
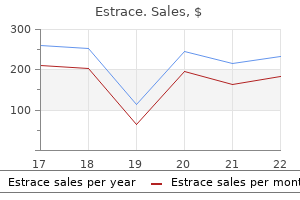
Estrace dosages: 2 mg, 1 mg
Estrace packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Estrace 1 mg buy free shipping
Epinephrine has a complementary and multifaceted position within the protection in opposition to hypoglycemia by stimulating hepatic glucose manufacturing (initially via glycogenolysis menstrual issues cheap estrace 2 mg mastercard, then gluconeogenesis from the liver and kidney) women's health issues and solutions estrace 1 mg generic fast delivery, adipose tissue lipolysis, and skeletal muscle glycogenolysis and proteolysis, whereas inhibiting glucose uptake by insulin-responsive tissues. Both can stimulate hepatic glucose manufacturing (gluconeogenesis) and inhibit glucose uptake. However, the contribution of each of those hormones is just about 20% to that of epinephrine. The glucose threshold for the technology of autonomic signs and signs is plastic in nature however is often 60 mg/dL (3. It should be famous that hunger, per se, is a poor symptom discriminator for hypoglycemia. The origins of autonomic indicators and symptoms are complicated but sympathoadrenal output appears to be the primary driver. Epinephrine is answerable for 20�25% of the symptoms of hypoglycemia, suggesting that a big portion of signs and symptoms come up from sympathetic neural activation (32). The ability to acknowledge hypoglycemic symptoms inside oneself is identified as hypoglycemia consciousness. Autonomic signs and symptoms are the symptoms most recognizable to the affected person, but the particular mixture of symptoms skilled during a hypoglycemic episode varies interand intra-individually. Hormonal counter-regulatory responses and hypoglycemic symptoms happen at similar thresholds in women and men, but in women, peak counter-regulatory hormone ranges are lower (33,34). Without adequate glucagon secretion, the usual rapid response (10�15 minutes) of glucose manufacturing from the liver is decreased. Glycogenolysis and later gluconeogenesis (if glycerol, lactate, pyruvate and amino acids are available) may also be impaired. The ability to promote glucose recovery from hypoglycemia is dependent upon epinephrine-mediated beta-adrenergic mechanisms in the glucagon deficient state (36). This is r particularly outstanding after antecedent hypoglycemia or related to traditional diabetic autonomic neuropathy. Without sufficient epinephrine stimulation, hepatic glycogenolysis and later hepatic and renal gluconeogenesis are impaired. The inhibitory effect of epinephrine on skeletal muscle glucose uptake is misplaced and hypoglycemia could be extended. Signs and signs: Symptom responses turn into blunted together with reduced hormonal counter-regulatory responses (37). Reduced epinephrine ranges are an element, however decreased sympathetic neural outflow may be implicated. Failure of these protective mechanisms can lead to severe, unimpeded hypoglycemia. A blunted epinephrine response increases the risk of iatrogenic hypoglycemia 25-fold (38). Patients additionally develop hypoglycemia unawareness, in which signs are delayed and blunted and may be unrecognizable to the person. Prolonged low to moderate endurance train blunts counterregulatory responses to subsequent hypoglycemia (45), whereas, reciprocally, antecedent hypoglycemia blunts counter-regulatory responses to train (46). In both situation, the patient is uncovered to a larger risk of creating hypoglycemia. During sleep, counter-regulatory responses to and awareness of hypoglycemia are delayed and reduced (47), and prolonged nocturnal hypoglycemia is a common prevalence (48). Furthermore, nocturnal hypoglycemia blunts responses to next-day hypoglycemia (49). A variety of interventions have been shown to at least partially rescue counterregulatory responses to hypoglycemia. First, strict avoidance of hypoglycemia by Hypoglycemia relaxing glycemic targets and educating patients about preventive strategies can help to recuperate hypoglycemia awareness and epinephrine responses (50). Age Considerations Compared to their youthful counterparts, older folks with diabetes are at increased danger of extreme hypoglycemia, especially in instances of longer length diabetes and limited residual insulin secretion (52). Regular schooling regarding symptom identification and therapy choices is crucial in this inhabitants in addition to ongoing assessment of cognitive function (56). On additional questioning, he stories waking in the middle of the night time 2� 3 times per week with hunger and sweats. He reviews comparable symptoms after the lunch meal and this prevents him from a day walk. Do You Think His Current HbAc Is an Appropriate Target in View of His Age/Longevity of Diabetes/and Other Factors This case illustrates the untoward effects of over-aggressive blood glucose therapy in aged