
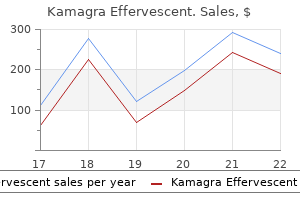
Kamagra Effervescent dosages: 100 mg
Kamagra Effervescent packs: 1 pack, 2 pack, 3 pack, 4 pack, 5 pack, 6 pack, 7 pack, 8 pack, 9 pack, 10 pack

100 mg kamagra effervescent quality
Without them erectile dysfunction protocol scam or real kamagra effervescent 100 mg for sale, cells could be unable to extract enough vitality from the vitamins erectile dysfunction at age 17 100 mg kamagra effervescent cheap with amex, and basically all mobile capabilities would cease. Cardiac muscle cells (cardiomyocytes), for instance, use large quantities of vitality and have far more mitochondria than fat cells (adipocytes), which are much much less lively and use less energy. Furthermore, the mitochondria are concentrated in these parts of the cell liable for the main share of its vitality metabolism. Some mitochondria are only some hundred nanometers in diameter and are globular in shape, whereas others are elongated and are as large as 1 micrometer in diameter and seven micrometers long. Many infoldings of the inside membrane form shelves or tubules called cristae onto which oxidative enzymes are connected. In addition, the inside cavity of the mitochondrion is filled with a matrix that incorporates massive portions of dissolved enzymes needed for extracting energy from vitamins. These enzymes function in association with oxidative enzymes on the cristae to cause oxidation of vitamins, thereby forming carbon dioxide and water and, at the identical time, releasing power. Cell cytoskeleton composed of protein fibers referred to as microfilaments, intermediate filaments, and microtubules. Cells which might be confronted with elevated energy demands-for example, in skeletal muscle tissue subjected to continual exercise training-may improve the density of mitochondria to provide the extra power required. Cell Cytoskeleton-Filament and Tubular Structures the cell cytoskeleton is a community of fibrillar proteins organized into filaments or tubules. As an instance, giant numbers of actin microfilaments frequently occur within the outer zone of the cytoplasm, called the ectoplasm, to form an elastic help for the cell membrane. Intermediate filaments are generally sturdy ropelike filaments that always work together with microtubules, providing energy and support for the fragile tubulin constructions. They are known as intermediate because their common diameter is between that of narrower actin microfilaments and wider myosin filaments found in muscle cells. All cells have intermediate filaments, though the protein subunits of those constructions vary, relying on the cell kind. Specific intermediate filaments found in varied cells embody desmin filaments in muscle cells, neurofilaments in neurons, and keratins in epithelial cells. A particular type of stiff filament composed of polymerized tubulin molecules is used in all cells to assemble strong tubular constructions, the microtubules. Another example of microtubules is the tubular skeletal structure in the middle of every cilium that radiates upward from the cell cytoplasm to the tip of the cilium. Also, both the centrioles and mitotic spindles of cells present process mitosis are composed of stiff microtubules. A major function of microtubules is to act as a cytoskeleton, offering inflexible physical buildings for sure elements of cells. The cell cytoskeleton not only determines cell shape but also participates in cell division, permits cells to move, and offers a tracklike system that directs the movement of organelles in the cells. Microtubules serve as the conveyor belts for the intracellular transport of vesicles, granules, and organelles similar to mitochondria. Nucleus the nucleus is the management heart of the cell and sends messages to the cell to develop and mature, replicate, or die. Comparison of sizes of precellular organisms with that of the average cell within the human body. During mitosis, the chromatin material organizes in the type of highly structured chromosomes, which might then be simply recognized using the light microscope, as illustrated in Chapter 3. The nucleolus enlarges significantly when the cell is actively synthesizing proteins. Formation of the nucleoli (and of the ribosomes within the cytoplasm outdoors the nucleus) begins in the nucleus. Correspondingly, the functions and anatomical organization of the cell are additionally much more complicated than those of the virus. The important life-giving constituent of the small virus is a nucleic acid embedded in a coat of protein. Thus, the virus propagates its lineage from era to generation and is therefore a living structure in the same way that cells and people are living constructions. As life evolved, different chemical substances along with nucleic acid and simple proteins became integral components of the organism, and specialized capabilities began to develop in different parts of the virus. A membrane formed the nuclear envelope, is definitely two separate bilayer membranes, one inside the other. Large complexes of proteins are hooked up on the edges of the pores so that the central area of each pore is simply about 9 nanometers in diameter. Even this size is large enough to permit molecules as much as a molecular weight of 44,000 to move by way of with cheap ease. The nuclei of most cells include one or more extremely staining structures known as nucleoli. In nonetheless later levels of life, notably within the rickettsial and bacterial levels, organelles developed contained in the organism. These represent physical constructions of chemical aggregates that carry out features in a extra efficient manner than what may be achieved by dispersed chemicals throughout the fluid matrix. Finally, within the nucleated cell, nonetheless more complicated organelles developed, the most important of which is the nucleus. The nucleus distinguishes this type of cell from all lower forms of life; it offers a control middle for all cellular actions and for copy of latest cells technology after technology, with each new cell having nearly exactly the same structure as its progenitor. Most substances pass via the cell membrane by the processes of diffusion and lively transport. Diffusion includes easy movement through the membrane caused by the random movement of the molecules of the substance. Substances move by way of cell membrane pores or, in the case of lipid-soluble substances, by way of the lipid matrix of the membrane. Active transport entails actually carrying a substance by way of the membrane by a physical protein construction that penetrates all the way through the membrane. Large particles enter the cell by a specialised perform of the cell membrane referred to as endocytosis (Video 2-1). Pinocytosis means the ingestion of minute particles that kind vesicles of extracellular fluid and particulate constituents contained in the cell cytoplasm. Phagocytosis means the ingestion of huge particles, such as bacteria, whole cells, or portions of degenerating tissue. Pinocytosis occurs frequently in the cell membranes of most cells, but is very fast in some cells. For example, it occurs so quickly in macrophages that about 3% of the entire macrophage membrane is engulfed in the type of vesicles each minute. Even so, the pinocytotic vesicles are so small-usually solely one hundred to 200 nanometers in diameter-that most of them can be seen only with an electron microscope. Pinocytosis is the one means whereby most massive macromolecules, such as most proteins, can enter cells.
