
Oxytrol dosages: 5 mg, 2.5 mg
Oxytrol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount oxytrol 2.5 mg amex
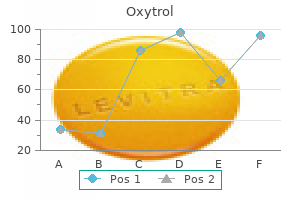
There is evidence to suggest that if the serial impedance values at a location are comparable treatment dry macular degeneration buy oxytrol 2.5 mg on-line, typically within 50 ohms 897 treatment plant rd 2.5 mg oxytrol quality, the lead is much less prone to dislodge as in contrast with situations the place beat-to-beat lead impedance values fluctuate to a higher extent. With larger or steeper slew rates, the alerts become sharper and simpler to identify and record. However, slurred signals with low slew rates can additionally be recorded regardless of good tissue contact between the lead tip and myocardium. Repeat pacing at a lot larger amplitudes may be necessary to resume capture on the minimal threshold or even at a brand new subthreshold amplitude. The � labeled values on the first strengthduration curve are the preliminary threshold measurement during testing. Rheobase represents the minimal amplitude with the longest duration, or pulse width, to attain threshold. Theenergyexpenditure curve depicted in green on this determine was arbitrarily added to illustrate the probably gadget vitality expenditure at various pulse widths andamplitudes;itisnotaccuratenortoscale. Conventional electrical present flows through individual conductors from cathode to anode. This is usually from a cathode on the electrode tip to an anode, which is typically the ring electrode. An built-in bipolar circuit usually entails a lead tip cathode and a defibrillation coil or ring anode. Unipolar circuits embrace the lead tip (cathode) and pulse generator (anode) and are massive. Intraprocedurally, a unipolar circuit may be readily achieved by connecting the cathode (black) programmer pacing cable connector to the lead tip and the anode (red) connector to a surgical instrument. Unipolar pacing is more readily identified on floor electrocardiography by a much larger pacing stimulus artifact, is extra susceptible to detecting noncardiac alerts, and stimulating extramyocardial tissues as compared with bipolar circuits. The power expenditure curve depicted in green on this figure was arbitrarily added to illustrate the likely device energy expenditure at varied pulse widths and amplitudes;itisnotaccuratenortoscale. Hence it could be overcome by growing pacing amplitude or surgical revision of the lead. Sensing algorithms should be succesful of differentiate between native intracardiac indicators, far-field alerts including activity in other cardiac chambers, delayed depolarization and repolarization in the same chamber, pacing artifact, myopotentials, and numerous sources of electromagnetic interference. This propagation wave generates intracardiac electrical signals which may be sensed when the wave of depolarization reaches the recording electrode. During myocyte depolarization the surface of the cell initially becomes electrically impartial with respect to the inside of the cell, leaving the endocardial electrode tip with a relative positive cost as compared with the depolarized area. Initial sensing on the recording electrode tip will include native indicators, along with many undesirable and nonspecific waveforms. The measured frequencies, with bandpass filters of various device producers, could differ considerably, with variations as a lot as forty Hz between vendors. Near-field refers to a comparatively narrow circuit and is just applicable to true bipolar or some built-in bipolar circuits. In addition, myopotentials and exterior electrical interference usually tend to happen with unipolar sensing. The small amplitude of P waves limits the utility of unipolar sensing in these devices. However, unipolar sensing is mostly secure and effective for ventricular techniques given the larger amplitude of ventricular alerts and the power to enhance the sensitivity threshold sufficiently massive to avoid detection of different, undesirable alerts. True bipolar circuits are less prone to far-field sign oversensing as a outcome of each a slim short interelectrode sensing distance and integral sensing dynamics. An benefit of unipolar compared with bipolar sensing is the ability to determine the placement of origin and direction of propagation of the depolarization wavefront. In the unipolar setting, as a depolarization wavefront strikes in path of the sensing electrode, a constructive deflection is inscribed, whereas a negative waveform is inscribed when the depolarization front dissipates away from the recording website. A systematic diagnostic and troubleshooting approach is essentially the most efficient way to take care of these issues (Box 29-2). It is critical that the lead cable connectors or alligator clips be properly connected on the cathode and anode, in addition to the interface with the lead analyzer. The values obtained with the atrial and ventricular parts must be very related. If those self same settings are then used to test the atrial lead undersensing might happen. Patient-related elements that would contribute to undersensing include severe metabolic or electrolyte disturbances corresponding to acidosis or hyperkalemia, although such derangements usually tend to cause difficulties with stimulation quite than sensing. Lead insulation breach, lead fracture, or lead failure also can lead to undersensing. A defective and nonfunctional generator may also end in undersensing, however this has hardly ever been reported. Apparent undersensing can even occur if explicit atrial or ventricular events fall inside their respective blanking periods. A myocardial-lead interface downside can be readily dominated out with intraprocedural testing by way of the analyzer, and this downside can usually be remedied by altering the blanking durations, when appropriate. A main concern with oversensing is inhibition of pacing output, which may be deadly in pacemakerdependent sufferers. Finally, atrial oversensing with associated tracking to the ventricles can lead to very speedy ventricular pacing. Hence a complete diagnostic and troubleshooting approach is critical both to quickly establish the reason(s) for oversensing and to promptly correct the problem (Box 29-3). Lead Issues Many of the beforehand mentioned etiologies responsible for undersensing can result in oversensing (see Boxes 29-2 and 29-3). The preoperative chest radiograph, chronicity of the findings, historical setting, and intraoperative testing are crucial to troubleshooting and resolving these points (Case Study 29-3). Metabolic and Structural Factors Some metabolic situations might lead to oversensing. B, Intracardiac electrograms depicting T-wave oversensing by the ventricular channel. Their cautious evaluation and understanding are critical for long-term affected person follow-up so as to establish applicable rhythm diagnosis and remedy. A temporary evaluate of these algorithms can be useful for intraprocedural analysis of detection and defibrillation particularly during safety margin or defibrillation threshold testing. Of these, three are for both monitoring and therapy and the fourth is for monitoring alone. The three zones that allow for remedy supply use completely different algorithms and have totally different therapies tailor-made for each zone. The clinician defines the limits of each, based mostly on the rate and period of the arrhythmia. Based on the assorted classification strategies, typically referred to as discriminators, the detected episode is categorized as a ventricular arrhythmia, a supraventricular arrhythmia, or different. All of those parts are essential, and the authors choose to promote the extra inclusive notion of defibrillation testing, rather than simply focus on ensuring that the amount of vitality delivered is sufficient to terminate an induced arrhythmia, so-called defibrillation margin testing. Intraprocedural defibrillation testing is designed to consider all of the elements necessary to efficiently detect and terminate an induced arrhythmia. The incidence of defibrillation take a look at failures requiring intervention now is in the vary of 2% to 3%.
