg periactin amex, fetal inflammatory response, and mind damage in very low birth weight infants. Cytokine responses in cerebrospinal fluid from preterm infants with posthaemorrhagic ventricular dilatation. Risk factors for repeated cerebrospinal shunt failures in pediatric sufferers with hydrocephalus. Serial lumbar punctures for at least momentary amelioration of neonatal posthemorrhagic hydrocephalus. Repeated lumbar or ventricular punctures in newborns with intraventricular hemorrhage. Effects of intraventricular urokinase on clot lysis and posthemorrhagic hydrocephalus. Intraventricular streptokinase after intraventricular hemorrhage in newborn infants. Long-term expertise with subcutaneously tunneled external ventricular drainage in preterm infants. Early versus late treatment of posthaemorrhagic ventricular dilatation: results of a retrospective examine from five neonatal intensive care units in the Netherlands. Neurosurgical treatment of progressive posthemorrhagic ventricular dilation in preterm infants: a 10-year single-institution research. Randomized clinical trial of prevention of hydrocephalus after intraventricular hemorrhage in preterm infants: brain-washing versus tapping fluid. Randomized trial of drainage, irrigation and fibrinolytic therapy for premature infants with posthemorrhagic ventricular dilatation: developmental consequence at 2 years. Neuroendoscopic lavage for the therapy of intraventricular hemorrhage and hydrocephalus in neonates. Optimal timing of mesenchymal stem cell therapy for neonatal intraventricular hemorrhage. Pivotal function of mind derived neurotrophic issue secreted by mesenchymal stem cells in extreme intraventricular hemorrhage in the new child rats. Laptook � There is strong rationale for additional investigation of therapeutic hypothermia. Therapeutic hypothermia is an effective therapy for neonatal encephalopathy when the probability of a hypoxic-ischemic origin is high. Multiple randomized trials demonstrated that comparatively small reductions in core temperature either alone, or in combination with lowered head temperature, reduced demise or incapacity at 18 months. Disability was usually extreme and might be any of cognitive, motor, or sensory deficits. Neuroprotective effects of therapeutic hypothermia endured even at 6 to 7 years. Induction represents the time from initiation of cooling to reaching goal temperature; maintenance represents the duration of maintaining the infant at the goal temperature; and rewarming represents the reestablishment of a normothermic temperature. Specifically, the age of initiation was always lower than 6 hours after birth, the extent of temperature reduction was 33. The similarity in hypothermia regimens facilitated meta-analyses of multiple trials to provide more correct estimates of affected person outcomes. Meta-analysis indicated that outcomes are comparable irrespective of the mode of cooling. Additional trials of hypothermia could presumably be considered as diverting valuable research sources from investigation of different potential neuroprotective brokers, such as erythropoietin, xenon, and melatonin. Furthermore, most of the hypothermia components used within the first sequence of trials1�6 represented "a finest estimate" based on animal investigation and pilot human research. Third, the applying of therapeutic hypothermia was restricted to a selected group of newborns-that is, these with a diagnosis of hypoxia-ischemia presenting at lower than 6 hours of age and with a gestational age of no much less than 36 weeks. Second, will there be clinical trials and observational studies that address extending hypothermia to infants not enrolled in the first sequence of hypothermia trials The depth of temperature reduction used within the first series of hypothermia trials1�6 was extrapolated from preclinical investigation and pilot studies in newborns. Recognition that small adjustments in mind temperature modified the extent of hypoxicischemic brain harm in adult animals13 prompted perinatal animal investigations to study the consequences of depth and length of "modest hypothermia" at various occasions after mind hypoxia-ischemia. Modest hypothermia encompassed a spread of temperature reductions from as little as 2�C to as much as 5�C using newborn swine, rat pups, and fetal sheep. Comparison of the extent of neuroprotection associated with hypothermia utilizing animals wants an awareness of the relative temperature discount and the absolute temperature achieved. The optimal temperature to use for hypothermic intervention in scientific trials was not identified however was guided by existing animal data and the assessment of incremental reductions in core temperature in pilot human studies of head cooling combined with body cooling20,21 and whole-body cooling. The absence of sturdy proof for the depth and period of cooling and the approximate 46% of infants with an end result of dying or incapacity despite hypothermia therapy offered unequivocal rationale for additional investigation. The primary outcome was dying or incapacity at 18 to 22 months adjusted for sixty six Neurology Cooling Duration 33. Infants who met standards for therapeutic hypothermia (biochemical and/or clinical standards adopted by average or severe encephalopathy on neurologic examination) had been randomly assigned to one of four groups as indicated by the four cells of the diagram. The analyses examined the margins of the figure for differences in demise or disability. Similarly, infants in both cells carried out at 72 hours had been in contrast with infants in each cells carried out at a hundred and twenty hours for determination of period for cooling. The trial was closed to affected person enrollment after 364 of a deliberate 726 infants had been enrolled based mostly on recommendations of an independent Data Safety Monitoring Committee. Cooling for 120 hours was related to more arrhythmias, anuria, and an extended size of hospital keep compared with 72 hours of cooling, whereas cooling to 32. Despite the paucity of data to support the depth and period of hypothermia in the first sequence of cooling trials,1�6 the Optimizing Cooling Trial helps the continued practice of whole-body hypothermia at 33. The time of initiation of hypothermia represents the component of a hypothermia routine studied in probably the most systematic style in preclinical investigations. These experiments supplied the rationale for initiation of cooling inside 6 hours of birth within the first sequence of human cooling trials. As noted for the preclinical research of the depth of temperature reduction, information from animal models may not be readily extrapolated to newborns. Other necessary considerations are births in rural communities distant from facilities that present hypothermia, evolution of encephalopathy after 6 hours of age, and late recognition of encephalopathy. All these variables might restrict application of hypothermia within a putative slim therapeutic window. However, initiation of hypothermia after 6 hours has been reported despite the absence of evidence.
