
Innopran XL dosages: 80 mg, 40 mg
Innopran XL packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

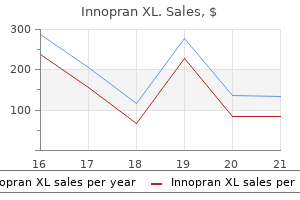
Innopran xl 80 mg effective
Deltoid tubercle: Anterior border of the lateral one-third might show a small tubercle called as deltoid tubercle pulse pressure 22 purchase innopran xl 80 mg mastercard. Attachment Anterior border: Origin of deltoid muscle from the anterior (including deltoid tubercle) border and the adjoining superior surface blood pressure medication to treat acne discount innopran xl 40 mg with visa. Posterior border: Insertion of trapezius in the posterior border and adjoining superior surface. Ends Sternal or medial finish: this finish is enlarged and presents a convex rough articular floor to articulate the clavicular notch to manubrium from the sternoclavicular joint. Costoclavicular ligament on the tough area on the inferior aspect of the sternal end. Coracoclavicular ligament-this ligament connects the clavicle and coracoid means of scapula. Clavicle incessantly fractured because of indirect violence as a end result of fall on the outstretched hand or on the shoulder. Fracture usually takes place at the junction of medial two-thirds with the lateral onethird where two curvature meet which is the weakest a part of the bone. Lateral fragment is displaced downwards by the load of the upper limb consequently drooping of the shoulder. Clavicle could additionally be congenitally absent or not properly developed in a disease situation known as cleidocranial dysostosis. Two major facilities of ossification between the fifth and sixth weeks within the shaft of intrauterine life. One secondary heart seem within the sternal end in cartilage about 18 years, which fused with the shaft begins about twenty years and accomplished the fusion about thirty-one years. Occasionally, a secondary center might appear on the acromial finish between eighteenth and twentieth years. In male, the lateral end is both on the same level or barely larger than the medial end. Infraglenoid tubercle It additionally has head, which characterize glenoid cavity and remainder of the bone varieties the physique. Arises from most of the costal floor together with the rounded ridge except the area of the neck. First and second digitations from the superior angle to the point opposite the spinous strategy of scapula. Third and fourth digitations from the alternative the apex of the spinous of the scapula to the superior a part of the inferior angle of the scapula. The dorsal surface presents a triangular self like projection known as spinous course of. By the spinous course of the dorsal surface is split in to upper smaller space called supraspinous fossa and bigger area known as infraspinous fossa. S lateral border of the spinous strategy of and the dorsal aspect of the neck, transmits the suprascapular vessels and nerves to the infraspinous fossa. Side Determination the glenoid cavity will decide the aspect to which the bone belongs. Teres minor-from the upper two-thirds of the rough strip on the dorsal surface near the lateral border. Teres major-from the lower one-third of the tough strip alongside the lateral border of the dorsal floor. Attachments Muscle: Others: the suprascapular notch is converted in to suprascapular foramen by the suprascapular ligament, which transmits the suprascapular nerve, however supras-capular vessels pass above the foramen. Superior Angle Characters: Formed by the junction of the superior and medial borders. Having the supraglenoid tubercle lies above the glenoid cavity and root of the coracoid process. Surgical neck is represented by a line passing from the anterior margin of the suprascapular notch to the infraglenoid tubercle, and posteriorly line passes via the spinoglenoid notch. Glenoid cavity is a pear-shaped articular floor (provides shallow and limited socket for the head of the humerus) and varieties the shoulder joint. The glenoid cavity made deep by the glenoidal labrum attached to the margins of the glenoid cavity. Capsular ligament of the shoulder joint hooked up to the peripheral margins of the glenoid cavity beyond the glenoidal labrum superiorly extends to the root of the coracoid course of to enclose the original lengthy head of biceps brachii. It helps to type the spinoglenoid notch transmits suprascapular vessels and nerve (spinoglenoid notch is fashioned by the lateral border of the spinous process of scapula and dorsal facet of the neck of the scapula). Spine consists of base, apex, anterior, posterior and upper borders, and upper and decrease surfaces. Anterior border: Fused with the dorsal surface of the scapula obliquely upwards and laterally. The upper lip laterally continuous with the medial border of the acromion course of. The lower lip continuous with the lateral border of acromion course of on the lateral angle. Lateral border: It is thick, rounded and free and varieties the medial boundary of the spinoglenoidal notch. Upper surface: It is gently concave and is steady with the supraspinous fossa. Lower floor: It is barely convex and is steady with the infraspinous fossa. Its medially having a small articular aspect for articulation with the clavicle to form the acromioclavicular joint. Capsular ligament of the acromioclavicular joint-at the margins of the articular facet on the medial border. Horizontal part directed forwards and twisted, having lateral and medial borders and upper (it is rough) and lower surfaces (it is smooth) and a tip. Attachments Muscles Origin: brachii-from the tip of the coracoid means of which coracobrachialis is medially and biceps laterally. Insertion: Pectoralis minor-from the medial border of the horizontal part and adjoining upper surface. Conoid a part of the coracoclavicular ligament to the tough impression on the junction of ascending and horizontal parts. Trapezoid a half of the coracoclavicular ligament attached to the ridge on the higher surface of the horizontal part. Supraclavicular ligament to the ascending part, which forms the upper margin of the suprascapular notch. Coracoacromial ligament to the lateral border of the horizontal part each in front and behind.