Purchase 5 mg oxytrol otc
Activation maps determine the origin of a rhythm treatment goals cheap oxytrol 2.5 mg visa, in addition to regions of concurrent activation symptoms quad strain order 2.5 mg oxytrol amex, which illustrate the spread of propagation. Activation is outlined as the utmost spinoff of an action potential upstroke or the corresponding maximum adverse by-product in a unipolar electrogram at a recording site. Although simply applied to paced rhythms or simple well-organized tachycardias, figuring out activation time is a difficult task during fibrillation when there are a number of simultaneous wavefronts dynamically colliding and altering the native signal morphology of electrical alerts, along with different variables, together with structural far-field interference and sign artifacts. Several algorithms implement interpolation or data fit methods to compensate for the diversity in signal morphology and enhance the accuracy of extracting activation time. Healthy tissue is a uncommon incidence clinically, and fractionated electrograms additional complicate the efficiency of such algorithms. Bipolar electrograms remove most of the far-field sign contributions however introduce a dependence on the orientation of the propagating wavefront. Due to the difficulties associated with defining activation time and assessing the reproducibility of these patterns over time, researchers started to search for various approaches to identifying spatiotemporal patterns. Spectral evaluation is carried out in an try and discretize regions by the speed of excitation. The dominant frequency for every time sequence is ascertained from the ability spectrum in the frequency domain. However, as each recorded time collection is represented by a single parameter, dominant frequency is a stationary measure of group. The regularity and organization index30,31 are further parameters that can be extracted from the facility spectrum to quantify the dominance of a frequency band and try to capture the variability of frequency inside the arrhythmia. These two measures quantify how properly the sign may be approximated with a sinusoid of frequency equal to the identified dominant frequency. There are time scales of organization, a lot of that are necessary to understanding the global structure of fibrillation. Therefore a steady-state measure of the frequency content may comprise some priceless details about group. The ideal parameter would symbolize the habits of the propagating wavefronts in both the temporal and spatial domain. Some researchers are working on implementing sturdy time-frequency evaluation strategies to search for temporal variations in dominant frequency. Phase evaluation was first introduced to the cardiac subject by way of analytical fashions. In reality, the details on how to apply this method on to experimental observations in a regular manner are nonetheless being worked out. In the Nineteen Seventies analytical fashions began to handle the way to replicate the spatiotemporal dynamics of spiral and scroll waves noticed by Winfree in chemical Belousov-Zhabotinsky medium in two and three dimensions (3D). The language used to describe this reentrant propagation in two dimensions varies throughout the area: main circle, vortex, crucial level, rotor, spiral wave, centers of self-organization, and pivot points of reentrant circuits. Three-dimensional reentry is generally identified underneath the name "scroll wave," coined by Winfree. Due to the noticed similarities, researchers turned to section analysis, which is a nonlinear dynamic techniques evaluation method often utilized in physics and utilized mathematics to quantify oscillating habits and turbulence stability. Phase analysis entails a translation from a time sequence into the section aircraft, where organized quasiperiodic indicators turn into closed-loop trajectories and the angle alongside the trajectory with respect to a known origin is outlined as the section. If the sign is arbitrarily random in time, the trajectory in the section airplane is equally random, whereas the trajectory in the section plane has a particular shape if the system is deterministic. The definitive form of the chaotic oscillator in section domain clearly distinguishes it from noise. The chaotic sign has many qualitative similarities with potential signals throughout fibrillation, which is why it was considered as a technique for identifying underlying organization in arrhythmias. In order to carry out the conversion into the new coordinate system, there have to be two parameters that oscillate in time and are out of section with each other. The easiest fashions of cardiac excitability define two parameters to characterize physiologically observed behaviors: excitability and refractoriness. A distinctive value now defines every cut-off date within the interval of an oscillating sign. Critically, with this method the interval is a dynamic length of time as a substitute of a set value to adjust for beat-to-beat variability. A topological analysis of the part can be used to extract patterns of group and assess the steadiness of those patterns in time and house. In a secure two-variable system the crucial factors are mathematically defined because the intersection of the nullclines in area. In steady spiral waves this is additionally the point in area where the spatial gradient of phase diverges. Additionally, the technology or annihilation of phase singularities throughout electrical therapy can be utilized to assess the mechanism of induction of arrhythmia or a successful antiarrhythmic therapy. We will address parameters that affect the dynamics of rotors intimately within the subsequent section. Phase analysis requires no less than two impartial state variables so as to outline part. However, in medical and most research circumstances only one variable is recorded from each electrode, the electrical potential. Techniques wanted to be launched to be able to create a second state variable and observe the section transitions and singularities in a reconstructed section airplane. Instead, a part singularity is outlined as a degree around which all phases of a cycle are current. A section singularity has a topological cost of +/- 1 relying on the chirality of the rotation. The spatial map of the topological cost identifies the phase singularity at the level of divergence in Panel C. One helpful method to create a second state variable is to use the potential sign offset by a time delay (V[t +]). Several groups have advised totally different definitions of, together with a fraction of the worldwide cycle length or the lag on the first zero-crossing of the autocorrelation of V(t). Bray and Wikswo have proven that the selection of can considerably affect the number and stability of phase singularities from the identical dataset. The Hilbert transform has gained favor as a end result of it creates a linear transition via the cycle and removes the variability of an arbitrary time delay. This technique converts a real recorded sign to a fancy "signal," where the imaginary portion is instantaneously shifted by -/2. Simultaneously plotting the part from a single pixel calculated utilizing two time embedding approaches and the Hilbert transform emphasizes the morphological variability in the section transition, particularly through the second motion potential. A shows a representative spiral wave with sturdy coupling usingtheFitzHugh-Nagumomodel. When the sign morphology deviates from this shape, it turns into less appropriate to immediately apply this remodel. The Hilbert remodel can be sensitive to giant noise fluctuations in the same method. Striking differences may be observed between the trajectories within the section domain relying on which definition of second state variable is used.
Oxytrol 2.5 mg discount fast delivery
Keeping the wires in a steady place during the process is best accomplished with the catheters in a straight line resting on the table medicine 75 buy oxytrol 2.5 mg cheap. There are several components that influence the chance of lead dislodgment during removing of the guiding catheter treatment multiple sclerosis generic 5 mg oxytrol. The use of a delivery information impacts lead dislodgement by way of the dimensions and ultimate place of the lead. Use of a delivery guide impacts lead dislodgment through the final position of the stylet. With giant veins, a 9-Fr supply information permit larger (6- to 7-Fr), extra secure leads to be placed compared with the smaller, 6- to 7-Fr delivery guides (4- to 5-Fr leads). B, Injection system is attached to the vein selector via a rotating Y-adapter. Again,tousetheveinselector in a protected and effective method and to reduce contrast use, both handsmustbeonthecatheter. Slicing Versus Peeling for Coronary Sinus Catheter Removal Slicing requires the operator to repair the result in the slicer, fix the position of the slicer and lead, then pull the catheter straight back over slicer with out transferring the chopping hand or permitting the result in lead to buckle or detach from the slicer. A natural tendency is to pull the catheter off to one aspect, disengaging the blade from the catheter. Before peeling, an assistant stabilizes the lead distally by pinching the walls of the sheath against the lead where the sheath exits the body. With the lead secure, the hub is cracked and the sheath peeled down to the fingers of the assistant. The cycle of withdrawal, pinch, and peel is repeated until the sheath clears the body and the assistant can safe the lead. The sliceable plastic hub is joined to the braided catheter via an overlapping of the plastic and braid. The resistance to slicing will increase considerably as the blade reaches the plastic hub and then decreases abruptly as the blade reaches the guide. The telescoping delivery guide supports the lead within the target vein while the angioplasty wire is removed and the stylet is advanced. The significance of using a soft curved stylet becomes apparent once guides and sheaths are eliminated. Usingthe assist provided by the vein selector and wires, the supply information is advanced towards the ostium of the goal vein. B, Support supplied by the extrasupport wire and the delivery information allows the result in be advanced deepintothesmallvein. Thesheathdetermines the length of the lead within the body, particularly in the right atrium. Pressure Products achieves this by exposing the catheter when the valve is damaged in two pieces. Jude have built-in, slittable hemostatic hubs where the troublesome transition between hub and guide is averted. B, Without moving the lead, the operator cuts the third-generation information down to the SafeSheath hub. The operator removes the lead from the reduce guide and secures it to the cutter by inserting the lead in the