Kamagra effervescent 100 mg purchase line
One of the jaws remained stationary while the opposite opened and closed under the management of a mosquito like clamp at the proximal end of the catheter vasculogenic erectile dysfunction causes 100 mg kamagra effervescent discount amex. The degree of curvature of the bioptome might be modified between 45� and 90� by preshaping the shaft and adjusting the diploma of closure of the deal with ratchet mechanism impotence lack of sleep purchase 100 mg kamagra effervescent amex. Spring-loaded adjustable nuts allowed the operator to adjust the amount of force applied with opening and shutting of the surgical like clamp. Because this bioptome was reusable, it required cautious cleaning after every use and in the end wanted retool ing and sharpening of the slicing edges of the jaws after 50 procedures. Richardson13 of Kings College Hospital in London intro duced a smaller-diameter (1. A modification of this bioptome allowed intra cardiac electrocardiographic monitoring (1 980). Although the bioptome allowed easy maneuverability through the vas culature and throughout the tricuspid or aortic valve, the flexible tip required a stylet to be superior into the bioptome shaft earlier than an endomyocardial biopsy could possibly be performed. The preformed sheath is generally superior over an angled pigtail or balloon flotation catheter and remains within the ventricular cavity throughout the biopsy process. In distinction, the preshaped bioptomes are introduced through a short venous sheath and maneuvered as indepen dent catheters to access the right ventricle. They are stiffer and allow greater control of the course and direction of the instrument by the operator. The degree of curvature of the preshaped bioptome can be modified by the operator to suit the angulation required to traverse the tricuspid valve. For the uncommon affected person in whom the comparatively stiff preshaped bioptome fails to enter the right ventricle, biopsy can still be performed by advancing a preformed sheath into the ventricle over either a guidewire or a ballooned-tipped catheter. Disposable biop tomes and sheaths are available for use from the best or left j ugular vein, subclavian vein, femoral vein, or femoral arteries and range in length, form, jaw size, and diameter. They are, however, single-use and disposable gadgets that remove the chance of patient to-patient disease transmission, pyrogen reaction, need for retooling and resharpening of the chopping edges, and mechan ical malfunction generally seen in the earlier reusable devices. Patients normally quick for 8 hours previous to the procedure, however sedative premedications are usually not required for this outpatient procedure. Monitoring through the procedure consists of continuous electrocardiogram, pulse oximetry, and blood pressure. These anatomical features can be recognized more simply by having the patient briefly carry his or her head just off the desk. Internal jugular venous can nulation must be attempted in the center third of the tri angle outlined by the landmarks noted above. In addition, this larger loca tion in the anterior triangle lessens the chance of pneumotho rax. Use of echo guid ance has been demonstrated to improve the frequency of suc cessful vein cannulation, decrease access time, and reduce complication charges. Successful puncture of the interior jugular is facilitated by distension of the vein-in patients with low venous pressure or a small inner jugular vein, this might be achieved by inserting the affected person in a head down Trendelenburg position, elevating the legs on a wedge, or having the affected person perform a Valsalva maneuver during needle development. A 25 -gauge needle is used to apply a small intradermal bleb of 2% Xylocaine at the web site of deliberate sheath entry. A 22-gauge needle is then used to anesthetize the realm from the superficial bleb towards the internal jugular vein. The incision is then expanded with the tip of a mosquito clamp to ensure that the pores and skin will accommodate the 7F venous sheath. In a classic method, the 22-gauge anesthesia needle is directed towards the antici pated venous pathway at an angle of approximately 3 0� to 40� from vertical and 20� right of the sagittal aircraft and is superior in small increments, aspirating earlier than infiltration of small quantities of lidocaine to present native anesthesia. Excess lidocaine infiltration should be avoided, since it could end in venous compression or infiltration of vocal cords or carotid sheath leading to transient hoarseness or Horner syndrome. Once venous blood is aspirated, indicating entry into the internal jugular vein, the operator notes the position and path of the needle, and a second 1 8-gauge single wall puncture needle with syringe is advanced parallel to the "finder" needle. Continuous aspiration is applied because the nee dle is advanced in small increments, particularly in individu als with small internal jugular veins or a low central venous pressure. Usually the "give" of the vein wall is palpable, even before blood return is evident. If the initial makes an attempt at venous entry are unsuccessful, the probing needle is retracted to simply beneath the pores and skin level and redirected more laterally. If venous return continues to be not achieved, the needle may be directed more medially (toward the plane of the carotid artery). Should arterial puncture happen, the probing needle and syringe will spontaneously fill with well-oxygenated blood, and the needle must be removed and compression applied for 5 minutes or till hemostasis is achieved. As described above, this downside can be prevented by utilizing echo steering when the preliminary puncture attempt is unsuccessful. Once this has entered the jugular vein and superior vena cava, the inside cannula and 0. The cannula is then removed, and a 7 or 8 French self-sealing sheath is inserted over the guidewire. This is facilitated by passing the wire from the superior vena cava, throughout the right atrium, and into the inferior vena cava, avoiding runs of ventricular ectopy seen when the wire tip enters the proper ventricle. Once the sheath is in the appro priate position, the guidewire and the dilator are removed, the sheath is aspirated and flushed, and the center biopsy process can proceed. To decrease blood losses and the chance of air aspiration, the needle hub and the hub of the dila tor sheaths should be occluded with a gloved finger dur ing guidewire and sheath exchanges. A additional various is to use a micropuncture vascular access Glidesheath package, which features a 2 1 -gauge needle, a 0. The use of sheaths with hemostatic valves is preferred, as they scale back the danger of air aspiration. The normal website of entry for subsequent coronary heart biopsy is the infraclavicular area, lateral to the world of the bend of the clavicle. The preceding recommendations regard ing anesthesia application and vein entry apply on this case as nicely. The needle is directed medially in a aircraft virtually parallel to the surface of the x-ray desk toward the region of the supraclavicular notch. If that is unsuccessful, approaches more inferior or at a steeper angle to the chest wall can be attempted. In each the internal j ugu lar and subclavian methods, fluoroscopy should be used to be sure that the guidewire is directed downward towards the inferior vena cava or right atrium quite than upward toward the top. Nonetheless, some investigators19 have described using two-dimensional echocardiography, versus fluoroscopy, which the authors consider reduces the danger of perforation. Visualization of the biopsy forceps is technically troublesome and requires con siderable operator and technician experience. We and oth ers19�21 have used echocardiography to biopsy intracardiac lots in the right or left coronary heart, but routinely perform endo myocardial biopsy underneath fluoroscopy. This is facilitated by the reality that the direction of the bioptome head is concordant with that of the handle; nev ertheless, free motion and the specified orientation should all the time be confirmed fluoroscopically.