sufferers. This could be an opportunity to focus on in detail dietary and life-style adjustments that could improve the blood glucose levels with out further medical remedy. The addition of basal insulin, whilst efficient and started at a comparatively low dose, will increase the danger of hypoglycemia (as it did on this patient). Management of Hypoglycemia Most cases of hypoglycemia in sufferers with diabetes are self-diagnosed and E. Take 15�20 grams of carbohydrate: r 3-4 glucose tablets; r 4 oz (1/2 cup) of fruit juice; r 6 oz (1/2 can) of regular soda. If the person is handled with an alpha-glucosidase inhibitor, only pure glucose gel or tablets should be taken, as this drug class inhibits absorption of other forms of carbohydrate. Blood glucose must be measured 15 minutes after consuming carbohydrate, and extra carbohydrate should be ingested if hypoglycemia or hypoglycemic signs persist. Glucagon kits can be prescribed to patients with diabetes, and friends, relations or co-workers Plasma Glucose<70 mg/dL (3. The results of glucagon, which acts through stimulation of hepatic glycogenolysis, are delayed by roughly 10 minutes from time of injection and are solely inducible in those with obtainable glycogen shops. Of note, family members or responders should keep away from sublingual placement of carbohydrates. After resolution of hypoglycemia, a full meal or advanced snack must be consumed as an insulin depot should be active and to restore glycogen stores. Severe hypoglycemia requiring help of a second or third party ought to be assessed and addressed within the hospital setting. Consideration ought to at all times be given to different acute medical conditions which will mimic or coincide with hypoglycemia. However, speedy recognition of a low glucose is imperative as prolonged severe hypoglycemia may end up in irreversible brain injury, cardiovascular strain, and demise (25,57). The majority of protocols for emergency medical responders point out using 25 g of 50% dextrose in water (D50), although some protocols point out D10 (10% dextrose) or present each D10 and D50 as remedy choices (58). D50 is an irritant and supply via a large gauge port and vein, followed by a saline flush, is preferable. Alternatively, D20 (20% dextrose) or D10 are much less irritating and could be administered via a peripheral vein in a proportionally bigger volume. As in self-treated sufferers, once euglycemia is attained, a meal or a snack including carbohydrate and protein must be ingested to forestall a recurrent episode of hypoglycemia.
Estrace 2 mg discount visa
Hyperthyroidism after allogeneic hematopoietic stem cell transplantation: a report of four circumstances breast cancer surgery estrace 2 mg generic without prescription. Successful treatment of thyroid storm with plasmapheresis in a affected person with methimazole-induced agranulocytosis women's health magazine birth control estrace 2 mg order on line. Severe hypercalcemia related to hepatocellular carcinoma secreting intact parathyroid hormone: a case report. Parathyroid hormone-related peptide as a potential cause of hypercalcemia in a hepatocellular carcinoma affected person. Parathryoid hormone related peptide inflicting hypercalcaemia in a affected person with hepatocellular carcinoma. Denosumab for treatment of immobilization-related hypercalcaemia in a patient with superior renal failure. Teriparatide efficacy in the treatment of extreme hypocalcemia after kidney transplantation in parathyroidectomized sufferers: a series of 5 case stories. Combination remedy of denosumab and calcitriol for a renal transplant recipient with severe bone loss because of therapy-resistant hyperparathyroidism. Dramatic increase in parathyroid hormone and hypocalcaemia after denosumab in a kidney transplanted patient. Mechanisms of bone loss following allogeneic and autologous hemopoietic stem cell transplantation. Tertiary "hyperphosphatoninism" accentuates hypophosphatemia and suppresses calcitriol levels in renal transplant recipients. Endocrine and Metabolic Changes with Aging Endocrin-Aging: Recognizing and Managing Care in Older Frail Persons Angela M. The presence of persons over the age of sixty five is projected to enhance from 8% in 2012 to 16% by 2050. The presentation of endocrine problems in older persons is often delicate and the prognosis is well missed. New consensus guidelines have suggested that hypoglycemia needs to be averted, and for wholesome older persons glycosylated hemoglobin (HbA1C) targets ought to be between 7. End-of-life care typically focuses on the care of an individual within the last two years of their life. Introduction Over the last century, global demographics have persistently underlined a substantial rising pattern in the number of elderly persons worldwide. A number of physiological modifications in