notch of the cutter beneath thethumb. C D Pinching the lead between the walls of the sheath stabilizes the lead and sheath distally. It is way harder, if not impossible, to successfully pinch a catheter with wire braid integrated in the wall. After an assistant releases the sheath/lead, the rest of the sheath is drawn again over the lead under fluoroscopic remark. As the tip of the sheath exits the body and the pacing lead turns into seen, the assistant secures the lead position with fingers within the pocket. The two issues of importance are the physical traits of the stylet and how the stylet is withdrawn. An unsupported lead with a stylet may result within the tip of the lead withdrawing from the target vein. The longer the stylet remains able vulnerable to displacing the lead, the extra probably the lead might be displaced. Consider a comparability of the relative threat of arterial to venous system issues. In an artery, the blood is under excessive strain and can lengthen the dissection underneath the flap. Highpressure and the course of blood flow in the artery (arrows) will raise the flap andextendthedissection. However, the impact of catheter-induced trauma leading to closure of a venous structure is of no acute or long-term significance other than the shortage of venous entry. Longer procedure times doubtlessly enhance issues with sedation and the risk of infection. Contrast stains that develop with using open-lumen catheters initially triggered great concern regularly with termination of the procedure. In reality, contrast stains are clues and when identified rapidly, point out a misstep that may be corrected earlier than vital harm occurs. Use of distinction material identifies the "catheter" location at all times, limiting unintentional trauma. When distinction materials is injected with the balloon inflated, the distal pressure will increase, additional forcing blood and distinction material into and through the venous disruption. A, Medtronic Attain 6218 guide is superior over a wire and small catheter (second-generation telescoping system) into the lateral wall target vein. D, Lead is removed, and distinction materials is injected into the posteriorlateralvein. SafeSheath sealing adapter is press-sealed into the hub and removed by cracking the hub into two pieces (Pressure Products). To make finest use of the model new supply methods, physicians have to develop interventional skills that leverage these instruments. With use and adjustments in catheter design, our understanding of how delivery guides are finest used has developed. When the tips have been stiff, it was necessary for the shape of the delivery information to match the vein takeoff. The size, form, and flexibility of the new vein selector is healthier suited to deal with troublesome vein takeoffs than the delivery guide. With the vein selector liable for finding and offering a rail, just one shape of delivery guide is critical. Acuity Steerable the Acuity Steerable is the one Boston Scientific lead with an electrode at the tip.
Buy cheap oxytrol 2.5 mg online
The sensor should achieve price response at an applicable pace treatment rosacea cheap oxytrol 5 mg overnight delivery, with its response proportional to the extent of exercise load treatment urticaria purchase 5 mg oxytrol mastercard. Third, because the magnitude of the physical or physiologic adjustments monitored by a sensor can differ between patients, physician input is often necessary to regulate the algorithm, generally by programming a quantity of rate-response variables in order to obtain the clinically desired modulation of pacing rate. This requirement for handbook programming has been minimized by the introduction of optimization algorithms that routinely modify the rate-response settings. Minute air flow sensing affected by voluntary hyperventilation Standard implant process most popular Large size or requiring addition electrodes are problematic Energy consumption must not unduly hurt pacemaker longevity Important for sensors in direct contact with the blood steam Stability of central venous temperature sensor a priority Sensor algorithms could be complex, but programming ought to be simple. The programmable parameters of most rate-adaptive pacing techniques embody the decrease and upper charges, sensor thresholds, and rate-response slopes. These curves can be linear, curvilinear, or complicated depending on the relationship of the sensor to physical actions, and a set of such curves that can be chosen for a person affected person is available. In most units the sensor can be programmed in a passive mode such that the sensor output is collected but not used to modulate pacing fee. Different producers could use totally different terminology for these programmed parameters, and if the terminology is totally different from the above, will probably be recognized in italic within the following text. The physiologic or physical change detected by the sensor is convertedtoachangeinrateusinganalgorithm. Sensors which might be able to measuring the acceleration or vibration forces within the pulse generator are broadly referred to as exercise sensors. Technically, detection of physique motion could be achieved utilizing a piezoelectric crystal, an accelerometer, or different mechanical devices. Impedance is a measure of all elements that oppose the flow of electric current and is derived by measuring resistivity to an injected present across a tissue. Transthoracic impedance is used to assess respiratory fee and tidal quantity by measuring the continuous impedance between the heartbeat generator and an intracardiac electrode. Impedance can also measure surrogates of ventricular contractility, such as relative stroke volume or the proper ventricular preejection interval. The intracardiac ventricular electrogram resulting from a suprathreshold pacing stimulus has been used to provide several parameters to guide fee response. This parameter is delicate to adjustments in sympathetic activity corresponding to happen with train or emotional stress. The paced vector integrated R-wave space (termed ventricular depolarization gradient) has additionally been used for price response. These specialized leads embrace thermistors (used to measure blood temperature), piezoelectric crystal (right ventricular pressure), optical sensor (mixed venous oxygen level), and accelerometer on the tip of the pacing lead. For instance, oxygen saturation within the mixed venous blood is intently associated to oxygen consumption throughout train. Physical activities improve cardiac output and oxygen extraction from the blood decreasing the combined venous oxygen saturation with a widening of the arteriovenous oxygen distinction. The fall in combined oxygen saturation will trigger a rise in fee that will enhance cardiac output and minimize the lower in combined venous oxygen saturation. Sensing of changes in blood pH during exercise has been instructed as another possible sensor, although the requirement for a specialised lead has impeded its medical implementation. However, this sensor has recently been reintroduced in a leadless pacing pacemaker for fee response (see below). Over the years, many of these sensors have been carried out in implantable devices. Significant variations in price response have been discovered among sensors, notably between their sensitivity and specificity (Table 10-3). Sensors in particular leads have unsure long-term reliability and present challenges for matching the result in the heartbeat generator throughout pacemaker substitute. However, some of these sensors at the second are used for hemodynamic monitoring in heart failure (see Chapter 25). The leadless pacemaker is a type of a specialized lead such that rate-adaptive pacing can only be achieved with special lead sensors. At current, exercise or temperature sensors are used for rate response in leadless units. Although they is most likely not excellent proportional sensors, exercise sensors react promptly to the start of physical exercise. The first exercise sensors were piezoelectric crystals that responded mostly to the frequency of vibrations that were transmitted to the pulse generator. The particular use of an activity sensor for rate response was first described by Dahl11 in 1979 (an accelerometer configuration) after which by Humen et al12 (a pressure-vibration configuration). The chance of utilizing accelerometer-based exercise sensing for pacing rate modulation was reported for the first time in 1987. In a pacemaker, acceleration forces appearing on the body during train are detected by a device contained in the pacemaker case. With triaxially mounted accelerometers placed on the surface of an externally attached pacemaker, acceleration signals throughout a selection of exercises were measured. Right, Fourier-transformed acceleration amplitudes at totally different frequencies are showngraphically. It is evident that either the x-axis or z-axis can be utilized to detect the acceleration forces throughout strolling. On the other hand, the y-axis is useful only to detect body swaying throughout walking. In an implanted pacemaker, the x-axis would be more sensible than the z-axis because the top of the pacemaker can range with implantation or change with pacemaker rotation within the pocket, whereas the anteroposterior axis stays relatively fixed. The selection of an applicable accelerometer axis is crucial to ensure an appropriate rate response in a leadless pacemaker because the orientation of the accelerometer in such a tool is very variable. Effects of walking velocity and gradient on the acceleration indicators: Acceleration forces are represented by the built-in root mean sq. worth of accelerations. Although walking up a slope additionally will increase the acceleration forces, the rise is lower than that induced by strolling sooner. Frequency vary of acceleration forces throughout walking: During strolling, the fast-Fourier transformed acceleration shows that almost all of the sign is less than four Hz. Low-pass filtering at four Hz can due to this fact enhance the specificity and proportionality of the sensor. Other forms of train: Appropriate improve in acceleration force occurs throughout working. However, the acceleration forces during upper limb motion and biking are limited. Activity sensors had been first launched as piezoelectric crystals connected to the within of the pulse generator. Generally, the piezoelectric element produces potentials within the range of 5 to 50 mV throughout rest and as a lot as 200 mV during vigorous exercise. Because this mass is variable amongst sufferers and adjustments with pacemaker pocket maturation, variation in rate response from affected person to affected person for a similar level of activity is observed with the piezoelectric crystal sensor.