Cheap kamagra effervescent 100 mg without a prescription
Duplex ultrasound scan ning in the prognosis of renal artery stenosis: a potential evaluation erectile dysfunction pill brands kamagra effervescent 100 mg purchase amex. The utility of duplex ultrasound scanning of the renal arteries for diagnosing significant renal artery stenosis [see comment] impotence with diabetes generic 100 mg kamagra effervescent amex. Noninvasive screening for renal artery stenosis: comparison of renal artery and renal hilar duplex scanning. Stent angioplasty of extreme athero sclerotic ostial renal artery stenosis in sufferers with diabetes mellitus and nephrosclerosis. Four-year follow-up of Palmaz Schatz stent revascularization as treatment for atherosclerotic renal artery stenosis. Validation of Renal Duplex Ultrasound in Detecting Renal Artery Stenosis Post Stenting. The effect of cigarette smoking on train capability in patients with intermittent claudication. Effects on the risk of peripheral vascular issues, myocardial infarction and mortality. Blood oxygen stage de pendent magnetic resonance imaging identifies cortical hypoxia in extreme renovascular illness. Relation between peripheral vascular complications and lo cation of the occlusive atherosclerosis within the legs. Epidemiology of some periph eral arterial findings in diabetic men and women: experiences from the Framingham Study. The impact of intensive therapy of diabetes on the event and progression of long-term issues in insulin-dependent dia betes mellitus. Lp(a) lipopro tein is an impartial, discriminating danger issue for premature peripheral atherosclerosis among white males. Prevalence of hyper homocyst(e) inemia in sufferers with peripheral arterial occlusive illness. Blood viscosity, fibrinogen, and activation of coagulation and leu kocytes in peripheral arterial illness and the conventional population within the Edinburgh Artery Study. Plasma concentration of C-reactive protein and danger of developing peripheral vascular disease. Diagnosis and therapy of chronic arterial insufficiency of the decrease extremities: a crucial evaluation. The ratio of ankle and arm arterial pressure as an unbiased predictor of mortality. Mortality over a interval of 1 zero years in sufferers with peripheral arterial illness. Ankle-arm index as a marker of atherosclerosis within the Cardiovascular Health Study. Color flow Doppler ultrasonog raphy: comparability with peripheral arteriography for the investi gation of peripheral vascular illness. Limi tations of ultrasonic duplex scanning for diagnosing decrease limb ar terial stenoses within the presence of adj acent section illness. Value of color duplex sonog raphy for evaluation of tibioperoneal arteries in patients with femoropopliteal obstruction: a potential comparability with an terograde intraarterial digital subtraction angiography. Ankle/ arm strain index in asymptomatic middle-aged males: an in dependent predictor of ten-year coronary heart illness mortality. A comparison of common femoral waveform evaluation with aorto-iliac duplex scanning in evaluation of aorto-iliac disease. Duplex scanning for diagnosis of aortoiliac and femoropopli teal illness: a potential examine. Magnetic res onance imaging of angiographically occult runoff vessels in periph eral arterial occlusive illness. Value of duplex scanning in contrast with angiography and strain mea surement within the evaluation of aortoiliac arterial lesions. The potential for low er extremity revascularization without distinction arteriography: expertise with magnetic resonance angiography. Does correction of stenoses identified with shade duplex scanning improve infrainguinal graft patency A comparability of strategies for improved visualization of the arteries of the distal lower extremity. Because most cardiac signs are precipitated by exertion or another stress, nonetheless, it could even be important to assess hemodynamic efficiency throughout some form of stress similar to muscular train, pharmacologic intervention. Such an evaluation permits the doctor to assess the cardiovascular reserve and the relationship (if any) Patients with significant heart illness may have totally nor mal hemodynamics when assessed within the resting state during Muscular train, each dynamic and isometric, has been studied extensively in the cardiac catheterization laboratory, understood. There are maj or differences between the hemo dynamic responses to dynamic exercise (done either in the cise, and these two types of exercise are mentioned separately. This is accompanied by an increase in each oxy Some materials on this chapter was developed for earlier editions by Drs. Because carbohydrate metabolism produces extra carbon dioxide than fat metabo lism does, the respiratory quotient (ratio of carbon dioxide manufacturing to 0 consumption) rises from a resting worth of two 0. The supply of bloodborne oxygen and glucose to working skeletal muscle is enhanced within the pres ence of regular vasculature by a reduction in skeletal muscle vascular resistance mediated by metabolic byproducts and by sympathetically mediated vasoconstriction elsewhere, which causes a redistribution of blood away from the renal and splanchnic beds to the exercising muscle. This formula could additionally be used to calculate the expected cardiac index for a given level of zero consumption (X), and a pair of the predicted cardiac index may then be compared with sured in an individual patient is appropriate to the extent of exercise and elevated oxygen uptake. O; minute air flow will increase ing muscle is inadequate, anaerobic metabolism of glucose develops, causing metabolic acidosis and an increase in respi tion to improve oxygen supply. When the intensity and dura 2 tion of train are such that oxygen delivered to the exercis. It is finest to conduct exercise studies in the catheterization laboratory in out of proportion to zero consumption. Beyond this anaerobic 2 threshold, the buildup of hydrogen ions normally causes could be sustained for several minutes. This strategy permits to determine whether or not the increase in cardiac output is appro priate for the rise in zero consumption occurring at that 2 particular degree of train. An train factor < 6 indicates a sub normal response in cardiac output; like exercise index of < zero. This equation can be used to calculate a predicted automotive diac index by measuring 0 consumption during dynamic 2 exercise. Several investigators analyzing the responses of cardiac see below), however increased sympathetic nervous system activity seems to be the most important issue leading to enhanced upright dynamic train and tends to improve linearly in relation to zero consumption. During dynamic supine exercise 2 in the catheterization laboratory, tachycardia is the predomi nant think about increasing cardiac output. Tachycardia exerts a constructive inotropic effect (the so-called treppe phenomenon, stantial decrease within the resistance of the systemic vasculature. Heart price increases constantly throughout each supine and Exercise Factor Another method of using this relationship between cardiac out put and 0 consumption includes calculation of the train 2 issue, which is the rise in cardiac output with train divided by the corresponding enhance in 0 consumption: 2 of supine train in normal subj ects and showed that the increase in cardiac output is caused primarily by an increase in coronary heart fee with a negligible contribution by increased stroke volume. In contrast, studies of older regular subj ects or patients with atypical chest ache diastolic filling and end-diastolic fiber rigidity, resulting in a rise in stroke quantity by means of the Frank-Starling mechanism. Normal women and men can obtain U pright Versus Supine Exercise the contributions of coronary heart price and stroke quantity to cardiac output differ in supine and upright bicycle train.
