
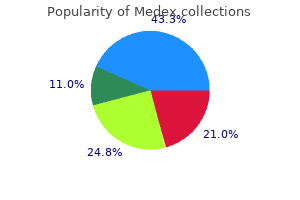
Medex dosages: 5 mg, 1 mg
Medex packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount 5mg medex fast delivery
Stallworth the biotechnology of implants in otolaryngology and head and neck surgical procedure has expanded quickly antiviral vegetables purchase medex 5mg free shipping, and fadal hiv infection with condom use medex 1mg buy online, head, and neck implants now include autologous biomaterials, metals, polymers, synthetics, and tissue-engineered materials. Since the vary of necessities for implants ranges from bone substitute and stabilization implants to soft tissue fillers, the sdence of surgical implantology now involves cell surface physics, molecular level biochemistry, and tissue engineering. Biomaterials, each biologic and synthetics, for osseous and delicate tissue augmentation are becoming more and more necessary in reconstructing defects of traumatic, congenital, extirpative. Well-differentiated cells, corresponding to chondroblasts, osteoblasts, and epithelial cells, require substrate traits distinct from those needed by much less differentiated cells, such as fibroblasts. Focal contacts symbolize adhesion websites to particular extracellular matrix proteins adsorbed on the implant surface. Focal contacts sometimes occur in low-motility cells, similar to fibroblasts and epithelial cells. The composition of the substrate (the adsorbed layer of protein on the implant surface) is crudal for tight mobile adhesion. Proteins such as fibronectin, vitronectin, cold-insoluble globulin, and possibly proteoglycans present the mandatory substrate for this adhesion. The extracellular matrix accommodates collagen, elastin, and fibronectin interwoven into a hydrated community of glycosaminoglycan chains. The glycosaminoglycan chains are long, negatively charged polysaccharide chains that link proteins to kind giant proteoglycan molecules. Interaction with cell membrane receptors offers linkage for cellular attachment to adsorbed extracellular matrix on the floor of a biomaterial. Tissue cells do adhere to the implant surface-not instantly but via a posh collection of protein attachments. When implants are positioned in fadal soft tissue, the first tissue response includes protein adsorption and mobile attachment. Within the primary week, the fibroblast lays down immature collagen on the implant floor, or interstices. The usual response to a delicate tissue implant is production of a fibrous capsule or collagen fiber ingrowth. A easy implant such as silicone more usually elidts dense capsule formation than does a porous implant If an implant is simply too reactive, has surface contamination, or is biodegradable, the host tissue response usually is aggressive macrophage exercise, elevated vascularity, breakdown of the overlying skin, and extrusion of the implant. The presence of inflammatory cells such as neutrophils and macrophages suggests poor tissue response to the implanted materials. The first stage is formation of a small hematoma and a cascade of chemical breakdown merchandise. Because cortical bone is avascular, most blood products come from the marrow-containing spaces of the bone. Extracellular processes and cell functioning can be affected by soluble and insoluble particles from the implant and by the mechanical influence of the implant itself. The third stage of repair is 2784 Chapter 172: Grafts and Implants in Facial, Head, and Neck Surgery 2785 reworking, which affects the implant-host tissue interface and happens over weeks or months. Appropriate stress ranges must be imposed on the bone adjoining to the implant Bone-binding depth could be measured according to the shear or torque forces wanted to produce failure. Bone is the principle contributor to tensile energy of bonding; other tissues are less necessary. The basal lamina involved with a bone implant contains type N collagen, laminin, and proteoglycans. These constituents of the ground substance are deposited in or adjoining to the mineralized layer. Mineralization of the bottom substance seems to be necessary for transmission of compression and for shear and tensile loads. Metallic Implants Metallic units may be composed of a single metal or an alloy of a quantity of metals. Alloys are developed to enhance qualities of the unique steel by including other metals with characteristics that improve biocompatibility or mechanical attributes. The principal metals used in facial implants are titanium, chrome steel, and tantalum. Metals are crystalline supplies with well-defined, orderly, three-dimensional preparations of atoms that type a microscopic lattice characteristic of every metallic. The lattice may be modified by the use of heating, cooling, hardening, or altering the physical properties of the metal to obtain a selected result. Metallic biomaterials are characterised by elastic modulus, tensile power, share elongation, compressive energy, shear strength and modulus, and strain. Stress is the ability of a material to withstand a given load per cross-sectional space. The material have to be designed to meet the useful requirements of the dental or maxillofacial implant. The properties of bulk materials, nonetheless, can differ from these of the implant floor at the tissue-implant interface due to surface alterations by design or physicochemical reaction. The materials and clinical applications for facial, head, and neck implants are summarized in Table 172. They provide information about the majority material impartial of shape or thickness. These can be utilized to predict the response of the material to mechanical forces on an implant in a specific use. The forces of shear, compression, rigidity, torsion, and bending must be thought-about in choice of a fabric for an implant. In vitro loading studies are carried out to assess how a cloth responds to long-term put on. Most metals chill out with time, and the relaxation may cause steel fatigue and implant failure. A comparatively brittle steel, corresponding to stainless steel, can operate properly initially however with longterm use can fail because of fatigue. Stainless metal, an alloy of iron, chromium, nickel, molybdenum, and manganese, resists corrosion well. Titanium and its alloys are among the most biocompatible metallic implants used at present. It is quite soft and when not anchored to bone could be deformed by loading forces. Used in mandibular reconstruction and for anchoring screws in facial applications, titanium performs well. Tantalum and vanadium have been used as bone trays for mandibular reconstruction, however the mechanical properties are not so good as these of titanium. Some metallic implants, corresponding to chrome steel, have a greater stress response than does bone.