Generic oxytrol 2.5 mg
The adrenergic stimulation can be anticipated utilizing the intravenous average sedation before injection of the native anesthetic underneath shut monitoring of blood strain and oxygenation treatment bladder infection cheap 5 mg oxytrol with amex. Stress on the shoulder cuff ought to be averted symptoms quitting weed discount oxytrol 2.5 mg without prescription, as a result of this will likely cause postprocedural shoulder complaints. Thesuperiorparasternal incision mark is positioned 14cm above the xiphoid and 1cm left parasternal, in a craniocaudal direction. It is essential to forestall too much skin traction by the drapes, as this will likely displace the incision websites. Additionally, the surgical work field can be covered with plastic adhesive drapes (Ioban; 3M, St. The second method, the two-incision technique, was introduced to improve the cosmetic end result, scale back the possibility of wound infection, and cut back procedure time. In obese patients, care must be taken to ensure the pocket is under all the adipose tissue directly on the muscular fascia. Most of the pocket can be made with blunt dissection, but electrocautery can be used for areas troublesome to reach deep within the pocket. The actual anatomic aircraft of the pocket depends on the size and position of the latissimus dorsi muscle. This will prevent defibrillation failures which will occur when the can is positioned too removed from the chest wall due to both underlying muscle or fatty tissue. The decrease a half of the can ought to be positioned on the parallel line from the xiphoid to the midaxillary line. The middle a half of the can is ideally placed on the midaxillary line as talked about earlier. Online we provide movies exhibiting the three-incision approach (Video 28-1) and the two-incision method (Video 28-2). The preformed grooves are used to bind the suture sleeve to the electrode shaft with nonabsorbable suture material. Although proof is at present missing, the two-incision technique might cut back infection risk, because it omits one incision from the three-incision approach. Experience in a recent, bigger cohort (unpublished) confirms our earlier printed results. The two-incision approach consists of only one parasternal incision on the xiphoid position, much like the one described above, and abandons the superior parasternal incision. The electrode is inserted into the subcutaneous sheath till the suture sleeve reaches the opening of the sheath. It is feasible to affirm manually that the tip of the lead is within the appropriate superior parasternal position. The parasternal incision requires no less than two suture layers to make sure that sufficient tissue is pulled over the generally superficially positioned subcutaneous lead. The pocket incision requires a minimum of three suture layers, as traction on the wound could cause sutures to break when only one or two layers are used. Case Study 28-1 presents a patient in whom suboptimal positioning of both the lead and the pocket resulted in a excessive defibrillation threshold. In these sufferers, the gadget could be positioned completely submuscular to reduce local tissue stress and enhance the beauty end result. Below we describe and supply visualization of the approach to the completely submuscular placement of the can. The serratus anterior muscle is innervated by the long thoracic nerve, originating from the brachial plexus and travels inferiorly on the floor of the muscle. The fascia between the third and fourth muscle slips is dissected consistent with the muscle fiber path towards the scapula. When these kind of anatomic variations are noticed on routine preimplantation chest x-rays, an alternative implant strategy could also be thought-about because the usual place may end in an ineffective shock vector or suboptimal sensing. In these sufferers, the parasternal lead could be placed on the right aspect of the sternum to optimize the shock and sensing vectors. Online we offer a video of an explant of the subcutaneous lead and can approximately 2 years after implant (Video 28-4). With both choices, full restoration from the infection earlier than a new device is implanted is essential. Device programming and function are optimized by running the automatic setup with the affected person in both supine and upright positions to guarantee enough sensing of the center rhythm. During the implant process, this could be accomplished solely with the affected person in supine position and is subsequently suboptimal. Depending on the severity of the infection and the recovery course of, patients can endure reimplant procedures after between 6 weeks and three months when full recovery is achieved. When an infection is also current or suspected, this should be treated by device extraction to allow full recovery. In most circumstances, the can is positioned too far anteriorly or indirectly on the chest wall but embedded in a layer of subcutaneous fats. In our expertise, this can be corrected in most cases by implanting the can deeper within the precise position described earlier in this chapter. One case report describes a different administration strategy the place the lead was positioned substernally to overcome the high defibrillation threshold. Current restricted experience with the gadget shows an improved beauty results of the pocket. Implanters and supporting staff have to build experience as they did with transvenous devices. Optimal positioning of the can and lead based mostly on anatomic landmarks ensures adequate sensing and defibrillation. Van Opstal J, Geskes G, Debie L: A fully subcutaneous implantable cardioverter defibrillator system functioning concurrently with an endocardial implantable cardioverter defibrillator programmed as pacemaker. Tanner J, Norrie P, Melen K: Preoperative hair removal to cut back surgical web site an infection. Dumville J, McFarlane E, Edwards P, et al: Preoperative pores and skin antiseptics for preventing surgical wound infections after clear surgical procedure. Webster J, Alghamdi A: Use of plastic adhesive drapes throughout surgery for preventing surgical web site an infection. Lipp A, Phillips C, Harris P, Dowie I: Cyanoacrylate microbial sealants for skin preparation prior to surgery. The goal of this chapter is to present the reader with both a basic and a complicated understanding of intraprocedural assessment of stimulation, sensing, detection, and defibrillation. In addition to having a complete understanding of cardiac pacing and sensing physiology, careful preprocedural affected person evaluation to identify clinical options that may instantly or indirectly influence their utility (Box 29-1) is important. This leads to a conformational change of that advanced and permits binding of the myosin head to the uncovered actin-binding sites. They are composed of a phospholipid membranous outer layer, and their electrical state is characterized by a resting transmembrane electrochemical potential stemming from an actively maintained milieu of ions and charged particle gradients. In the traditional steady state, the outer membrane is permeable to K+ ions generating a predominantly negative inside and constructive outer cost distribution steering the membrane potential towards -90 mV. During this course of, the positively charged Na+ and Ca2+ ions are transported or enabled to move intracellularly, whereas negatively charged ions, corresponding to Cl-, circulate out into the extracellular space yielding a change within the membranes electrochemical distribution with the intracellular compartment becoming more constructive (+40 mV or greater) and the extracellular more negative. The resting transmembrane potential is subsequently reestablished and maintained by energyconsuming processes such as the sodium-potassium exchange pump.
Syndromes
- Stemetil
- Protecting against injury
- Birth defects (especially "chiari malformation," in which part of the brain pushes down onto the spinal cord at the base of the skull).
- C-reactive protein (CRP)
- Carry hand sanitizer with you, and use it often during the day.