Innopran xl 80 mg buy generic line
Attachments Its apex is attached to the pit on the head of the femur heart attack toni braxton babyface 40 mg innopran xl discount with mastercard, however its base is connected to the margins of the acetabular notch and likewise blends with the transverse acetabular ligament arrhythmia high blood pressure 80 mg innopran xl purchase with amex. Attachments Apex Blends with the capsular ligament and with the deep side of the medial band of the iliofemoral ligament. Base Attached to the iliopubic eminence, superior ramus of the pubis and to the obturator crest. Posteriorly Below upwards � Tendon of the obturator externus covered by the quadriceps femoris � Obturator internus and gemelli � Piriformis � Sciatic nerve � the gluteus maximus. Superiorly � Reflected head of the rectus femoris which is roofed by the gluteus minimus (in the medial side) 322 Human Anatomy for Students. Inferiorly � Piriformis � Obturator externus � Lateral fibers of the pectineus � Gracilis � Adductor longus � Adductor brevis � Adductor magnus � Hamstring muscle tissue. Human Anatomy for Students Nerve Supply � � � � � � Femoral nerve by way of the nerve to rectus femoris Superior gluteal nerve Obturator nerve through its anterior division Accessory obturator nerve From the nerve to the quadratus femoris Sometimes by the sciatic nerve via the posterior capsule, generally these branches directly come up from the sacral plexus. Medial Rotation Muscles involved � Tensor fascia lata � Gluteus medius and minimus. Lateral Rotation Muscles involved � Obturator muscular tissues (Externus and internus) � Gemelli (Superior and Inferior) � Quadratus femoris. Injuries to the hip joint: At young age: Green stick fracture of neck of femur and displacement of the head of femur. Sciatic nerve harm: Sciatic nerve could additionally be injured in case of posterior dislocation of hip joint as a end result of hip joint posteriorly related to the sciatic nerve. Disease of the hip could trigger referred pain on the knee due to widespread (femoral, sciatic and obturator) nerves supplying both the joints. It is caused by the beneath improvement of the acetabulum and head of the femur iii. Although dislocation happens after birth, but the abnormality of the bones develops throughout intrauterine life iv. Positionoftheheadofthefemur: � Child is born with head of the femur outside the acetabulum � the head of the femur ascends on to the gluteal floor of the ilium above and behind the acetabulum vii. Limb actions: � Inabilitytoabductthethigh � Affected limb turn into shorter because of head of the femur of the dislocated facet displaced extra higher than the traditional facet. Examination of the limbs by Ortolani take a look at: � Patient lies on the back with hips and knees are flexed ix. Correction: this condition must be recognized at start with early remedy by splinting the joint in abduction, get hold of glorious end result. Effects: About 25 p.c of the arthritis of the hip joint in adults is the direct result of residual defects from congenital dislocation of the hip joint. This injury is frequent among the childrens between the three to nine years of age ii. Fractures of the neck of the femur: It is probably the most troublesome of all of the fractures. Intracapsular fracture: � Itmaybesubcapital,transcervicalandbasal � In intracapsular neck femur fracture usually blood supply of the pinnacle of the femur disrupt, resulting in delay in healing or nonunion of the fracture or total loss of blood provide results in aseptic avascular necrosis. Radical hip alternative: It is indicated in severe traumatic damage and degenerative illness of the hip joint. Articular Surfaces � Lateral and medial condyles of femur with articular cartilages. Modification of the capsular ligament Coronary ligament: the part of the capsular ligament between the menisci and the tibia typically called as coronary ligament. Short lateral ligament: � It is a cord-like thickening of the capsule lies deep to the fibular collateral ligament � It extends from the lateral femoral condyle to the medial border of the apex of the fibula. Other constructions strengthened the capsular ligament Anteriorly: By the medial and lateral patellar retinacula. Openings of the capsule � One in to the suprapatellar bursa � Another in the exit level of the tendon of the popliteus muscle � Sometimes different gaps that are talk with the bursae deep to medial head of gastrocnemius and deep to the semimembranosus. Synovial membrane � It is probably the most complicated synovial membrane within the physique � It is anteriorly connected to the margins of the articular surface of the patella � It lines the capsular. Ligamentum Patellae � It is the central portion of the quadriceps femoris tendon � Its size is about 7. Attachments Above: To the adjoining margin and rough area on the decrease a part of the posterior floor of the patella. Oblique Popliteal Ligament It is present in the floor of the popliteal fossa in touch with the popliteal artery. Attachments Above: Lateral part of the inter-condylar line and lateral condyle of the femur. Anterior limb: Lateral condyle of femur and connected with the lateral head of gastrocnemius. Tibial Collateral Ligament Attachments Above: Whole of the medial epicondyle of the femur, just under the adductor tubercle. Below: Medial condyle of the tibia and higher posterior part of the medial surface with medial border of the shaft of the tibia. Fibular Collateral Ligament Attachments Above: Lateral epicondyle of the femur just above the groove for the tendon of the popliteus. Below: To the intermediate space on the proximal floor of the tibia, instantly anterior to the anterior attachment of the lateral meniscus. Below: Posterior part of the posterior intercondylar area of the tibia, simply posterior to the posterior end of the medial meniscus. Transverse Ligament Attachments It connects the anterior ends of the medial and lateral menisci. Medial meniscus Attachments Anterior horn: Anterior to the tibial intercondylar space in entrance of anterior cruciate ligament. In between the attachments of posterior horn of the lateral meniscus and posterior cruciate ligament. Peripheralborder: To the fibrous capsule and the deeper side of the tibial collateral ligament of knee joint. Lateral meniscus Attachments Anterior horn: In entrance of the intercondylar eminence, behind and lateral to the anterior cruciate ligament. Posterior horn: Behind the intercondylar space of the tibia in entrance of the posterior end of the medial meniscus. Subcutaneous prepatellar bursa: It lies between the pores and skin and the anterior floor of the patella. Subcutaneous infrapatellar bursa: It lies between the pores and skin and the tubercle of the tibia the place ligamentum patellae is connected. Deep infrapatellar bursa: It lies behind the patellar ligament in the interval between the previous and the anterior surface of the upper end of tibia. Suprapatellar bursa: It lies between the quadriceps femoris and the decrease end of femur and also communicates with the knee joint.
Diseases
- Achondrogenesis
- Usher syndrome, type 3
- Vitiligo psychomotor retardation cleft palate facial dysmorphism
- Paroxysmal cold hemoglobinuria
- Robinson Miller Bensimon syndrome
- Atrial septal defect
- Acute myeloid leukemia
Innopran xl 40 mg buy with visa
It is characterised by involuntary pulse pressure over 80 80 mg innopran xl buy with mastercard, rhythmical oscillatory movements of the eyes ii hypertension research generic innopran xl 80 mg with amex. It extends from the fascial sheath of the inferior rectus and inferior indirect to the decrease margin of the inferior tarsus ii. Lower head: From the lateral floor of the lateral pterygoid plate of sphenoid bone. Insertion Posteroinferior part of the medial surface of the ramus and angle of the mandible. Moves the mandible from side-to-side (by alternating exercise of the left and right sides) iii. Superficial layer: Angle and lower posterior half of the lateral floor of the mandibular ramus ii. Nerve Supply Deep temporal branches of the anterior trunk of the mandibular nerve. Elevates the mandible which helps to close the mouth and approximates the teeth ii. Retracts the mandible after protrusion of the mandible by the posterior fibers iii. Outer surfaces of the alveolar processes of the maxilla and the mandible reverse the three molar teeth ii. Insertion All fibers converge on the angle of mouth and arranged in to higher, middle (central) and lower units of fibers i. During mastication they assist the tongue in course of meals between molar enamel. In second stage of deglutition, blowing and suckling In each case closure of pharyngeal isthmus is important c. During sneezing, partial closure of isthmus happens so that air may also pass through oral cavity. During coughing, sputum may move by way of mouth as a substitute of narrow nasal passage which can be damaged. Number of mucous glands on this floor Short Notes on Head, Neck and Face 471 (These glands form the main mass of the palate). Lined by ciliated columnar epithelium except posterior part which is lined by stratified squamous epithelium. Tensor veli palatini ending in palatine aponeurosis which splits to enclose musculus uvulae 7. It forms the fibrous framework of the soft palate where all of the muscular tissues of palate are hooked up. Presence of a conical projection within the center, projects downwards generally identified as uvula c. They are folds of mucous membrane containing palatoglossus and palatopharyngeus muscle tissue respectively. Attachments In Front To the posterior border and under surface of onerous palate as a lot as palatine crest. Structures of Soft Palate Structurally it consists of a bilaminar fold of mucous membrane which accommodates following constructions (including nerves and vessels). Nasal mucous membrane (lined by mainly ciliated columnar besides posterior part which is lined by stratified squamous epithelium) 2. Posterior fasciculus of palatopharyngeus Lymphatic Drainage Drains in to deep cervical lymph nodes. Parasympathetic postganglionic secretomotor fibers arising from the facial nerve through the pterygopalatine ganglion vi. Musculus Uvulae A paired small muscles (enclosed by splitted palatine aponeurosis). Insertion Ends in palatine aponeurosis and behind the palatine crest on the horizontal plate of the palatine bone. Nerve Supply Nerve to medial pterygoid branch of mandibular nerve before its division. Anterior part of soft palate is stretched and depressed for palatoglossal closure ii. Origin Anterior fasciculus from posterior border of the exhausting palate and both from the upper floor of the palatine aponeurosis. It helps in closure of pharyngeal isthmus by approximating the palatopharyngeal arches. Insertion In to side of tongue on the junction of its anterior two-thirds and posterior one-third. Short Notes on Head, Neck and Face 473 Nerve Supply of Muscles All the muscular tissues of soppy palate besides tensor veli palatini are provided by cranial a part of the accent nerve by way of pharyngeal. Cleft palate: Congenital defect because of failure of fusion between the elements forming the hard palate (primitive palate and two horizontal palatine course of from maxillary process-fusion is Y-shaped). So, cleft palate could also be incomplete or full or may be associated with hair lip. Due to paralysis of the palatal muscles causes nasal voice and regurgitation of food via the nose when particular person tried to swallow of meals. In case of diphtheria, soft palate might typically be paralyzed resulting in nasal regurgitation of food and nasal tonation of voice. Persistent a part of bucconasal, membrane which is a fold of ectoderm with a core of mesoderm inside it b. It arises from inner facet of frontonasal process inside stomodeum towards buccopharyngeal membrane. It extends from the incisive fossa to the higher jaw lateral to the incisor tooth ii. Complete cleft palate (anterior and posterior): In this anomaly the cleft appears Y-shaped. Perpendicular plate of palatine bone, together with its orbital and sphenoidal processes vii. It is roofed by skin with coarse curved hairs called vibrissae, sebaceous and sweat glands. They are curved shelf like bony projections directed downwards and medially within the posterior a half of lateral wall of nostril ii. The conchae improve the surface area of the nose for air-conditioning of the impressed air. Sometimes fourth concha is present on the lateral wall at the spheno-ethmoidal recess known as highest nasal concha. Situated above the superior meatus and above the posterior half of the middle concha c. They are the passages in the lateral wall inferolateral to the overhanging conchae b. Limen nasi: A curved muco-cutaneous ridge on the junction between atrium and vestibule. Ethmoidal infundibulum: It is a curved channel extends upward from the anterior a half of the hiatus semilunaris its wall receives anterior ethmoidal sinuses.