Diseases
- Onychomadesis
- Pulmonary arterio-veinous fistula
- Dementia progressive lipomembranous polycysta
- Glass Chapman Hockley syndrome
- Inhalant abuse, aliphatic hydrocarbons
- Cholelithiasis
- Schwartz Jampel syndrome
- Dementia, HIV
- Cerebral amyloid angiopathy, familial
Buy periactin 4 mg line
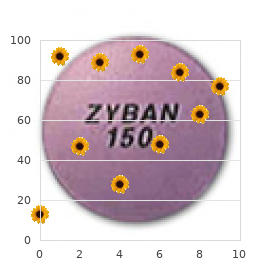
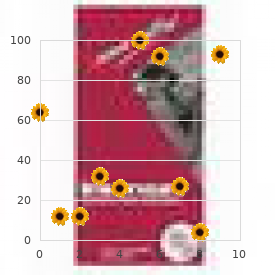
Carbapenem antibiotics similar to meropenem and imipenem have wonderful anaerobic exercise towards each gram-positive and adverse organisms and can be used allergy testing redmond wa periactin 4 mg buy generic on-line. The remedy of neonatal infections attributable to Ureaplasma urealyticum and Mycoplasma hominis is difficult by the susceptibility patterns of those organisms as they usually are proof against allergy shots nasal polyps generic periactin 4 mg with visa most antibiotics commonly utilized in neonates. The timing of the repeat lumbar puncture shall be decided partially by the medical findings and preliminary spinal fluid evaluation. Ventriculitis occurs in a minimum of 70% of instances; nevertheless, ventricular fluid is poorly accessible to systemically administered antibiotics. There are echogenic debris and septation according to purulent materials throughout the dilated lateral ventricle. Neonatal Meningitis: Current Treatment Options 197 Question 7: What Is the Duration of Treatment for Meningitis in Neonates In basic, length of remedy relies on the causative organism, site(s) of an infection, clinical severity, and course. This is often 7 days for uncomplicated bacteremia, 7 to 10 days for sepsis and pneumonia, and 14 to 21 days for meningitis, relying on the causative agent. Performance of another lumbar puncture after 21 days of therapy in infants with gram-negative enteric meningitis and earlier than discontinuation of antibiotic therapy may be useful to determine the adequacy of remedy. For meningitis attributable to group B streptococcus, a minimum of 10 days of antimicrobial remedy is beneficial. The decision of whether or not to carry out an "finish of remedy" lumbar puncture in these neonates could be primarily based on medical course. The timing and the explanation for performing neuroimaging studies are essential concerns in the determination of which kind of study should be performed. Computed tomography will present information on whether the course of meningitis has been complicated by a cerebral abscess, hydrocephalus, or subdural collections. In basic, however, computed tomography scans should be averted besides when neuroimaging is required on an emergent basis as its use has been associated with subsequent neurodevelopmental impairment and elevated danger for most cancers. A, On the T2-weighted pictures, small foci of high sign are seen in the periventricular white matter in the frontoparietal and occipital regions. These characterize areas of cystic encephalomalacia, according to periventricular leukomalacia. B, Small foci of hemosiderin deposition (black arrow) is seen within the posterior right temporo-occipital area along with cystic encephalomalacia changes (white arrows). Following gadolinium administration, a big ring-enhancing lesion is seen that extends from the posterior aspect of the temporal lobe into the adjacent parietal and occipital white matter. Question 9: Should Other Adjunctive Therapies Be Provided to an Infant With Meningitis Dexamethasone has been shown in some research to lower neurologic morbidity in older infants and kids with meningitis. However, intraventricular hemorrhage may end up in inflammatory modifications corresponding to pleocytosis with predominance of polymorphonuclear cells, elevated protein concentration, and hypoglycorrhachia within the absence of an infectious course of, making the performance of a lumbar puncture earlier than initiation of antimicrobial therapy essential. At discharge to residence at three months of age, he handed an automated auditory brainstem response test. At 22 months corrected gestational age, he had gentle impairment in each mental and psychomotor development indexes by Bayley Scales of Infant Development. Despite enhancements in neonatal care and antibiotic remedy, vital morbidity and mortality persist. Approximately 20 T to 30% of affected infants die, and neurologic sequelae are found in 35% to 50% of survivors. Ten % have extreme sequelae outlined as failure to develop beyond the age at which the disease occurred or requirement of custodial care. On the opposite hand, youngsters not identified early as having major sequelae performed intellectually, socially, and academically in a fashion much like different relations. Conclusion Meningitis is a serious infection for which early remedy is necessary to enhance both short- and long-term outcomes. Ultimately, however, its prevention might be achieved when neonatal sepsis is controlled, an elusive however not unimaginable objective in neonatal medicine. Clinical microbiology of bacterial and fungal sepsis in very-low-birthweight infants. Lower vitamin D ranges are related to increased danger of early-onset neonatal sepsis in time period infants. Risk components for invasive, early-onset Escherichia coli infections within the period of widespread intrapartum antibiotic use. Very low birth weight preterm infants with early onset neonatal sepsis: the predominance of gram-negative infections continues in the National Institute of Child Health and Human Development Neonatal Research Network, 2002�2003. To faucet or to not faucet: excessive likelihood of meningitis without sepsis amongst very low delivery weight infants. Neonatal Candida meningitis: significance of cerebrospinal fluid parameters and blood cultures. No lumbar puncture within the evaluation for early neonatal sepsis: will meningitis be missed Should a neonate with potential late onset an infection always have a lumbar puncture The cerebrospinal fluid: physiologic aspects and alterations related to bacterial meningitis. Cerebrospinal fluid analysis in neonates: comparison of high-risk infants with and without meningitis. Intrauterine an infection and the danger of cerebral palsy in very low-birthweight infants. Evaluation of routine lumbar punctures in new child infants with respiratory distress syndrome. The role of the lumbar puncture within the admission sepsis evaluation of the untimely toddler. Meningitis in premature infants with respiratory distress: position of admission lumbar puncture. Neonatal Escherichia coli bloodstream infections: clinical outcomes and impact of initial antibiotic therapy. Diagnostic value of cytokines and C-reactive protein in the first 24 hours of neonatal sepsis. Inflammatory mediators for the diagnosis and treatment of sepsis in early infancy. Revised reference ranges for circulating neutrophils in very-low-birth-weight neonates. Circulating neutrophils in septic preterm neonates: comparison of two reference ranges. Enhanced identification of group B streptococcus and Escherichia coli in young infants with meningitis utilizing the biofire filmarray meningitis/encephalitis panel. Effect on neutrophil kinetics and serum opsonic capacity of intravenous administration of immune globulin to neonates with clinical signs of early-onset sepsis. A practical approach to evaluating and treating neutropenia within the neonatal intensive care unit.
Periactin 4 mg cheap fast delivery
The ovary is suspended between two attachments: laterally to the pelvic wall by the suspensory ligament of the ovary (contains the ovarian vessels allergy medicine expiration dates buy periactin 4 mg on-line, lymphatics allergy symptoms 7dpiui effective periactin 4 mg, and autonomic nerve fibers) and medially to the uterus by the ovarian ligament. The uterine tubes (fallopian tubes), about 8-10 cm long, are suspended within the mesosalpinx portion of the broad ligament and are subdivided into 4 components: � Infundibulum: fimbriated, expanded distal portion that opens on the ostium into the peritoneal cavity and lies near the ovary. Coughing or straining Increased intraabdominal pressure Increased intraabdominal stress Urine loss Patient with defective fascial assist of urethrovesical (U-V) junction. Bulging of anterior vaginal wall on straining Normal pubocervical fascial assist Torn pubocervical fascial sling Increased strain Closes urethra Opens urethra Increased intraabdominal strain forces urethra against intact pubocervical fascia, closing urethra and sustaining continence. Defective fascial assist permits posterior rotation of U-V junction owing to increased strain, opening urethra and causing urine loss. Male Pelvic Reproductive Viscera the male pelvic reproductive viscera embrace the prostate gland and paired seminal vesicles. The testes descend into the scrotum late in human prenatal growth and are linked to the seminal vesicles by the ductus (vas) deferens, which passes in the spermatic twine, ascends in the scrotum, passes through the inguinal canal, and then courses retroperitoneally to be part of the duct of the seminal vesicles (ejaculatory ducts) (Table 5. Chapter 5 Pelvis and Perineum 245 5 Clinical Focus 5-4 Uterine Prolapse Uterine prolapse could happen when the help buildings of the uterus, especially the cardinal ligaments, uterosacral ligaments, and levator ani muscle, are weakened. Slight descent (1st degree) Cervix at introitus (2nd degree) Procidentia scientific look Urinary bladder Uterus Characteristic Description Prevalence Age Risk components Some descent widespread in parous women Late reproductive and older age groups Birth