Discount kamagra effervescent 100 mg otc
It permits mother and father to perceive the nature of the cardiac lesion and to focus on available remedy options and the prognosis to in the end come to an informed choice erectile dysfunction natural cures 100 mg kamagra effervescent order fast delivery. The detection of the cardiac defect may end result within the identification of chromosomal or related extracardiac anomalies that alter the prognosis of an isolated cardiac defect erectile dysfunction after radiation treatment for prostate cancer 100 mg kamagra effervescent. In selected sufferers, fetal cardiac intervention could alter the pure history and enhance outcome. With transposition of the good arteries, outflow tract obstruction or coarctation of the aorta, a reduction in mortality, morbidity and preoperative brain damage has been observed. Question 3 Explain the function of pharmacologic therapy in fetal supraventricular tachycardia: Answer 1 Generally, therapy is only indicated if supraventricular tachycardia is sustained (>50% of the time) or in the presence of hydrops. Digoxin, sotalol and flecainide have been widely used as first-line remedy for supraventricular tachycardia; nonetheless, no randomised controlled trial has been performed to reveal the prevalence of any of those medicine. Answer 6 c and e Question 3 Summarise your arguments for and in opposition to a surgical approach to asymptomatic cystic lung lesions. Moreover, after the second 12 months, the rate of resection for recurrent respiratory infection diminishes, and there have been no resections in those older than 5 years of age. Furthermore, the overwhelming majority of lesions recognized are small and seem to Answer 7 a. Answer 1 In macrocystic lung lesions, the ultrasound options embody a cystic lesion(s) of various measurement within the thorax with or without Self-Assessment e33 proceed to reduce in measurement because the lung grows in youth, with up to 5. A complication rate of 5% to 23% in elective procedures carried out on asymptomatic infants has been described, and these embody air leak, infection, effusion and demise in one case. Type 2 Type 2 Type 3 Type zero Type 1 Type 1 Question 5 Which are true regarding microcystic lung lesions In intralobar pulmonary sequestration, the lesion lies throughout the visceral pleura. Extralobar pulmonary sequestrations at all times communicate with the gastrointestinal tract. All cystic lung lesions require common antenatal follow-up to assess for hydrops and mediastinal shift. Left-sided pulmonary agenesis carries a mortality risk twice that of right-sided agenesis. In right-sided instances, liver herniation is an impartial predictor of postnatal consequence. Gastroschisis is commonly comparatively straightforward to repair but is associated with feeding difficulties in both the quick neonatal interval and infancy. Observed to expected lung space to head circumference ratio in the prediction of survival in fetuses with isolated diaphragmatic hernia. A randomized controlled trial of fetal endoscopic tracheal occlusion versus postnatal administration of severe isolated congenital diaphragmatic hernia. Fetal tracheal occlusion for extreme pulmonary hypoplasia in isolated congenital diaphragmatic hernia: a scientific review and meta-analysis of survival. In general, fetuses with very large kidneys or severe oligohydramnios are likely to have a poor consequence. With regular amniotic fluid volumes and moderately enlarged kidneys (<4 normal deviations), the prognosis appears to be higher with a high likelihood of survival without vital morbidity in infancy. Typically seen late in being pregnant, these foci are defined by their effect on acoustic shadowing. Chapter 33 Question 1 What are the sonographic traits of extreme and terminal fetal renal impairment The circumference of the chest must not be beneath 50% to 60% of the stomach circumference. Answer 1 Progressive growth of severe oligohydramnios in a fetus with a uropathy is suggestive of terminal renal failure. The presence of hyperechogenic renal parenchyma, vital thinning of the cortex (<3 mm), loss of corticomedullar differentiation and cortical cysts are signs of extreme renal damage. Answer 2 e Answer 2 Pyelectasis is defined as a dilation of the renal pelvis only, whereas hydronephrosis consists of a dilatation of both the renal pelvis and the calyces. Measuring the anteroposterior diameter of the renal pelvis is the generally accepted methodology to quantify pyelectasis. A consensus on the ideal threshold value to diagnose urinary tract dilation is missing, but essentially the most accepted cutoff values are four mm within the second trimester and seven mm in the third. Answer three d Answer 3 the analysis of the underlying trigger and the counselling of the dad and mom on the long-term prognosis in circumstances of bilateral, isolated hyperechogenic kidneys and not using a family historical past or renal cysts can be difficult. Isolated hyperechogenic kidneys are most Question four For every of the following sonographic findings, choose which diagnosis fits greatest: a. Chapter 35 Question 1 It is necessary to diagnose micro- or retrognathia prenatally to a. Answer 5 d Chapter 36 Question 1 Describe three of the 4 mechanisms of irregular fluid distribution in hydrops fetalis conditions. Answer 1 b Answer 1 Any three of the next 4 mechanisms: � Increased hydrostatic capillary strain � Reduced intravascular osmotic stress � Obstructed or lowered lymphatic flow � Damaged peripheral capillary integrity Question 2 What is an indispensable view of the fetal face in sufferers at high threat for facial clefts The flipped face view Self-Assessment e37 Question 2 Name the highest three aetiologic categories for nonimmune fetal hydrops. It is the event of maternal oedema in affiliation with fetal hydrops and results in maternal preeclampsia. Question 3 Apart from quick long bones and hydrops, which function is seen in all eight skeletal dysplasia circumstances that are related to nonimmune fetal hydrops Ultrasound features, including massive mass, a suspected diagnosis of teratoma, or signs of obstruction such as polyhydramnios or a small or absent abdomen bubble, increase the chance of airway obstruction. Question 2 Is there an in utero therapy that has a proven profit in sacrococcygeal teratomas In utero remedy must be reserved for fetuses demonstrating signs of in utero compromise. The data are limited for all strategies and will only be provided by skilled operators. Answer 3 Although the overall numbers stay small, information counsel that some fetuses at risk for poor in utero end result could be predicted. Suggestive high-risk options include highly vascular lesions, those with a high progress price (>61 cm3/week) and teratomas with a tumour quantity to fetal weight ratio of greater than zero. It can be necessary to contemplate the morphology of the teratoma because those with a subjective analysis of larger than 50% strong part have poorer outcomes. Question 2 What are the main issues when deciding to intervene for a growth-restricted fetus A gestational age should be chosen when the prospective mother and father would be prepared to assume the dangers of prematurity in a growth-restricted fetus. Existing information provide level I evidence that use of umbilical artery Doppler velocimetry decreases the danger for perinatal mortality. Safety has been shown by retrospective scientific studies and efficacy in a randomised managed trial.