Innopran xl 40 mg proven
Anterior filaments of the meningeal rami of the maxillary nerve (nervus meningeus medius) and mandibular nerve (nervus spinosus) hypertension lisinopril buy innopran xl 80 mg on line. Via the nervi meningeus medius and spinosus and also fibers from the trigeminal ganglion ii blood pressure chart monitor 80 mg innopran xl generic with visa. A recurrent tentorial nerve branch of ophthalmic division, supplies the tentorium cerebelli. In the posterior cranial fossa: Ascending meningeal branches of the first, second and third cervical nerves. It extends from the foramen magnum to the decrease border of the second sacral vertebra iii. Caudally from the lower border of second sacral vertebra the dura mater covers the filum Brain and Spinal Cord 565 the prostatic veins drain in to the venous plexus within the epidural area which may outcomes metastasis affecting the vertebral our bodies in carcinoma of prostate. The spinal dura mater has tubular prolongations across the roots and nerves as they move out of the intervertebral foramina vi. The spinal dura mater is separated from the periosteum of the vertebral canal by an epidural or extradural area (Table eleven. Epidural or extradural space: It is current between the spinal dura mater and the periosteum of the vertebral canal and ligaments within the vertebral canal. Extent: It extends from the foramen magnum to the hiatus sacralis, and projects bilaterally up to the intervetebral foramina. Contents: It incorporates loose connective tissue, fats and inside vertebral venous plexus. This is so named as a outcome of numerous spider like trabeculae prolong between the arachnoid mater and pia mater within the subarachnoid house iii. This presents two special features- subarachnoid cisternae and arachnoid granulations. Cerebellomedullary cistern or cisterna magna Situation: It is located between the inferior surface of the cerebellum and the dorsal surface of the decrease part of the medulla oblongata. As epidural area is traversed by the roots of spinal nerves that are enveloped by the sheaths of the spinal meninges, sometimes anesthetic fluid is injected in the epidural house to produce segmental and regional anesthesia significantly applied for the painless child delivery. The venous plexus within the epidural space are communicates with the vertebral canal and azygos venous system, and receives immediately few venous tributaries from the prostate, thyroid and mammary glands ii. Consists of single layer There is a few hole between the periosteal layer and dura mater and comprise some loose areolar tissue, fatty tissue and venous plexus It has no process It is thinner 1. It has 4 processes (falx cerebri, falx cerebelli, and tentorium cerebelli and diaphragma sellae) It is thick and tough 566 Human Anatomy for Students. Continuation: With the supracallosal cistern over the superior floor of corpus callosum. Cistern of the lateral fossa Situation: It is formed by the bridging of the arachnoid mater over the stem and posterior ramus of the lateral sulcus. Cisterna ambiens or superior cistern Situation: Between the splenium of the corpus callosum and superior surface of the cerebellum. All the three meningeal layers with subdural and subarachnoid areas surround the optic nerves up to the posterior part of the eyeballs, therefore papilledema is an early indication of increased cerebrospinal fluid strain. The lymphatics from the roof of the nasal cavity run with the olfactory nerves which could be the possible route of spread of an infection (microbial or viral) to produce meningitis or encephalitis. These are elevations, tasks primarily in to the superior sagittal sinus and its venous lacunae ii. These are extra distinguished alongside the margins of the median, longitudinal fissure, from which they project in to the superior sagittal sinus v. With the advance aged particular person these granulations are enlarged and erode the skull bones producing granular pits along the perimeters of the superior sagittal sinus. This invests the spinal twine loosely ii this extends up to decrease border of second sacral vertebra iii. The spinal cistern: It is a wide subarachnoid house, lies distal to caudal finish of the spinal wire and lies intervenes between the decrease borders of L1 and S2 vertebrae. It is a fragile membrane which intimately invests the surfaces of the mind and spinal cord ii. It varieties the tela choroidea as a bilaminar fold of pia mater containing the choroid plexuses, which is invaginated in to the adjacent ventricles. In the fourth ventricle: It is located between the inferior vermis of cerebellum dorsally and the ependymal roof of the caudal a half of the fourth ventricle ventrally. In the third ventricle: It lies between the corpus callosum and the fornix above and the ependymal roof of the third ventricle and the thalamus beneath. In the lateral ventricle: On the floors of the our bodies and inferior horns of the lateral ventricles. These are continuation of pia mater which are flat, fibrous sheets located on all sides of the spinal cord between the ventral and dorsal spinal nerve roots b. The last pair exits between the twelfth thoracic and first lumbar spinal nerves 568 Human Anatomy for Students vii. Below the conus medullaris the pia mater continues as a coating of the filum terminale with none ligamentum denticulatum. Forcible detachment of the endosteal layer in case of head accidents with or with out fracture of the cranium produces extradural meningeal hemorrhage. The blood in case of meningeal hemorrhage generally outcomes compression over the totally different functional areas of the surface of the brain which is manifested by the symptoms. The most typical artery to be broken is the anterior division of the center meningeal artery c. The arterial or venous injury is particularly liable to occur if the artery and vein enter a bony canal on this area d. Bleeding happens and strips of the meningeal layer of dura mater from the inner floor of the cranium thereby intracranial stress raises and enlarging the blood clot. Bleeding could happen through the fracture line to form a delicate swelling beneath the temporalis muscle. It results from tearing of the superior cerebral veins on the point of entrance in to the superior sagittal sinus b. The trigger is usually a blow on the front or the again of the head, causing extreme antero-posterior displacement of the mind inside the cranium c. This condition is much more common than the center meningeal hemorrhage, which might produce by a sudden minor blow d. Acute and chronic types of the clinical condition happen depending on the speed of accumulation of fluid within the subdural area. Results from leakage or rupture of a congenital aneurysm on the circle of Willis or less generally from an angioma b. The symptoms are sudden in onset embrace severe headache, stiffness of the neck and the loss of consciousness. It is generally attributable to rupture of the skinny walled lenticulostriate artery, branch of middle cerebral artery b. The hemorrhage involves the corticobulbar and corticospinal fibers in the internal capsule and produces hemiplegia on the other aspect of the body.