trauma, weight problems, chronic cough, lifting, weak ligaments Complete prolapse cross part Rectum Clinical Focus 5-5 Cervical Carcinoma Approximately 85% to 90% of cervical carcinomas are squamous cell carcinomas, whereas 10% to 15% are adenocarcinomas. Most carcinomas occur near the exterior cervical os, the place the cervical epithelium modifications from simple columnar to stratified squamous epithelium (the transformation zone). Composite abstract of sizes and websites Interstitial (intramural) Subserous Pedunculated, subserous Subserous, displacing uterine tube Pedunculated, submucous Characteristic Description Prevalence 30% of all women; 40�50% of ladies older than 50 years; commonest benign tumor in ladies Nulliparity, early menarche, African-American (4- to 10-fold increase) Stimulated by estrogen, oral contraceptives, epidermal growth factor Intraligamentary Cervical Submucous Risk elements Growth Pedunculated, submucous, protruding by way of exterior os Clinical Focus 5-7 Endometriosis Endometriosis is a progressive benign condition characterised by ectopic foci of endometrial tissue, referred to as implants, that grow within the pelvis-on the ovaries and within the rectouterine pouch, uterine ligaments, and uterine tubes-or in the peritoneal cavity. It often occurs between the ages of fifty five and 65 years, and threat components embody the next: � � � � � � � Obesity (increased estrogen synthesis from fat cells without concomitant progesterone synthesis) Estrogen substitute therapy with out concomitant progestin Breast or colon most cancers Early menarche or late menopause (prolonged estrogen stimulation) Chronic anovulation No prior pregnancies or periods of breastfeeding Diabetes Uterine tube Early carcinoma involving only endometrium More in depth carcinoma deeply involving muscle Ovary Extensive carcinoma invading full thickness of myometrium and escaping via tube to implant on ovary Clinical Focus 5-9 Chronic Pelvic Inflammatory Disease Recurrent or continual infections of the uterine tubes or different adnexa (uterine appendages) lead to cystic dilation (hydrosalpinx) and might account for about 40% of feminine infertility cases. The etiology and pathogenesis are intensive and include native uterine, ovarian, or adnexal issues, as properly as systemic and pregnancy-related issues. Because of the potential medical danger of an ectopic being pregnant, the being pregnant is normally terminated medically (if detected early enough) or surgically (often laparoscopically). Sites of ectopic implantation Tubal (ampullar) Abdominal Interstitial Tubal (isthmic) Ovarian Infundibular (ostial) Unruptured tubal pregnancy Cervical Villi invading tubular wall Chorion Characteristic Prevalence Age Causes Risk factors Description 10�15/1000 pregnancies (highest rates in Jamaica and Vietnam) >40% in 25- to 34-year-old group Uterine tube injury or poor tubal motility Tubal harm (infections), previous historical past, age (>35 years), nonwhite, smoking, intrauterine contraceptive system use, endometriosis Hemorrhage in tubal wall Lumen of tube Amnion Section by way of tubal being pregnant Clinical Focus 5-12 Assisted Reproduction Approximately 10% to 15% of infertile couples might benefit from varied assisted reproductive methods. From 85% to 90% of all malignancies happen from the surface epithelium, with cancerous cells often breaking by way of the capsule and seeding the peritoneal surface, invading the adjoining pelvic organs, or seeding the omentum, mesentery, and intestines. Additionally, the most cancers cells spread through the venous system to the lungs (ovarian vein and inferior vena cava) and liver (portal system) and via lymphatics. Risk factors include the next: � � � � � � � Family history of ovarian cancer High-fat diet Age Nulliparity Early menarche or late menopause (prolonged estrogen stimulation) White race Higher socioeconomic standing Routes of metastases Transdiaphragmatic communication of pleural and belly lymphatic vessels leads to pleural effusion. Malignant cells in peritoneal fluid embolize to lymphatic vessels of proper hemidiaphragm. Subdiaphragmatic cell circulate Flow over omentum Flow along paracolic gutters Paraaortic nodes Pelvic nodes Lymphatic unfold primarily to pelvic and paraaortic lymph node chains Peritoneal seeding of free-floating malignant cells commonest mode of spread Parenchymal pulmonary metastasis Spread by way of portal v. Sperm mature and are stored in the epididymis, � a long coiled tube about 6 meters in length if uncoiled. The testis is split into about 250 lobules, each containing one to four seminiferous tubules of the testes and each about 50 cm (20 inches) long on average at full length. The complete cycle of spermatogenesis takes about seventy four days and 12 more days for the sperm to mature and pass via the epididymis. The seminal vesicles have the next features: � Contribute fluid to the ejaculate and account for about 70% of the ejaculate volume. Prostate gland Seminal colliculus Prostatic utricle Opening of ejaculatory duct External urethral sphincter m. The prostate is a walnut-sized gland that surrounds the proximal urethra and has the following options: � Contributes fluid to the ejaculate and accounts for about 20% of the ejaculate volume. About three to 5 mL of semen and a hundred million sperm/mL are current in each ejaculation. In each sexes, the peritoneum on the lower inner facet of the anterior abdominal wall displays off the midline from the urinary bladder as the median umbilical ligament (a remnant of the embryonic urachus). In males, the peritoneum displays off of the urinary bladder and instantly onto the anterolateral facet Clinical Focus 5-14 Vasectomy Vasectomy provides birth control with a failure fee beneath that of the capsule, condom, intrauterine gadget, and tubal ligation. The muscular vas is recognized, and a small segment is olated between two small metal clips or sutures. The isolated section is resected, the clipped ends of the vas are cauterized, and the incision is closed (or, in the nonincisional strategy, the puncture wound is left unsutured). Incision sites Testis (phantom view) Palpate spermatic wire through the pores and skin Vasclip Site of skin incision Vas identified by contact (causes peristaltic contraction) Small puncture website Vas being clipped with Vasclip Vas isolated in ring clamp Clinical Focus 5-15 Testicular Cancer Testicular tumors are heterogeneous neoplasms, with 95% arising from germ cells and almost all malignant. Of the germ cell tumors, 60% show mixed histologic features, and 40% present a single histologic sample. Surgical resection normally is performed using an inguinal strategy (radical inguinal orchiectomy) to avoid spread of the most cancers to the adjoining scrotal tissues. It has a excessive incidence among Caucasians, with the best prevalence rates in Scandinavia, Germany, and New Zealand. Tunica albuginea (usually limits tumor) Seminoma (30% of germ cell tumors) Teratocarcinoma (most widespread mixed tumor) Hemorrhagic necrosis Embryonal carcinoma (ill-defined, invasive masses) Clinical Focus 5-16 Hydrocele and Varicocele the most typical reason for scrotal enlargement is hydrocele, an extreme accumulation of serous fluid throughout the tunica vaginalis (usually a possible space). An an infection in the testis or epididymis, trauma, or a tumor could result in hydrocele, or it may be idiopathic. Varicocele is an abnormal dilation and tortuosity of the pampiniform venous plexus. Almost all varicoceles are on the left aspect (90%), perhaps because the left testicular vein drains into the left renal vein, which has a barely greater pressure, rather than into the larger inferior vena cava, as the best testicular vein does. A varicocele is clear at bodily examination when a affected person stands, however it usually resolves when the patient is recumbent. This growth can lead to urinary urgency, decreased stream force, frequency, and nocturia. Primary lesions invade the prostatic capsule after which unfold along the ejaculatory ducts into the house between the seminal vesicles and bladder. The pelvic lymphatics and rich venous drainage of the prostate (prostatic venous plexus) facilitate metastatic spread to distant websites. Lymph node and visceral metastases Node groups numbered in order of frequency of involvement, with relative incidence indicated by dots. Urinary bladder Carcinoma Rectum Characteristic Site Metastases Etiology Prevalence Description 90% come up in outer glands (adenocarcinomas) and are palpable by digital rectal examination Regional pelvic lymph nodes, bone, seminal vesicles, bladder, and periurethral zones Hormonal (androgens), genetic, environmental factors Increased in African-Americans and Scandinavians, few in Japan Extension of carcinoma into bladder, peritoneum, and rectal wall Chapter 5 Pelvis and Perineum 257 5 Female: superior view (peritoneum and loose areolar tissue removed) Medial umbilical lig. Cervix of uterus and uterine fascia Rectum and rectal fascia Presacral (potential) area (spread open) Pelvic fascia and ligs. Cervix Distal (vertical) portion of pubocervical fascia supports urethra and U-V junction and offers backstop in opposition to which urethra is compressed throughout straining Presacral fascia (pulled away) Median umbilical lig. Superior fascia of pelvic diaphragm (superior levator ani fascia) Obturator canal and obturator a. Reflection of the peritoneum in females causes a trough or pouch to kind between the bladder and the uterus, referred to as the vesicouterine pouch.