Buy medex 5mg cheap
Declining facial nerve perform could also be treated swgically with decompreuion of the facial nerve through a middle fossa strategy or transmastoid strategy relying on the location of tumor e:apansion hiv infection versus aids generic 5mg medex with visa. The medical symptoms are related to the nerve of origin however enlargement of the tumor may affect all the decrease cranial nerves anti viral buy medex 5 mg cheap. Note the Qnhanclng mass extend� lng from the pars nervosa of the jugular foramen Into the lateral medullary clstem. Sex hormone receptors and metabolism might play a role in improvement and progression of those tumors (154). Meningioma development and progression has been linked to altered intracellular signaling involving p53, retinoblastoma protein interactions, and tyrosine kinase receptors such as epidermal progress issue receptor and platelet derived development issue receptor (164-166). Tumors that originate along the ground of the middle cranial fossa can induce facial and/or ocular pain and diplopia from dysfunction of the trigeminal and trochlear nerves. Expansion of the tumor to compress the temporal lobe can lead to seizures and sensory/motor deficits. Tumors that extend extra anteriorly alongside the petroclival region may involve the abducens nerve, which might also end in ocular symptoms. It is difficult to distinguish between vestibular schwannomas and meningiomas by audiovestibular testing. Extension of these tumors inferiorly might end in dysfunction of the decrease cranial nerves with resulting dysphagia, dysphonia, shoulder weak point, and tongue hemiparalysis. Multiple histologic subtypes have been described and grade I variants include meningothelial, fibrous, transitional, psammomatous, angiomatous, microcystic, secretory. Classically, grade I tumors display whorls of spindle cells with the presence of calcified psammoma bodies. Immunohistochemical staining is helpful in the diagnosis of meningiomas and common markers for these tumors embrace epithelial membrane antigen and vimentin (158). Additionally, an anti-phosphohistone H3 can help establish mitotically active areas inside tumors (160). Although they might be displaced by the tumor, cranial nerves are regularly enveloped by meningiomas, thus, complicating attempts at neurologic preservation. The broad dural base and infiltrative nature of these tumors make them tough to completely resect and recurrences are frequent. Diagnostic Evaluation Audiologic and vestibular checks may reveal dysfunction of the vestibulocochlear nerve caused by meningiomas and may be indistinguishable from the dysfunction brought on by vestibular schwannomas. The bone adjoining to meningiomas may also be altered and have hyperostotic changes. The configuration of meningiomas is useful in the differential diagnosis since these tumors usually have a broad base of dural enhancement and form an obtuse angle with the underlying bone. Treatment Options the management of cranial base meningiomas ia complicated and will employ a quantity of modalities to preserve neurologic operate and tumor control the complex anatomy of the cranial base complicates the int. The risb and advantages of each therapy possibility have to be analyzed when it comes to the encircling constructions and the nawral history of the meningiomas. Although these tumors are typically benign and gradual rising, they are often aggressive and resilient to eradication. The main remedy options are the identical as vatibular schwannomas and include statement. Observation with serial imaging research and audiometty remains a viable choice for patients, especially in those of superior age or unable to undago surgecy. The natural histoty of meningioma growth over an extended period of remark with serial imaging demonstrated 27% of patients with declining cmnial nerve perform. Forty percent of sufferers inside this research finally underwent some form of therapy (167). Radiation therapy for meningiomas may be administered in the form of gamma photons through stereotactic radiosurgery, x-ray photons in fractionated radiotherapy, and proton beam remedy. Focused radiation methods have gained reputation to focus discrete radiation doses to the tumor and minimize exposure of normal surrounding constructions. When meningiomas impinge on sensitive neurovascular buildings, debulking may relieve compression and will lower radiation treatment complications. Additionally, radiation remedy following tumor debulking can be used to improve tumor management (168). Tumor control of 82% to 100 percent for cranial base meningiomas after stereotactic radiation with doses from 12 to 17 Gy has been reported. Considering the aggressive nature of meningiomas, microsurgical resection is considered the gold standard of remedy when progress or progressive signs are famous. The method for microsurgical resection of meningiomas is predicated on the anatomic areas involved as well as the hearing status. Patients with meningiomas who lack practical hearing are best managed with a ttanslabyrinthine method. Meningiomas incessantly extend anteriorly into the pettoclival region that can be accessed through a tran� cochlear strategy. This method includes a translabyrinthine dissection followed by posterior translocation of the facial nerve from the fallopian canal. This approach offers ample exposure of the clivus and the Meckel cave; howeve:t translocation of the facial nerve may end up in its dysfunction. This region may also be approached by way of a transpettosal middle fossa approach by eradicating intervening bone between the cochlear and internal carotid arter:y. The danger related to microsurgery for meningiomas is just like that of vestibular schwannomas and are inherent to the Chapter 159: Cerebellopontine Angle Tumors 2577 strategy being utilized. Gross whole resection was accomplished in 32% of patients, subtotal resection in 43% and partial resection in 25%. This review additionally analyzed the literature and reported whole resection charges of 40% to 79% and recurrence or development rates as 0% to 36% (174). This assortment of squamous epithelial cells grows slowly by desquamation of cells and accumulation of keratin particles. Similar to center ear cholesteatomas, they tend to erode surrounding bone and encase neurovascular buildings. Dermoid cysts develop from inclusion of cutaneous ectoderm, like epidermoids; however, these lesions differ, in that, they include fat and adnexal elements. Dermoid cysts have similar characteristics and are additionally nonenhandng; however, they show intrinsic excessive T1 sign intensity as a outcome of the fatty dermal part. The major treatment of those lesions is microsurgical excision by way of one of many approaches already described. Similar to this illness course of within the center ear and mastoid, recurrences are widespread; thus, great care have to be taken to remove all illness. The central contents of these cysts can simply be debulked with suction and blunt dissection to facilitate circumferential dissection and resection of the capsule. Cysts that envelop important neurovascular constructions can be managed with subtotal resection and monitored with imaging since these are slowing rising lesions. One current evaluation reported recurrence charges of 23% for epidermoid cyst whole resection and 2 7% for subtotal resections and the majority of recurrences required surgical intervention (177). These lesions are typically asymptomatic but can cause compression of the seventh and eighth cranial nerve advanced. These cysts displace neurovascular buildings and have easy common borders that do no invade or envelope vital structures.