- 40 or older who has never had a baseline mammogram
- Nausea
2.5 mg oxytrol buy with mastercard
This can greatest be managed by lubricating the lead with sterile saline or different fluid treatment laryngitis cheap 5 mg oxytrol visa, then using clean forceps to slide the sleeve into place medicine man dr dre oxytrol 5 mg buy discount line. Some implanters use multiple sutures rather than a single suture, as mentioned for ventricular lead placement. Generally, the suture sleeve and lead are anchored to the pectoral muscle parallel to the vein. The securing course of is identical, and one ought to avoid acute angulation of the lead and the creation of factors of lead stress. However, defibrillation vectors seem to favor placement on the left aspect, particularly with dominant can-active ("scorching can") methods now in almost common use. At instances, standard single-lead coil-can-based defibrillation is inadequate to accomplish defibrillation with acceptable safety margins and when further defibrillation electrodes are determined to be indicated. A small electrode patch may be added through a small left anterior chest incision. The lead is inserted into the sheath after elimination of the stylet, after which the sheath is slit for removal. The body of the azygos vein lies anterior to the thoracic vertebrae and to the right of the descending aorta, immediately behind the guts. In flip, the peel-away sheath can then be superior over the mix of the wire and the inner catheter to roughly the same location at the degree of the diaphragm. It can be tough to advance the lead past the sheath, so it is very important try to position the tip of the sheath on the diaphragm. In restricted personal experiences, the former has been extra successful and each more so than advancing to coil right into a more anterior location. Retained guidewire or multiple venipuncture strategies could be employed for all of those intravenous coil approaches. The improve process requires new venous access for the introduction of a quantity of new leads. New venous entry can also be wanted for introduction of a model new ventricular lead due to problems with the prevailing lead. Upgrade procedures usually contain a standard strategy utilizing one of many beforehand described percutaneous methods or a venous cutdown. If the first ventricular lead was placed through the cephalic vein, the percutaneous method is sort of necessary for the upgrade. Conversely, in sufferers handled with an preliminary percutaneous subclavian approach, the brand new lead may be introduced both by cutdown of the cephalic vein or through percutaneous venous access. In the case of an preliminary percutaneous strategy, the ventricular electrode can function a map. Using fluoroscopy, one can use the prevailing ventricular lead as a goal to guide the percutaneous needle. Care ought to be taken to not touch or injury the implanted lead(s) with the needle. The lead should be used as a reference landmark for the expected location of the subclavian vein. Bognolo et al103,104 described a technique to reestablish venous entry utilizing the unique ventricular lead. The patency of the venous constructions could be assessed as beforehand described with the injection of radiographic distinction materials. Note posterior retrocardiac mediastinal location and drainage into the superior vena cava. The puncture of the vein could be expedited with a easy technique: A guidewire or catheter is handed to the vicinity of the subclavian vein by way of a vein within the arm. The guidewire or catheter may be palpated or seen fluoroscopically, thus serving as a reference for venous entry. In the case of a cutdown on a beforehand unused cephalic vein, the Ong-Barold percutaneous sheath set method can be utilized. Preprocedural consideration of this is crucial in obviating very challenging intraprocedural problems. Either the vessel is thrombosed or some form of obstruction precludes the position of additional leads from the same aspect. Early injection of radiographic distinction material may expedite the choice to use this strategy. The use of the contralateral axillary or subclavian (rather than cephalic) vein is really helpful for this approach. The identical percutaneous strategies and precautions as previously described are used for the venipuncture/introducer strategy. The incision want only be giant sufficient to enable anchoring of the lead and securing of the suture sleeve. As in an preliminary implantation, the incision should be carried down to the pectoral fascia. Once the lead has been positioned and secured, it can be tunneled to the original pocket. The maneuver of passing a lead or catheter via tissue from one location to another is referred to as tunneling. It always involves the passage of a catheter from one wound through tissue to a second wound remote from the first. The monitor of the tunnel from the satellite tv for pc wound to the pocket is infiltrated with native anesthesia by the use of an 18-gauge spinal needle. The free end of the Penrose drain is then delivered to the receiving wound from the satellite tv for pc wound in the subcutaneous tissue. The tip of the clamp is pushed bluntly in the subcutaneous tissue from the receiving wound on to the satellite wound. Care is taken to maintain the tunnel as deep as possible, normally on the surface of the muscle. The free finish of the Penrose drain is grasped and pulled back from the satellite tv for pc wound to the receiving wound. The the rest of the Penrose drain containing the electrode connector pin is pulled through the observe to the receiving wound. A second, older method delivers the Penrose drain to the receiving wound by use of a "passer," usually a knitting needle or dilator. In this technique, the free finish of the Penrose drain is fastened to the back finish of the passer with a tie. The pointed tip of the passer is inserted into the satellite tv for pc wound and pushed to the receiving wound. The tip of the passer is grasped and pulled into the receiving wound with the Penrose drain hooked up. The the rest of the Penrose drain with the lead is then pulled into the receiving wound. After the observe of the tunnel is infiltrated with an 18-gauge spinal needle, the needle is passed from the wound of origin to the receiving wound.
Discount oxytrol 5 mg with visa
Mishra A useless id symptoms 2.5 mg oxytrol discount fast delivery, Seethamraju K treatment herniated disc oxytrol 2.5 mg on line, Delaney J, et al: Long-term in vitro hydrolytic stability of thermoplastic polyurethanes. Kolodzinska K, Kutarski A, Grabowski M, et al: Abrasions of the outer silicone insulation of endocardial leads of their intracardiac part: a brand new mechanism of lead-dependent endocarditis. Bogossian H, Mijic D, Frommeyer G, Winter J: Insulation failure and externalized conductor of a single-coil Kentrox lead: an ongoing story Beyersdorf F, Kreuzer J, Schmidts L, Satter P: Examination of explanted polyurethane pacemaker leads using the scanning electron microscope. Kolodzinska A, Kutarski A, Koperski L, et al: Differences in encapsulating lead tissue in sufferers who underwent transvenous lead removal. Stokes K, Coury A, Urbanski P: Autooxidative degradation of implanted polyether polyurethane gadgets. Stokes K, Urbanski P, Upton J: the in vivo auto-oxidation of polyether polyurethane by metal ions. Novak M, Dvorak P, Kamaryt P, et al: Autopsy and medical context in deceased patients with implanted pacemakers and defibrillators: intracardiac findings close to their leads and electrodes. Polewczyk A, Kutarski A, Tomaszewski A, et al: Lead dependent tricuspid dysfunction: evaluation of the mechanism and management in patients referred for transvenous lead extraction. Polewczyk A, Kutarski A, Tomaszewski A, et al: Late issues of electrotherapy-a scientific analysis of indications for transvenous removing of endocardial leads: a single centre experience. Cassagneau R, Jacon P, Defaye P: Pacemaker lead-induced extreme tricuspid valve stenosis: complete percutaneous extraction underneath extracorporeal life assist. Zoppo F, Rizzo S, Corrado A, et al: Morphology of right atrial appendage for everlasting atrial pacing and threat of iatrogenic perforation of the aorta by lively fixation lead. Uijlings R, Kluin J, Salomonsz R, et al: Pacemaker lead-induced severe tricuspid valve stenosis. Ribeiro H, Magalh�es P, Ferreira C, et al: Pacemaker leadinduced tricuspid stenosis: a report of two circumstances. As i = ei/2, multiplication or division by i imparts a section shift of +/2 or -/2, respectively, to a complex quantity in the advanced airplane. The first phrases in these equations are the actual integrals and supply the options for Equation A11-1. The subsequent terms are the complementary capabilities and provide the options for Equation A11-1. The electric current I lags the entire voltage V in phase by the argument of the impedance (-arg Z in Equation A11-1. In Elementary differential equations, ed 6, New York, 1981, Collier Macmillian, pp 84�99. The unfavorable signal implies the work carried out by the field in transferring the charge from level A to point B is the potential energy misplaced during the course of. The point electrical charge q1 establishes a (vector) electrical field E1 round it: E1 (r) = q1 1 (r - r1) 4 0 r - r1 three [A11-2. This allows the definition of a (scalar) electrical potential 1 (unit volt [V]): 1 (rB) - 1 (rA) = rB -W = - E1 d rA q [A11-2. For q1 and q2 of opposite polarities, U will increase (becomes much less negative) as the separation r will increase. The equipotential surfaces and electric field traces all the time intersect at right angles. In practice, usually only the dipole moment and