
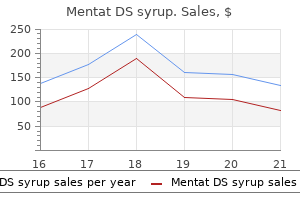
Mentat DS syrup dosages: 100 ml
Mentat DS syrup packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles

Buy mentat ds syrup 100 ml line
Requirements for multidisciplinary care rely upon the extent of related organ involvement medicine cabinet home depot mentat ds syrup 100 ml purchase free shipping. Happle subsequently reviewed the literature and established that the Conradi� H�nermann sort has an X-linked dominant mode of inheritance132 medications54583 mentat ds syrup 100 ml low price. Treatment Case reviews have noted variable enchancment of skin lesions with topical tretinoin or systemic retinoid therapy, however emollients and corticosteroids are ineffective. This speculation displays the role hedgehog signaling is understood to play in conferring left�right asymmetry during embryogenesis. Cholesterol has important capabilities during mammalian development, together with hedgehog signaling, and inborn errors in cholesterol biosynthesis trigger a number of other malformation syndromes. However, ranges of the end product ldl cholesterol sulfate are regular in plasma and fibroblasts due to X-inactivation134,one hundred thirty five. Impaired cholesterol synthesis during a crucial period of mammalian growth is believed to be responsible for the phenotype. The erythroderma resolves considerably, if not completely, within the first weeks or months of life. In older youngsters, hyperkeratosis is essentially replaced by linear or patchy follicular atrophoderma with dilated follicular openings, ice-pick-like scars, and mild residual scaling. The atrophoderma is most pronounced on the forearms and dorsal arms, whereas the palms and soles are usually spared. Hyper- or hypopigmentation alongside the lines of Blaschko may coexist individually from atrophodermic areas132. Nail changes embody onychoschizia and flattening of the nail plate, while the enamel are normal. They embrace frontal bossing, malar hypoplasia, a flat nasal bridge, a short neck, rhizomelic shortening of the limbs, and scoliosis. Widespread premature calcifications manifest as stippling (chondrodysplasia punctata) of the lengthy bone epiphyses, tracheal cartilage, and vertebrae. Unilateral cataracts, which are present at start or develop inside the first months of life, are the most typical ocular abnormality and could additionally be accompanied by microphthalmia or microcornea. Boys with the allelic X-linked recessive syndrome have a collodionlike presentation at delivery and evolution to a variable ichthyosis phenotype133. Additional options embrace cardiovascular, craniofacial, and skeletal anomalies in addition to the Dandy�Walker malformation, hydrocephalus, cataracts, and cryptorchidism. Hyper- and hypopigmentation in "pigmentary mosaicism", incontinentia pigmenti, and epidermal nevi (including epidermolytic variants) observe the lines of Blaschko but lack follicular atrophoderma. Pathology Hyperkeratosis with focal parakeratosis is common and most outstanding in follicular ostia, the place dystrophic calcification may be observed within keratotic plugs. The granular layer is diminished and keratinocytes comprise small vacuoles with needle-like calcium inclusions on electron microscopy. Accumulation of 8(9)cholesterol in plasma may be detected by gas chromatography�mass spectrophotometry in order to confirm the prognosis. Treatment Although the erythema gradually resolves, residual mild scaling may benefit from application of emollients and merchandise containing urea or a keratolytic agent. Additional associated findings embody hyperhidrosis, maceration, blistering, malodor, ache, and fungal infections. The onset and severity of disease expression depend in part on mechanical stress. In addition, substantial variability can usually be observed within the identical family. Patients could suffer from hyperhidrosis, maceration, blisters, fungal infections, malodor, constricting keratotic bands (pseudoainhum), and severe pain. The underlying molecular defect could contain epidermal proteases as well as proteins of the keratinocyte cytoskeleton, cornified envelope, desmosome, or gap junction. Continued 925 Palmoplantar Keratodermas could require referral for cardiac, audiologic, ophthalmologic, or dental analysis. A pores and skin biopsy for histologic examination could provide further diagnostic clues (Table 58. Genetic evaluation is sometimes helpful to establish the specific diagnosis, facilitate identification of affected relations, and enable prenatal analysis. This confusion underscores the necessity for cautious histologic examination and generally multiple biopsy specimens to determine epidermolytic hyperkeratosis. The expression of keratin 9 is proscribed to the suprabasal cell layers of palmar and plantar skin. Clinical options the palmoplantar skin is initially purple, adopted by the looks of thick, yellow hyperkeratosis by 3�4 years of age. In the "tonotubular" subtype, electron microscopy reveals whorls of keratin containing tubular structures11. Histologic findings also include coarse keratohyalin granules, acanthosis, and marked orthohyperkeratosis. The findings of epidermolytic hyperkeratosis are often subtle and patchy, requiring a cautious search and often a quantity of biopsy specimens to allow their identification. Such mutations are extremely disruptive to keratin filament assembly, inflicting tonofilament clumping and cytolysis that end in blistering in addition to hyperkeratosis. Mechanical debridement with a blade or dental drill is useful for problem areas, adopted by software of a keratolytic agent to help keep away from fissure formation. The Gamborg Nielsen (Norrbotten) type23 is presently considered a variant of Mal de Meleda24. Aquaporins are transmembrane proteins that permit the osmotic movement of water across the cell membrane. This gene encodes the serine protease inhibitor family B member 7, which has an unknown protease goal within the skin25. Mal de Meleda is an autosomal recessive situation that was first described in inhabitants of the island of Mljet (Meleda) off the Dalmatian coast. The hyperkeratosis is variably thick and hyperhidrosis is common, with frequent dermatophyte infections and pitted keratolysis. The Bothnia sort includes a characteristic white spongy look upon exposure to water16. Fungal superinfection is widespread, and hyperkeratosis of the fingers could lead to sclerodactyly and digital constrictions (pseudoainhum). The elbows, knees, wrists, and ankles in addition to the dorsal surfaces of the palms and feet could be concerned, and the nails show thickening, koilonychia, and subungual hyperkeratosis. Angular cheilitis and involvement of the lips and perioral pores and skin may be observed19,27. Hyperpigmented macules, melanoma, and Bowen disease inside the keratotic areas have been reported28,29. This disorder is brought on by mutations within the gene encoding loricrin, a glycine-rich cornified envelope protein33�35 (see Ch. Generalized desquamation or options of a collodion baby could additionally be evident at start, with subsequent evolution to a mild generalized ichthyosis.