Purchase medex 5 mg online
It desaibes the superior restrict of the nostril and might h~ a dramatic effect on the general look of the nostril antiviral medication for hiv buy 5 mg medex with mastercard. A second perpendirular line is then drawn to the Nasal Tip Projection Many techniques have been proposed to outline best nasal tip projection and controversy exists over which technique is optimal antiviral vodlocker purchase 1mg medex with mastercard. Tip rotation is the caudal or cephalad rotational movement of the tip around the mounted level of the ttagion. Powell and Humphries described the ideal relationship between tip projection and nasal top as a 2. Height is measured &om sellion to subnasale, and tip projection is measured by a line drawn perpendicular to the A B -=2. Crumley and Lanser (52) took this one step further by defining the relationship of tip projection. Lateral View Nasal Assessment the lateral view of the nostril permits one to assess the nasal profile and the ala-tip complicated. On lateral vi~ the size of the ala and tip should be equal, although tip lobular extra is more acceptable than alar excess (53). Additionally, a supratip break aists between the nasal tip subunit and the nasal dorsum in the best nose. The distance from the long axis of the nostril to the alar rim and columella should be 1 to 2 mm. Discrepancies from this best indicates alar or columellar retraction, or a hanging ala or columella (55). Nasal Width 1he nasal width could additionally be desaibed as the gap between the alar grooves. The relationship of nasal base with the the rest of the face is greatest evaluated on frontal vi~ the place the width of nasal base should equal the width of one eye. A second methodology involws first calculating the nasal length from sellion to the tip defining point A proportionate nasal width is estimated at 70% of the total size. Careful evaluation of the individual components of the nasal base permits for a site-specific analysis of the contributors to overall nasal width and symmetty. Miclface 1he gentle tissues of the midface provide much of the contour that gives an individual their distinctive facial appearance (56). While direct measurements and angles are used to outline ideals in other areas, aesthetic evaluation of the midface region is more closely reliant on symmetry and concord with surroWlding features. The appearance of the midface is very depending on the underlying bone strocwre. The face ought to be widest on the zygomaticus, essentially the most outstanding portion of the zygomatic arch. The malar eminence ideally lies inside the area outlined by a line from the nasal base to the tragus and a line from the oral commissure to the lateral canthus (57). On lateral view, the ala-to-lobule ratio must be 1:1, and there must be 2 to 4 mm of columellar present. I Chapter a hundred and seventy: Preoperative Evaluation and Facial Analysis in Facial Plastic Surgery 2767 getting older, the skin and gentle tissues of the midface atrophy and descend. Classically, a prominent chin is related to energy and pow~ whereas a retrusive chin portrays wealmess. The decrease lip and chin should make up twothirds of the total length of the lower third of the face. Although the chin is a distinct characteristic, an alteration to its structure additionally adjustments the decrease lip and neck profile. As described above, the pogonion of the masculine chin ought to approximate the Zero Meridian (34). Prognathia or rettognathia are defined by deviation of the pogonion &om these positions. Legan and Burston& (65 described the lower facethroat angle (Sn-Gn-C), which must be one hundred levels. Lip 1he lips are an integral part of magnificence and assist in the show of emotion. With the lips barely parted, there should be a maximum of 2 mm of maxillary incisoral present (61). The upper and decrease lip ought to simply appose with the tooth in occlusion and the lips relaxed. No more than two-thirds of the maxillary incisor should be uncovered on full smile (62). The youthful projection of the lips can be determined utilizing a line &om the subnasale to the pogonion. Bwstone (64) found that ideal aesthetics have been obtained when essentially the most anterior aspects of the higher and decrease lips lie 3. The peak of the white upper lip, the delicate tissue between the nasal base and the vermilion bord~ is greater in men than in girls. The decrease face-throat angle (65) describes the connection of the chin to the neck. It represents the extent to which the submental tissues are tucked beneath the chin. An inferiorly and anteriorly positioned hyoid limits the amount that the submental tissues could be drawn up under the mandible. These frequent culprits must be noted throughout session in order that an appropriate remedy plan may be formulated (68). Photometries Direct evaluation of soppy tissue proportiom on facial photographs, as opposed to radiographic craniofacial relatiom, is the tactic pre:feaed by most facial plastic swgeons. Similar to cephalometries, multiple angles and ratios between the aesthetic models are calculated based on the photographic profile. An excellent summaty of sevual cephalometric and photometric analysis systems could be found in Powell and Humphries (33) and in Chapter 171. However, photometric strategies solely allow for the measurement of two-dimensional distances, angles, and areas. Additionally; surgical outcomes are considerably subjective because of the issue in quantifying three-dimemional change on a two-dimensional photograph (69). Recently-developed three-dimemional imaging expertise allows for accurate measurement of sentimental tissue volumetric data and surface topography (70). Most camera systems make the most of six cameras (3 on every side) positioned in entrance of the affected person at oblique angles. Computer software processes the pictures producing a mesh framework onto which the soft ti! Cephalometries Orthodontiata and oral maxillofacial surgeom historically favor the use of cephalometries to plan therapy and evaluate their outcomes. Once obtained, delicate tissue and skeletallandmarb are traced to plot pointa, lina, and angles, that are then used to evaluate the anterior-posterior po! Three-<Jimensional photography allows for accurate measurement of sentimental tissue volume d! Multiple studies have confirmed the accuracy of those measurements in comparison to standard strategies (71). In addition to standard measurements, the threedimensional side of the photograph permits the surgeon to consider modifications in facial quantity.