Innopran xl 40 mg buy with amex
The inferior and posterior articular surfaces of every condyle kind the tibial articular surface blood pressure control 80 mg innopran xl generic overnight delivery, which articulates with the corresponding condyles of the tibia arrhythmia triggers innopran xl 80 mg order without prescription. The tibial articular surfaces are separated from one another by intercondylar notch. Posterior a part of the articular floor project backwards beyond the extent of the popliteal floor. In this fracture the retinacular arteries are injured main delay in healing or nonunion or could results in avascular necrosis of head of the femur ii. In children and adolescents the epiphysis of the top of the femur may slip away the neck as a end result of weakness of the epiphyseal plate. The angle of inclination (neck-shaft angle) usually in grownup 125 degree and kids 160 diploma, its abnormality produces two circumstances: i. When angle is elevated the condition is called coxa valga present in congenital dislocation of hip, which results the adduction of the hip joint is limited ii. Fracture between the larger and lesser trochanters called intertrochanteric fracture or via the trochanters called pertrochanteric fracture, these fracture also generally seen in above 60 years. Medicolegally secondary middle of ossification for decrease end is essential when the query arises for infanticide as the secondary heart for the lower end appears just earlier than start (nine months of intrauterine life). Anterior cruciate ligament (upper end)- to the medial floor of the lateral condyle from a impression. Posterior cruciate ligament (upper end)- to the lateral surface of the medial condyle (cruciate ligaments are intracapsular however extrasynovial). Origin of lateral head of gastrocnemius-from a groove on the posterosuperior a part of the lateral epicondyle. Primary middle: One primary heart seems in center of the shaft about seventh week of embryonic life. Fracture of neck of the femur is fairly common in older persons above 60 years extra in females because of osteoporosis outcomes 780 Anatomical Position Human Anatomy for Students 1. Side Determination the larger a part of the articular surface on which side belongs will determine the side of the bone. Anterior floor is subcutaneous, rough and nonarticular with presence of quite a few vascular foramina and marked by numbers of longitudinal ridges viii. The articular part divided by a vertical ridge in to large and deeper lateral and small and medial elements Attachments 1. Ligamentum patellae- to the apex and decrease a half of the nonarticular area on the posterior surface 2. Vastus medialis on the medial one-third and vastus lateralis on the lateral twothirds in a similar aircraft iii. The larger lateral articular a half of the posterior surface articulates with the lateral condyle of the femur Osteology 781 ii. The smaller medial articular part of the posterior floor articulates with the medial condyle of the femur iii. The vertical ridge on the articular a half of the posterior surface suits in to the groove on the patellar floor of the femur iv. The nonarticular part of the posterior surface subdivided in to upper and decrease elements: a. It ossifies from the a quantity of facilities, they seem during the third to sixth years, and unite shortly ii. A fracture patella could additionally be difficult to heal due to the robust pull of the quadriceps muscle. Patella fractured as a end result of direct violence generally in an automobile accident the place patella is broken in to many small items. Patella might fractured on account of indirect violence brought on by the sudden highly effective contraction of the quadriceps femoris in semiflexed or flexed knee where snapping the patella throughout the front of the condyles of the femur. Traumatic dislocation of patella (with or with out fracture) outcomes from direct trauma to the quadriceps attachments of the patella especially vastus medialis. Congenital recurrent dislocation of patella happens because of underdevelopment of the lateral condyle of the femur. Patella commonly dislocated laterally because of the lateral angulations between long axis of the thigh and leg. Insertion of vastus medialis on the medial border of the patella extends decrease level than the vastus lateralis on the lateral border. Side Determination the medial malleolus will decide the opposite aspect of the bone. Lateral meniscus-it is in contact with the anterior, posterior and lateral margins of the superior articular floor. Capsular ligament of the superior tibiofibular joint-margins of the fibular facet. Origin (sometimes) of few fibers of extensor digitorum longus and peroneus longus- to the lateral surface simply in front of the fibular side. Deep infrapatellar bursa-presents on anterior convex surface of both the condyles. Iliotibial tract and deep fascia of leg- to the sharp margin separating it from the lateral surface of the shaft. Lateral a part of the superior articular surface extends over the medial facet of the medial intercondylar tubercle. Medial meniscus-it is in contact with the anterior, posterior and medial margins of the superior articular floor. Insertion of semimembranosus- to the groove, its lower lip and on the lateral part of the groove having a rough tubercle. Capsular ligament of the knee joint and brief posterior fibers of the tibial (medial) collateral ligament of the knee joint-at the higher margin of the groove. Medial patellar retinaculum-on the anterior and medial surfaces of the medial condyle. Tuberosity of the Tibia Characters: It is a distinguished bony eminence on the higher finish of the anterior border. It is tough space between the articular surfaces of the medial and lateral condyles. In the center the realm is slim, irregular and elevated known as intercondylar eminence. The intercondylar eminence is formed by the lateral and medial intercondylar tubercles. Begins from the decrease a half of the tuberosity of the tibia to finish beneath on the anterior margin of the medial malleolus. Relations-just above the medial malleolus the anterior border is crossed by the: i. Saphenous nerve Lateral or Interosseous Border Characters Begins from the anteroinferior a half of the fibular side, and ends beneath by dividing to enclose a triangular tough notch at the lateral aspect of the lower finish.