Periactin 4 mg buy on line
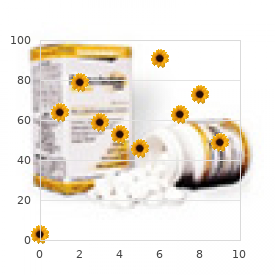
Postoperative Amplitude-Integrated Electroencephalography Predicts Four-Year Neurodevelopmental Outcome in Children with Complex Congenital Heart Disease allergy medicine over the counter best buy discount periactin 4 mg on-line. Perioperative and bedside cerebral monitoring identifies cerebral harm after surgical correction of congenital aortic arch obstruction xyzal allergy testing periactin 4 mg on line. Sepsis-associated electroencephalographic adjustments in extraordinarily low gestational age neonates. Carbon dioxide and glucose have an result on electrocortical background in extraordinarily preterm infants. The results of hypercapnia on cerebral autoregulation in ventilated very low start weight infants. Amplitude-integrated electroencephalography in newborns with inborn errors of metabolism. Glass, Michael Seed, and Vann Chau 15 � Transposition of nice arteries and hypoplastic left coronary heart syndromes are two of the most common indications for neonatal cardiac surgery. These elements embody prematurity,2 family historical past,9,10 maternal continual circumstances (such as diabetes mellitus, hypertension, obesity, phenylketonuria, thyroid problems, systemic connective tissue problems, and epilepsy),eleven,12 maternal consumption of sure drugs,13 and fetal exposures to alcohol,14 tobacco,15,16 and congenital infections. Indeed, mind lesions are sometimes clinically silent in the neonatal period, partly due to pharmacological sedation and paralysis in the early postoperative interval. Neuromonitoring tools are additionally taking half in a extra active position in improving care and outcomes on this inhabitants. Unilateral ventriculomegaly and increased extraaxial spaces most common abnormalities. The presence of shunts, malformed valves, or obstructed blood circulate could trigger lowered oxygen supply owing to the blending of venous and arterial blood. This malformation results in two parallel circulatory techniques and causes the affected infant to be cyanotic. One of these methods carries deoxygenated venous blood from the body to the right atrium after which returns it to the systemic circulation by way of the best ventricle and aorta. The different system brings oxygenated venous blood from the lungs to the left atrium and sends it again to the lungs by way of the left ventricle and pulmonary artery. Postnatally, affected infants can current with cyanosis, tachypnea, coronary heart murmurs, and diminished femoral pulses. The severity of symptoms is inversely related to the degree of blending between the 2 parallel circulations and the presence of other cardiac anomalies. This stabilization first consists of a continuous intravenous prostaglandin E1 infusion to keep the patency of the ductus arteriosus to optimize the intercirculatory mixing between the two methods. In this intervention, throughout cardiac catheterization a balloon is pulled vigorously across the atrial septum by way of the foramen ovale or an current defect, leading to elevated atrial mixing. In this cardiac malformation, the center is physiologically corrected such that the systemic deoxygenated venous blood returns to the pulmonary circulation and oxgenated pulmonary venous blood returns to the systemic circulation. In this syndrome, the left ventricle is considerably hypoplastic and can be associated both with atresia, stenosis, and hypoplasia of the aortic or mitral valves; with hypoplasia of the ascending aorta and arch; or each. Affected infants are comparatively asymptomatic initially; nevertheless, when the ductus arteriosus closes and the pulmonary vascular resistances decrease, as anticipated shortly after start, these infants rapidly go into cardiogenic shock and respiratory insufficiency. The surgical palliative restore usually consists of a three-staged method, with preliminary surgical procedure performed in the neonatal period (Norwood procedure), then at 3 to 6 months of age (bidirectional Glenn procedure), and at 18 to 30 months of age (Fontan procedure). In the Norwood procedure, a neoaorta is created through the use of the proximal pulmonary artery and homograft material, then linked to the native ascending aorta. When the child reaches 3 to 6 months of age, pulmonary vascular resistance has dropped sufficiently to enable substitution of the arterial shunt to the pulmonary circulation with a venous shunt, thus unloading the ventricle. During the bidirectional Glenn procedure (or cavopulmonary shunt), the original shunt is removed and the superior vena cava is anastomosed end-to-side to the right pulmonary artery. As the child grows additional, the Fontan process is carried out, usually between 2 and 3 years of life. In this third stage, the inferior vena cava is connected to the pulmonary arteries, permitting the entire systemic venous return to flow passively to the lungs. Advanced ultrasound with Doppler measurements can be informative of the circulate in the largest venous sinuses. Unfortunately, the reliability of cranial ultrasound for the detection of ischemic lesions is poor, with as much as one-third of infarcts being missed. Multiple, bilateral punctate white matter lesions are seen within the frontal and parietal white matter. Multiple areas of acute diffusion restriction are seen in the left basal ganglia and right thalamus. Bilateral frontal parasagittal hemorrhages with surrounding edema are seen suggestive of cerebral sinovenous thrombosis. Brain Dysmaturation Brain improvement through the fetal period requires a high power provide from the placenta. In human newborns, latest works have led to the popularity of irregular mind maturation in utero and the significance of impaired mind maturation as a substrate for postnatal injury. Both procedures carry a danger of injury for the neonatal brain and are incessantly associated with postoperative lesions. As shown by several research, mind injury is widespread before and after coronary heart surgical procedure. Anisotropic molecules are restricted in their movement by the presence of cellular architecture. Long-term outcome knowledge from cohorts of very lowbirth-weight infants adopted to adulthood point out that even mild developmental impairment on the time of college entry can translate into significantly impaired practical outcomes with lower charges of educational achievement, impartial living, and employment. Temperature control remains a crucial part to postoperative management, the place gentle hyperthermia is proven to exacerbate injury in animal models. Antenatally, maternal hyperoxygenation could also be a potential treatment for cardiac ventricular hypoplasia. The feasibility of this method has been demonstrated in fetuses with impaired ventricular growth. Several gaps proceed to exist in the understanding of the best administration of the sick toddler, and there are multiple areas of potential improvement. What stays relatively unknown is the ideal time throughout which surgical therapy maximizes brain growth whereas continually enhancing survival charges. Prevalence of congenital coronary heart illness assessed by echocardiography in 2067 consecutive newborns. Prevalence, timing of analysis and mortality of newborns with congenital coronary heart defects: a population-based research. The problem of congenital coronary heart illness worldwide: epidemiologic and demographic details. Birth prevalence of congenital coronary heart disease worldwide: a systematic review and meta-analysis.
atomic number 34 (Selenium). Periactin.
- What other names is Selenium known by?
- Protecting against prostate cancer.
- How does Selenium work?
- Are there safety concerns?
- Preventing complications and death in critical illness (burns, head injury, etc).
- Preventing selenium deficiency.
- Diabetes.