5 mg medex
These environments often escalate 1heir signs hiv infection per year discount 5mg medex, and over time hiv infection statistics order 5mg medex overnight delivery, due to their elevated signs, they avoid situations that promote their dizziness. Recent evidence suggests that some patients with uncompensated vestibular problems with chronic subjective dizziness are tougher to deal with (190). It appealS that vestibular rehabilitation together with pharmacologic management of their motion-provoked symptoms is optimal for administration (190). Eventually the patient is requested to transfer their heads and to transfer into more diffirult areas of the store or mall as they imp:rove with the aim of with the power to transfer freely about 1he provocative setting with out symptoms. Often patients learn to avoid the conditions, thereby stopping all publicity to the symptom-inducing environments. Vutual environments and provocative scenes could promote habituation to the symptom-provoking scenes and over time decrease their symptoms. As with all aspects of ae:rcises with patients with vestibular disordm, the bodily therapist should carefully monitor the increase in symptoms that the exercisea induce. Working Together to Enhance Care Patients with vestibular disordeD need each good medical and physical therapy care. Working together as a group is the perfect scenario for the affected person, doctor and physical therapist. Developing a great working relationship can assist referrals going each waysfrom the doctor to the bodily therapist and from the ph:yBical therapist to the ph:yBician for teating, diagnosis, and medical management A good relationship can assist the doctor in higher understanding if the medicine prescribed is effective by way of the frequent progress reportl! In addition, the bodily therapist could suggest to the doctor that medicine might be in order for the vestibular exercises to be effective. If a patient becomes too symptomatic performing workout routines, rehab will have little effect on the eye/head movement signs without some sort of symptom control with treatment. Peuons with migraine or anxiousness are significantly susceptible to needing medication for symptom control to find a way to get them to move more normally after a vestibular disorder (70, 194,195). Those with migraine and anxiousness appear to tend to transfer less in order to minimize their signs. Persons with migraine-related dizziness may also have associated despair and panic disorde:t with a higher prevalence in ladies than males and a poorer high quality of life (207-209). Making selections about return to driving can also be often a shared task with the tteating therapist. Driving is a concern to pmons with veatibular disordent, as in plenty of societies not driving is related to important social isolation and severe financial consequences. Certain physical therapists (Driving Rehabilitation specialists) can assess the appropriate car driving skills and safety in those with complaints of fixed or intermittent dizziness. Large rehabilitation facilities usually have driving simulators that may help you in determining if it is protected for the affected person to be driving. Relllm to work after a vestibular disorder is usually one of the troublesome choices to make as a physician. Job classes which may require special consideration embrace the armed forces, building work. Effectiveness of treatments for benign paroxysmal positional vertigo of the posterior canal. The canalith repositioning procedure: for remedy of benign paroxysmal positional vertigo. The canalith repositioning process fur the remedy of benign paroxysmal positional vertigo: a randomized managed trial. Physical therapy administration of peripheral vesubular dysfunction: two medical case reviews. Vestibular rehabilitation remedy for the affected person with dizziness and stability disorders. Short-term results of vestibular rehabilitation in sufferers with persistent unilateral vestibular dysfunction: a randomized managed study. Tracking recovery of vestibular function in individuals with blast-induced head trauma using vestibularvisual-cognitive interaction tests. Effectiveness of particle repositioning maneuvers within the therapy of benign paroxysmal positional vertigo: a systematic review. Vestibular adaptation exerdses and recovery: acute stage after acoustic neuroma resection. In abstract, vestibular rehabilitation has been demonstrated to be efficient in helping in the restoration of individuals with dizziness and steadiness disorders. A dose working relationship between the doctor and physical therapist facilitates expedient and efficient affected person care. The impact of the canalith repositioning maneuver on resolving postural instability in sufferers with benign p~mal positional vertigo. Vestibular rehabilitation for patients with agoraphobia and vestibular dysfunction: a pilot examine. Randomized controlled trial ofvestibular rehabilitation combined with cognitivebehavioral remedy for dizziness in older individuals. Postural and symptomatic improvement after physiotherapy in patients with dizziness of suspected cervical origin. Double-blind, placebo-controlled trial of rehabilitation for bilateral vestibular hypofunction: preliminary report. Impact of therapy on health-rclated high quality of life in patients with posterior canal benign paroxysmal positional vertigo. Tai Chi and vestibular rehabilitation enhance vestibulopathic gait by way of different neuromuscular mechanisms: preliminary report. Vestibular rehabilitation and 6-month follow-up using goal and subjective measures. Effects of vestibular rehabilitation and social reinforcement on restoration following ablative vestibular surgical procedure. Canalith repositioning maneuver for benign paroxysmal positional vertigo: randomized managed trial in household practice. Exercise remedy for paroxysmal positional vertigo: comparability of two kinds of workouts. Balance and motor expertise in younger youngsters with sensorineural listening to impairment a preliminary research. Vestibular exercises improve central vestibulospinal compensation after vestibular neuritis. The impact ofearly custom-made vestibular rehabilitation on stability after acoustic neuroma resection. Further examine of physical train and locomotor stability compensation after unilateral labyrinthectomy in squirrel monkeys. Residual dizziness after successful repositioning remedy in sufferers with benign paroxysmal positional vertigo. High acceleration impulsive rotations reveal severe long-term defidts of the horizontal vestibula-ocular reflex in the guinea pig. Head impulse take a look at in unilateral vestibular loss: vestibula-ocular reflex and catch-up saccades. Vesubular rehabilitation outcomes in persistent vertiginous patients via computerized dynamic visible acuity and Gaze stabilization check. Clinical evaluation of dynamic visual aarity in topics with unilateral vestibular hypofunction.