Trusted 100 ml mentat ds syrup
Most sufferers have peripheral blood eosinophilia medications on backorder mentat ds syrup 100 ml generic without prescription, lymphopenia medications with codeine generic mentat ds syrup 100 ml mastercard, and an increased serum IgE level. Edematouspinknodulesand Reported neoplastic and infectious associations are listed in Table 25. The most commonly related malignancies are T-cell lymphoma and gastric carcinoma28. The dermis is usually normal in look, but it may have mild acanthosis with parakeratosis and delicate spongiosis. A superficial and mid-dermal mixed lymphohistiocytic infiltrate with variable numbers of eosinophils and a few plasma cells can additionally be seen. In these sufferers, the differential diagnosis consists of different causes of erythroderma corresponding to psoriasis, cutaneous T-cell lymphoma, atopic dermatitis, pityriasis rubra pilaris, and drug eruptions (see Ch. In patients with predominantly flattopped pruritic papules, the differential analysis contains lichen planus, pityriasis lichenoides chronica, papular eczema, and lichenoid drug eruption. Introduction Wells syndrome is a cutaneous dysfunction of unknown etiology characterized clinically by edematous (early) to indurated (late) plaques that initially resemble cellulitis. The basic histopathologic findings consist of a diffuse dermal infiltrate of eosinophils plus characteristic "flame figures". History Wells described the first affected person in 1971 as "recurrent granulomatous dermatitis with eosinophilia". Epidemiology Over a hundred circumstances of Wells syndrome have been reported to date, ranging from newborns to patients over 70 years of age. Local hypersensitivity because of so-called "triggers" has been proposed; the latter embrace insect bites or stings, medication, allergic contact dermatitis, an underlying myeloproliferative dysfunction, and infections. Of notice, peripheral lymphocytes isolated from sufferers with Wells syndrome have been reported to show exaggerated responses to mosquito salivary gland extracts33. The infiltrate is most outstanding within the mid to deep dermis, with occasional involvement of the subcutaneous fats, fascia, and skeletal muscle. The superficial dermis might have huge papillary dermal edema to the purpose of subepidermal bulla formation. In addition to intact eosinophils, extracellular eosinophil granules are present in the dermis. In addition, a palisade of histiocytes and a few multinucleated large cells partially surround flame figures. Flame figures can be seen in different disorders by which degranulation of eosinophils happens including arthropod bite and sting reactions, scabies and eosinophilic ulcer of the oral mucosa and fewer typically parasitic infections. Treatment Initial therapy with prednisone 10�80 mg every day ends in dramatic improvement within a few days in most sufferers. Other therapeutic options include minocycline, colchicine, antimalarials, dapsone, griseofulvin, interferon-, and antihistamines. Early on, bacterial cellulitis and erysipelas are the most common medical mimics. The histopathologic findings of both erysipelas and bacterial cellulitis can even embody important edema, but neutrophils are the predominant inflammatory cell in these soft tissue infections. Other causes of pseudocellulitis, together with exaggerated reactions to arthropod bites, are listed in Table seventy four. Reports of Wells syndrome occurring in patients with chronic lymphocytic leukemia and nonHodgkin lymphoma might symbolize the latter. Initially, the lesions are shiny pink, after which they fade to a pink�brown, green, brown, or slate-gray shade. The extremities are most regularly affected, however involvement of the trunk additionally occurs. The most typical systemic criticism is malaise, with fever in lower than 1 / 4 of patients. Precipitating events, together with arthropod bites and stings, have been described in a minority of patients. Toxocara canis and other parasitic infections can current with scientific and pathologic findings resembling Wells syndrome. Other issues that will present with urticarial plaques because of infiltrates of eosinophils are listed in Table 25. Late (mature) lesions of Wells syndrome could clinically, but not histopathologically, resemble morphea. History Prior to 1968, patients with marked blood eosinophilia, within the absence of helminthiasis or allergic illness, had been identified using varied terms. In 2011, consultants from a number of disciplines came to a consensus relating to terminology and classification standards in the course of the Working Conference on Eosinophil Disorders and Syndromes6,forty. Hereditary hypereosinophilia and hypereosinophilia of undetermined significance had been also defined40. While the pathogenesis of the primary and secondary forms is now higher understood (see below), the etiologies of the opposite varieties are probably varied40. These sufferers develop severe pruritus, eczema, erythroderma, and/or urticaria and angioedema. Therefore, patients with such clones should be regarded as having premalignant or malignant T-cell lymphoma and be intently observed43. These patients develop splenomegaly, endomyocardial fibrosis, cardiomyopathy, elevated serum vitamin B12 ranges, and, sometimes, mucosal ulcers. The coronary heart is usually involved, with thrombus formation and development to subendocardial fibrosis and restrictive cardiomyopathy. Mitral or tricuspid valve insufficiency results from tethering of chorda tendineae. The central and peripheral nervous methods may also be affected, along with the lungs and, not often, kidneys52. Embolic events also occur, notably through the thrombotic stage, and constitute a medical emergency because of their likely serious sequelae; cutaneous involvement with splinter hemorrhages and/or nail-fold infarcts may be current and may present the initial clues to thromboembolic disease. Biopsies from papules or plaques occasionally exhibit spongiosis in addition to the dermal infiltrate that usually accommodates a minimal of a few eosinophils. The principal means of eosinophil degranulation is through cytolysis, and eosinophils lyse inside tissues throughout or quickly after infiltration. However, thromboembolic phenomena may produce lesions that mimic vasculitis (see Ch. A history of travel to endemic areas or a suggestive dietary history implicates helminthiasis. In such sufferers, serologic testing for antiStrongyloides antibodies and three stool samples for ova and parasites must be obtained. Inappropriate remedy of Strongyloides stercoralis with systemic corticosteroids or other immunosuppressives might lead to extreme sequelae, including dying. Patients present with signs and signs related to the organ methods affected by eosinophilic infiltrates, and mucocutaneous lesions occur in more than half of all affected individuals.
Diseases
- Glycogen storage disease
- Glutathione synthetase deficiency
- Mansonelliasis
- Galactose-1-phosphate uridylyltransferase deficiency
- Contact dermatitis, allergic
- Oculomelic amyoplasia
Buy 100 ml mentat ds syrup with amex
Variations in severity may rely upon variations within the timing of amniotic rupture or variable expressivity of genetic trait(s) symptoms flu generic 100 ml mentat ds syrup with mastercard. Constriction rings present as circumferential grooves of variable depth on the digits medicine 44334 mentat ds syrup 100 ml discount free shipping, extremities, neck, or trunk; this have to be distinguished from the circumferential creases of the "Michelin tire child" syndrome (see Ch. Deep lesions situated on an extremity could also be associated with distal lymphedema, nerve compression, deformity, or intrauterine amputation. Acrosyndactyly may end up from a constriction band that encircles adjoining digits. Plastic surgery with wound closure via Z-plasty, anterior sheath Y�V plasty, or belly Scarpa fascia launch is indicated for release of constriction bands that limit development, compress underlying nerves, or interfere with vascular and/or lymphatic circulation. Characteristic findings embrace constriction rings and amputations of the limbs and digits that are associated with fibrous bands. Pseudoamniotic band syndrome is a uncommon complication of invasive intrauterine procedures in monochorionic twins. The extrinsic theory postulates that rupture and repair of the amniotic Other Developmental Anomalies Associated With Cutaneous Diseases Skin problems which would possibly be related to cleft lip/palate or congenital digital anomalies are introduced in Tables sixty four. Notethesupernumerary nipplewitha surroundingareolaina typicallocationonthe inframammary 9 1073. The main sections in this chapter are: the origin and performance of the melanocyte the formation and function of the melanosome regulation of melanin biosynthesis. More lately, it was shown that cutaneous melanocytes can also arise from neural crestderived Schwann cell precursors that migrate along nerves to the skin through a distinct ventral pathway7. Presumably, the dying of melanocytes throughout the leptomeninges, inside ear, and skin is liable for the aseptic meningitis, auditory symptoms, and areas of vitiligo, respec tively, seen in patients with the Vogt�Koyanagi�Harada syndrome (see Ch. In the internal ear, notably in the stria vascularis, melanocytes are thought to play a job within the improvement of listening to. Aberrant migra tion or survival of melanocytes inside the internal ear, the iris, and midportions of the forehead and extremities explains the presence of congenital deafness, heterochromia irides, and patches of leukoderma, respectively, in patients with Waardenburg syndrome, the classic neuro cristopathy. Also, aberrant migration or survival of enteric ganglion cells, another neural crestderived cell population, provides an explana tion for the association of aganglionic megacolon (Hirschsprung disease) with Waardenburg syndrome or hardly ever piebaldism. The survival and migration of neural crestderived cells throughout embryogenesis depends upon interactions between particular receptors on their cell surface and extracellular ligands. Transcription elements represent another group of proteins that play an important role throughout embryogenesis. Several of the genes that, when mutated, give rise to Waardenburg syndrome encode transcription components. During embryogenesis, melaninproducing melanocytes are found diffusely throughout the dermis. However, by the top of gestation, active dermal melanocytes have "disappeared", except in three main anatomic areas � the pinnacle and neck, the dorsal features of the distal extremities, and the presacral area10. Some of the dermal melanocytes have clearly migrated into the epidermis, but, given the absolute numbers of cells within the two compartments, apoptosis of pigment cells has additionally occurred. The three websites the place active dermal melanocytes are nonetheless current at the time of birth coincide with the most typical sites for dermal melanocytoses and dermal melanocytomas (blue nevi). Cells which are actively producing melanin are easily recognized in the matrices of pigmented anagen hairs, whereas melanocytes inside the outer root sheath are often amelanotic and tougher to identify11. Melanocytes include a unique intracytoplasmic organelle, the melanosome, which is the location of melanin