Order 80 mg innopran xl fast delivery
The research concerned 625 patients and showed no significant variations when it comes to mortality: nevertheless arrhythmia associates of south texas discount 40 mg innopran xl fast delivery, at 3-month follow-up there was an 11% absolute increase in the variety of sufferers who had completely recovered or with minimal consequences arterial nephrosclerosis 80 mg innopran xl buy with mastercard. In brief, the shorter the time interval between the onset of stroke and thrombolysis, the higher likelihood of better outcomes, strengthening the concept of "Time misplaced, mind misplaced. The symptomatic hemorrhage price varied according to the definition used, but was in preserving with previous trials, being larger in the group treated with fibrinolytics. Intra-arterial thrombolysis is a promising choice, as evidenced by a series of instances which should be validated in the future. In theory, this technique would offer some advantages compared to intravenous remedy, together with simpler recanalization rates, widening of the therapeutic window (all by direct infusion in to the thrombus), in addition to the potential for lowering the opposed effects of the drug, and so forth. Disadvantages embrace the necessity for a specialised neuroradiologist and group available 24 hours 7 days a week. However, there are situations where it may be beneficial: � Presence of cardioembolic stroke at excessive danger of recurrence; for example: atrial fibrillation, artificial heart valves, acute myocardial infarction with mural or intracavitary thrombi, left atrial thrombosis. Moreover, hypocholesterolemia is taken into account a predisposing issue for the development of spontaneous intracerebral hemorrhage, and never ischemic stroke. Statins have potential benefits, together with: � Protection of the vascular endothelium. From a medical point of view, statins: � Decrease the incidence of mind and cardiovascular events. It is our present follow to use of simvastatin or atorvastatin forty mg every day for 1 week after which continue with 20 mg/day for the first 3 months after an ischemic cerebrovascular event. Brain oxygenation and power metabolism: part I-Biological perform and pathophysiology. Supplement to the guidelines for the management of transient ischemic assaults: A assertion from the 771 Intensive Care in Neurology and Neurosurgery � � � � � � � � � � � � � � � Ad Hoc Committee on Guidelines for the Management of Transient Ischemic Attacks, Stroke Council, American Heart Association. Clinical follow pointers: diagnosis and immediate management of transient ischemic assaults in adults. Report of the joint stroke tips development committee of the American Academy of Neurology and the American Stroke Association. The American Academy of Neurology affirms the value of this assertion as an educational device for neurologists. Primary prevention of ischemic stroke: a statement for healthcare professionals from de Stroke Council of the American Heart Association. Validation and refinement of scores to predict very early stroke threat after transient ischemic attack. Circulation 2006; 113: e409-49 Carotid Disease � Brott T, Brown R, Meyer F, et al. Carotid revascularization for prevention of stroke: carotid endarterectomy and carotid artery stenting. Safety and efficacy of endovascular therapy of carotid artery stenosis compared with carotid endarterectomy: a Cochrane systematic review of the randomized proof. Beneficial results of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. Stroke 1985; 16: 885-90 � Treatment of Ischemic Stroke � 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: Part 9: Adult stroke. Stroke Council of the American Stroke Association: Guidelines for the early administration of sufferers with ischemic stroke: A scientific statement from the Stroke Council of the American Stroke Association. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset. Expansion of the time window for treatment of acute ischemic stroke with intrave- � � � � � � � � � � 774 Acute Ischemic Stroke: General Approach � � � � � � � � � � � � � � � � � � � nous tissue plasminogen activator: a science advisory from the American Heart Association/American Stroke Association. Serum glucose degree and diabetes predict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic stroke. Body temperature in acute stroke: relation to stroke severity, infarct measurement, mortality and consequence. Disturbances of sodium in critically grownup neurologic sufferers: A clinical evaluation. Acute hyperglycemia and the innate immune system: scientific, cellular and molecular features. Neurology 2002; 59: 67-71 776 forty three Ischemic Penumbra: Role of Neuroimaging in Treatment Decision Alvaro Cervera 1, Geoffrey A. However, because of the slender time window, lower than 5% of patients with this condition obtain this drug. To be able to deal with a higher number of patients it would be essential to extend this time window. There are different approaches aimed at growing the traditional three hour time window. There are studies analyzing the efficacy of alteplase in eligible patients who present with acute ischemic stroke in either the 3-4. The second approach is to choose sufferers that are extra likely to reply to the thrombolytic remedy. This will result in ischemic damage, which magnitude and localization will depend upon the extent, severity, and length of the perfusion deficit. However, not all of the hypoperfused tissue surrounding the ischemic core can be called ischemic penumbra. This idea arose by clinical observations of fluctuating neurological deficits that suggested different perfusion thresholds for loss of neuronal perform and cell demise. Schematic representation of the of those thresholds in experimental mod- ischemic tissue after a serious vessel occlusion. The ischemic penumbra duced cerebral blood move, absent electri- is represented by the "A" space. This is the tissue cal activity, but preserved ion homeostasis that can be salvaged after using thrombolytic and transmembrane electrical potentials. Penumbral tissue is an abnormal tissue with physiological and biochemical characteristics of cellular dysfunction however not cellular dying, brought on by hypoperfusion. The main relevance of this tissue is that it may possibly either survive or progress to necrosis, and its salvage is associated with better scientific consequence. The tissue surrounding the infarct core stays viable, but severely compromised because of metabolic, hemodynamic, and neurochemical alterations attribute of the ischemic surroundings. The dissociation between metabolism and flow is pronounced in focal cerebral ischemia. Maintenance or focal will increase in glucose utilization have been noticed in brain areas adjoining to the ischemic core. Therefore, the uncoupling of metabolism and circulate is a vital pathogenetic mechanism that affects the critical energy balance within the penumbra. Lastly, the ischemic penumbra is a dynamic tissue structure of restricted viability surrounding a focus of dense cerebral ischemia. Therefore, with time will increase the viability of the penumbra will decrease and more tissue will be recruited within the core. There are many neuroimaging tools which have shown efficacy in penumbra evaluation.
Wintersweet (Oregano). Innopran XL.
- How does Oregano work?
- Parasites in the intestines.
- What is Oregano?
- Are there safety concerns?
- Dosing considerations for Oregano.
- Asthma, croup, bronchitis, cough, indigestion and bloating, painful menstrual periods, arthritis, headaches, heart conditions, and other conditions.
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96635
40 mg innopran xl mastercard
They then go on to pulse pressure product buy generic innopran xl 40 mg the portal vein and are transported to the liver and different tissues as free fatty acids or sure to albumin pulse pressure fluid responsiveness purchase 80 mg innopran xl free shipping. They have the advantage of not being stored as fat in the physique and are oxidized rapidly and utterly. Octanoic acid accumulates in these sufferers, so signs could seem much like hepatic encephalopathy. The major protein losses occur by way of the urine and feces, the latter due to intestinal secretions and cell desquamation. In this specific situation, a ratio of nonprotein calories per gram of nitrogen (100 to 150/1) have to be maintained. In septic sufferers this ratio ought to be eighty kcal of nonprotein nitrogen per gram of nitrogen. Using tables that show the day by day losses of nitrogen in several medical conditions (replacement must equal losses). Measured urea in 24-hour urine: nitrogen excretion in urine is the ultimate product of protein metabolism to acquire vitality; therefore, the protein requirements can be decided by calculating the every day losses of nitrogen from the elimination of urea in 24-hour urine. For the proper calculation of nitrogen excretion, a steady food plan should maintained for twenty-four to forty eight hours beforehand. When using amino acids as a nitrogen source, some measures must be taken in to account: 1. The nutrient answer should embrace all the important amino acids and traces of the nonessential ones. In basal circumstances the day by day quantity of water required is 25 to 35 ml/kg/day, and these needs improve in hypercatabolic states up to 50 to 70 ml/kg/day. Multiple factors modify water Recommended doses Nitrogen (g/kg/day) losses, such as high-protein diets, fever, polyuria, vomiting and kidney failure. Vitamin necessities may be affected by modifications in food plan, use of some medicines, diseases similar to malnutrition, sepsis and trauma, and artificial nutrition, primarily parenteral diet. The deficit of the water-soluble vitamins occurs more simply as a result of the fat-soluble vitamins are saved in the physique and have a slower turnover (Table 20. Vitamin B12 must be taken 2 