not the magnitude of the electric charges and their distance aside may be directly measured. At the electrode-electrolyte interface, the "parallel plate capacitor" (as depicted in the circuit symbol) notion no longer applies and an alternative interpretation of capacitance is necessary. A dipole could also be considered the best type of capacitor and might be used to illustrate the therapy of capacitance as a property of an electrical subject. If allowed, the optimistic charge +q will move alongside path (the straightest and most direct route within the electrical field) down the steepest potential gradient to the unfavorable cost -q. Consider a modicum of charge +q moving from the constructive pole to the negative pole. Assuming q q (so that the electric field E inside the dipole is minimally altered by the move and the voltage V throughout the dipole in the circuit stays largely constant), the vitality released by +q travelling down path within the electrical area is: W = q - pole + pole E d [A11-2. B and C, the electrical subject and potential along the axis of the dipole (blueforthepositivecharge;redforthenegativecharge;greenforthe dipole). Comparedwithapointcharge,theelectricfieldhasaminimum amplitude higher than zero inside, however decreases more rapidly outdoors, thedipole. The derivation above assumes the electrical area within the dipole and the voltage throughout the dipole stay largely constant during the charge transfer. If path is truncated into a number of segments j of length dj (1 j n, 1 on the unfavorable pole and n at the constructive pole), then Equation A11-2. Ifallowed, the optimistic cost +q will move alongside path (the straightest and most direct route in the electrical field) down the steepest potential gradient tothenegativecharge-q. Their relevance to lead design and functioning lies in modeling the electrode-electrolyte interface, an integral a part of any electrochemical system. The facilities of the nucleus and the digital cloud coincide, so the whole atom carries no general electrical cost. The electrons in the atoms of some materials, such as metals and a few types of carbon, are free to transfer from atom to atom, making them electronic conductors. However, the electron cloud in the atom of a dielectric will still shift slightly toward an external) - (j-) q [A11-2. The change at each level (q) is identical as the potentialenergy(q)impartedatthatpointby+qatthepositivepole, whatever the preexistent costs at the two poles. The separation of �q by a distance a creates a dipole second p of magnitude qa parallel to the inducing electrical subject E in the polarized atom. The electric subject of a dipole has a short vary, and hence the electric subject of a polarized atom (which opposes the inducing external electric field) has negligible results on the native electrical field of the adjoining atoms, resulting in uniform polarization inside the dielectric. Ignoring the higher-order electrical poles, the polarization density P (defined by means of effects on the electric field) is similar as the dipole moment density: P = Np the surface cost density is given by: � = � (Nq) a = � N (qa) = � P p [A11-2. Hence the majority stays electrically neutral, and web charges appear solely on the surfaces of a quantity of dielectric in an electric area, no matter its size. If is the floor cost density on the capacitor plates, the small box encloses a charge of �A. As the electric field is zero within a conductor, the only floor of the small box that should be included in evaluating the surface integral in Equation A11-2. Ignoring edge effects and assuming the electrical field is uniform and perpendicular to the floor of the plate: E A = A E= zero zero [A11-2. Polarization throughout the dielectric successfully allows an electrical present to "flow via" the insulator and throughout vacuum betweentheconductorplates.
Buy generic oxytrol 5 mg online
Discussion 4 the Epworth Sleepiness Scale is an eight-question assessment of daytime sleepiness in which the respondent rates how probably one is to fall asleep in quite a lot of conditions treatment for strep throat 5 mg oxytrol order otc. Scores lower than 10 are regular medications and mothers milk 2016 2.5 mg oxytrol cheap amex, and scores greater than 10 may counsel the necessity for added evaluation by a sleep specialist. K complexes first appear in which of the next phases throughout one full sleep cycle Vertex shape waves often seem toward the end of which of the next sleep phases On the Epworth Sleepiness Scale, scores lower than are normal, and scores greater than might suggest the necessity for added analysis by a sleep specialist. Section the Cardiopulmonary System throughout Unusual Environmental Conditions Chapter 18 Chapter 19 3 Exercise and Its Effects on the Cardiopulmonary System High Altitude and Its Effects on the Cardiopulmonary System Chapter 20 High-Pressure Environments and Their Effects on the Cardiopulmonary System 547 � freesoulproduction/Shutterstock. Describe the interrelationships amongst muscle work, oxygen consumption, and cardiac output. Differentiate between stroke quantity and coronary heart rate in increasing the cardiac output. Describe how body temperature and cutaneous blood flow relate to a quantity of symptoms collectively referred to as warmth stroke. Introduction During heavy train, parts of the cardiopulmonary system may be confused close to their restrict. Alveolar ventilation may enhance as a lot as 20-fold, oxygen diffusion capacity as a lot as 3-fold, cardiac output as a lot as 6-fold, muscle blood flow as a lot as 25-fold, oxygen consumption as much as 20-fold, and heat manufacturing as much as 20-fold. The dimension of the heart chambers and the guts mass in elite athletes, such as marathon runners, may be elevated by forty %. When the extent of exercise is greater, nonetheless, than the flexibility of the cardiopulmonary system to provide a sufficient supply of oxygen to the muscles, anaerobic metabolism ensues. The level at which anaerobic metabolism develops is called the anaerobic threshold. Exercise causes the physique to eat a large amount of oxygen and, concurrently, to produce a appreciable amount of carbon dioxide. Cerebral Cortex 1 Motor fibers (collateral) Medulla oblongata 2 Sensory fibers Trachea Lungs Ventilation Exercise Diaphragm 3 Increased temperature chemoreceptors have been identified on the venous aspect of circulation, or within the lungs, that might account for the elevated alveolar ventilation throughout train. The cerebral cortex sending alerts to the exercising muscle tissue may send collateral signals to the medulla oblongata to improve the rate and depth of respiratory. Proprioceptors in the transferring muscles, tendons, and joints transmit sensory alerts through the spinal twine to the respiratory centers of the medulla. The improve in physique temperature during train additionally may contribute to elevated air flow. Alveolar Ventilation During normal quiet respiratory, an grownup exchanges about 6 L of gas per minute. Depending on the intensity and length of the train, alveolar ventilation should increase to (1) provide adequate oxygen to the blood and (2) eliminate the excess carbon dioxide produced by the skeletal muscle tissue. Note (a) the abrupt enhance in ventilation at the outset of train and (B) the even bigger, abrupt decrease in ventilation at the end of train. During very heavy train, nevertheless, both an increased depth and frequency of air flow are seen. The tidal volume is often about 60 p.c of the vital capability, and the respiratory rate may be as excessive as 30 breaths/min. Three distinct consecutive respiratory patterns are seen throughout gentle and moderate exercise. The first stage is characterised by an increase in alveolar ventilation, within seconds after the onset of train. The second stage is typified by a slow, gradual further improve in alveolar ventilation developing during roughly the primary three minutes of train. Alveolar ventilation during this era increases virtually linearly with the amount of labor carried out. In fact, when approximately 60 to 70 percent of the maximal exercise degree is reached through the linear second stage, alveolar air flow increases proportionately more than the oxygen uptake. The extra stimulation is believed to be caused primarily by the buildup of lactic acids in the blood after the anaerobic threshold has been reached. The maximum alveolar air flow generated during heavy train beneath regular conditions is simply about 50 to 65 p.c of the maximum voluntary ventilation (also called most respiration capacity). This supplies the athlete with an necessary reserve of alveolar air flow, which can be required in such circumstances as short bursts of elevated train, train at high altitudes, or train during very popular and humid situations. As discussed later, the inability of the center to pump adequate blood to the working muscle tissue is the major limiting issue. When the anaerobic threshold is reached, there will be an abrupt increase in alveolar ventilation The oxygen diffusion capacity could enhance as much as 3-fold during most train. It has been shown that the elevated oxygen diffusion capability outcomes from the elevated cardiac output throughout train. As extra blood flows by way of the lungs, more alveolar-capillary models become out there for gas exchange. This offers a greater surface area by way of which oxygen can diffuse into the pulmonary capillary blood. An common P(A 2 a)O of 33 mm Hg has been reported for endurance runners exercising at their Blood move to the working muscles could enhance as much as 25-fold, and the total cardiac output may increase as much as 8-fold. The