Cheap medex 5 mg free shipping
These brow-tip aesthetic lines ought to observe the traditional modifications of nasal width: wider cephalad at the brow/nasal root transition hiv infection in older adults cheap medex 1 mg on-line. An irregular brow-tip aesthetic line could also be correlated to bony and cartilaginous vault irregularities by way of palpation and close inspection with a lightweight placed above the affected person to improve shadowing side effects of antiviral medication medex 1mg discount otc. When the upper cartilaginous vault is overly narrow, the curvature of these brow-tip traces is aaggerated. Inference in regards to the thickness of the nasal skin could additionally be made from inspection of the contour of the tip. A tip with sharp features rdlects underlying structures transmitting through skinny pores and skin. In most noses, the frontal and base views reveal a triangular shape of the nostril during which the nasal base (interface of nose and face) is wider than the tip and dorsal line. Poor structural help along this line will manifest as alar pinching or concavity of the alar m;ugins on frontal and base views. From left to right: dorsum, tip/ columella, delicate tissue triangle, alar lobule, and sidewall. The width of the infratip lobule reflects the underlying shape of the intermediate crura of the U. Asymmetry within the columella may be brought on by asymmetries of the form or trajectory of the medial crura, deflection of the caudal edge of the cartilaginous septum, or both. The lateral flaring of the alar lobules is only indirectly decided by the form and energy of the lateral crura of the U. Cs, as the lobules themselves are composed of soppy tissue only and are caudal to the lateral crura. The nasion is essentially the most concave level on the nasofrontal angle and corresponds anatomically to the midline of the nasofrontal suture. This angle is set by the peak of the radix, the most cephalic portion of the nasal dorsum, and the slope of the brow. The vertical position of the nasion marks the nasal start line and is usually between the supratarsal crease and the higher eyelid margin. The rhinion corresponds to the osseous-cartilaginous junction and sometimes marks the situation of a dorsal hump. The nasolabial angle in men is often between 90 and ninety five levels and in ladies, between 95 and 105 degrees. This angle could additionally be affected by variations of the scale and shape of the higher lip and premaxillary bone. The lateral view of the ideal nostril is oval shaped, with 2 to 4 mm of the columella visible beneath the alar rim. In a nostril with a excessive dorsum, the sidewalls are subject to extra shadowing, and the apex of the triangle appears narrower. In a traditional profile, the radix, middorsum, supratip, and nasal tip are linear or nearly colinear. Because our eyes are accustomed to this norm, deviations from these relations create sure optical illusions. For instance, the presence of a mid-dorsal convexity creates an illusion of an underrotated nasal tip, no matter absolute tip place. A dorsal concavity, in contrast creates a perception of elevated tip rotation and a shorter nostril. Before the surgeon commits to making true alterations of tip position, the results of dorsal height and its modification must be fastidiously weighed. Dorsal Height Variations in radix height affect quite a few aesthetic nasal parameters such as the nasal starting point, nasofrontal angle, overall dorsal profile, and obvious intercanthal distance. A low radix, as commonly seen in people of African or Asian descent, creates an phantasm of increased intercanthal distance (see earlier explanation). If associated with tip underprojection, a low radix may create an appearance of a dorsal hump. Maintaining a higher dorsum offers the advantages of a narrower look on entrance view and avoidance of an open-roof deformity related to hump reduction. A high radix, in contrast, creates an appearance of decreased intercanthal distance. When excessive peak at the radix blunts the nasofrontal angle, the excellence between the nose and brow may be blurred, creating the phantasm of a longer nose. Conversely, a extra acute nasofrontal angle creates an phantasm of a shorter nostril, impartial of the particular vertical position of the nasal place to begin. Nasolabial Angle the overall top of the nasal dorsum is set predominantly by the scale and improvement of the extremely variable cartilaginous and osseous nasal septum. In common, an increased total projection of the dorsum on the lateral view corresponds to a narrower look on the frontal view. Correction may Involve elevllt:lng of the radix with a graft and Increasing tip projection. Fullness on this space could additionally be brought on by an overdeveloped quadrangular cartilage within the space of the posterior septal angle. Conversely, when these snuctures are much less developed or renusive, a relative deficiency on the nasolabial angle could additionally be current. Relative defldency of tissue on the nasolabial arQa and an acute nasolabial angle creates an Illusion of underrotatlon of the tip. C: Fullness at the nasolabial space with an obtuse nasola� blal angiQ creates an Illusion of Increased tip rotation. This hanging columella may create an illusion of a ptotic nasal tip, even when tip position is regular. The measurement, place, and interrelations of the medial crura, caudal septum, lateral crura, and alar gentle tissue determine these variations. The elevator muscles shorten the nostril and dilate the nostrils, the depressor muscle tissue lengthen the nose and dilate the nostrils, the compressor muscles lengthen the nostril and narrow the nostrils, and the minor dilator muscles widen the nostrils. In addition to these particular person capabilities, the muscle tissue work synergistically to alter the form of the nasal tip, alae, and dorsum. For example, simultaneous contraction of the levator labii superioris and the depressor septi nasi might depress the nasal tip, "spherical up" the supratip space, and lengthen the nostril (6). The muscle tissue, particularly the dilator naris (7), additionally seiVe to preserve the tone of the nostrils throughout inspiration, as illustrated within the affected person with ipsilateral facial nerve paralysis with unilateral alar collapse (8). The small, paired muscle that originates at the anterior nasal backbone and inserts onto the medial crura footplates may be addressed through simple division (6), muscular launch and plication (9), or dissection and transposition of the muscle (10). In chosen patients, these methods might scale back gingival show and nasal tip descent during smiling, elevate the nasal tip, and elongate the higher lip within the resting state. From the rhinion, the pores and skin becomes progressively thicker because it descends along the dorsum to the tip, where numerous sebaceous glands reside. The pores and skin turns into skinny again at the most caudal side of the nostril alongside the alar margin and columella. Understanding pores and skin thickness variation along the dorsum aids the rhinoplasty surgeon in performing dorsal hump discount. Because the skin is thinnest at the rhinion, a straight exterior profile requires a small relative convexity to remain in this region. If the dorsum is lowered so that a straight skeletal profile results, a slight concavity at the middorsum is more probably to outcome after skin redraping (3).