synthesis and deposition. Compared with frivolously pigmented skin, darkly pigmented pores and skin has melanosomes that comprise more melanin and are bigger; as quickly as transferred to keratinocytes, the melanosomes are singly dispersed and degraded more slowly. Tyrosinase is the vital thing enzyme in the melanin biosynthetic pathway and the two main types of melanin produced in melanocytes are brown�black eumelanin and yellow�red pheomelanin. The production of eumelanin versus pheomelanin is influenced by the binding of melanocyte stimulating hormone to the melanocortin 1 receptor. As a result, repigmentation of patches of vitiligo during which the hairs are still pigmented relies upon activation and subsequent upward migra tion of the melanocytes current in the outer root sheath11. Of observe, melanocyte stem cells have been recognized within the decrease portion of the hair follicle bulge, i. By immunohistochemical staining, melanocytes are recognized throughout the fetal dermis as early as 50 days of gestation13. Melanincontaining melanosomes are recognizable by electron microscopy in the course of the fourth month of gestation. Although the cell physique of the melanocyte sits on a specialised region of basal lamina, its dendrites come into contact with keratinocytes as far away as the mid stratum spinosum. This association of a melanocyte with ~30�40 surrounding keratinocytes to which it transfers melanosomes has been called the epidermal melanin unit14. However, melanocytes fail to form desmo somal connections with neighboring keratinocytes; their interactions with keratinocytes are via cadherins. In different phrases, a person who has minimal baseline pigmentation and an lack of ability to tan has a similar density of melanocytes in comparison with an individual whose skin is dark brown to black in colour. Several factors play a job in deter mining the level of melanocyte exercise; they embrace particular character istics of the person melanosomes. Several of the enzymes within the melanin biosynthetic pathway are glycoproteins that require the attachment of sugars to have the ability to gain full operate. The targeting of proteins to the plasma membrane versus intracytoplasmic organelles and the targeting of particular proteins to the right type of organelle are difficult processes. It then follows that these patients have dysfunction of a couple of intracytoplasmic organelle, i. The related hypopigmentation could be explained by the failure to effectively deliver melanogenic proteins. As melanin is deposited inside the melanosome, the organelle migrates by way of micro tubules into the dendrites in preparation for transfer into the neighbor ing keratinocytes, both within the epidermis or within the anagen hair matrix. The numerous phenotypes are defined by the tissuespecific expression of those three genes. All three genes are expressed in melanocytes and as anticipated, the related diffuse pigmentary dilution is a mirrored image of a lack of transfer of melano somes from the melanocytes to nearby keratinocytes. Histologically, quite a few melanosomes are seen to congregate within the center of the melanocytes. To reiterate, normal pigmentation of the skin depends on an orderly transfer of melanosomes from melanocytes to keratinocytes. The activity of a melanocyte is reflected in the number and size of melanized melanosomes it pro duces as nicely as in its efficiency at transferring these melanosomes to keratinocytes. The "starting material" for the production of melanin, both the brown�black eumelanin and the yellow�red pheomelanin, is the amino acid tyrosine. Competitive inhibi tors of tyrosinase exercise embody hydroquinone, which is used to treat issues of hyperpigmentation such as melasma, and Lphenylalanine.
Order mentat ds syrup 100 ml without prescription
In continual plaque psoriasis medications you can take during pregnancy 100 ml mentat ds syrup with mastercard, preliminary improvement is noticed between 1 and seven weeks and maximum enchancment could be anticipated after 8�12 weeks of remedy medications you can give your cat 100 ml mentat ds syrup cheap amex. Potential unwanted aspect effects restrict its use to moderate to severe illness immune to topical therapies and photo(chemo)therapy and/or conditions in which these are contraindicated. Based on giant managed research, cyclosporine is a highly effective treatment for the extreme manifestations of psoriasis. Cyclosporine can be utilized safely, provided that the guidelines are strictly followed. Additional/unusual Osteopathy (pain, osteoporosis, compression fractures) Ventricular cardiac arrhythmias Lowered seizure threshold � � *Absolute contraindications. Cyclosporine can produce dramatic speedy improvement of psoriasis, but this have to be balanced by the requirement for an acceptable alternative therapy, given the necessity to finally cease cyclosporine therapy. Guidelines for pre-cyclosporine screening and long-term analysis throughout cyclosporine administration are outlined in Chapter one hundred thirty. An essential aspect is assessment of renal function, and creatinine clearance must be estimated utilizing the Cockcroft�Gault formula: (140 - age in years) � (weight in kg)) serum creatinine (mg/100 ml) � 72 In aged sufferers and patients with a history of hypertension, the risks of renal impairment and hypertension are increased. Although cyclosporine is an immunosuppressive agent, no improve in severe infections has been reported in patients treated with cyclosporine alone. Other side effects include: gastrointestinal discomfort, hypertrichosis, paresthesias, gingival hyperplasia, headache, vertigo, muscle cramps, and tremor79. Metabolic side effects embrace hyperkalemia, hypomagnesemia, hyperuricemia (due to decreased clearance of uric acid), and elevated ldl cholesterol and triglycerides. The efficacy of cyclosporine for psoriasis has been clearly proven in a number of managed and uncontrolled research. Efficacy of cyclosporine has been demonstrated in all variants of psoriasis (including nail psoriasis), however less so for psoriatic arthropathy. Systemic retinoids By the Thirties, vitamin A deficiency was identified to trigger hyperkeratosis of the skin (phrynoderma). Thirty years later, modifications of the vitamin A molecule resulted in the discovery of the so-called first technology of retinoids, including all-trans-retinoic acid (tretinoin) and 13-cis-retinoic acid (isotretinoin). Further analysis resulted within the improvement of the second generation of retinoids, the mono-aromatic retinoids, etretinate and its free metabolite acitretin. Acitretin is an effective treatment for psoriasis, but a major problem with systemic retinoids is their teratogenicity, making contraception obligatory in ladies of childbearing age during remedy and (depending on the drug half-life) for a interval of 1 month (isotretinoin) to three years after discontinuing therapy. Chapter 126 offers a description of the modes of motion, pharmacologic elements, and unwanted effects of systemic retinoids. The efficacy of acitretin monotherapy in chronic plaque psoriasis is proscribed, with roughly 70% of sufferers attaining a reasonable or better response. Combination treatment with photo(chemo)therapy and/or vitamin D3 analogues results in a considerable improvement in medical response. As monotherapy, acitretin is highly effective in erythrodermic and pustular psoriasis. Chapter 128 supplies a description of the modes of motion, dosages, unwanted side effects, and monitoring recommendations for these biologic agents. Biologic therapies are indicated for patients with average to severe psoriasis and/or psoriatic arthritis. Both indications and contraindications for presently commercially available therapies are outlined in Table eight. The relative efficacies of the various biologic brokers are reviewed in Chapter 128. The latter have demonstrated greater efficacy than etanercept86,86a or ustekinumab87,87a in scientific trials. Additional systemic therapies which have been reported as useful in the administration of psoriasis are outlined in Table eight. Aggravating factors such as focal infections, medicines and psychological stress have been described above. The visibility of the lesions and symptoms such as pruritus are relevant factors, and psychoemotional stress and the response of family and friends to the � � � *Frequency varies amongst clinicians. Individual patients report a wide variation with respect to their scientific response to numerous therapies. For instance, some sufferers, even these with widespread disease, could experience wonderful enchancment with a light topical therapy, whereas patients with localized illness may prove recalcitrant to even high-dose systemic remedies. Relative and absolute contraindications to the various treatment options have to be recognized, particularly in the case of photo(chemo) therapy and systemic drugs. Because psoriasis is a chronic situation, patients have to cope not only with their illness, but also with the varied treatments and their costs for prolonged periods of time. For example, particular person circumstances could restrict the time available for intensive day by day therapies. Therefore, remedy choice is a multivariable decisionmaking course of and never a easy stepwise therapeutic ladder. Management with topical brokers It is necessary before instituting topical therapy that the affected person understands that due to the Koebner phenomenon, trauma. For patients with mild to average involvement, topical remedies are the 156 Table 8. Patients with extra widespread involvement can also be handled with a topical agent; however, a excessive degree of compliance is required and this can be difficult to achieve. Evidence for the efficacy of varied topical treatments was reassessed in a recent meta-analysis89. From this analysis, it was concluded that solely very potent topical corticosteroids tended to be more effective than monotherapy with the vitamin D3 analogue calcipotriene. In ambulatory sufferers, calcipotriene was more effective than anthralin, coal tar, the opposite vitamin D3 analogues (tacalcitol and calcitriol), and the retinoid tazarotene. The efficacy of coal tar and anthralin are difficult to assess, as the success of those topicals is extremely dependent on the treatment setting. A day-care or inpatient setting is optimal, as it permits the affected person to more simply deal with the unwanted effects of staining, stinging and irritation. Combination treatment is suggested for the overwhelming majority of patients, thereby growing efficacy and lowering side effects90. For instance, the fixed combination of calcipotriene and betamethasone dipropionate applied as soon as daily proved to be superior to twice-daily calcipotriene or twice-daily betamethasone dipropionate monotherapy. One frequent preliminary strategy is to apply either calcipotriene twice day by day or a potent corticosteroid once day by day for a period four to 8 weeks (except for delicate pores and skin areas and the scalp). In the case of an inadequate response or irritation, one other vitamin D3 analogue or tazarotene could additionally be tried as monotherapy or in combination with a topical corticosteroid. A trial of tar or anthralin could additionally be tried, especially in patients with longstanding disease and incomplete responses or fast relapses.