or 3 times a week and at very extensive intervals thereafter. Fat-soluble vitamins should be administered as quickly as per week and vitamin K twice every week. These substances are concerned in multiple cellular capabilities and varied enzyme methods. Daily requirements Electrolite Sodium (Na+) Chlorus (Cl-) Kalium (K+) Calcium (Ca++) Phosphorus (P) - 1-2 mEq/kg 1-2 mEq/kg 0. A main form of remedy, artificial vitamin performs an important role within the complete care of critically sick patients since a dietary deficit can work together with the disease and prolong the therapeutic course of or have devastating penalties. The routes of administration are enteral nutrition and parenteral diet, discussed below. During the course of critical sickness, the gut virtually always stays inactive because of ileus or different frequent problems that stop feeding and require nasogastric aspiration. Besides its role in the digestion and absorption of nutrients, the gut also acts as an enteral flora barrier which prevents host invasion by microorganisms or their toxins. In sufferers who receive no meals or nutrients in to the digestive tract, the intestinal mucosa turn out to be more permeable to the passage of germs and their merchandise in to the bloodstream, resulting in continual hypermetabolism and a number of organ failure. Volumes of 200 to four hundred ml four to 6 instances a day can cause nausea, vomiting, diarrhea, cramps and bloating, with a excessive threat of aspiration. Intermittent administration is given in small amounts of 80 to one hundred sixty ml from 20 to half-hour every hour; however, tolerance is poor in some patients and the method is impractical since it occupies plenty of nursing employees time. An alternative way to be used in sufferers requiring extended enteral vitamin includes continuous administration of enteral solutions at a rate of 160 ml/hour for 12 hours. Isotonic options ought to be started at an infusion rate of fifty ml/ hour, after which gradually elevated, as tolerated, up to 80 ml/hour. If intolerance develops, the quantity or focus of the food plan should be decreased to the previous level of tolerance, and then increased after enough time for adaptation has elapsed. Wherever possible, regulators ought to be equipped with a move or infusion pump to reduce the potential for inadequate volumes, resulting in much less bloating and diarrhea, lower residual volume and less danger of aspiration. The quantity must be increased every 24 to forty eight hours till it covers the whole dietary requirement with an intermittent bolus of 300 to 400 ml each, each three to four hours. The gastric residual must be controlled before each administration and administration discontinued if it is >150 ml. The affected person ought to be rechecked after 2 hours and feeding could be restarted if the gastric residual is lower than the said value. This route of administration of nutrients will not be used in neurocritical patients due to the chance of aspiration. The tube ought to be placed distal to the Treitz ligament to decrease the danger of aspiration. The method for tube placement could additionally be blind (high failure rate) or by endoscopy, fluoroscopy or ultrasound-guided. The use of prokinetic agents facilitates, no less than in principle, the passage of the pylorus, regardless of the approach. Also, these tubes could be positioned by invasive methods similar to endoscopic percutaneous jejunostomy, radiological percutaneous jejunostomy and conventional surgical procedure or by laparoscopy. Use of enteral vitamin, primarily jejunal nutrition, is appropriate for early postoperative feeding, is protected and effective, as intestinal paralysis is predominant in the stomach and colon, and likewise it causes poor pancreatic stimulation. Bolus administration of hyperosmolar solutions within the small intestine could cause bloating, diarrhea and electrolyte disturbances. To keep away from these antagonistic effects, volumetric pumps can be utilized and options with half of the specified focus should be started at infusion fee of 50 ml/hour. The concentration of the options must be elevated till the whole osmolality of the nutritional method is obtained. The most important limiting think about intolerance to the food plan is the osmolar load (intake per unit time) acquired by the digestive tract, so a gradual enhance within the infusion fee, 410 Nutritional Support in Critically Ill Patients however not the concentration of the formulation, is recommended, while maintaining a caloric density of 1 kcal/ml. Accordingly, protocols has been devised underneath which the quantity ought to be 20 ml/hour for the primary 6 hours and then incremented by 10 ml/hour each 6 hours till the desired volume is reached, or to start with 20 ml/hour for eight hours with increments of 20 ml/ hour each 8 hours until the infusion fee matches the requirements. If the patient develops diarrhea, and antidiarrhetic may be given, but when it persists or different antagonistic results come up, feeding should be suspended for forty eight hours. The presence of abdominal distention, diarrhea or other unwanted effects have to be checked periodically. Homogenized diets are prepared with natural foods underneath technical homogenization; they differ from regular food only in consistency and methodology of administration by way of a catheter. These diets are ready from milk, yogurt and ice cream, and different vitamins are added. Milk-based diets use milk as the primary protein source and different sources of protein like eggs are added; calories are provided as lactose, dextrins, milk fat and soybean or corn oil. They are poorly tolerated in patients with disaccharidase deficiency and can cause diarrhea.
Innopran xl 40 mg buy with amex
Cardiac arrhytmias after subarachnoid hemorrage: threat elements and impact on outcome pulse pressure example 40 mg innopran xl with mastercard. J Cardiovascular Electrophysiol 2002; 13: 444-8 � Guias 2005 de la American Heart Association sobre resucitacion cardiopulmonar y atencion cardiovascular de Emergencia blood pressure medication coreg buy cheap innopran xl 40 mg on line. Sudden dying in epilepsy: a complete review of the literature and proposed mechanisms. Cardiac Conduction abnormalities in kids with progressive muscular dystrophy: Electrocardiographic features and morphologic correlates. Acetazolamide opens the muscular Kca channel: A novel mechanism of actions that may clarify the terapeutic effect of the drug in hypokalemic periodic paralysis. Muscle Nerve 1994; 171145-55 358 17 Mechanical Ventilation within the Neurologic Critically Ill Patient Guillermo Bugedo 1, Jaime Retamal 1 1 Intensive Medicine Department, Pontificia Universidad Cat�lica de Chile, Santiago, Chile 17. Respiratory depression, by itself or as a contributing factor, is among the primary causes of respiratory failure within the neurologic critically unwell patient. Respiratory melancholy induces alveolar hypoventilation, airway obstruction, gastric content aspiration and hypoxemia, amongst others. Therefore, aggressive airway management and ventilatory assist are key to managing these sufferers. In a large-scale epidemiological examine on mechanical air flow performed in 1998 and involving a cohort of 5,183 ventilated patients, "coma" was cited as the reason for ventilatory help in 17% of the examine population, and the mortality price was 36%. Similar findings had been reported by a second research published in 2004, in which 19% of the ventilated sufferers received respiratory help because of neurologic causes. The 28-day mortality fee was 48%, 35%, and 28% in sufferers with hemorrhagic stroke, ischemic stroke, and head trauma, respectively. There is powerful proof that hypoxia is likely certainly one of the main causes of secondary neuronal injury after head trauma, almost doubling mortality. This is composed of several teams of neurons situated bilaterally within the medulla oblongata and pons of the brainstem, and is chiefly liable for ventilatory exercise. Respiratory complications may produce secondary mind harm because of hypoxemia and hypoventilation, promoting vicious circles which jeopardize affected person outcome. Lung mechanoreceptors and cardiovascular baroceptors ship info on practical residual capability. The respiratory system effectors are answerable for regulating the ventilatory cycle: airway (genioglossus and cricoarytenoideus muscles), and chest wall muscle tissue (diaphragm, intercostal and equipment muscles). Respiratory depression is a scientific syndrome characterized by a dysfunction of the respiratory centre. Its analysis requires a variable but fixed altered degree of consciousness and respiratory abnormalities (Table 17. The most common medical penalties of respiratory despair are apnoea, bradypnoea or periodic breathing abnormalities, and the lack to maintain a patent airway (tongue falling backwards, retention of secretions and hypotonia of pharyngeal muscles), which can lead to alveolar hypoventilation. Therefore, airway management should be managed early in sufferers with progressive drowsiness and coma. Patients with trauma and intracranial hypertension could present delayed gastric emptying. It follows that any patient with head trauma or stroke must be treated as a affected person with a full stomach at excessive risk for aspiration. Any sign of vomiting in an unconscious patient is highly suspicious for gastric aspiration. Clinics of aspiration depend upon the standard and quantity of aspirated liquid, the aspiration of bilious contents or blood being much less poisonous than acid or meals contents. In any case, the chance of secondary an infection is excessive and will prompt antibiotic therapy. A 29-year-old patient underwent surgical procedure for elimination of a tumour of the posterior fossa (Cx1). The patient was carefully noticed, but later that day he had to be intubated because of