100 mg kamagra effervescent generic with visa
Although angi nalike ache can be seen in sufferers with noncoronary car diac abnormality erectile dysfunction pills cost kamagra effervescent 100 mg purchase on line. In these patients erectile dysfunction pills by bayer buy cheap kamagra effervescent 100 mg, coronary angiography is carried out primarily to look at the extent of underlying atherosclerosis 98 Provoca tive maneuvers to initiate spasm had been as quickly as frequent to con agency the diagnosis and evaluate drug therapy. Ongo ing remedy with any of these brokers may render provocative tests falsely negative. Parenteral nitroglyc erin (1 00-200 mglmL) have to be premixed and loaded in a labeled syringe before the testing begins. It is also advisable to have an intracoronary calcium channel blocker (verapamil 1 00 pg/mL, diltiazem 250 pglmL) or nitroprusside (1 00 pg/mL) close at hand in case nitroglycerin-refractory spasm devel ops. Temporary pacing and defibrillator gear must also be out there to treat the bradyarrhythmias or tachyar rhythmias that sometimes accompany coronary spasm. After each electrocardiogram, coronary angiography is carried out, wanting both at both arteries or solely at the artery of highest scientific suspicion for vasospasm. In the absence of clinical symptoms, electrocardiographic adjustments, or focal coronary vasospasm, the next ergonovine dose is run, and the cycle is repeated till the entire dose of zero. The provocative test must be considered optimistic provided that focal spasm (> 70% diameter stenosis) occurs and is asso ciated with scientific symptoms and/or electrocardiographic adjustments. These brokers are stimulants of the a-adrenergic and serotonin receptors in coronary vascular clean muscle. Testing for coronary spasm must be performed solely after baseline angiographic analysis of each the left and proper coronary arteries. Some operators have used an intracoronary methy lergonovine administration protocol, in which a 4-min ute intracoronary infusion (1 zero 11g/minute in the right and 1 6 11g/minute within the left coronary) is carried out. Alternatively, discrete doses of 5 to 1 zero 11g may be administered into a coro nary artery, waiting for three minutes and imaging between doses (maximal complete dose 50 11g per vessel). These intracoronary protocols may be advantageous in that they produce much less systemic impact (hypertension, esophageal spasm). The same caveats relating to ready availability of potent intracoronary vasodilators to treat spasm also apply to any of these provocational protocols. It can be important to distinguish the extraordinary focal spasm seen in patients with variant angina from the conventional delicate (1 5-20%) diffuse coronary narrowing seen as a phar macologic response to ergonovine in regular patients. Pleating is refractory to nitroglyc erin but resolves immediately when the stiff guidewire is withdrawn. Despite angiographic normality, intravascular ultrasound examination may show regular vessel wall architecture, inti mal thickening, or atheromatous plaque 8 7 In these patients, coronary blood circulate (as described in Chapter 24) might fail to rise normally with pacing tachycardia or train, and the coronary vascular resistance is elevated abnormally. Such an operator can be more likely to misread the angiographic findings, with probably serious medical con sequences. The following discussion summarizes a few of the most common pitfalls that may lead the inexperienced coro nary angiographer to mistaken conclusions. Each maj or vessel should be viewed in an isolated style as if it stands other than different vessels. Usually, the angulated views mentioned earlier in this chapter are essential to visualize clearly the anatomy of the proximal left anterior descending and circumflex arteries. I nadeq uate I njection of Contrast Material the inexperienced operator or assistant has a tendency to hold again on the volume and pressure of inj ection into the coro nary circulation. This results in insufficient or intermittent, pulsatile opacification of the coronary arterial tree as contrast move falls short of peak coronary flow throughout diastole. To the inexperienced operator, this will likely give the impression of whole occlusion of the nonvisualized ves sel. Adequate inj ection to give a continuous (nonpulsatile) reflux of contrast agent back into the sinus of Valsalva will assist the operator to acknowledge ves sels that originate proximally to the catheter tip and thus keep away from the interpretation error of superselective injection. It is seen mostly when the proper coro nary artery is engaged selectively, though it could occur rarely within the left anterior descending artery as well. If coronary narrowing suggests the prevalence of spasm to the operator, sublingual, intravenous, or intracoronary nitroglyc erin must be given and the inj ection repeated. Congenital Variants of Coronary O rig in and D istribution this topic has been discussed earlier in this chapter and in Chap ter 1 6, but it bears reemphasis. Variation in origin and distribu tion of the coronary artery branches may confuse the operator and trigger him/her to mistakenly diagnose coronary occlusion. Double ostia of the proper coronary artery or origin of the circumflex artery from the right coronary artery may be equally complicated and result in misdiagnosis. Myocard ial B rid ges As mentioned earlier, coronary arteries occasionally dip under the epicardial floor under small strips of myocardium. During systole, the phase of the artery surrounded by myocardium is narrowed and appears as a localized steno sis. These myocardial bridges happen most commonly within the distribution of the left anterior descending artery and its diag onal branches. The key to the recognition of those bridges is that the obvious localized stenosis returns to regular dur ing diastole. Recent research using the circulate wire present clear derangement in phasic flow dynamics in muscle bridge seg ments and their normalization by stent placement. Such occlusions are primarily acknowledged by visualization of the distal section of the occluded vessel via collateral channels or by noting the absence of the usual vascularity seen in a selected portion of the heart. Comparison of invasive and conservative strategies after therapy with intravenous tissue plasminogen acti vator in acute myocardial infarction. Read earlier than the Eighth Annual Convention of the American College of Cardiology, Philadelphia, 1959. The coronary angiogram and its seminal contribu tion to cardiovascular medication over five many years. Investigation of the mecha nism of chest ache in sufferers with angiographically normal coro nary arteries using transesophageal dobutamine stress echocardiog raphy. Clinical utility of computed tomography and magnetic resonance methods for noninvasive coronary angiography. Appropriate makes use of of angiographic follow-up in the evaluation of new technologies for coronary intervention. Coronary bypass graft fate and patient consequence: angiographic comply with up of 5,065 grafts associated to survival and reoperation in 1,388 patients throughout 25 years. Electrocardiographic adjustments in selective coronary arteriography: the importance of ions. Pretreatment with corticosteroids to alleviate reac tions to intravenous contrast materials. Use of balloon flotation pacing catheters for professional phylactic temporary pacing throughout diagnostic and therapeutic cath eterization procedures. Lumen diameter of normal human coronary arteries-influence of age, sex, anatomic variation, and left ventricular hypertrophy or dilation. Physiologic basis for assessing important coronary ste nosis-instantaneous move response and regional distribution dur ing coronary hyperemia as measures of flow reserve. Measurement of fractional flow reserve to assess the practical severity of coronary-artery ste noses. Coronary air embolism: incidence, severity, and advised approaches to treatment.