capacity of an individual to enhance cardiac output to the muscles is the most important determinant of how lengthy and to what intensity the train can be sustained. Thus, the circulatory system is as important because the muscle tissue themselves in setting the limits for train. During exercise, the next important physiologic responses should happen in order for the circulatory system to supply the working muscle tissue with an sufficient quantity of blood: (1) sympathetic discharge, (2) enhance in cardiac output, (3) increase in arterial blood strain, (4) enhance in pulmonary vascular pressures, and (5) dilation of muscle capillaries. Sympathetic Discharge At the onset of exercise, the mind transmits indicators to the vasomotor middle in the medulla oblongata to set off a sympathetic discharge. This sympathetic discharge has two circulatory results: (1) the heart is chapter 18 Exercise and Its Effects on the Cardiopulmonary System 555 stimulated to increase its price and power of contraction, and (2) the blood vessels of the peripheral vascular system constrict, except for the blood vessels of the working muscles, which strongly dilate in response to local vasodilators within the muscle tissue themselves. Increase in Cardiac Output the elevated oxygen calls for during train are met almost entirely by an increased cardiac output. The increased cardiac output throughout train outcomes from (1) elevated stroke volume, (2) elevated coronary heart price, or (3) a mixture of both. Thus, the degree of vasodilation in the working muscular tissues instantly influences the stroke quantity; subsequently, the higher the vasodilation within the working muscle tissue, the larger the stroke volume and cardiac output. Another factor that facilitates an elevated venous return during train is the sympathetic discharge.
Buy generic oxytrol 5 mg online
It is rare to find pseudostratified epithelia created from cuboidal or squamous cells; therefore symptoms vaginal yeast infection oxytrol 2.5 mg low price, the most common subtype is pseudostratified columnar epithelium treatment 4th metatarsal stress fracture oxytrol 5 mg cheap fast delivery. Pulmonary alveolus one of many numerous terminal air sacs within the lungs where oxygen and carbon dioxide are exchanged. Pulmonary congestion an extreme accumulation of fluid within the lungs, usually associated with both an irritation or congestive heart failure. Pulmonary edema the buildup of extravascular fluid in lung tissues and alveoli, triggered most commonly by congestive heart failure. Serous fluid is pushed through the pulmonary capillaries into alveoli and rapidly enters bronchioles and bronchi. Pulmonary embolus the blockage of a pulmonary artery by fats, air, tumor tissue, or a thrombus that usually arises from a peripheral vein (most frequently one of the deep veins of the legs). Predisposing elements include an alteration of blood constituents with increased coagulation, injury to blood vessel partitions, and stagnation or immobilization, particularly when related to pregnancy and childbirth, congestive coronary heart failure, polycythemia, or surgical procedure. Pulmonary embolism is troublesome to distinguish from myocardial infarction and pneumonia. Pulmonary infarction, which regularly occurs within 24 hours after the formation of a pulmonary embolus, is further characterised by pleural effusion, hemoptysis, leukocytosis, fever, tachycardia, atrial arrhythmias, and striking distension of the neck veins. Pulmonary embolism is detected by chest radiographic films, pulmonary angiography, and radioscanning of the lung fields. Initial resuscitative measures embrace external cardiac massage, oxygen, vasopressor medicine, embolectomy, and correction of acidosis. The formation of further emboli is prevented by the use of anticoagulants, typically using streptokinase or urokinase, and in addition surgical intervention. Ambulation, train, and use of sequential compression gadgets on the lower extremities are also really helpful for prevention. Pulmonary emphysema a continual obstructive illness of the lungs, marked by an overdistention of the alveoli and destruction of the supporting alveolar structure. Pulmonary hypoplasia incomplete development of the lungs, resulting in an abnormally low number or dimension of bronchopulmonary segments or alveoli. A congenital malformation, it most often occurs secondary to other fetal abnormalities that intervene with regular growth of the lungs. Pulmonary shunting that portion of the cardiac output that enters the left side of the center without exchanging gases with alveolar gases. Pulmonary surfactant one of sure lipoproteins that reduce the surface rigidity of pulmonary fluids, allowing the trade of gases within the alveoli of the lungs and contributing to the elasticity of pulmonary tissue. The resistance in the pulmonary vascular mattress against which the best ventricle must eject blood. Glossary 611 Pulse oximeter a device that measures the amount of saturated hemoglobin in the tissue capillaries by transmitting a beam of sunshine via the tissue to a receiver. This noninvasive technique of measuring the saturated hemoglobin is a useful screening tool for determining fundamental respiratory perform. Pyelonephritis a diffuse pyogenic an infection of the pelvis and parenchyma of the kidney. Capillary shunting is often attributable to (1) alveolar collapse or atelectasis, (2) alveolar fluid accumulation, or (3) alveolar consolidation. Resonance high quality of the sound heard on percussion of a hole structure such because the chest or stomach. Respiratory acidosis a situation marked by excessive ranges of carbon dioxide and a low pH within the blood, due to hypoventilation. Respiratory alkalosis a respiratory condition in which an increased alveolar air flow. Respiratory misery syndrome an acute lung illness of the newborn, characterized by airless alveoli, inelastic lungs, a respiration rate higher than 60 breaths per minute, nasal flaring, intercostal and subcostal retractions, grunting on expiration, and peripheral edema. It is brought on by a deficiency of pulmonary surfactant, leading to overdistended alveoli and at instances hyaline membrane formation, alveolar hemorrhage, severe right-to-left shunting of blood, increased pulmonary resistance, decreased cardiac output, and extreme hypoxemia. The illness is selflimited; the toddler dies in 3 to 5 days or utterly recovers with no aftereffects. Treatment includes measures to correct shock, acidosis, and hypoxemia and use of continuous optimistic airway strain to prevent alveolar collapse. R Racemic epinephrine a mix of dextro- and levo-isomers of epinephrine that, when nebulized, can be utilized within the treatment of croup and bronchiolitis. Red blood cells mature purple blood cell (also known as erythrocytes); a biconcave disk about 7 m in diameter that contains hemoglobin confined inside a lipoid membrane. It is the main cellular element of the circulating blood and transports oxygen as its principal operate. The variety of cells per cubic millimeter of blood is often maintained between four. For instance, a rise to a level of eight million/mm3 can usually happen at over 10,000 toes above sea stage. New erythrocytes are produced at a price of slightly greater than 1% a day; thus a relentless degree is usually maintained. Acute blood loss, hemolytic anemia, or continual oxygen deprivation could cause erythrocyte production to increase greatly. Maturation proceeds from a stem cell (promegaloblast) via the pronormoblast stage to the normoblast, the final stage earlier than the mature grownup cell develops. Relative shunt a capillary shunt exists when blood flows from the proper side of the heart to the left 612 Glossary Restrictive lung dysfunction restrictive respiratory illness is caused by conditions that restrict lung enlargement, similar to fibrothorax, obesity, a neuromuscular disorder, kyphosis, scoliosis, spondylitis, or surgical removal of lung tissue. Characteristics of restrictive respiratory disease are decreased compelled expired very important capacity and total lung capability, with elevated work of respiration and inefficient trade of gases. Acute restrictive circumstances are the most common pulmonary explanation for acute respiratory failure. Rhinitis irritation of the mucous membranes of the nose, often accompanied by swelling of the mucosa and a nasal discharge. Serum clear watery fluid, particularly that moistening surfaces of serous membranes or exuded irritation of any of those membranes; the fluid portion of the blood obtained after removing of the fibrin clot and blood cells; generally used as a synonym for antiserum. Shunt to flip away from; to divert; an irregular passage to divert flow from one path to one other. Shunt-like effect pulmonary capillary perfusion in extra of alveolar ventilation; generally seen in patients with continual obstructive lung issues and alveolar-capillary diffusion defects. Sign an objective finding as perceived by an examiner, similar to fever, a rash, or the whisper heard over the chest in pleural effusion. Many signs accompany symptoms; for example, erythema and a maculopapular rash are often seen with pruritus. Smooth muscle muscle tissue that lacks crossstriations on its fibers, is involuntary in action, and is discovered principally in visceral organs. Soft palate the structue composed of mucous membrane, muscular fibers, and mucous glands, suspended from the posterior border of the hard palate forming the roof of the mouth. When the taste bud rises, as in swallowing and in sucking, it separates the nasal cavity and the nasopharynx from the posterior part of the oral cavity and the oral a half of the pharynx.