- HIV/AIDS; hardening of the arteries (atherosclerosis); arthritis (osteoarthritis); rheumatoid arthritis; macular degeneration (eye disease); hayfever; gray hair; mood disorders; chemotherapy side effects, swelling after surgery, abnormal pap smears; infertility; cataracts; chronic fatigue syndrome (CFS); bird flu; preventing miscarriage; protecting against colorectal cancer, esophageal cancer, gastric cancer, and overall cancer risk; and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96964
Effective periactin 4 mg
The tumor seems as a large lobulated stable mass displacing the neighboring organs allergy virus symptoms periactin 4 mg purchase on-line. Other belly strong tumors with related location have to be differentiated with neuroblastoma allergy symptoms ginger 4 mg periactin purchase free shipping. However, neuroblastoma arises in the adrenals, mostly shows calcification, pushes the kidney inferiorly, and encases the vessels. However, in contrast to neuroblastoma, it typically secretes steroids, leads to Cushing syndrome, virilization, and so forth [1,2]. Sites apart from belly are cervical, cervico-thoracic, mediastinal, and retroperitoneal other than adrenal. They arise along the sympathetic chain, and most of them show calcification with or without intraspinal extension. Despite intensive multimodality approach to remedy in cases of neuroblastoma, approximately, solely 30%e40% long-term survival charges might be achieved in its high-risk group [3,4]. However, low-risk and intermediate-risk teams have survival rates of more than 90% with surgical procedure and with or with out chemotherapy. It will get concentrated within the primary tumor as well as in metastatic websites like bone, bone marrow, and lymph nodes in 90%e95% of the patients [8e23]. Its finer image high quality and decrease radiation dose quickly made it the popular imaging modality. The delayed imaging approach can additionally be of assist in differentiation between true positive lesions and bowel tracer exercise, as it gets cleared later with time. There is all the time the probability of lacking the lesion in close proximity to these areas [30,31]. Post-therapy patients with a microscopic illness can give false unfavorable results [34e36]. This delineation is essential within the staging of the affected person of less than 18 months of age. However, physiologically increased demand in progress plates of kids makes metastatic evaluation tough and may lead to false positive or unfavorable result in bone scintigraphy. Persistence of uptake after eradication of tumor involvement can even result in falsepositive bone scans [62,63]. The malignant cells present an elevated rate of division, and so their metabolism results in elevated glycolysis in comparison to nonmalignant cells. Many new radiopharmaceuticals have shown potential in analysis and response evaluation of neuroblastoma. These include F-18 fluorodopamine, F-18 dihydroxyphenylalanine, F-18 fluorothymidine, F-18 fluoro-3-iodobenzylguanidine, PeF-18 fluorobenzylguanidine, C-11 hydroxyephedrine, and C-11 epinephrine. Complicated radiopharmaceutical preparation and wish of on-site cyclotron to make C-11 are the major hurdles for additional research and use of these radiopharmaceuticals within the near future [78e86]. Somatostatin receptor expression is inversely proportional to the aggressiveness of the tumor. High somatostatin receptor expression is related to decrease scientific stage and favorable medical outcome [71e73]. It is tagged with the radioisotope Indium-111 (111In) for scintigraphic imaging function. A major variation in 111 In-Pentetreotide uptake is noted in instances of neuroblastoma. Also, no direct affiliation could be established with scintigraphic uptake, and disease prognosis could presumably be established [74e77]. Previous studied demonstrated a 37% response rate in relapsed circumstances of neuroblastoma [90]. When it was tried in newly identified highrisk cases, a response fee was noted in 66% of sufferers after the administration of two cycles 131 one hundred forty eight. Method and Precautions the therapeutic intervention team is include medical oncology team, skilled nuclear medication doctor, radiation security officer, and technical personnel. The room must be shielded with thick concrete and lead must be used within the doors and windows. The toilet ought to be adjacent to the therapy room and ought to be used by sufferers only. The shielding of the isolation area should be examined by a radiation security officer before its use. Transparent glass home windows and video cameras could also be utilized by the caregivers and nursing workers to monitor kids. Nursing workers and attendant must be given radiation security counseling earlier than initiation of the remedy. To reduce the radiation publicity, the helping individual ought to spend minimal time and maintain maximum distance with the affected person. One ought to keep away from radiation contamination and will use a defend whenever attainable. The attendant ought to follow radiation safety instructions while aiding the patients for meals and use of toilets. It is essential that the used diapers must be rigorously handled as these shall be contaminated with radioactive urine and stools. There should be correct directions and amenities for the disposal of contaminated catheters, daily used articles for private hygiene, radioactive urine bags, vomiting, and fecal matters. Radiation security counseling should be given to the affected person and relations after discharge. However, growth of secondary malignancy is very rare and needs long-term follow up [91,one hundred and one,102]. Functional imaging plays a significant role within the analysis of metastasis, response to therapy, and further prognosis. Newer radiopharmaceuticals for imaging are displaying improved resolution and better quantification. Extensive analysis and long-term observe up might be wanted for further development of the therapy. Continuous blood stress monitoring is suggested in patients in the course of the remedy and the subsequent 2e3 days. Hematologic toxicity is famous mainly in sufferers having bone marrow metastasis and in patients receiving greater whole-body radiation doses. Symptomatic and prolonged instances want platelet transfusion and stem cell help [96,97]. Second malignancy like secondary myelodysplastic syndrome or acute myeloid leukemia, Disclosure No funding obtained from any organization for this study. I-131 metaiodobenzylguanidine: diagnostic use in neuroblastoma patients in relapse. Radioiodobenzylguanidine scintigraphy of neuroblastoma: conflicting results, when compared with standard investigations. A potential comparison between magnetic resonance imaging, metaiodobenzylguanidine scintigraphy and marrow histology/cytology in neuroblastoma. Iodine-131metaiodobenzylguanidine and bone scintigraphy for the detection of neuroblastoma. Efficacy of metaiodobenzylguanidine as a scintigraphic agent for the detection of neuroblastoma.
4 mg periactin with amex
It is efficient in patients with aqueductal stenosis or fourth ventricular outlet obstruction yorkie allergy treatment periactin 4 mg purchase without prescription. If the patient has a tracheostomy allergy shots poison ivy 4 mg periactin with visa, the ties securing the airway must be removed in order that the surgeon has access to the neck; the tracheostomy may be removed and replaced with an endotracheal tube secured to the contralateral side of surgery. Temperature monitoring, underbody forced air warming, and fluid warmers as properly as rising ambient room temperature are helpful. Neuromuscular blockade, if used, must be fully reversed on extubation to guarantee an adequate neurologic examination on the finish of the process. The catheter portion of the shunt may be impregnated with antimicrobial substances to forestall an infection. Reservoirs are often placed in newborns with posthemorrhagic hydrocephalus or intrathecal drug delivery. During the belly portion, care have to be taken to forestall perforation of the bowel or uptake of mesenteric elements through the peritoneum. Tunneling takes place by way of a steel rod lined with a plastic sheath or with an connected massive thread and superior via rotary movements, ensuring the rod passes through the subcutaneous aircraft and above the clavicle and ribs. They have a unprecedented capacity to take in giant fluid volumes and carry much less problems than the other shunt varieties. They are rarely placed besides in premature infants with very low delivery weight and with intracerebral hemorrhage of prematurity or hemorrhagic hydrocephalus. Another kind of shunt not often positioned in trendy times is the ventriculopleural shunt, which is vulnerable to pleural effusions, scarring, and empyema. The incidence of shunt an infection varies broadly and most frequently occurs from direct surgical wound contamination by pores and skin flora or by gramnegative peritoneal flora within the subacute or chronic interval. Antibiotic prophylaxis is run, and correct scrub preparation of the scalp and pores and skin is crucial as most shunt infections originate throughout shunt insertion. An incision is made, with a small flap to expose the cranium for drilling of a small Burr hole. The order of occasions varies, but often cranial and abdominal entry the commonest downside with the distal catheter causing shunt failure is fracture of the catheter. This often happens at points where the catheter is most vulnerable to movement, corresponding to between the mastoid and the clavicle, as the catheter is secured to the skull above and chest wall and abdomen below. Other problems embody inadequate size as the patient grows in dimension, ensuing within the catheter pulling out of the atrium or peritoneum. While often positioned in infancy for congenital hydrocephalus, they normally need alternative as the affected person matures. A 23-year-old man presents to the emergency division with a historical past of 1 week of malaise and difficulty concentrating. The cerebral aqueduct or aqueduct of Sylvius is the connection between the third and fourth ventricles. Altered valve settings can result in each over- and underdrainage inflicting hydrocephalus or herniation. A 2-day-old, 28-week untimely infant with intraventricular hemorrhage has bulging fontanelles and signs of impending herniation. Medical treatment might temporize and stabilize patients until both of those procedures is performed. Ventriculosubgaleal shunts are not often carried out except in premature low-birthweight infants with hydrocephalus. If native anesthetic is given by the surgeon at the cranial and stomach incisions, systemic opioids could be avoided during a general endotracheal anesthetic. After an uneventful intubation and affirmation of endotracheal tube