circulating hormones happen with aging (Table 11-1) (1). Insulin resistance with aging results in an increase in metabolic syndrome and sort 2 diabetes mellitus in older individuals. Increases in aldosterone and vasopressin can result in hypertension and hyponatremia, respectively. Hip fractures are related not only with the decline in bone and muscle mass, but in addition because of delirium, which can be as a end result of hypothyroidism, hypoandrenalism, vitamin B12 deficiency, hyponatremia, and hypercalcemia. Finally, diseases similar to sleep apnea, that are quite common in older individuals can lead to hypertension, hyperglycemia, and osteoporosis, as a end result of a rise in cortisol, aldosterone, and catecholamines. This article will give consideration to endocrine emergencies that are frequent in older persons. In explicit, completely different displays that always occur in older individuals might be stressed as will the problem in diagnosing hypo-endocrine problems whose symptoms can be similar to a number of the common modifications in regular aging. Pituitary Dysfunction within the Elderly the anterior and the posterior lobes of the pituitary gland endure subtle changes throughout superior aging. In explicit, the anterior lobe undergoes modifications primarily because of fibrosis and vascular alterations. Depending on the degree of scientific penalties of such alterations, treatment may be Endocrine and Metabolic Changes with Aging: Endocrin-Aging necessary. Even although fibrosis and vascular alterations could lead to hypopituitarism, a lot of the causes of hypopituitarism within the aged are just like those in youthful populations. In older individuals, pituitary cell destruction causes more than 95% of hypopituitarism. There is an increase in the percentage of pituitary adenomas found in the aged (2). Clinical presentation is usually insidious, being characterized by non-specific manifestations, similar to weight reduction, fatigue, lowered urge for food, low muscle energy, or hypotension. Considering that many of those signs overlap with these of normal getting older, hypopituitarism could be simply underdiagnosed within the elderly. Large adenomas can even compress anterior pituitary cells, thus leading to an insufficient secretion of hormones (3). With aging, bitemporal hemianopia is the most common visual subject defect with pituitary tumors (which are often large non-functioning adenomas), nevertheless, this usually goes undiagnosed because visual disturbances associated to compression are often attributed to other common causes of visual disturbance in this population. Other causes of hypopituitarism include an infection, traumatic brain harm, cerebral ischemia, which in turn results in decreased blood supply to pituitary vascularization. Older individuals could be afflicted with numerous comorbidities with polypharmacy, which can in turn influence hormonal metabolism (2). With aging, there are adjustments in the circadian rhythm of the discharge of hypothalamic releasing hormones. Stressors also can alter the release of hypothalamic hormones with the classical example of hypoxia associated with sleep apnea leading to a rise in cortisol and aldosterone with related hypertension and hyperglycemia. Primary hypothyroidism is a extra frequent discovering amongst older adults related to decline in thyroid perform and autoimmune illness. Numerous factors have been proven to have diverse degrees of implications on pituitary-thyroid operate in old age. There could be very little clinical proof that the thyroid hormone effects associated with physiological modifications of getting older significantly play a job within the growth of frailty (7). Symptoms of hypothyroidism are extra refined in older individuals and sometimes mimic regular growing older complaints. Common symptoms are weight gain, fatigue, hair loss, non-pitting edema, macroglossia, hoarse voice, constipation, reminiscence loss, melancholy, hypertension, and bradycardia (8). The presence of a goiter or a surgical scar in the neck increases the chance of hypothyroidism. Treatment is required to forestall potential harmful clinical outcomes (myxedema coma, heart failure, hyponatremia, Angela M. In order to stop adrenal disaster, patients should receive glucocorticoid therapy as indicated earlier than beginning thyroid hormonal remedy (10). Alternatively, consideration for excluding adrenal insufficiency by acceptable testing should happen prior to starting thyroxine therapy in both sufferers with main or secondary hypothyroidism. Myxedema coma is a severe type of hypothyroidism with delirium or coma, pericardial effusion, seizures, toxic megacolon, hypothermia, hypoventilation, and bradycardia (11). It is usually precipitated by ailments such as an infection, myocardial infarction, stroke, trauma, or drugs.