100 ml mentat ds syrup purchase
An intraepidermal blister cavity just below the granular layer is seen in friction blisters symptoms 5 days before missed period 100 ml mentat ds syrup purchase free shipping, whereas a subepidermal split with sweat gland/follicular necrosis is attribute of coma bullae symptoms enlarged spleen cheap 100 ml mentat ds syrup fast delivery. Based upon the distribution pattern, scientific appearance and histologic findings, multiple fastened drug eruption may be excluded. In non-comatose sufferers, frequent postural modifications assist to resolve and stop the dysfunction. Almost every particular person remembers growing such lesions when carrying a brand new pair of sneakers. They are notably widespread in young and energetic individuals, especially those engaged in the navy and sports activities. Repetition of this rubbing action over a time period can induce the appearance of blisters. Rubbing of moist pores and skin produces higher frictional forces than with very dry or very wet skin15. Clinical Features Friction blisters most regularly develop in areas with thick stratum corneum (soles, heels, palms, fingers). The lesions initially start as erythematous macules at websites of friction and later turn into blisters. The patients complain of an related burning sensation or ache, and the blister fluid could also be clear or blood-tinged. Pathology Friction blisters are intraepidermal blisters ensuing from necrosis of keratinocytes. The stage of the break up is variable however normally within the stratum spinosum just below the stratum granulosum. The roof of the blister is shaped by the stratum corneum, the stratum granulosum, and some mobile debris. Pale and degenerated keratinocytes that stain faintly are found inside the upper portion of the floor of the blister cavity. There is just a sparse perivascular inflammatory infiltrate within the superficial dermis. Vesicles and bullae can develop in a wide range of drug eruptions, that are outlined in Table 33. Introduction Although most insect chew reactions present as pruritic erythematous papules (see Ch. Histopathologically, a leukocytoclastic vasculitis is seen (in addition to a subepidermal blister with epidermal necrosis), which differentiates this entity from other blistering diseases. Epidemiology There seems to be no distinction within the incidence of insect bites primarily based on sex, race or age. Certain people could also be bitten more incessantly because of their physique temperature, odor, use of perfumes, or carbon dioxide excretion. Children tend to have extra severe reactions than adults as a end result of the latter tend to become desensitized by repeated exposures over time. Both humoral (IgE-mediated) and 557 Other Vesiculobullous Diseases military research at a Combat Support Hospital, the prevalence of foot friction blisters was 33% and so they had been extra common in those who were unable to break in their boots14. In the case of bullous mattress bug reactions, cutaneous vasculitis could also be taking half in a role21. Malignant B cells, then again, might stimulate Th2 cells to produce interleukin-5, explaining the associated tissue eosinophilia. Clinical Features 558 Insect bites often appear as intensely pruritic erythematous papules or nodules. Flea bites are the most likely to cause blisters, especially on the legs, and bedbug bites may additionally be bullous. In probably the most extreme reactions, a short course of systemic corticosteroids may be necessary. While systemic corticosteroids can lead to improvement of exaggerated reactions, lesions are inclined to recur when the dose is lowered. History the first report of this phenomenon is attributed to Barker and Cotterill in 1980. However, it seems to happen to a point in virtually every patient with a thermal burn involving more than 30% of the physique surface area27. Most descriptions discuss with sufferers with thermal burns, where delayed blisters have been observed on the spontaneously healed pores and skin, graft donor websites, and graft recipient sites26. They have additionally been seen after pores and skin grafting for toxic epidermal necrolysis and within laser-resurfaced skin28. Pathogenesis Pathology the everyday pattern is that of a superficial and deep perivascular and periadnexal lymphocytic infiltrate with ample eosinophils. During the preliminary part, intraepidermal spongiotic vesicles are current and they can be related to eosinophilic spongiosis. Flame figures (extruded eosinophilic granules aggregated onto collagen fibers which are classically related to eosinophilic cellulitis) could be observed, particularly within the exaggerated reactions seen in sufferers with hematologic malignancies. The antigenic components of the traditional dermal�epidermal junction appear sequentially throughout fetal life or wound healing. Therefore, it has been hypothesized that this phenomenon is due to the improved fragility of a newly synthesized, "immature" dermal�epidermal junction26,27. Clinical Features Tense vesicles or blisters develop several weeks after the injured skin (burned, donor website, recipient site) has utterly healed. In one examine, blisters appeared between 19 and 55 days after the sufferers had sustained their burns, with a mean of 37 days27. Differential Diagnosis the presence of intense pruritus and lesion distribution often suggests a bullous chew response. However, these reactions can mimic bullous pemphigoid, linear IgA bullous dermatosis, bullous erythema multiforme, bullous impetigo, allergic contact dermatitis, and even viral infections. Of notice, the exaggerated reactions described above are additionally referred to as "eosinophilic dermatosis associated with hematological problems" or "eosinophilic dermatosis of hematologic malignancy"24; the time period Pathology Histologically, subepidermal blisters with a minimal inflammatory infiltrate are seen. Electron microscopy has shown that the blisters happen either in the dermis (below the dermal�epidermal junction) or intraepidermally by way of the basal keratinocytes. Bullous dermatitis artefacta (self-inflicted injury)30,31 � Pathogenesis the bullae usually develop on the legs in association with an acute exacerbation of continual edema. This can be because of hypoalbuminemia, congestive coronary heart failure, renal illness, hepatic cirrhosis, venous occlusion (thrombosis) or drugs, particularly calcium channel blockers. With acute exacerbations of continual edema, blisters appear and enlarge slowly to attain a diameter of up to several centimeters. Pathology Marked epidermal spongiosis is observed, with dilated dermal blood vessels and a gentle inflammatory infiltrate. Treatment these blisters resolve quickly when the trigger of the edema is efficiently handled. Diuretics, discontinuation of calcium channel blockers, leg elevation, and compressive bandages (followed by maintenance compression hose) could prove useful. Differential Diagnosis Blistering within the setting of acute edema is often not tough to diagnose. However, the risk of bullous pemphigoid, bullosis diabeticorum, or a bullous drug eruption must also be thought of. Frieden A extensive variety of circumstances could cause vesicles, pustules, bullae, erosions, and ulcerations during the newborn interval and infancy.