coma. Total atelectasis of the left lung because of loss of muscular tone, decreased residual lung capacity and decreased cough, was secondary to respiratory depression. A sedation scheme for brain-injured sufferers in use on the Centro de Pacientes Cr�ticos, Universidad Cat�lica de Chile [Riker, 1999]. However, beyond the objective of facil363 Intensive Care in Neurology and Neurosurgery itating mechanical ventilation, sedation might lower oxygen metabolism and intracranial hypertension, and control seizures. The selection of medication and doses when ventilating sufferers with brain damage is extraordinarily heterogeneous. Sedation in patients with trauma or stroke ought to be based mostly on: the necessity of medical evaluation; oxygen metabolism; intracranial pressure; cerebral blood flow and perfusion stress amongst others. Goal-oriented monitoring of depth of sedation and periodic adjustment are essential to prevent over- and undersedation, which can have an effect on major outcomes and prices. Undersedation may improve metabolism, oxygen consumption and intracranial hypertension. In neurological critically unwell patients, a sedation protocol may lower infections and secondary hypoxemia and so enhance such major outcomes as long-term cognitive functions. There can be proof that hyperventilation may exacerbate ischemia in hypoperfused zones of the brain. In this setting, hyperventilation could additionally be deleterious and treatment must be oriented to improve oxygen delivery (inotropes or vasopressors), decrease oxygen consumption (sedatives) or decrease brain edema (hypertonic therapy). This last correlation is particularly essential when applying therapeutic hypothermia. At 48 hours, the affected person required orotracheal intubation and mechanical ventilation because of respiratory failure secondary to aspiration of gastric contents. Recruitability, or the potential for recruitment, refers to the capability of the lung parenchyma to incorporate previously closed alveolar items to gasoline exchange. A 53-year-old man was admitted because of a right-sided traumatic epidural hematoma. Recruitment manoeuvres involving high airway strain over quick periods of time may open in any other case collapsed alveoli and have a diagnostic position in assessing recruitability in sufferers with extreme hypoxemia. Overdistention and the repetitive opening and closing of unstable alveoli generate mechanical stress and strain on the lung cytoskeleton, which may rupture the alveolocapillary membrane, activate endothelial and epithelial cells, and amplify the inflammatory response. In an observational research involving 86 sufferers with extreme head damage, Mascia et al. The trial was stopped prematurely for safety causes as a result of the event of lung harm was higher within the Vt-10 ml/kg group (13. Finally, the protecting strategy doubled the number of patients from whom the lungs could possibly be harvested (54 vs. This research underscores the importance of protective ventilation even in brain-injured patients with a poor prognosis. This is particularly relevant in the neurologic population, since excessive tidal volumes have been incessantly beneficial in the past to induce hypocapnia. Brain injury induces systemic inflammation which might have an effect on distant organs, together with the lungs. In different words, high Vt will induce lung harm in beforehand injured or infected lungs but not in the healthy lung.
Innopran xl 80 mg trusted
Situation: Groove on the superior border of the petrous a half of the temporal bone arrhythmia questions and answers 80 mg innopran xl discount. Thrombosis of the superior sagittal sinus: the superior sagittal sinus may be thrombosed attributable to unfold of infection from the nostril pulse pressure in athletes purchase innopran xl 40 mg visa, scalp and diploe resulting following: i. Delirium and typically convulsions as a end result of congestion of superior cerebral veins iii. Paraplegia of higher motor neuron sort because of bilateral involvement of the paracentral lobules of the cerebrum. Thrombosis of the sigmoid sinus: the sigmoid sinus may be thrombosed attributable to secondary to an infection within the tympanic cavity or within the mastoid course of (mastoiditis). Occlusion of cerebral veins and dural venous sinuses this will likely end result from a thrombus, thrombophlebitis, or tumors (meningiomas). The extradural hemorrhage is arterial where as subdural hemorrhage is venous in nature ii. In case of extradural hemorrhage paralysis first appears within the face, then spread to the decrease part of the physique where as in subdural hemorrhage the spread of paralysis is haphazard iv. Sinuses Running Transversely and Communicating the Paired Sinuses of the Opposite Sides Anterior Intercavernous Sinus Situation: Anterior border of the diaphragma sellae. Posterior Intercavernous Sinus Situation: Posterior border of the diaphragma sellae. Extension: From the posteroinferior angle of the parietal bone to the posterior a part of the jugular foramen. Course After origin, it passes backwards to the apex of the petrous a half of temporal bone. Situation One on all sides of sella turcica of the superior surface of the physique sphenoid bone, at the junction of body and higher wing. Termination It terminates by dividing in to superior and inferior petrosal sinuses. Part of inside carotid artery Posteriorly Semilunar ganglion of trigeminal nerve. Structures current between the endothelium of cavernous sinus and the dura mater: 1. Internal carotid artery with sympathetic plexus near the medial wall of the sinus 2. With the inner jugular vein-by inferior petrosal sinus and a venous plexus across the internal carotid artery three. With the superior sagittal sinus-through the superficial center cerebral vein and superior anastomotic vein. It drains in to superior and inferior petrosal sinuses as a substitute of draining in to a longer vein. Due to shut relation with the inner carotid artery, in case of fracture on the middle cranial fossa, there could also be probability of arterio-venous communication, results to-pulsating tumor of the orbit, assortment of blood behind the eyeball producing pulsating exophthalmus. Suppurative ailments of paranasal sinuses, higher nasal cavity or from danger area of face might cross to cavernous sinus causing septic thrombosis of cavernous sinus and meningitis. Severe ache within the eye and forehead in the area of distribution of the ophthalmic nerve because of this nerve is the content material of cavernous sinus b. Involvement of oculomotor, trochlear and abducent nerves ensuing paralysis of the muscles supplied by them. Venous signs: Edema of the eyelids, cornea and root of the nostril, with exophthalmos ensuing from congestion of the orbital veins. Infection can unfold from the danger area of face through the next veins cavernous sinusinferior ophthalmic vein-Facial vein. Infection behind the auricle within the scalp spreads via following method: Posterior auricular vein-mastoid emissary vein-Junction of sigmoid sinus-the transverse and sigmoid sinuses-superior petrosal sinus and cavernous sinus. Enlargement of pituitary gland causes obstruction to the venous flow as a outcome of the pressure on cavernous sinus. Situation It is located in the infratemporal fossa, slightly below the foramen ovale. It lies medial to the mandibular nerve It lies lateral to the tensor veli palatini In entrance of the middle meningeal artery Behind the medial pterygoid muscle It surrounds the origin of the nerve to the medial pterygoid muscle. Preganglionic fibers are derived from the inferior salivatory nucleus of the medulla oblongata then passes successively through a. Sympathetic root is derived from the plexus across the center meningeal artery ii. It carries postganglionic fibers arising from the superior cervical ganglion of sympathetic trunk iii. Postganglionic parasympathetic fibers of the ganglion join with the auriculotemporal nerve to provide the parotid gland which is secretomotor in perform ii. Postganglionic sympathetic fibers which cross by way of the ganglion with out relay be a part of with the auriculotemporal nerve to supply the parotid gland which is vasomotor in operate iii. The fibers from the nerve to the medial pterygoid move by way of the ganglion with out relay and provides the tensor veli palatini and tensor tympani muscular tissues iv. The chorda tympani nerve and nerve of the pterygoid canal is connected to the otic ganglion. These connections type an alternate pathway of style from the anterior two-third of the tongue to the geniculate ganglion of facial nerves. The ciliary ganglion lies between the optic nerve and the lateral rectus muscle ii. The ophthalmic artery normally lies medial to the ganglion Connections or Roots the roots enter or go away the ganglion posteriorly. It consists of preganglionic fibers from Edinger westphal nucleus, and relay in the ganglion iii. The postganglionic fibers arising in the ganglion cross by way of the brief ciliary nerves and supply the sphincter pupillae and ciliaris muscular tissues. It incorporates postganglionic fibers from the superior cervical sympathetic ganglion iii. Situation Near the apex of the orbit about 1 cm in front of medial finish of the superior orbital fissure. It is an important loop which lies in entrance of the carotid sheath on every of side a half of entrance of the neck ii. It is on the stage of decrease part of laryngopharynx at the degree of fifth or sixth cervical vertebrae. The inferior root or descending cervical nerve is derived from second and third cervical spinal nerves. Then the superior and inferior roots be a part of together in entrance of the frequent carotid artery. Superior root is steady with the descending department of the hypoglossal nerve Type Sensory nerve. Origin this nerve arises from the ophthalmic nerve in the anterior a half of the cavernous sinus.