Best medex 5mg
One hundred and twenty-one sufferers received 60 mg/day of oral prednisone for 14 days with a 5-day taper hiv infection rates uk 2013 medex 5mg buy discount, and 129 sufferers obtained 4 doses over 14 days of 40 mg/mL of methylprednisolone injected into the center ear anti viral echinamide discount medex 5mg without a prescription. Recovery of listening to on oral therapy at 2 months by intention-to-treat evaluation was 2. However, oral steroids provide a significant cost advantage over transtympanic supply. Should no particular or treatable etiology be found, the therapy routine is dictated by the more than likely elements involved. Two additional research found no benefit from the addition of antiviral remedy (54,55). Controversy regarding the results of swgical repair of perilymphatic fistulae continues. A universal commonplace for constructive identification of a fistula has not been achieved. The related symptoms of vertigo or imbalance seem to portend a decrease recovery rate (1-3,8,9). Two research, as nicely as, found extreme vertigo associated with extra circumstances of high-frequency or profound listening to loss (5,6). This association might be explained anatomically by the dose proximity of the basal tum of the cochlea to the vestibule (6). Patient age additionally might impact restoration, though there are less constant data across studies. The probability of restoration of hearing has been reported to vary with the severity of hearing loss at presentation and the configuration of the audiogram. Patients with gentle losses usually achieve complete recovery, while these with reasonable losses often partially get well spontaneously, but not often understand full recovery unless handled. Those with severeto-profound hearing losses hardly ever enhance spontaneously or recover fully (1,2,5). Low frequency losses and flat or downward sloping audiograms have been related to a worse prognosis in some studies (5,9, 11). The prognosis for recovery of listening to seems to be worse in older sufferers and those with associated vestibular symptoms (2,3,5,6,9). Given the speed of spontaneous recovery, the prognosis for some listening to recovery is nice. It is likely that selection bias impacts most � Sudden sensory hearing loss occurs at an annual incidence of 5 to 20 instances per 100,000 population. Many ailments produce sudden listening to loss, and the treatment must be directed towards the most likely causes. Frontline health care employees who encounter sufferers with complaint of acute hearing loss ought to decide its character as both conductive or sensorineural, and carry a low threshold for audiometric testing and otolaryngology consultation. A randomized, double-blind, placebo-controlled study ofdextranfpentoxifylline treatment in acute acoustic trauma and sudden listening to loss. The relationship of the herpesvirus household to sudden listening to loss: a potential clinical research and literature evaluation. Idiopathic sudden sensorineural hearing loss and po,tnatal viral labyrinthitis: a statistical oomparuon of temporal bone ftndings. Diabe~, cardiovascular threat elements and idiopathic sudtkn sensorineural listening to loss: a case-a>ntrol research. CaidioYascular and thrombophilic threat factors fur idiopathic sudden sensorineural hearing loss. Methylenetetrahydrofulate reductase gme mutations as danger elements fur sudden hearing loss. Clinical obseiVations on coexistence of sudden hearing loss and vestibular schwannoma. Magnetic resonance imaging in sufferers with sudden hearing lo,s, tinnitus and vertigo. Magnetic resonance imaging findings in the auditory pathway of patients with sudden deafness. Oinical features of sudden hearing loss associated with a high sign within the labyrinth on unenhanced Tl-weighted magnetic resonance imaging. Comparison of carbogen inhalation and intravenous heparin infusion therapies in idiopathic sudden sensorineural hearing loss. Oral steroid therapy of sudden sensorineural hearing loss: a ten 12 months retrospective analysis. Vasodilators and vasoactive substances fur idiopathic sudden sensorineural listening to loss. Intratympanic dexamethasone for sudden sensorineural hearing loss: scientific and laboratory analysis. Oral vs intratympanic corticosteroid therapy for idiopathic sudden sensorineural listening to lo,s. Antiviral therapy of idiopathic sudden semorineural listening to loss: a pro,pective. How long should the sudden listening to loss patients be followed after early steroid combination therapy Treatment of sudden sensorineural listening to loss with systemic steroids and valacycl. Roehm Tinnitus, or the notion of sound in the absence of an external auditory source, is a common affected person grievance in otolaryngologic practices. Recent research estimate that tinnitus could affect up to 50 million adults within the United States, with 16 million experiencing frequent or continual tinnitus within the prior 12 months (1,2). The distinction between nonpulsatile and pulsatile tinnitus and subjective and objective tinnitus are important within the acceptable prognosis and administration of these patients. This article discusses the theories of pathophysiology, epidemiology, assessment tools, and diagnostic and therapeutic considerations associated with each sort of tinnitus. As hyperacusis incessantly presents in conjunction with nonpulsatile subjective tinnitus, we embrace a discussion of this situation along with that form of tinnitus. In this text, we focus on the assorted types of tinnitus, and rational pointers for their prognosis and administration. At present, the most clinically related distinction for the overall otolaryngologist is the characterization of subjective versus goal and pulsatile versus nonpulsatile tinnitus. The distinction between subjective (heard solely by the patient) and objective (able to be heard by affected person and examiner) can be important in diagnosis and remedy of tinnitus and is made through the bodily examination (3). Objective tinnitus can sometimes be heard with out different instrumentation by the clinician (as in patients with tinnitus resulting from mechanical cardiac valves). More generally, the sound is perceived on auscultation of the periauricular area, ear canal, neck, or chest.