Syndromes
- Tissue biopsy
- Worse in the scalp, temples, or back of the neck, and possibly in the shoulders
- Biopsy of the mucus membranes
- Leukemia and other blood cancers
- Fast and weak pulse
- Look the same on both legs
- Will ask the most questions of any age
Mentat ds syrup 100 ml cheap without prescription
The most typical aspect impact of topical retinoids is native irritation leading to erythema treatment brown recluse bite 100 ml mentat ds syrup for sale, dryness symptoms rheumatoid arthritis cheap 100 ml mentat ds syrup otc, peeling, and scaling. This tends to peak after 2�4 weeks of remedy and improve with continued utilization; transient application of a low-potency topical corticosteroid could additionally be of Table 36. Tetracycline derivatives: tetracycline, doxycycline, minocycline (level 1 proof for all 3). Instruct sufferers not to decide or manipulate lesions Provide a written handout together with your particular instructions Recommend additional dependable instructional sources about zits and its treatment. Because of this and the fact that systemic retinoids are identified teratogens, the utilization of topical tretinoin in being pregnant is discouraged. That said, dietary intake of vitamin A has been shown to have a larger affect on serum retinoid ranges than facial software of tretinoin55. Unlike tretinoin, adapalene is light-stable and proof against oxidation by benzoyl peroxide. Tazarotene is a synthetic acetylenic retinoid that, as quickly as applied, is converted into its lively metabolite, tazarotenic acid. Both daily in a single day application of tazarotene and short contact remedy regimens have been shown to be efficient within the treatment of comedonal and inflammatory pimples. It also has gentle comedolytic properties and is particularly efficient when utilized in mixture with different therapies. In contrast to topical antibiotics, microbial resistance to benzoyl peroxide has not been reported. Many preparations for all skin sorts are available in each over-the-counter and prescription formulations. These include bar soaps, washes, gels, lotions, creams, foams, and pads in concentrations starting from 2. As benzoyl peroxide is a bleaching agent, whitening of clothing and bedding can occur. Development of contact dermatitis (irritant > allergic) to benzoyl peroxide is also possible, and this should be suspected in sufferers who develop marked erythema with its use. Topical antibiotics are widely used for the therapy of acne and are available alone in addition to in combination with benzoyl peroxide or a retinoid. Clindamycin and erythromycin characterize the two mostly utilized antibiotics and the formulations range from lotions and gels to options and pledgets (see Ch. It is out there as a topical 20% cream, which has been shown to be effective in inflammatory and comedonal pimples, in addition to a 15% gel marketed for rosacea. It also reverses the altered keratinization of follicles affected by acne and thus demonstrates comedolytic properties. The exercise of azelaic acid against inflammatory lesions could also be larger than its exercise against comedones. Azelaic acid is utilized twice daily and its use is reported to have fewer local side effects than topical retinoids. It is formulated in a 10% lotion, suspension, foam and cleanser, either alone or in combination with 5% sulfur. Of notice, a temporary yellow�orange staining of the pores and skin and hair sometimes happens with concomitant application of topical dapsone and benzoyl peroxide. Delivery methods have been developed to permit a larger concentration of retinoid whereas lowering irritancy, primarily via managed sluggish release. An zits flare might happen through the initial month of therapy with a topical retinoid, however resolves spontaneously with continued utilization. Tretinoin (all-trans-retinoic acid), a naturally occurring metabolite of retinol, was the primary topical comedolytic agent used for the remedy of pimples. To lower the potential for irritation, therapy is often started with a lower-concentration cream formulation of tretinoin and the power later increased. Alternate-night to every-third-night application could also be essential initially, with increased frequency as tolerated. However, Other topical medicines Salicylic acid is a extensively used comedolytic and antibacterial agent (see Ch. In this setting, a major mechanism of action of these medicines is suppression of the expansion of P. However, several of these antibiotics also possess intrinsic anti-inflammatory properties. Details concerning the mechanisms of motion, really helpful dosages, and unwanted facet effects of tetracyclines and macrolides are reviewed in Chapter 127. Recent pointers recommend that the length of oral antibiotic courses for pimples must be restricted to three to 6 months52a,56a,57. Minocycline, a lipophilic by-product of tetracycline, has larger penetration into the sebaceous follicle; although this has been postulated. While doxycycline-related phototoxicity may be problematic, minocycline is associated with a higher incidence of great antagonistic occasions, together with a minocycline-induced hypersensitivity syndrome and autoimmune reactions (see Ch. Hormonal therapy Hormonal remedy is a longtime second-line treatment for female sufferers with acne and could be very efficient, irrespective of whether or not the serum androgen levels are irregular. Although ladies and adolescent girls with acne could have higher serum levels of androgens than these without zits, the levels in pimples patients are often inside the regular range. Combined oral contraceptive tablets, which block each ovarian and adrenal production of androgens, are notably effective for inflammatory zits. A current meta-analysis discovered that oral contraceptive tablets are equal to oral antibiotics in decreasing the number of zits lesions after 6 months of therapy58. Combined oral contraceptive formulations contain an estrogen plus a progestin so as to decrease the danger of endometrial most cancers, which is thought to occur with unopposed estrogen administration. Although progestins have intrinsic androgenic exercise, second-generation progestins. The first is a triphasic oral contraceptive composed of a norgestimate�ethinyl estradiol (35 mcg) combination. The second contains a graduated dose of ethinyl estradiol (20�35 mcg) in combination with norethindrone acetate, whereas the third contains a stable dose of ethinyl estradiol (20 mcg) plus drospirenone (3 mg) with a 24-day dosing regimen. Side results from oral contraceptives include nausea, vomiting, irregular menses, weight gain, and breast tenderness. Agents containing drospirenone can lead to elevations in serum potassium ranges, however this is usually not clinically important in otherwise wholesome individuals. The enhance in threat of venous thromboembolism ranges from 2�4-fold with levonorgestrel or norethindrone to 3. Overall the risk is highest for women over the age of 35 years, smokers, and people with different prothrombotic risk factors such as hereditary thrombophilia63. The standard contraceptive formulation combines cyproterone acetate (2 mg) with ethinyl estradiol (35 or 50 mcg). This preparation is widely utilized in Europe as the therapy of alternative for sexually energetic ladies with hormonally responsive pimples. Approximately 75�90% of sufferers treated with either the standard contraceptive formulation or larger doses of 50�100 mg every day (with or without ethinyl estradiol 50 mcg) show substantial improvement64.