placement, the affected person is positioned with his head turned to the side. Ten minutes later, whereas the surgeon is working near the proper clavicle, the oxygen saturation decreases from 100 percent to 92%. Endotracheal tubes can migrate distally into a primary stem bronchus when the top is turned laterally. Breath sounds ought to be auscultated after positioning to guarantee correct tube placement. Tension pneumothorax can also current with unilateral breath sounds but is often accompanied by hemodynamic instability. Idiopathic normal stress hydrocephalus: a scientific evaluation of diagnosis and consequence. Laparoscopic surgery in patients with ventriculoperitoneal shunts: security and monitoring. A comparison of ventriculoatrial and ventriculoperitoneal shunts in a 20-year material. Cerebrospinal fluid shunt infections in children over a 13-year interval: anaerobic cultures and comparability of clinical indicators of an infection with Propionibacterium acnes and with different bacteria. Risk of infection after cerebrospinal fluid shunt: an evaluation of 884 first-time shunts. Characteristics and treatment outcome of cerebrospinal fluid shuntassociated infections in adults: a retrospective analysis over an 11-year interval. Pediatric hydrocephalus: systematic literature review and evidence-based guidelines. She reports that these signs are gradual in onset, with no worsening with activity or place. She denies other medical history, has undergone normal prenatal monitoring, and denies latest journey or sick contacts. She was positioned on high-dose standing dexamethasone and underwent an endoscopic biopsy and resection at 33 weeks, which improved her visual symptoms. At 37 weeks she had worsening visible loss and was beneficial to endure induction of labor. An epidural catheter was positioned for analgesia, and, after a failed induction, the patient underwent an uncomplicated cesarean delivery under epidural anesthetic. She subsequently underwent a definitive resection of her tumor at 6 weeks postpartum. While she had no recovery of the imaginative and prescient misplaced at 37 weeks, she has remained disease-free for 24 months. This is thought to be potentially due to a progesterone-mediated improve in sensitivity, but it could even be associated to a lower in cerebrospinal fluid in the lumbar epidural space because of engorgement of epidural veins. Intraabdominal pressure is increased in pregnancy, and the vena cava is commonly immediately compressed by the uterus. Both of these serve to increase strain (and subsequently size) of the epidural veins, predisposing to epidural hematoma with acute will increase in intraabdominal stress. Progesterone-mediated mucosal changes cause increased gentle tissue edema and friability of the pharyngeal and laryngeal buildings, making nasal intubation and nasogastric tube placement controversial within the pregnant patient.
4 mg periactin purchase otc
The celiac nodes allergy testing guidelines periactin 4 mg cheap with mastercard, subsequently allergy testing queenstown cheap periactin 4 mg fast delivery, will obtain the majority of the lymphatic drainage from the abdomen. Other adjacent nodes can also be concerned, but not to the identical diploma as the celiac nodes. Thus, venous blood move would go from portal tributaries (superior rectal veins) into the caval (systemic) tributaries (middle and inferior rectal veins) in an effort to return blood back to the center. The epiploic foramen (of Winslow) connects the lesser sac (omental bursa), a cul-de-sac area posterior to the stomach, with the larger sac (remainder of the abdominopelvic cavity). The superior mesenteric artery passes between the neck and the uncinate strategy of the pancreas and then anterior to the third portion of the duodenum. The ureter crosses the common iliac vessels about halfway on its journey to the urinary bladder. It is slightly stretched and its lumen narrowed because it crosses these vessels, so a calculus can become lodged at this level. Blockage of the cystic duct is most likely not associated with jaundice, and obstruction of the main pancreatic duct would probably trigger pancreatitis. All the other portions of his bowel that are listed are innervated by the vagus nerve and its parasympathetic nerve fibers (innervates the foregut and midgut embryonic derivatives of the bowel). Only the descending colon is a hindgut embryonic derivative and it receives parasympathetic efferents from the S2-S4 pelvic splanchnic nerves. The surgeon would wish to incise the parietal peritoneum to enter the belly cavity, move the apron of the higher omentum apart, and then incise the mesentery of the small bowel to entry the arterial arcades. The duodenum, especially its proximal portion, would current largely as epigastric pain. The other portions of the bowel could be extra likely to current with periumbilical pain. The genitofemoral nerve is kind of always discovered mendacity on the anterior floor of the psoas major muscle. Most doubtless that is the end result of an early division of the ureteric bud, which ultimately offers rise to the ureters, renal pelvis, calyces, and collecting ducts. The first part of the duodenum is susceptible to ulcers (peptic ulcers) and is largely retroperitoneal. Ulcerative colitis can also happen in some portions of the retroperitoneal massive bowel however not as commonly as duodenal peptic ulcers. Volvulus, or a twisting, of the bowel is commonest in the small bowel (supplied by the superior mesenteric artery). The inferior mesenteric artery provides the distal portion of the transverse, descending, and sigmoid colon and the proximal rectum. The ache localizes to the decrease left quadrant once the somatic pain fibers of the peritoneal wall are stimulated. A hiatal hernia is a herniation of a portion of the stomach through a widened space between the muscular right crus of the diaphragm that forms the esophageal hiatus. Sliding (also known as axial or rolling) hernias account for the vast majority of hiatal hernias. It happens about 2 toes from the ileocecal junction and is a diverticulum of the distal ileum (midgut derivative). With the rotation of the duodenum, the ventral bud "flips" over and fuses with the larger dorsal bud, forming part of the top and uncinate strategy of the pancreas. The hepatoduodenal ligament, a portion of the lesser omentum, accommodates the proper hepatic artery (which provides blood to the gallbladder and liver), the frequent bile duct, and the portal vein. The pancreas develops from a dorsal bud and a ventral bud that are endodermal outgrowths of the longer term duodenum. As the primitive intestine tube begins to rotate, the future duodenum swings proper and the ventral pancreatic bud (which varieties the head and uncinate process of the pancreas) swings posteriorly and fuses with the dorsal pancreatic bud. During this rotation, a portion of the ventral pancreatic bud could swing anterior to the duodenum and entrap the duodenum by forming an anular pancreas. This referred pain from the gallbladder is conveyed again to the spinal ganglia of the midthoracic spinal cord by way of the higher thoracic splanchnic nerve (T5-T9), which offers sympathetic fibers to the foregut derivatives and conveys visceral ache afferents again to the spinal twine by way of its splanchnic nerves. This visceral ache is perceived as somatic ache at the dermatome ranges of the thoracic spinal wire segments associated with that sympathetic outflow. The internal abdominal indirect muscle gives rise to the cremasteric (middle spermatic) fascia. The exterior spermatic fascia is derived from the exterior abdominal oblique aponeurosis, and the inner spermatic fascia is derived from the transversalis fascia. This portosystemic anastomosis provides another route for portal blood to bypass the obstructed liver and attain the best atrium of the heart (see Clinical Focus 4. It also usually occupies the left upper quadrant, usually has a larger diameter, and has fewer arcades, nevertheless it has longer vasa rectae. The other options (villi, follicles) are inside options, not routinely visible to a surgeon. This visceral ache from the ureter is conveyed by sympathetic fibers from the T11-L2 splanchnic nerves to the corresponding dorsal root ganglia at these spinal twine ranges. The referred pain from probably the most proximal portion of the ureter (L1) is perceived somatically along this dermatome; the L1 dermatome of the iliohypogastric nerve supplies skin above the pubic bone. Each of those findings suggests a hyperactive suprarenal (adrenal) gland, which is releasing epinephrine and norepinephrine into the bloodstream. The location of the tumor just superior to the left kidney and to the left of the aorta is in maintaining with this diagnosis (see Clinical Focus four. The superior mesenteric artery passes between the dorsal and ventral pancreatic buds of the embryonic pancreas, and postnatally is often found crossing the uncinate strategy of the embryonic ventral pancreatic bud, simply to the left of the pancreatic head and anterior to the third a part of the duodenum. None of the other vessels are as carefully associated to the pancreatic head and uncinate course of as this artery. The appendicular artery is a branch of the ileocolic artery from the superior mesenteric artery, which supplies blood to the embryonic midgut derivatives. Blood from the ascending colon, an embryonic midgut derivative, is drained by the superior mesenteric vein, which then is joined by the splenic vein to kind the portal vein. The left renal vein passes anterior to the abdominal aorta before emptying into the inferior vena cava. The finest reply is the splenic vein as a result of the splenic artery provides blood to the abdomen (via the quick gastric arteries and left gastroepiploic artery), pancreas (via quite a few branches to the neck, physique, and tail), and spleen. The superior rectal veins possess portosystemic connections with the center and inferior rectal veins (these veins in the end connect with the inferior vena cava). The superior rectal veins drain into the inferior mesenteric vein (part of the portal venous drainage to the liver). In this air contrast barium enema, the transverse colon is clearly seen crossing horizontally from proper to left. The pancreas is seen posterior to the stomach; the abdomen (F) on this image is basically obliterating a view of the omental bursa. The bones of the pelvic girdle demarcate the following two areas: � Greater or false pelvis: the decrease portion of the stomach that lies between the flared iliac crests. The pelvic inlet is the upper border of the true pelvis (the pelvic brim) and the pelvic outlet is the decrease border of the true pelvis. The pelvis incorporates the terminal gastrointestinal tract and urinary system and the internal reproductive organs.