Innopran xl 40 mg trusted
A point is taken 2 cm lateral to the midpoint between third and 4th thoracic spines blood pressure cuff cvs buy cheap innopran xl 40 mg on line. Another level is taken 3 cm lateral to the midclavicular line on 4th intercostal area blood pressure chart high systolic low diastolic innopran xl 40 mg buy with visa. Transverse Fissure (Right Side Only) It is represented by a line drawn from the midline at proper 4th costal cartilage up to proper midaxillary line, to meet oblique the fissure. Joining the 2 points by a curved convex to the left downwards line which, cuts the costal margin between the ideas of left ninth and tenth costal cartilages. Another level is taken on the left fifth intercostal house on the left midclavicular line iii. Joining the 2 factors by a line with convexity upwards represents the fundus of stomach. Join the third and fourth factors by a line convexity laterally which passes via the primary point. Hilum of the left kidney must be above the transpyloric aircraft and higher pole more inclined medially than the lower pole. Join the hilar concavity with the adjoining third and fourth points by traces convexity medially. Take a degree on the transpyloric plane 5 cm lateral to the midline 724 Human Anatomy for Students. Take one other level 5 cm under the transpyloric airplane and similar distance lateral to the midline iii. Take one other level on the junction of upper onethird and lower twothirds of a line drawn from a degree 1. Take some extent four cm away from the midline at the degree of lower border of first lumbar spine ii. Take another point over a dimple which overlies the posterior superior iliac spine. Another point is taken on the left 5th intercostal house under and medial to the left nipple iii. Joining these factors by a line with barely concavity downwards on the midline opposite the xiphoid course of. Joining this level with the right finish of superior border by a line with convexity to the right represents the right border of liver. Inferior Border It is represented by a line drawn from the lower end of right border and left end of superior border. Draw two lines from first and fifth points they passes upwards on the sixth level, which represents the neck, body and tail of pancreas. Join the above points by a line which slopes downwards and to the right, on the border presents a slight notch opposite the tip of the proper ninth costal cartilage for the fundus of the gallbladder. Take another level 4 cm beneath the umbilicus and about similar distance to the left of the midline iii. Join the above two points by a curved line which is slightly convexity to the left represents the inferior mesenteric artery. Take some extent 5 cm above the transpyloric airplane and 2 cm right to the median plane ii. Fundus of Gallbladder It is represented by some extent mendacity opposite the tip of proper 9th costal cartilage within the angle between proper costal arch and lateral border of proper rectus abdominis muscle. It is represented by two parallel lines 2 cm aside begins barely to the left of midline at the level of physique of T12 then the traces descends downwards to 10 cm ii. Then it ascends and enters in to the thorax by piercing the diaphragm at the degree of 8th thoracic vertebra behind the sternal finish of right 6th costal cartilage. Second Part Draw comparable lines (like first part) on the best lateral plane which extends from the end of the primary half then downwards for 7. Fourth Part Draw two strains which extends from the left end of the third half to the duodenojejunal flexure which lies 1 cm under the transpyloric airplane and three cm to the left of the median plane. Take one other point on the midpoint between the anterior superior iliac backbone and symphysis pubis. Join the above two points by a line with slight lateral convexity represents the common and external iliac arteries. Ileocecal Valve or Orifice It is represented by two parallel horizontal traces 2 cm apart, simply at the junction of proper lateral plane and transtubercular plane. Transverse Colon Draw two parallel lines 5 cm apart which begins from the higher part of the ninth costal cartilage, then runs downwards and medially to the umbilicus, again the strains run upwards and laterally, crossing the transpyloric and in addition the left lateral aircraft, to finish at the eight costal cartilage. Base of Appendix It lies simply 2 cm below the junction between the transtubercular and right lateral planes. Left Colic Flexure It is marked by some extent above the transpyloric airplane to the left of the left lateral plane on the stage of left 8th costal cartilage. Rectum and anal canal are marked on the again superior iliac spines to the anus ii. The lower a half of these strains from 1 cm beneath the second sacral spine represent the rectum and anal canal. Ascending Colon Draw two parallel traces 5 cm apart good to the right lateral plane, from the extent of the transtubercular plane extends above to the higher part of the ninth costal cartilage. Right Colic Flexure It is marked by some extent opposite the tip of the best 10th costal cartilage and beneath the transpyloric aircraft. Another level is taken above and in entrance of the wrist joint between the tendon of flexor carpi radialis and the outstanding margin of lower end of radius iii. By joining these two points by a line with convexity laterally in its upper onethird and in the decrease twothirds of the line will be vertical. A point is taken in front of the wrist joint between the tendon of flexor carpi radialis and the outstanding margin of the lower finish of radius ii. Another level is taken beneath the prominency of coracobrachialis in the axilla iii. Another point is taken 1 cm beneath the bend of the elbow just medial to the tendon of biceps brachii. Bifurcation of Brachial Artery It is represented by a point 1 cm beneath the bend of the elbow medial to the tendon of biceps brachii. A level is taken 1 cm beneath the bend of elbow simply medial to the biceps brachii tendon ii. A point is taken at the lateral facet of the pisiform bone and is joined to the medial epicondyle of humerus by a straight line iii. Another point is taken on the junction of higher onethird and decrease twothirds of this straight line iv. A point is taken 1 cm below the bend of the elbow joint immediately medial to the tendon of biceps brachii Pisiform Bone i.