Mentat ds syrup 100 ml purchase amex
In Cockayne syndrome acute treatment generic mentat ds syrup 100 ml with amex, irregular transcription-coupled repair leads to apoptosis of metabolically active cells symptoms you need glasses mentat ds syrup 100 ml purchase online. Pathology By mild microscopy, hair shafts present transverse fractures (trichoschisis) along side an irregular floor and diameter. Occasionally, a nodal look just like trichorrhexis nodosa or 180� twists as in pili torti may be observed. Polarizing mild microscopy is the gold standard for detecting the attribute light and darkish bands, the so-called "tigertail" or "zigzag" sample (see Ch. On transmission electron microscopy, an abnormal arrangement of microfibers as well as an absence of the exocuticle and cuticular A-layer may be seen. If ichthyosis is present, histopathologic changes are usually similar to those found in ichthyosis vulgaris (see above). Other diagnostic checks Molecular testing through gene sequencing and deletion/duplication analysis is available. Hair sulfur content material can be semi-quantitatively analyzed by scanning electron microscopy. Determination of cysteine content material via amino acid analysis of hydrolyzed hair can additionally be potential. Differential Diagnosis Although Cockayne syndrome shares a number of features with the photosensitive form of trichothiodystrophy, the previous lacks ichthyosis and tiger-tail hairs. Likewise, the attribute microscopic hair findings distinguish trichothiodystrophy from different conditions with congenital alopecia or hypotrichosis, including Menkes disease. Symptomatic aid is finest achieved with humectants, keratolytics, and (in more extreme cases) systemic retinoids. Multidisciplinary care is critical to tackle neurologic points and other manifestations. Clinical Features Trichothiodystrophy is characterized primarily by hair, pores and skin, and neurologic abnormalities. The compulsory discovering in every kind is short, unruly, fragile hair of the scalp, eyebrows, and eyelashes because of an abnormally low sulfur content material, i. Eighteen years later, Mendes da Costa presented an in depth medical description of the illness in a mother and daughter, reviewed eight previously reported cases, and coined the name "erythro-et keratodermia variabilis"104. Over the subsequent a quantity of a long time, large Dutch and Swiss kindreds with this condition were described. The first case within the American literature was reported by Barsky and Bernstein in 1964105. The erythematous part is most prevalent during childhood and later slowly subsides. More than 50% of sufferers present at start or in the neonatal interval, and 90% within the first yr of life, with transient erythematous patches that can involve any part of the integument. All reported mutations result in amino acid substitutions of conserved residues, thereby altering the structure/activity of hole junction channels, impairing cytoplasmic 914 a blanched halo. Individual lesions often persist for much less than minutes to hours, although they may last for days. In about 35% of patients, the erythema is preceded or accompanied by a burning sensation, which can cause discomfort. The exceptional variability in number, measurement, shape, location, and duration of erythematous patches is reflected within the name of the disease. Hyperkeratosis evolves simultaneously with or following the appearance of transient erythematous lesions. In roughly half of all patients, the thickening of the pores and skin extends onto the palms and soles, whereas the flexures, face, and scalp tend to be spared. The surface could be ridged, verrucous or velvety, and it could have collarette-like peeling or fantastic, adherent scales. Lesions on the elbows, knees, Achilles tendons, dorsal aspect of the ft, and waistline are particularly frequent and have a tendency to persist for months to years. In a subset of patients with extreme disease, hyperkeratosis is generalized and chronic, with a yellow�brown�gray thickening of the pores and skin and accentuated pores and skin markings. Some sufferers develop thick, dark plates of hyperkeratosis with a spiny, hystrix-like appearance, particularly on the lower extremities. Skin lesions could also be triggered by elements corresponding to emotional stress, sudden temperature changes, mechanical friction, and solar exposure. There are dilated, elongated capillaries with minimal perivascular inflammation in the papillary dermis. Severe papillomatosis with suprapapillary thinning may end in a "church spire" configuration of the epidermis. Ultrastructural studies have had variable results, including a reduced number of lamellar bodies within the granular layer. Other diagnostic exams Molecular genetic testing is out there for the associated genes. The time period "erythrokeratodermia variabilis et progressiva" was proposed to embody each entities109. Nevertheless, the utilization of retinoids ought to all the time be considered fastidiously, since chronic remedy is necessary to avoid relapse and long-term unwanted effects, particularly in youngsters, may ensue. Avoidance of sudden temperature adjustments, friction, and irritation could also be beneficial. The hyperkeratotic plaques slowly increase in number and size throughout childhood, but they have an inclination to stabilize after puberty. Autosomal dominant and, much less regularly, autosomal recessive transmission have been reported. Pathology Acanthosis of the epidermis with basket-weave and often patchy parakeratotic hyperkeratosis is seen. Dilated capillaries and sparse lymphocytic perivascular infiltrates are discovered within the papillary dermis. Occasionally, swollen mitochondria and irregular keratohyalin granules could also be observed. Diffuse palmoplantar keratodermas, especially the transgredient kind described by Greither, could additionally be related to hyperkeratotic plaques on the knees, elbows, and different extensor surfaces. Olmsted syndrome options periorificial and intertriginous erythematous, hyperkeratotic plaques plus mutilating palmoplantar keratoderma, oral leukokeratosis, and alopecia. The presence of perifollicular papules, islands of sparing, and a salmon colour distinguish pityriasis rubra pilaris, whereas psoriasis has characteristic micaceous scale and distinctive histopathologic findings. Treatment Topical keratolytics (-hydroxy acids, salicylic acid) and humectants (urea, propylene glycol) are often not very useful. A subset of sufferers initially presents with bright pink, progressively thickening plaques on the cheeks. Subsequently, a number of case reviews emerged within the literature utilizing totally different names to describe the pores and skin involvement, similar to "atypical erythrokeratodermia with deafness", "atypical ichthyosiform erythroderma", and "ichthyosiform dermatosis". Although several authors argued that the pores and skin findings represent erythrokeratoderma quite than ichthyosis69,117, the widely-used acronym prevailed. All pathogenic mutations identified to date have been heterozygous missense mutations. The first manifestation is commonly transient erythroderma at delivery or during infancy.

Mentat ds syrup 100 ml order overnight delivery
The disease is characterised by numerous 1�2 mm 3 medications that affect urinary elimination cheap 100 ml mentat ds syrup amex, pruritic medicine gif mentat ds syrup 100 ml cheap with amex, skincolored papules, usually pierced by a hair, forming massive areas of what looks like "goose bumps". Six years later, the primary affected person was described within the English literature by Mishima and Rudner18. It can start in the course of the second decade of life and is characterised by background erythema and hyperpigmentation in addition to tiny follicular papules. However, in pores and skin kind I sufferers, there may be only erythema, resulting in vital overlap with keratosis pilaris rubra. Numerous pinheadsized follicular papules are present throughout the involved areas, and they seem relatively hypopigmented. Patients may also have keratosis pilaris of the higher outer arms, with a small rim of erythema surrounding the follicular keratotic plug (see Ch. In a collection of eleven sufferers, topical tacalcitol ointment (daily for 12 weeks) decreased roughness and scaling, however had a limited impact on facial erythema22. Laser remedy of the background erythema or hyperpigmentation may be tried, however it requires multiple classes. Keratosis Pilaris Atrophicans Keratosis pilaris atrophicans encompasses a gaggle of issues in which the abnormality in follicular keratinization is accompanied by atrophy and scarring alopecia. The key features of ulerythema ophryogenes, atrophoderma vermiculatum, keratosis follicularis spinulosa decalvans, and folliculitis spinulosa decalvans are outlined in Table 38. Treatment with keratolytics, topical retinoids, topical or intralesional corticosteroids, oral antibiotics and phototherapy has limited efficacy, but mixture therapy may benefit particular person patients and, anecdotally, oral retinoids and intense pulsed gentle have been reported to result in improvement. In later stages, laser resurfacing, dermabrasion, and/or dermal fillers could help to improve the appearance of atrophic scarring. Pathology There is slight follicular hyperkeratosis with elevated epidermal pigmentation. Diameters of the hair shafts and outer root sheaths are decreased, as is the thickness of the inner root sheath. Both the thickness and the compactness of the sexy layer are often increased20. By quantitative histopathology, a rise within the % area of superficial blood vessels was noticed which correlated with visible grading of the associated erythema21. Differential prognosis the differential prognosis of erythromelanosis follicularis faciei contains primarily keratosis pilaris rubra and a combination of melasma plus telangiectatic erythema from photodamage. However, the latter mixture lacks tiny follicular papules, whereas keratosis pilaris rubra of the cheeks lacks hyperpigmentation and favors children (see Ch. The former entails the anterolateral aspects of the neck with apparent sparing of the midsubmental region. The areas of erythema are a mirrored image of multiple interfollicular telangiectasias. Because the telangiectasias spare the immediate thin rim of skin around every follicle, these areas appear comparatively hypopigmented. Less usually, two disorders inside the spectrum of keratosis pilaris atrophicans, ulerythema ophryogenes and atrophoderma vermiculatum, could additionally be thought-about (Table 38. Atrophoderma vermiculatum impacts the cheeks however presents with honeycomb scarring or a worm-eaten appearance (see Ch. Additional (probably coincidental) associations reported in the literature embrace seborrheic dermatitis, a drug reaction (omeprazole), Hodgkin disease, Crohn disease, syphilis, and an id response to fungal infections. Lichen spinulosus favors the neck, shoulders