Periactin 4 mg
Saddle embolus allergy forecast topeka ks order periactin 4 mg, on the opposite hand allergy forecast berkeley buy periactin 4 mg with visa, is an emergency that may precipitate acute cor pulmonale (right-sided coronary heart failure) and circulatory collapse. Sources of pulmonary emboli Most Common Sources of Pulmonary Emboli Less Common Sources of Pulmonary Emboli Massive embolization Right aspect of heart Gonadal (ovarian or testicular) v. Lung most cancers arises both from alveolar lining cells of the lung parenchyma or from the epithelium of the tracheobronchial tree. Although there are a number of types, squamous cell (bronchiogenic) carcinoma (about 20% of lung cancers in the United States) and adenocarcinoma (from intrapulmonary bronchi; about 37% of lung cancers within the United States) are the most common sorts. For instance, in Pancoast syndrome, this apical lung tumor could unfold to contain the sympathetic trunk, affect the decrease portion of the brachial plexus (C8, T1, and T2), and compromise the sympathetic tone to the pinnacle. Emphysema is characterized by everlasting enlargement of air areas at and distal to the respiratory bronchioles, with destruction of the bronchiole walls by persistent irritation. As a end result, lung compliance increases as a result of the elastic recoil of the lung decreases, inflicting collapse of the airways during expiration. This increases the work of expiration as sufferers attempt to drive air from their diseased lungs and might lead to a "barrel-chested" look caused by hypertrophy of the intercostal muscles. She might have persistent cough and sputum manufacturing, and need accent muscular tissues and pursed lips to help her breathe. Radiographic imaging typically reveals parts of airway wall thickening, extreme mucus, and emphysema. Chapter 3 Thorax Connective tissue sheath (visceral layer of pretracheal fascia) Tracheal cartilage (ring) Elastic fibers Gland Small a. Lymph vessels Nerve Epithelium erior wal A nt 115 three Thyroid cartilage Cricoid cartilage Connective tissue sheath (visceral layer of pretracheal fascia) Tracheal cartilages Mucosa of posterior tracheal wall reveals longitudinal folds fashioned by dense collections of elastic fibers Superior lobar (eparterial) bronchus To superior lobe Middle lobar bronchus To center lobe To inferior lobe Right and left major bronchi Inferior lobar bronchus Cross section through trachea Posterior wall Esophageal m. Upper lobe Superior division of bronchus To Lingular bronchus superior Middle lobe lobe To lingula Lower lobe To inferior lobe Inferior lobar bronchus Upper lobe l Trachealis (smooth) m. Lingula Lower lobe Intrapulmonary Extrapulmonary Intrapulmonary Normal chest x-ray with superimposed drawing of main and secondary bronchi. The left facet of the center receives the blood from the pulmonary circulation and pumps it into the systemic circulation, thus perfusing the organs and tissues of the whole body, together with the guts itself. The atrioventricular groove (coronary sulcus) separates the 2 atria from the ventricles and marks the locations of the right coronary artery 116 Left common carotid a. Pericardium (fibrous layer) Respiratory diaphragm Heart drawn out of opened pericardial sac: left lateral view Superior vena cava Arch of aorta Pulmonary trunk Transverse pericardial sinus Left pulmonary vv. Bleeding could additionally be brought on by a ruptured aortic aneurysm, a ruptured myocardial infarct, or a penetrating harm (most widespread cause) that compromises the beating coronary heart and reduces venous return and cardiac output. The anterior and posterior interventricular grooves mark the locations of the left anterior descending (anterior interventricular) department of the left coronary artery and the inferior (posterior) interventricular department of right coronary, respectively. The right coronary artery courses in the proper atrioventricular groove and passes across the acute angle (right side) of the center. During ventricular diastole, blood enters the coronary arteries to supply the myocardium of each chamber. Although variations in the coronary artery blood provide to the varied chambers of the center are frequent, in general, the proper coronary artery supplies the: � Right atrium. In the remaining instances, both the best and the left coronary arteries may contribute to this department or it might be absent and branches from both coronaries could provide this area. Inferior (posterior) interventricular (posterior descending) branch of proper coronary a. Additionally, numerous smallest cardiac veins (thebesian veins) empty venous blood into all 4 chambers of the center, but largely into the right atrium. These chambers receive blood from the systemic circulation and pump it to the pulmonary circulation for fuel trade. In both ventricles the papillary muscles and their chordae tendineae present a structural mechanism that forestalls the atrioventricular valves (tricuspid and mitral) from everting (prolapsing) during ventricular systole. The papillary muscles (actually a part of the ventricular muscle) contract because the ventricles contract (ventricular systole) and pull the valve leaflets into alignment. This prevents them from prolapsing into the atrial chamber above because the stress in the ventricle one hundred twenty Opened right atrium: proper lateral view Superior vena cava Right pulmonary a. Pericardial reflection Ascending aorta Chapter three Thorax Right auricle (atrial appendage) Crista terminalis Septal leaflet (cusp) of right atrioventricular (tricuspid) valve Pectinate mm. Interatrial septum Fossa ovalis Inferior vena cava Opening of coronary sinus Valve of coronary sinus Valve (eustachian) of inferior vena cava Pulmonary trunk Nonadjacent semilunar leaflet (anterior semilunar cusp) Right adjoining semilunar leaflet (cusp) Right atrium Anterosuperior leaflet (anterior cusp) Septal leaflet (cusp) Inferior leaflet (posterior cusp) Chordae tendineae Superoposterior (anterior) papillary m. Apical trabeculations Left adjacent semilunar leaflet (cusp) Conus arteriosus Septal papillary m. Chordae tendineae Coronary sinus Tricuspid valve Inferior vena cava Inferior (posterior) papillary m. Left atrium Pericardium Epicardial fats Section via left atrium and ventricle with mitral valve minimize away Left coronary leaflet (semilunar cusp) Aortic valve Right coronary leaflet (semilunar cusp) Nonadjacent leaflet (posterior semilunar cusp) Right pulmonary vv. This could explain why pain from visceral constructions is commonly mistakenly perceived as somatic ache. If indicated the physician could choose to use coronary angioplasty to widen the partially occluded artery, which may embrace using a stent to hold the artery open. Revascularization of the myocardium after an ischemic episode by angiogenesis, bypass surgical procedure, or percutaneous coronary intervention is important for establishing blood circulate to the ischemic myocardium. Recruited pericytes contribute to stabilize the three-dimensional construction of the brand new vessel. Angiogenesis Sprouting capillary Pericytes Newly shaped blood vessels hook up with one another, forming loops and increasing the capillary community. During ventricular diastole, the muscle relaxes and the tricuspid and mitral valves open normally to facilitate blood move into the ventricles. Toward the end of ventricular diastole, the atria contract and "high off " the ventricles, just previous to ventricular systole. In addition to providing attachment factors for the valves, the cardiac skeleton separates the atrial myocardium from the ventricular myocardium (which originate from the fibrous skeleton) and electrically isolates the atria from the ventricles. The following normal heart sounds outcome from valve closure: � First coronary heart sound (S1): outcomes from the closing of the mitral and tricuspid valves. Necrosis usually happens approximately 20 to 30 minutes after coronary artery occlusion. Anterior infarct Anterolateral infarct Occlusion of proximal left anterior descending a. Infarct Infarct True posterior infarct Diaphragmatic or inferior infarct Occlusion of distal circumflex a. Sounds are finest heard by auscultating the world where turbulent blood circulate radiates. Major issues embody stenosis (narrowing) or insufficiency (compromised valve operate, usually resulting in regurgitation). These preganglionic fibers synapse within the upper cervical and thoracic sympathetic chain ganglia, after which ship postganglionic fibers to the cardiac plexus on and around the aorta and pulmonary trunk.