Balsam Oregon (Oregon Fir Balsam). Kamagra Effervescent.
- What is Oregon Fir Balsam?
- Dosing considerations for Oregon Fir Balsam.
- Burns, sores, cuts, heart and chest pain, tumors, and other conditions.
- Are there safety concerns?
- How does Oregon Fir Balsam work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96500
Generic kamagra effervescent 100 mg on-line
An activated clotting time of > 350 seconds is beneficial during retrograde procedures to minimize the danger of thrombosis in the instrumented collateral ves sels erectile dysfunction treatment las vegas cheap 100 mg kamagra effervescent amex. Large-caliber guides enhance assist and permit change of cumbersome units or balloon-trapping strategies stress and erectile dysfunction causes 100 mg kamagra effervescent generic mastercard, whereas long-access sheaths help overcome peripheral vascular tortuosity that may otherwise hinder information efficiency. Techniques to minimize radiation publicity to the affected person and the operator (reducing cine and fluoroscopy frame charges, using "store" fluoroscopy quite than cineangiography when applicable, and utilizing further pro tective shielding) must be employed for these doubtlessly lengthy procedures. If unsuccessful, and if the pathway to the distal lumen is clear, escalation to more and more stiff, nontapered wires is acceptable. A wire-directed retrograde through collaterals to the distal cap can provide a goal for antegrade approach. With a micro catheter within the subintimal space for support, reentry into the distal true lumen is tried with a stiff wire. The Sting ray system (BridgePoint Medical) could be superior over a wire into the subintimal house. Once successful antegrade wiring is achieved, low-profile balloons are used to cross the occlusion to set up a chan nel for stenting. Generally a low-profile over the-wire balloon or a microcatheter is used to assist an extended hydrophilic wire. Once the wire is negotiated into the distal target vessel, retrograde to the distal cap, the septal is dilated with a small balloon (1. A microcatheter is superior to the distal cap and the occlusion is traversed using considered one of a number of strategies, such as antegrade puncture with the retrograde wire as a target, retrograde puncture, or reverse subintimal dissection and reentry. If the lesion is crossed ret rograde, subsequent treatment of the lesion is most simply achieved by crossing this new lumen antegrade and com pleting the process in a normal antegrade fashion. In this approach, maintaining microcatheter place through the septal collaterals is crucial to forestall septal injury during the wire manipulations. The externalized rail can then be used to complete the process in an antegrade fashion. A 55 -year-old man with prior bypass sur gery, together with a vein graft to the primary marginal, presents with unstable angina. The in-stent lesion is deemed low-risk for distal embolization and no-reflow on the time of intervention, and stenting of the lesion is carried out with out distal protection. Although atherectomy and thrombectomy have been tried to stop embolization and its attendant issues, solely the utilization of embolic protec tion gadgets has resulted in a reduction of opposed medical occasions (see Chapter 29). Any debris liberated by intervention stays trapped within the stagnant column of blood and is subsequently aspirated with a unique catheter before the occlusion balloon is deflated to restore antegrade flow. Procedural success with current techniques typically exceeds 90%59 depending partially on the presence of graft degeneration and lesion location. Heart disease and stroke statistics-20 1 2 replace: A report from the American Heart Associa tion. Heart illness and stroke statistics-20 1 three update: a report from the American Heart Associa tion. Heart disease and stroke statistics-20 1 1 replace: a report from the American Heart Associa tion. Decline in charges of dying and coronary heart failure in acute coronary syndromes, 1999-2006. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Systematic evaluate: the comparative effectiveness of percutaneous coronary interven tions and coronary artery bypass graft surgery. Comparison of coronary bypass surgical procedure with angioplasty in sufferers with multivessel disease. Coronary artery by move surgical procedure compared with percutaneous coronary interventions for multivessel illness: a collaborative evaluation of individual affected person data from ten randomised trials. Comparison of early invasive and conservative methods in sufferers with unstable coronary syndromes handled with the glycoprotein lib/Ilia inhibitor tirofiban. Fragmin and Fast Revascularisation During Instability in Coronary Artery Disease Investigators. Successful recanalization of persistent whole occlusions is associated with improved long-term survival. Impact of full revas cularization with percutaneous coronary intervention on survival in patients with a minimal of one chronic total occlusion. The functional reserve of collaterals supplying long-term chronic whole coronary occlusions in sufferers without prior myocardial infarc tion. Survival in subgroups of pa in the era of drug-eluting stents: Impact on antagonistic outcomes. Veterans administra tion cooperative study of surgical procedure for coronary arterial occlusive disease. The bypass surgical procedure on survival patterns in subsets of sufferers with left major coronary artery disease. Comparison of surgical and medical group survival in sufferers with left primary coronary artery dis ease. Stents versus coronary-artery bypass grafting for left main coronary artery disease. Randomized trial of stents versus retrograde method for recanalization of persistent whole occlusions: a step-by-step approach. Catheter Cardiovasc Interv: O f] Soc Cardiac Angiogr f Interv 20 1 2; seventy nine: 3- 1 9. Paclitaxel- versus Sirolimus eluting stents for unprotected left major coronary artery disease. Impact of bifurcation transplant recurrent focal and segmental glomerulosclerosis. Procedural and in hospital outcomes after percutaneous coronary intervention for persistent total occlusions of coronary arteries 2002 to 2008: Impact of novel guidewire techniques. Randomized trial of a distal method on 2-year clinical outcomes in 773 sufferers with distal unprotected left major coronary artery stenosis treated with drug eluting stents. Prediction of left ventricu embolic safety device throughout percutaneous intervention of sa phenous vein aorta-coronary bypass grafts. Evaluation of left ven tricular function three years after percutaneous recanalization of persistent total coronary occlusions. The pul monary circulatory system functions with one-twelfth the resistance to circulate noticed in the systemic vascular bed, in part as a outcome of the massive cross-sectional space of the pulmonary circulation 3 M oreover, a typical proper ventricular systolic strain of 25 mmHg is one-fifth the standard left ventricu lar systolic stress. For instance, occlusion of the pulmonary vasculature owing to pulmonary thromboembolic disease ends in ele vated right-sided pressures as blood is impeded from move Some of the material in this chapter was contributed by Samuel Z. This course of involves all layers of the vessel wall and is char acterized by intimal hyperplasia, medial hypertrophy, adven titial proliferation, and in situ thrombosis. Serotonin Serotonin is a vasoconstrictor that promotes smooth mus cle cell hypertrophy and hyperplasia.