and extensor surfaces of the arms, in addition to the stomach, buttocks and popliteal fossae, and the distribution sample could additionally be symmetric. Lesions typically arise suddenly in crops, enlarge over a week, after which remain stationary. Idiopathic lichen spinulosus normally seems during childhood and adolescence and is asymptomatic, although in some patients the lesions are pruritic and the patches could additionally be surrounded by faint erythema. Spinulosis of the face (tiny follicular keratotic spicules of the cheeks) may be a manifestation of lichen spinulosus. Grouped,skin-coloredfollicularpapulesonthe extensorsurfaceofthearm Centralkeratoticplugscanbe Pathology Histologically, lichen spinulosus most resembles keratosis pilaris. Topical therapies similar to 12% lactic acid, 20%�40% urea, and 6% salicylic acid may enhance the feel. There are anecdotal stories of profitable therapy with tacalcitol cream or tretinoin gel plus hydroactive adhesive applications. Treatment Differential prognosis the differential prognosis of lichen spinulosus includes phrynoderma, keratosis circumscripta, follicular ichthyosis, and juvenile pityriasis rubra pilaris (Table 38. Phrynoderma Phrynoderma, which implies "toad pores and skin", is seen primarily in Asia and Africa and is uncommon in high-income international locations, except in settings similar to intestinal malabsorption28, anorexia nervosa, or fad diets (see Ch. Phrynoderma is seen most often in affiliation with vitamin A deficiency, but some patients could have measurable deficiencies in different vitamins and/or proven malnutrition29. The lesions are agency, tender, erythematous papules or nodules that measure as much as 2 cm in diameter. Inflammatory response to hair keratin 38 Folliculitis and Other Follicular Disorders 625 Type Barbae Characteristics � � � Lupoid � � � Scarring form of deep folliculitis, usually affecting the beard space; could additionally be brought on by S. Women who shave may also develop pseudofolliculitis barbae, especially within the groin. Multiplefirm hyperpigmented papulesonthelower faceandneck(beard Pathogenesis the disorder is thought to be caused by intrafollicular and transfollicular penetration of tightly curled, coarse hairs inside the beard space. Thus, transfollicular penetration occurs when the minimize hair grows out of the follicle usually but penetrates the skin because it grows in a spiral style back toward the pores and skin floor. Clinical options Differential prognosis In men who shave, inflammatory papules appear within the beard space and on the anterolateral neck. Chronic lesions could cause the hair to create grooves within the pores and skin; the anterior neck and submandibular areas are notably susceptible to this complication. The sharp cut finish of the hair initially causes an invagination in the dermis, which is accompanied by inflammation and regularly by an intralesional microabscess. As the hair penetrates the epidermis, a heavy mixed inflammatory cell infiltrate develops as a response to the downgrowth of the dermis in an try and ensheathe the hair31. This is accompanied by abscess formation throughout the pseudofollicle and a international body large cell response at the tip of the invading hair. Naked Facial acne vulgaris is analogous in appearance, but differs by having comedones in addition to papules and pustules. Histologically, the overseas physique response needs to be differentiated from cutaneous sarcoidosis. Treatment Pathology Before remedy is initiated, the affected person should be given a candid explanation relating to the trigger of pseudofolliculitis barbae. It must be stressed that the one dependable way to cure the illness is to cease shaving, however there are a quantity of treatments that will management the process, together with laser remedy. In these with extreme disease, a hiatus of a quantity of months with out shaving is recommended. When sufferers resume shaving once the inflammatory lesions have completely cleared, they should be given recommendation on shaving strategies (Table 38. Benzashave) may be used in sufferers with delicate to moderate pseudofolliculitis barbae. However, these with severe and chronic disease normally have solely slight enchancment.
100 ml mentat ds syrup purchase otc
Signs and symptoms that time to the risk of a more extreme drug-induced eruption (see Table 21 medications that raise blood sugar mentat ds syrup 100 ml free shipping. Histopathologically medications with acetaminophen mentat ds syrup 100 ml buy generic online, nonspecific findings are typically seen in morbilliform drug eruptions, i. The major entity within the differential analysis of a morbilliform drug eruption is a viral exanthem. Peripheral blood eosinophilia and a polymorphous appearance level to a drug eruption, and within the absence of definitive proof, drug eruptions are favored in adults whereas viral exanthems are favored in youngsters. Usually, the eruption will disappear, however a couple of patients could expertise progressive worsening, leading to erythroderma. Liver, kidney, lung, muscle/heart, pancreas, or different organ and after exclusion of other explanations. Its incidence has been estimated to be between 1 in one thousand and 1 in 10 000 exposures to medication similar to aromatic anticonvulsants. Additional names for this syndrome have arisen partially as a outcome of not all sufferers have peripheral blood eosinophilia20,21. To assist in the medical diagnosis of this disorder, two scoring methods have been proposed as outlined in Tables 21. Immune mechanisms have additionally been implicated based mostly upon several observations including the requirement for sensitization, optimistic pores and skin checks for the wrongdoer drug in some sufferers, and a shorter time-to-onset upon rechallenge23. Fever and a cutaneous eruption are the most common symptoms, seen in 85% and 75% of sufferers, respectively22,32. Vesicles, bullae, erosions, crusts + ** Petechiae, purpura (in morbilliform drug eruptions, may be seen on lower legs) + Viral exanthem. Maculopapular rash creating >3 weeks after beginning remedy with a restricted variety of medication 2. Leukocyte abnormalities (at least one present): (a) leukocytosis (>11 � 109/L); (b) atypical lymphocytes (>5%); and (c) eosinophilia (>1. The face, upper trunk, and extremities are normally the initial websites of involvement. Internal manifestations include lymphadenopathy and hepatic involvement (~80% of patients); hardly ever, the latter might turn out to be lifethreatening (see Tables 21. Patients might develop interstitial nephritis, myocarditis, interstitial pneumonitis, myositis, thyroiditis, and even infiltration of the brain by eosinophils. The cutaneous and visceral involvement might persist for several weeks or months after drug withdrawal, and extra sites of involvement. Prominent peripheral blood eosinophilia is widespread and is a really attribute characteristic. Elevation of hepatic enzymes could be a worrisome discovering and requires serial analysis. The differential diagnosis consists of other cutaneous drug eruptions, acute viral infections, hypereosinophilic syndrome, lymphoma, and pseudolymphoma30. Early withdrawal of the offending drug is necessary, however this will not result in a speedy full restoration. B occur when the dosage is reduced, a slow taper of corticosteroids over a period of several weeks to months is often required33. Urticaria-like lesions, hemorrhagic *Especially when coadministered with valproic acid. Systemic involvement may be very uncommon, however suggestive symptoms are fever, myalgias, arthralgias, and/or headache. Internal manifestations embrace arthritis, nephritis, peripheral neuropathy, and gastrointestinal bleeding. Histopathologic examination of early lesions should be performed and can show leukocytoclastic vasculitis. Vasculitis usually develops 7 to 21 days after drug administration and inside 3 days if a rechallenge. Systemic corticosteroids might profit patients with systemic involvement; in any other case, discontinuing the culprit drug is normally adequate. Prior sensitization (including contact sensitization) would clarify the quick interval (<4 days) between drug administration and the onset of the eruption, as this means an immunologic recall phenomenon. Blood neutrophilia and the buildup of neutrophils within the lesions recommend the discharge of neutrophil-activating cytokines by drug-specific T lymphocytes. Edema of the face and palms, purpura, vesicles, bullae, erythema multiforme-like lesions, and/or mucous membrane involvement are noticed in ~50% of patients37. Lesions sometimes last from 1 to 2 weeks and are adopted by superficial desquamation. In a sequence of 58 sufferers, systemic involvement was detected in a minority (17%) of sufferers, with the primary websites being the liver and kidneys followed by the lungs (acute respiratory distress)38. Edema of the papillary dermis and a perivascular mixed infiltrate with neutrophils and a few eosinophils are often present. Additional laboratory abnormalities embrace delicate to moderate eosinophilia, transient renal insufficiency, irregular liver operate tests, and hypocalcemia. However, the presence of subcorneal pustules in biopsy specimens allows one to distinguish between the two entities. Withdrawal of the responsible drug is the major therapeutic intervention, along side topical corticosteroids and antipyretics. The list of medicine related to drug-induced Sweet syndrome continues to broaden. Following withdrawal of the accountable drug, the fever abates in 1 to 3 days and the lesions disappear within 3 to 30 days43. Systemic exposure to iodine-containing distinction media, irrigation of wounds with povidone-iodine, ingestion of iodide-containing dietary supplements, and the use of amiodarone are extra causes of iododerma. One necessary threat issue for the development of those reactions is acute or continual renal failure. Histologically, accumulation of neutrophils inside the dermis is seen and exocytosis of neutrophils into the dermis can lead to intraepidermal abscesses. Bromodermas and iododermas have to be differentiated from folliculitis, dimorphic fungal infections. Histologic evaluation and measurement of blood levels of iodine (40�92 mcg/L = normal range) and bromide (5�10 mg/ dl = normal range) help in establishing the prognosis. Halogenodermas may persist for weeks after drug withdrawal because of the gradual elimination price of iodides and bromides. Topical and systemic corticosteroids, in addition to diuretics, could hasten resolution, and, in extreme cases, cyclosporine could also be administered. Sweet syndrome is characterized by fever, peripheral blood neutrophilia, and painful erythematous plaques that favor the face and higher extremities and comprise dense neutrophilic dermal infiltrates. In drug-induced Sweet syndrome, the lesions often develop a few week after preliminary drug administration43 and neutrophilia is often absent.