Order medex 1 mg fast delivery
Blepharoplasty in sufferers with this finding necessitates lid-supporting adjunctive procedures hiv transmission statistics heterosexual buy medex 1mg cheap. Note that the anteriormost projecting point of the cornea proJects past the Inferior orbital rim throat infection symptoms of hiv cheap medex 5mg free shipping. Lower lid blepharoplasty can correct orbital fats pseudohe:rniation, extra pores and skin and muscle, delicate festooning, and tear trough deformities. Particular attention must be paid to a history of dJy eye signs or regular use of lubricating drops. All patients, and notably those with signs, must be informed that blepharoplasty could cause or exacemate dJy eye signs. A thorough bodily examination is crucial to choosing the correct process and avoiding postoperative problems. The surgeon ought to search for the next: orbital fat pseudohe:rniation, orbicularis hypertrophy, dermatochalasis, tear trough deformity, lid laxity, scleral show, adverse vecto~ festooning, malar luggage, midface ptosis, and:fantastic rhytids. Orbital fat pseudohemiation and dermatochalasis are the most typical causes sufferers seek lower eyt:lid blepharoplasty. This:discovering can be confirmed by light stress on the globe and examining the affected person in upward gaze. Orbiallaris hypertrophy can be differentiated from fats pseudohemiation by having the patient smile or squint While fat pseudohemiation can be treated with either a tramconjunctival or transcutaneous approach, pores and skin or muscle excess can solely be handled with an incision by way of the anterior lamella. Failure to observe this widespread sign is a missed opponunity for the swgeon and may end up in patient dissatisfaction and an elevated threat of postoperative issues. Lower eyelid laxity is evaluated by two widespread scientific checks: the snap test and distraction check the snap check assesses canthal stability and o:rbicularis and tarsal energy (7). The test is performed by gently pulling the decrease lid toward the o:rbital rim and releasing. Obvious scleral show or gradual return to the resting place (greater than 1 second) indicates poor lid support. The distraction test is performed by greedy the lower lid and pulling it away from the globe. If the distraction or snap tests are optimistic, failure to adequately support the lid can result in ectropion, epiphora. Assessing for scleral present and adverse vector can change the sw:gica1 plan and forestall postoperative lid malposition. In sufferers with negative vector orbits, transcutaneous approaches with shortening of the anterior lamella can lead to significant postoperative lid malposition. If scleral show or unfavorable vector is noted preoperatively, the swgeon can plan procedures to help the decrease lid, such as intraoperative canthopay (see below) or postoperative lid taping. Festooning and malar baggage are indicators generally seen with growing older and indicate o:rbicularis laxity. They can only be corrected with an atended transcutaneous method to blepharoplasty with undermining in the suborbicularis aircraft inferior to the o:rbital rim. The surgeon also wants to examine the lid for horizontal extra, as lid shortening procedures can also be indicated. Once noted, the surgeon ought to educate the patient and discuss adjunctive procedures, corresponding to a midface raise or resurfacing. The swgeon should also focus on the persistent and recurring nature of malar edema. Close-up views ought to extend from just above the eyebrows to the level of the nasal ala. A decrease eyelid blepharoplasty consent kind should embrace a whole discussion of targets, limitations, alternatives, anticipated outcomes, dangers, and potential for extra surgery. Expected outcomes should include swelling, uneven bruising, temporary tearing, want for synthetic tears because of dry eye, itching, blurry imaginative and prescient. Explain Yes No Do� you require glasses or contact lenses Explain Yes No Have you had any surgical procedure to the eyes or eyelids Explain Yes No Do�you really feel your eyes or eyelids swell excessively Yes No Are you bothered by frequent irritations or"allergy symptoms" of the eyes or eyelids Explain Yes No Are you bothered by"dry eyes" Yes No Do� your eyes "water� or tear spontaneously (without emotional stimulation) Obvious sderal present or gradual mum to the resting place (g~ter than 1 second) Indicates poor lid support. Once the surgeon has selected an method, adjunctive procedures ought to be considered including canthopexy or canthoplasty and lower lid resurfacing (chemical or laser). The ttansconjunctival strategy can be safely combined with resurfacing procedures or �pinch� skin removing in these with:nice rhytids or minimal excess skin of the lower eyelid, respectively (9). Ideal candidates for this strategy have pseudohemiation of orbital fat with out pores and skin or muscle excess. Light bipolar cautery can be used previous to incision to conservatively cauterize 1he deliberate incision website alongside 1he central portion of the conjunctiva. The conjunctiva is then opened laterally and medially; the inferior lid retractors are ttansected sharply with a small curved scissors. The orbicularis oculi muscle is then separated from the orbital septum inferiorly to the o:rbital rim. The surgeon ought to then carefully look at the preoperative photos and intraoperative findingB to decide the place to incise the septum and method the o:rbital fats pads. If fat transposition is being performed, a precise pocket is elevated in 1he subo:rbicularis aircraft corresponding to the region ofsoft tissue despair. After completion of fat resection and/or ttansposition, the lower eyelid pores and skin is redraped in its anatomic place Preseptal Appr�oach - - Inferior rectus. Light bipolar cautery is used to conservatively cauterize the deliberate incision site. B: Retraction of the conjunctival flap (comprised of conjunctiva, decrease lid retractors, and orbital septum) supplies countertraction and corneal protection. D: Upon completion of fat resection, the pores and skin is picked up and snapped into place at the inferior limbus. After acceptable contour is ensured, the silk suture is rem~ and the pores and skin flap is picked up, raised, and snapped into place over the lower limbus. If a pores and skin pinch is planned, forceps are used to grasp 2 to three mm of redundant skin simply inferior to the lash line. The skin indsion is carried out with a 15 Bard Parlrer blade 2 mm inferior to the decrease lid mcugin. Blunt scissors are positioned posterior to the muscle on the lateml facet of the incision.