Kamagra effervescent 100 mg buy cheap line
This was felt to reflect enhancements in approach which antihypertensive causes erectile dysfunction kamagra effervescent 100 mg cheap on-line, interventional devices erectile dysfunction drugs associated with increased melanoma risk 100 mg kamagra effervescent discount mastercard, and pharmacotherapy. Despite these limitations, the instant and long term results of angioplasty and endarterectomy had been equiva lent. Subsequently, smaller research confirmed the advantages of carotid stenting, although the potential for distal embo lization and consequent stroke remained a limiting issue (Table 34. To handle this concern, distal protection units were developed to decrease or stop distal embolization. Entry standards included asymptomatic carotid steno sis (> 80% by ultrasound) or symptomatic stenosis (> 50%), plus a minimum of one characteristic placing the affected person at greater threat for surgical endarterectomy. Patients had been screened by a staff including a vascular surgeon, an interventionalist, and a neurologist. C onsensus that the affected person was a great candi date for both procedures was required earlier than randomization; these rej ected as surgical candidates underwent stenting and have been included in a separate stent registry, whereas these rej ected as candidates for intervention underwent surgery and had been included in a surgical registry. Therefore, medical and anatomic features including operator experience ought to information one of the best revascularization technique in patients with severe carotid illness (Table 34. Once a extreme stenosis is iden tified, clinical and anatomical features must be considered and a call concerning the best method must be made at the facet of the affected person and family. We choose premedi cation with aspirin and clopidogrel (at least 300 mg previous to intervention with enough time to achieve efficacy), and pre hydration to decrease hypotension. Although one ought to be cautious and delib erate within the efficiency of those procedures, the variety of complications increases with additional intraarterial time. S) solely atraumatic guidewires ought to be advanced into the interior carotid artery to mini mize the risk of spasm or dissection. Eighth, when encountering resistance during advancement of balloons or stent supply techniques, removing and redilation with lower profile gadgets is suitable. Manipulation inside the area of the carotid sinus may cause both acute and extended hypoten sion and bradycardia,forty nine requiring fluid resuscitation, atropine or a-adrenergic agents. The femoral method is typically used, although the radial method in chosen circumstances is possible and could also be most well-liked. Almost all units are 6F suitable, allowing the usage of an 80-cm-long nonkinkable sheath. Unlike a 90-cm sheath, the 80-cm sheaths are com patible with standard bailout equipments which are usually one hundred em long. Subsequently, the glide wire is advanced into the external carotid artery Occasionally the wire is left in distal widespread carotid artery underneath shut watch not to accidently contact the lesion with sheath manipulation. The sheath is then superior over the diagnostic catheter (or slipcath) within the widespread carotid artery the professional cess might require several iterations of advancing catheters and removing slack from the system to obtain last positioning. Once a desired location is reached, the glide wire and catheter are slowly removed to prevent air trapping. Newer hybrid stents, the place the middle of stent is closed cell however ends are open are being developed. The filtering devices permit for contin uous visualization for precise stent placement and permit cere bral perfusion as antegrade blood circulate is unobstructed. The present filter pore size ranges from 80 to 1 5 zero microns, rais ing the query of what diameter of atheromatous debris is required to cause neurologic sequelae. The occluding units, by design, limit visualization and, in the absence of enough collateral circulation, might end in extended cerebral isch emia. Retrograde embolization to the aortic arch could occur if aggressive inj ection is carried out. However, occluding units provide the theoretical benefit of defending towards a wider range of particulate sizes. The optimal protection gadget or combination of protection gadget and stent remains unclear and is a source of intense clinical investigation. However, early knowledge point out that proximal safety could have some benefit over distal embolic devices. This complication most regularly happens from distal embolization prior to placement of the embolic safety gadgets or potential overload of the filters. Manipulation of the catheters and wires to place the sheath within the common carotid artery should be accomplished in deliberate however delicate method. Proper selection of patient and gear is critical to prevent such issues. One reason for this is cerebral hyperperfusion, which may be prevented by careful blood strain monitoring in most cases fifty eight Wire-related hemor rhage should be preventable by correct strategies. Aside from entry web site associated complications, the commonest carotid stenting problems are bradycardia and hypotension 59 the primary operator must be extremely careful during the process as cerebral hypoperfusion due to bradycardia and hypo rigidity might lead to seizure activity and sudden motion by the affected person. Intervention should be reserved for people with indisputable symptoms of vertebral basilar insufficiency (Table 34. Occasionally, patients with occluded carotid arteries are depending on vertebral blood move. While any sort of stroke could be devastating, posterior circulation or brain stem infarcts are extremely dangerous and will end in immediate death. The basilar artery alone is liable for perfusion to a selection of critical areas within the brainstem. Accordingly, bas ilar artery angioplasty is reserved for these uncommon instances with acute occlusion or important stenosis and signs related to posterior circulation. Intervention to this vessel could result in occlusion of pontine branches or embolization to posterior circulation. Given the excessive danger concerned in vertebral-basilar instrumentation, a multidisciplinary strategy that includes a neurologist and a neuroradiologist is important. Coronary stents are enough in most situations and even drug-eluting stents can be used. A full neurologic examination must be performed and patients ought to be monitored for no less than 24 hours. The use of embolic protec tion devices is controversial and should lead to problems similar to spasm or even plaque dislodgement. Subsequently, the vertebral artery is wired and a small coronary balloon is superior to the world of curiosity. Subclavian, Common Carotid, and Innominate Arteries Atherosclerosis is usually the reason for stenosis in the subclavian and great vessels. In our clinic the first check to affirm great vessel stenosis or occlusion is a noninvasive duplex ultrasound analysis, with willpower of the direction of move in the vertebral arteries (antegrade or retrograde, the latter indicating the presence of a steal phenomenon) and documentation of asso ciated carotid disease. Once a call concerning intervention has been made, premedica tion with aspirin is normal, with elective addition of clopi dogrel. The alternative of access web site is dependent on location of the lesion, involvement of the ostium, and visualization of great vessels. This will enable exact stent placement without j ailing the vertebral or inside mammary artery. This will provide a " roadmap" prior to gaining selective entry into the sub clavian or innominate artery. For subclavian intervention, we sometimes use a telescoping method with a 5 F diag nostic catheter inside a 6F sheath.