100 ml mentat ds syrup discount visa
Subsequent research in squirrel monkeys 911 treatment center buy generic mentat ds syrup 100 ml, which have digits much like medications during pregnancy mentat ds syrup 100 ml generic with visa those in humans, using in vivo autoradiography provided proof that nearly all, if not all, of the nail plate is generated from the classical matrix175. In these experiments, systemic injection of tritiated thymidine was adopted by amputations at totally different time factors, demonstrating that the thymidine reached the nail plate through the matrix. Injection of radiolabeled glycine into the nail unit of human volunteers who then had nail biopsies additionally showed that the classical matrix is the main supply of the nail plate176. In the early 1990s, Johnson and colleagues177 found that between the distal margin of the lunula and the tip of the nail mattress, the nail plate of the nice toe increases in thickness by ~20%. They inferred from this remark that the nail bed contributed this proportion of the nail plate. These outcomes instructed that the nail plate thickens due to compaction due to distal-to-proximal compression quite than an energetic contribution from the underlying nail bed178. Walking while carrying footwear produces low-grade, repetitive trauma to the free edge of the great toenail, which would explain such an effect178. Immunohistochemical staining with proliferating cell nuclear antigen or Ki-67 demonstrates minimal proliferative exercise in the nail bed however substantial exercise within the matrix, further supporting that the matrix is the source of the nail plate179. The correlation between anatomy and function explains the different patterns of nail disease that end result from pathology affecting the matrix versus the nail mattress (see Table seventy one. It also accounts for the potential for everlasting nail deformity following surgical intervention or biopsy of the matrix, but not for related interventions involving the nail bed. Because the proximal half of the matrix produces ~80% of the nail plate, surgical procedures or biopsies on this space are more doubtless to produce nail dystrophy than those of the distal matrix. Onychocytes migrate upward and distally alongside an indirect axis during their maturation and differentiation; in consequence, the proximal a half of the matrix produces the dorsal portion of the nail plate, while the distal a part of the matrix synthesizes the ventral portion of the nail plate. Abnormalities within the proximal matrix underlie medical findings similar to pitting and longitudinal ridging/splitting, whereas disruption of the distal matrix can cause true leukonychia. In labeling studies, basal cells from the proximal nail matrix continued longer than those from the distal matrix or nail bed165. Nail matrix melanocytes are most plentiful in the distal matrix and are found in suprabasal layers in addition to the basal layer, which can reflect a definite expression pattern of adhesion molecules. The major distribution sample of melanin within the nail plate is pigmented bands, referred to as longitudinal melanonychia, which vary in quantity, intensity, and width relying on their etiology (see Ch. Multiple streaks of longitudinal melanonychia because of active nail matrix melanocytes are generally present in people with darkly pigmented pores and skin, typically on account of trauma or irritation affecting the matrix. In contrast, nail matrix melanocytes in people with frivolously pigmented pores and skin are usually quiescent; longitudinal melanonychia in such patients, particularly an isolated band in an adult, usually requires a nail matrix biopsy to exclude the potential for melanoma (see Ch. Although the immune privilege could stop over-reactivity to environmental antigens, it could also increase vulnerability to human papillomavirus infections and their potential oncogenic effects, which can lead to periungual squamous cell carcinomas186. Collapse of immune privilege has been advised to underlie lichen planus of the nail unit as nicely as lichen planopilaris of the scalp148. Healthy nail Nail Keratins Psoriatic nail de Berker and Angus (1996); de Berker et al. The nail plate and matrix comprise "onerous" hair-type keratins with a massive quantity of sulfur-containing amino acids that facilitate cross-linking between keratin molecules. This reduces the quantity of water associated with these proteins and makes them extra rugged and resistant to chemical destruction in comparison with "delicate" epithelial keratins187. In addition, keratin 15 in the proximal ventral aspect of the proximal nail fold could characterize a marker of a keratinocyte stem cell population182. The sample of keratin expression inside the nail unit explains the involvement of this construction in several genodermatoses which are caused by keratin defects188,189. Nail fragility in addition to alopecia characterize the pure hair�nail ectodermal dysplasia that outcomes from mutations in the gene for keratin eighty five. In these patients, keratin 85 lacks two cysteine residues, which can compromise nail integrity via diminished cross-linking of amino acids within keratins. Courtesy, It has been postulated that the presence of the nail plate overlying the nail mattress inhibits further differentiation of the latter structure. Indeed, if the nail plate is avulsed, the nail bed develops a cornified layer over the next three to 4 weeks. Other molecules and parts throughout the nail plate embody water (normally ~10�15%, compared to ~15�25% for the epidermis), lipids (primarily cholesterol), and minerals. The nail plate is relatively porous and ~1000-fold extra permeable to water than is the epidermis; in consequence, nails may be quickly dehydrated and hydrated. Low water content in nails results in brittleness, while nails composed of >30% water are gentle and opaque. The nail also can contain markers of assorted metabolic processes and exposures to exogenous substances. Biomarkers within the nail plate include glycosylated keratin in sufferers with diabetes mellitus190, high sodium levels in those with cystic fibrosis191, and elevated quantities of lipids in hyperlipidemic individuals192. Exogenous substances which might be found in the nail plate in settings of systemic publicity due to environmental contamination include arsenic, lead, and other heavy metals193,194. Drugs taken for medical functions or recreationally may be present in the nail plate, depending on their binding properties and lipid solubility. Analysis of nicotine in the toenails can be utilized to observe exposure to cigarette smoke through inhalation195, and a spread of narcotics could be identified in nail clippings, either inside deposits beneath the free edge of the nail plate as a outcome of recent direct contact or included into the nail plate by way of systemic exposure over previous months196. When a systemic occasion or local trauma disrupts nail development for a quick period, a transverse groove reflecting the contour of the proximal margin of the matrix seems and grows outward with the affected nail, allowing the timing of the inciting phenomenon to be estimated. Multiple physiologic situations, medical problems and drug exposures can influence nail progress (Table sixty eight. The appearance of decreased nail progress is sometimes explained by substantial thickening of the nail plate that deviates the axis of development such that nail is accumulating upwards within the vertical axis in addition to outward within the longitudinal axis. In these instances, measurement of nail bulk rather than length illustrates that the nails are literally rising, but in a different direction. Factor/condition Age Time of day Seasons Anatomic location Physiologic states Extracutaneous issues Reduction of development Elderly Night Winter Toes Thumb, little finger Fever Poor nutrition Denervation, immobilization Infections. Chapter 68 reviews the construction and performance of the hair follicle in addition to regulation of the hair cycle. The determination to carry out scalp biopsies, hair shaft evaluation, and blood tests is guided by the differential diagnosis. Hair follicle loss could additionally be because of follicular agenesis, dysgenesis, or destruction whereas loss of hair shafts can result from shedding, plucking, miniaturization, or breakage. In alopecia of the scalp, the distribution could be diffuse, patterned, or circumscribed/focal, with androgenetic alopecia and telogen effluvium being the most typical forms of alopecia. In addition, a distinction is made between excessive shedding as in telogen effluvium and hair shaft fragility as in trichorrhexis nodosa due to cumulative cuticular injury or inherited hair shaft abnormalities. Alopecia can also occur in other sites, both at the facet of or independent of scalp alopecia. This article supplies a framework for classification of the alopecias that can facilitate accurate scientific prognosis and affected person administration. Women who develop balding shortly after puberty usually have a positive family history for sample hair loss in both male and female relations.