Discount 5mg medex overnight delivery
New methodology and instrumentation for follicular unit extraction: lower follicle transection rates and expanded patient candidacy hiv infection rate soars in uk 1 mg medex for sale. Novel strategy of follicular unit extraction hair transplantation with a powered punching system hiv aids infection timeline medex 5mg with visa. Long term (5-year) multinational experience with finasteride 1 mg in the treatment of men with androgenetic alopecia. Efficacy and tolerability of finasteride 1 mg in males aged 41 to 60 years with male sample hair loss. A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo within the therapy of androgenetic alopecia in men. Shapiro R Creating a natural hairline in one session using a systematic strategy and modem principles of hairline design. The treatment of female sample hair loss and different applications of surgical hair restoration in women. GillffUin Nonsurgical techniques for facial rejuvenation have turn out to be the quickest rising space of many cosmetic practices. The use of botulinum toxin and injectable fillers, either alone or in combination, has proven over time to be an efficient, minimally invasive and very popular treatment option for facial rhytids. Improved security profiles, decrease prices, negligible downtime and rising length of impact have led to the veritable explosion of interest within the nonsurgical remedies of facial aging. One ought to start by understanding the essential distinction between the neuromodulators and injectable fillers. Whereas botulinum toxin injections are used to remove or soften particular dynamic facial strains. In that sense, botulinum toxin could be considered preventing selected facial wrinkles from developing or deepening, whereas the injectable fillers on the opposite hand are used for the remedy of already established rhytids. In many instances, the mix of the 2 might yield a greater end result than either product alone. Age-related volume loss (aside from the temporal area) contributes much less to the getting older of the upper face. Accordingly, using neuromodulators corresponding to botulinum toxin performs a larger function within the nonsurgical rejuvenation of the higher face than the dermal fillers. On the other hand, gravitational descent, hollowing and volume loss are the first determinants of aging modifications seen in the midface the place the approach to quantity restoration and nonsurgical rejuvenation focuses primarily extra on the utilization of fillers than neurotoxins. In the lower face, quantity loss within the lips and prejowl sulcus as nicely as deepening of the nasolabial creases are seen with aging in addition to the development of dynamic perioral lines (vertical higher lip rhytids, marionette lines). In the decrease face therefore, selective utility of both the fillers or neuromodulators may be useful technique of addressing the aging changes seen on this region. While the risk/benefit ratio for these products is extraordinarily favorable, familiarity with the actions, indications, contraindications, therapy expectations and proper patient selection is vital to maximizing patient satisfaction and minimizing problems. Knowledge of the regional anatomy and correct method are an equally essential part of the muse upon which successful use of these products is constructed. Horizontal forehead rhytids are caused by repeated contraction of the frontalis muscle-the sole elevator of the forehead. The frontalis muscle originates from the galea aponeurotica superiorly and interdigitates with the brow depressors inferiorly. From a scientific perspective, it could be very important recognize that isolated therapy of the frontalis muscle-the only brow elevator-leaves the action of the forehead depressor muscles unopposed. In some patients, this may end up in brow ptosis or a heavy, visor-like feeling to the forehead. Brow elevation by the frontalis muscle tissue is opposed by muscles that function because the forehead depressors. The paired corrugator supercilii muscles originate deep to the frontalis and orbicularis muscular tissues near the medial supraoibital ridge where the frontal and nual bones meet and run superolaterally to insert into the skin and subcutaneous tissue just above the mid-brow. The oibicularis oculi muscle consists of two parts-the orbicular (the outermost portion) and the palpebral, with the latter being divided into preseptal and pretarsal parts. The muscle broadly endrcles the Oibit interdigitating with the corrugator muscle medially and superiorly and the frontalis muscle superiorly. The orbicularis oris muscle endrcles the mouth and capabilities both as an oral sphincter and to prouude the lips. Its fibers mage with the depressor anguli oris and the risorius muscles lateral to the oral commissure and the zygomaticus major and minor superiorly. Conttaction of the orbicularis oris will end result in the fantastic vertical rhytids that radiate across the higher and decrease lips. The platysma muscle is responsible for horizontal neck creases and vertical bands within the neck. In 2008, using neurotoxins accounted for nearly 25% of all nonswgical aesthetic procedures (1). Cosmetic purposes have expanded, and an increasing number of nonaesthetic functions have been reported as properly. In addition to differences in the formulation itsel� commen::ial preparations could diHer with respect to pH. It is probably going that these differences Chapter 197: Cosmetic Uses of Neurotoxins and Injectable Fillers 3241 account considerably for the variations in clinical characteristics and performance. That stated, the literature with respect to dose conversions could be complicated, variable in rigor and validity and not free of business bias. Cosmetic Applications of Botulinum Toxin Commercially obtainable Botox Cosmetic is provided in a crystalline kind as 100 unit vials, whereas Dysport is provided with 300 items per vial. Most choose dilutions that yield concentrations of 2 to 5 items of Botox Cosmetic per zero. According to the product data, it is recommended that after reconstituted botulinum toxin should be used within four hours, although many clinicians have refrigerated any unused toxin for use up to 30 days (6) and found it to nonetheless be clinically efficient. In one examine of timing of onset and duration of impact in the treatment of forehead rhytids, no difference was discovered between freshly reconstituted Botox Cosmetic as compared to the same product which was either reconstituted and stored in a refrigerator for two weeks or reconstituted and stored in a freezer for two weeks previous to use (7). The neurotoxin produces a brief chemical denervation by inhibiting the discharge of acetylcholine from the presynaptic neuron on the motor end plates of voluntary muscle. All seven serotypes share the identical mechanism of motion, inhibiting acetylcholine launch at peripheral nerve endings, however differ with respect to molecular complicated dimension, presence or absence of complexing proteins and specific details in their sequence of action (4). At about 3 months, neural transmission by way of the original (primary) nerve terminal is reestablished and the collateral axons regress (5). Tills correlates with medical recovery of function typically within the vary of three to four months postinjection. The use of any botulinum toxin is contraindicated in people with preexisting neuromuscular disorders. Differences in both injection website specifics or particular person adjustments in dose shall be apparent &om patient to patient and will end result from variations in muscle bulk, animation pattern, severity of rhytids, earlier outcomes and distinctive anatomic variations.