Kamagra effervescent 100 mg trusted
We perform this catheter proce dure with the infant intubated and paralyzed and receiving a prostaglandin infusion erectile dysfunction at 55 kamagra effervescent 100 mg sale. Catheter manipulation is more difficult from the umbilical artery owing to the inferoposterior loop in its course before it enters the descending aorta impotence hypertension purchase 100 mg kamagra effervescent fast delivery, however its use avoids harm to the femoral artery in these very small infants. Sur gical cutdown on the carotid artery for catheter access has additionally been employed. This method simplifies crossing the valve48 due to the straight path to the valve from the neck. But the process is com plicated by the event of great aortic regurgitation in 1 0% to 30% either immediately or inside weeks of the procedure (inversely associated to balloon/annulus ratio); fem oral arterial problems in 30% to 40% (inversely related to the size of the patient), and restenosis. Patient selection primarily based on echo criteria and improved catheter expertise are bettering outcomes on this difficult group. High stress within the ascending aorta and its branches predisposes these patients to many of the traditional risks associated with hypertension. Intracranial aneurysms may be current in as many as 1 0% of patients with coarctation 52 As a end result, the pure history of untreated coarctation consists of dangers of creating untimely coronary artery illness and cerebral aneurysm rupture. However, unlike sufferers with essential systemic hypertension, pharmacologic normaliza tion of cerebral and coronary pressures will proportionally scale back descending aortic strain, and might produce iatrogenic claudication with train, abdominal cramping with splanch nic hypoperfusion, and vital renal dysfunction (prerenal azotemia). Intervention on the coarctation is thus required to obtain normotension on this population. In neonatal crucial coarctation of the aorta, the transverse and isthmic portions of the aortic arch could also be hypoplastic and also in need of restore. The newborn will be asymptomatic initially because the carotids and subclavia are equipped adequately by the ascending aorta, whereas right to left shunting at the duc tus arteriosus supplies circulate to the lower a part of the physique (as mentioned earlier). The pulse and blood pressure in the lower extremities may not be considerably totally different from these in the arms. With ductal closure, the crucial obstruction of the aorta precludes adequate flow to the lower portion of the body. Pulses vanish within the decrease extremities solely, and a severe metabolic acidosis ensues. As surgical aortic arch reconstructions have turn out to be routine at maj or pediatric coronary heart facilities as a part of the stage I palliation of hypoplastic left coronary heart syndrome, neonatal arch restore stays the standard of care,53 and many centers con tinue to send all pediatric coarctation patients for surgical interventions as a main remedy, reserving transcatheter intervention for older (full-grown) sufferers, or for those with recurrent postoperative obstruction. Percutaneous balloon angioplasty of coarctation was first described in 1 98254 as an various alternative to surgical procedure and has been used since in pediatric patients with each native (unoperated) coarctation in addition to with recurrent (postoperative) coarc tation. Short- and long-term issues seen in that research, includ ing perforation/rupture leading to dying, dissection, and late aneurysm formation, have all been described in sufferers. Stent angioplasty for coarctation has turn out to be the process of selection in adolescents and adults in whom the stent may be expanded to a full, or practically full grownup aortic diameter, in order to keep away from the necessity for later redilation of the stent. The balloon dilation catheter is centered throughout the coarctation, inflated until the waist disappears, and deflated. The balloon catheter is exchanged for a smaller pigtail catheter to allow simultane ous measurement of the ascending aortic pressure with the pigtail as compared with the distal stress from the facet arm of the present sheath. A repeat aor togram should be performed following dilation to decide the angiographic impact of the inflation and to detect tears, ruptures, or dissections. If vital obstruction stays despite disappearance of the balloon waist throughout inflation, a larger balloon can be used. Although chest discomfort could additionally be quite vital during balloon inflation, persistent ache after balloon deflation suggests aortic rupture or dissection. In that sequence, procedures were thought of successful if the gradient was decreased by > 50% and the diameter was increased by > three zero %. Balloons considerably larger than the native aorta are necessary in this group, risking inj ury to the conventional aorta. Transverse aortic arch hypoplasia is another consistent predictor of suboptimal end result. Iliac artery rupture and a retroperitoneal hemorrhage outcome ing in demise have been reported in infants. The incidence of femoral artery inj ury has decreased with the availability of lower-profile balloons. During follow-up in the Boston collection, three sufferers have been discovered to have small asymptomatic aneu rysms on the angioplasty site (two recurrent and one native coarctation). Aneurysm formation following dilation of both native and recurrent coarctation has been reported by several teams. There seems to be little difference in the incidence of aortic inj ury between the 2 teams in printed data68 with an incidence of < 10% in both group. Pediatric Balloon Angioplasty Technique Under routine sedation, femoral venous and arterial access is obtained percutaneously. Coarctation is kind of all the time finest approached from a retrograde femo ral arterial approach, although transvenous, transseptal, and antegrade approaches have been reported (when residual aortic arch obstruction should be addressed following stage I surgical palliation of single ventricles, a venous strategy is usually used). Mul tiple levels of obstruction are possible-a bicuspid aortic valve is related to coarctation of the aorta in > 70% of sufferers. The diameters of the narrowest area of coarctation and of the normal proxi mal and distal aorta are measured. For native obstructions, the balloon is usually chosen to be Coarctation of the Aorta within the Adult the technique as outlined above can additionally be applicable to grownup sufferers, and several other collection have reported glorious outcomes in grownup sufferers with < 10% rupture, dissection, aneurysm formation, or restenosis fee. However, the implan tation of a stent, at the coarctation website has turn out to be first-line remedy for adults with coarctation. Stent implantation has decided advantages over balloon angioplasty in phrases of decrease resid ual gradients and decreased rates of restenosis, and is markedly simpler than balloon angioplasty alone in the affected person with gentle coarctation. Implantation of a stent eliminates the elastic recoil of the aortic tissue and allows the use of substan tially smaller balloons. This might lead to a smaller variety of aortic inj uries, although acute dissections and aortic rupture have additionally been reported with stenting. Where unavailable, coated stents have been manufactured within the cath lab by some physicians/8 for use as a main implant or for emergency use. The selection of stent, when all are available, ultimately shall be tailor-made to the wants of the affected person. For stenting within the extra proximal aortic arch, for example, naked steel stents will remain the treatment of option to reduce the chance of occluding carotid or subclavian arteries. In con trast, for patients with known aneurysm formation at the website of a local or previously repaired coarctation with residual obstruction, a lined stent is the clear selection over a bare metal stent. This reduces the bleeding threat, and the necessity for extended groin pres sure and bedrest, especially in heavier patients. Once the long sheath is handed through the coarctation, the stent is crimped onto the balloon (unless preloaded), and passed by way of the sheath to the delivery site. Rapid right ventric ular pacing is employed to decrease the forward pressure on the ballo on.