4 mg periactin discount fast delivery
It is very necessary 114 � Hydrocephalus allergy medicine that won't make you drowsy periactin 4 mg buy generic on-line, syringomyelia allergy treatment ramdev periactin 4 mg buy generic online, irregular spinal curvature, tethered spinal cord syndrome, atlanto- occipital fusion, and connective tissue problems such Ehlers-Danlos syndrome, craniosynostosis, Apert syndrome, Crouzon syndrome, achondroplasia, and different spinal defects are associated with Chiari malformation type I. Rare associations have been found with neurofibromatosis kind I and cystic fibrosis. If these cardiac and hemodynamic changes occur during surgical procedure, before starting pharmacological therapy, the anesthesiologist ought to ask the surgical group to lower the stress exerted by retractors or other devices in the surgical field as a outcome of this intervention would possibly appropriate these autonomic derangements. The surgical procedure consists of decompression of the posterior fossa, enlargement of the foramen magnum with higher cervical laminectomy, opening of the dura, and lysis of adhesions. The etiology for this complication consists of the tongue changing into entrapped between the tooth and impairment of venous and lymphatic drainage of the tongue from the endotracheal tube or as a result of rotation of the top and neck. The period of surgical procedure, as nicely as blood loss and fluid alternative, may also play a role in its etiology, subsequently a thorough airway evaluation including the presence of endotracheal tube leak must be performed earlier than extubation. If airway patency is unsure, we advise keeping the patient intubated until the airway edema subsides. Severity and the parts of the mind affected by the herniation characterize Chiari malformations. In the presence of unfavorable antibodies, we are able to wait to cross-match blood as the case state of affairs warrants. To keep away from inhalation anesthetic dosedependent cerebral vasodilation, we recommend the addition of a narcotic infusion (remifentanil, fentanyl, or sufentanil) to decrease inhalation agent necessities. Commonly associated comorbidities embody cervical syringomyelia and hydrocephalus in fewer than 10% of sufferers. Often, these malformations are related to myelomeningocele as nicely as with other lumbosacral neural tube closure defects, hydrocephalus, and syringomyelia. They are usually associated with agenesis of the corpus callosum, brainstem anomalies, and hydrocephalus. Type O Chiari malformation described by Iskandar and associates was defined because the presence of syringomyelia without tonsillar herniation that responds to posterior fossa decompression. Overall downward movement of the central nervous system secondary to lower in intrathecal pressures. These symptoms embrace aspiration, choking, dysphagia, persistent cough, and vocal wire dysfunction. The degree of tonsillar herniation has direct correlation to the diploma of neurologic signs and neurologic deficits. In severe instances, compression of the medulla can current with symptoms of dysphagia, dysphasia, cranial nerve palsies, apnea, palpitations, and sudden death. The presence of a tumor throughout the posterior fossa 116 � Neonates often current with rapid progressive neurologic dysfunction developing after 2 weeks of life. These symptoms are sometimes hallmarked by respiratory dysfunction due to involvement of the medulla oblongata. Decompressive surgical procedure is the remedy of choice for clearly symptomatic sufferers. The two surgical approaches embody decompression with dural opening and decompression with out dural opening. In common, the procedure involves a suboccipital craniectomy, cervical laminectomy, and duraplasty. Syndromes associated with Chiari malformations embody Ehlers-Danlos syndrome, craniosynostosis, Apert syndrome, Crouzon syndrome, and achondroplasia. Duraplasty is doubtless one of the options the neurosurgical group has to decompress the neurological buildings passing by way of the foramen magnum. Cranial nerve palsies can be present if the tonsillar displacement via the foramen magnum is extreme sufficient to produce traction on the cranial nerves. Malignant hyperthermia is linked to a rare disorder of muscle known as central core illness and King Denborough syndrome, however not to Chiari malformations. Which Chiari malformation involves cerebellar hypoplasia or aplasia, with patients not often surviving past infancy Anesthetic management in a baby with Arnold- Chiari malformation and bilateral vocal twine paralysis. Intraoperative neurophysiologic monitoring for prediction of postoperative neurological improvement in a child with Chiari Type I malformation. Suboccipital craniotomy for Chiari I results in evoked potential conduction changes. Dosing of remifentanil to forestall movement during craniotomy within the absence of neuromuscular blockade. Failure of succinylcholine to alter plasma potassium in children with myelomeningocele. Complications following decompression of Chiari malformation Type I in kids: dural graft or sealant Chapter Chiari malformation Youmans and Winn Neurological Surgery, 4-Volume Set, seventh ed. Management of parturients in lively labor with Arnold Chiari malformation, tonsillar herniation, and syringomyelia. Positional Magnetic Resonance Imaging for individuals with EhlersDanlos syndrome or suspected craniovertebral or cervical backbone abnormalities: an proof �based analysis. Mechanisms of cerebellar tonsil herniation in sufferers with Chiari malformations as information to clinical management. Rare affiliation between cystic fibrosis, Chiari I malformation, and hydrocephalus in a baby: a case report and evaluation of the literature. Difficult intubation in a parturient with syringomyelia and Arnold-Chiari malformation: use of Airtraq laryngoscope. Anesthetic management of a affected person with Arnold Chiari malformation type I with related syringomyelia; a case report. Anesthetic administration of a patient with syringomyelia and Arnold Chiari malformation sort I with autonomic dysfunction. Asymmetry of tonsillar ectopia, syringomyelia and scientific manifestations in grownup Chiari I malformation. Complications of posterior cranial fossa surgery�an institutional expertise of 500 patients. The affected person has achieved age-appropriate developmental and development milestones and acquired all of his necessary immunizations. Physical examination is notable for vital frontal bossing, a long and elongated cranium, regular airway anatomy, and a traditional cardiorespiratory examination. This includes visual area abnormalities which will progress to blindness, seizures, developmental delays, and other neurocognitive deficits. The three major causes of an abnormal head form in infancy embody molding, deformational plagiocephaly, and craniosynostosis. Molding could occur in utero or throughout a tough supply involving forceps or vacuum extraction, and it often resolves within hours of start to a number of weeks of age. Deformational plagiocephaly is brought on by fixed gravitational forces on the occiput that often happen in infants who remain in one place for a majority of the time. He subsequently undergoes imaging of the top which reveals craniosynostosis of the sagittal suture with no different notable abnormalities.