Generic oxytrol 5 mg amex
For example 5 medications post mi order oxytrol 5 mg, in the same patient symptoms nausea headache fatigue 5 mg oxytrol effective, a bradycardia pulse generator with 6 years of longevity underneath nominal pacing parameters might attain its replacement time in 2 years at one excessive or more than 10 years on the different extreme. Although such capacity is clearly helpful, it also can devour significant battery capability if done too frequently; thus it becomes one more necessary issue for consideration in gadget longevity. In general, the two other largest factors to think about are the anticipated frequency of tachyarrhythmia therapies and the percentage of time spent pacing the guts. It is possible for the longevity to range by an element of two to three due to these issues alone. In basic, this requires a battery to have some measurable characteristic, similar to voltage or impedance, which can be related to its state of discharge. Because longevity is a powerful perform of gadget settings, the longevity requirement is typically linked to a specific set of nominal pacing or defibrillation parameters. A detailed knowledge of the variations in battery performance, the changes in load present with pulse generator settings, and the accuracy of the end-of-service measurement circuitry is critical to make certain that these requirements shall be met. Typically, this indicator is designed to occur at least 3 months before the battery voltage drops to a degree that would end in erratic pacing, loss of seize, or lack of other important options. Battery Voltage the most common technique to point out impending battery depletion is to measure the battery voltage. Most trendy devices incorporate a voltage measurement circuit within the type of an analog-to-digital converter. For lithium/iodine batteries, the battery voltage stays relatively fixed throughout most of its discharge underneath low load situations. Voltage characteristics during discharge differ for different battery chemistries. On the opposite hand, implantable batteries are usually designed to have a declining voltage as they near depletion, making voltage measurement a a lot more correct monitor in this region. Some gadgets now change from one mode of measurement to another as the battery is depleted. This is especially true for the lithium/iodine battery because of its significant impedance. The battery voltage is normally measured during regular sensing and pacing operation and not throughout a defibrillation remedy when the battery voltage is depressed. This strategy is possible as a result of most battery designs have a lowered power capability as the battery approaches depletion. In fact, there are often important variations between numerous models provided by a single manufacturer. The first three primarily pertain to older pacemakers that may still be implanted in some sufferers. Recommended replacement time is indicated by a change within the pacing fee to a predetermined fixed rate (such as sixty five bpm) or a fractional change in fee (such as a 10% lower from the programmed rate). The magnet-pacing fee decreases in a stepwise fashion associated to remaining battery life. In trendy pacemakers the battery voltage or the battery impedance may be telemetered to the programming system. All producers provide technical manuals containing tables or graphs that indicate the connection between battery voltage or impedance and the estimated remaining service life of the gadget. This voltage is much much less sensitive to present variances than is the voltage chosen for a lithium/iodine battery as a outcome of the internal resistance of this battery is far decrease than the lithium/iodine battery; so for this method, voltage is a good indicator of remaining service life. Battery Impedance Battery impedance is one other parameter used to sign the elective substitute point. Consumed Charge A last methodology used to indicate remaining battery life has been to measure the cumulative sum of the cost faraway from the battery. This is accomplished by monitoring the present drawn from the battery or the current plus voltage. This methodology requires an correct data of the original deliverable capacity of the battery as a result of the method truly measures the capacity already used, and the amount left must be calculated by subtracting this from the preliminary worth. Blended Methods It is changing into more common to decide remaining battery life by blending two or extra of the methods described above. For example, many battery chemistries produce a relatively unchanging voltage and impedance in the early part of their discharge. The first implant of a pacemaker powered by a lithium/ iodine battery occurred in 1972. They have high energy density and a low price of self-discharge, leading to good longevity and small size. The inherently excessive impedance of the lithium/iodine battery has not been a big drawback as much as now because the current required by fashionable pacemaker circuits is low, sometimes about 10 �A. Note that the much bigger current delivered throughout a (short duration) pacing pulse is drawn from a capacitor, which may recharge between pacing pulses. The voltage and impedance characteristics of the lithium/iodine cell additionally enable the clinician to monitor the approaching end-of-service indication. This battery system is simple, elegant in idea, and inherently immune to many widespread modes of failure, as shall be discussed under. As a result, lithium/iodine batteries have attained a report of reliability unsurpassed amongst electrochemical power sources. Visible on this determine are the central anode with an embedded present collector wire and the iodine cathode that fills a lot of the volume contained in the battery. One of these is the electrical feedthrough that connects the anode to the skin of the cell. The case serves as the positioning of the electrical connection to the cathode, which is in direct contact with the inside of the container. The fill port is the means by which the cathode mixture is introduced into the cell, after which the fill port is hermetically sealed. Near the tip of battery life, the cathode resistance quickly dominates the resistance of the cell, because the cathode becomes lower in iodine content and less conductive. The area of discharge dominated by cathode resistance and declining cell voltage is used to sign the approaching end-of-service for many pacemakers powered by lithium/iodine batteries. For more than 4 decades the lithium/iodine battery system has supplied small, easy, extremely dependable power sources with power characteristics virtually ideally suited to the requirements of cardiac pacing. However, in the late 1990s several device options that required larger power started to emerge. In many circumstances, these peak energy requirements are past the potential of lithium/iodine batteries. These new options embrace elevated use of addressable reminiscence to capture and store information about the electrical exercise of the center, the necessity for faster and longer-range telemetry to transmit this info outside the body, new physiologic sensors, and new therapies with larger energy necessities, such as cardiac resynchronization and remedy of atrial fibrillation. These higher-power features are now being supported by new battery chemistries with similar vitality density to lithium/iodine however a a lot greater power capability. The battery is composed of a lithium anode, a porous polymer separator material, and the porous pressed-powder cathode pellet which are all inserted right into a case which is welded closed. The vitality density of this battery is similar to that of the lithium/iodine battery, but it delivers considerably higher energy.