Diseases
- Cleft lip and/or palate with mucous cysts of lower
- Al Gazali Sabrinathan Nair syndrome
- Fibrosing mediastinitis
- Osteopathia striata pigmentary dermopathy white forelock
- Ovarian dwarfism as part of Turner syndrome
- Medulloblastoma
Buy 2 mg estrace mastercard
Introduction: Emergency Management of Adrenal Disorders Post-mortem examination revealed bilateral adrenal tumors that had been described on the time as sarcoma and angiosarcoma (1 women's health center tuscaloosa al discount estrace 2 mg mastercard,2) pregnancy exercise classes generic estrace 2 mg online. A seismic change in our understanding of pheochromocytomas occurred in 2000, when Baysal et al. This new paradigm of pheochromocytomas and paragangliomas as syndromic tumors which might be a half of an inheritable genetic syndrome has changed our approach to management. It is now recommended that all patients be recommended on the worth of genetic testing, and that those who are found to have a genetic susceptibility be enrolled in a potential surveillance program (5,6). Further, family members may be recommended based on the results of the genetic testing of the proband, thereby identifying other at-risk individuals. Although more longitudinal research to determine the most effective and exact surveillance technique are nonetheless wanted, imaging is extensively used to survey for model new tumors. These insights then increase the question how we should change our screening practices to detect autonomous aldosteronism earlier in its pathogenesis, and when and the way we ought to always implement interventions (such as mineralocorticoid receptor antagonists) to mitigate the cardiovascular dangers associated with inappropriate aldosterone secretion. Since large cohort research have proven that inappropriate aldosterone secretion increases the risk for developing incident hypertension in normotensives (16,17), we await future studies that target early interventions to mitigate mineralocoritcoid receptor activation in these susceptible individuals. However, the last five years have witnessed an explosion in genetic mechanisms that contribute to autonomous aldosterone secretion, almost all of which involve alterations in cell membrane channels that increase intra-cellular calcium flux. These are overwhelmingly somatic mutations found in resected aldosterone producing adenomas; however, hardly ever some of them are inheritable. Incidentally Discovered Adrenal Tumors the rising use of cross-sectional abdominal imaging worldwide has elevated the detection of incidental adrenal neoplasia. The overwhelming majority of these incidentally discovered adrenal lots Introduction: Emergency Management of Adrenal Disorders are benign and non-functional; nevertheless, a notable proportion of those benign tumors should still hypersecrete adrenal cortical hormones, similar to cortisol. Elegant studies using steroid metabolomics have proven that even "nonfunctional" adrenal tumors hypersecrete glucocorticoids, thereby implicating a spectrum of glucocorticoid extra that extends properly beyond our traditional capability to detect circulating cortisol (21). Much focus has been placed on defining and detecting this subclinical hypercortisolism within the clinical setting (also defined as autonomous cortisol secretion). Numerous cross-sectional studies have advised that subclinical hypercortisolism is related to higher blood strain, impaired glycemia, and low bone density (22), and meta-analyses of anecdotal stories have instructed that surgical resection of the source of hypercortisolism may right these abnormalities (23). Longitudinal studies have proven that subclinical hypercortisolism in patients with adrenal tumors is related to greater danger for creating heart problems and diabetes (24,25). These situations continue to require physicians to practice the "art of medication" and assess each affected person on a case-by-case basis to determine the risk-tobenefit ratio of therapy versus on-going monitoring. Conclusions In abstract, the last 5�10 years in adrenal drugs and science have been transformative. Despite the exceptional insights gained from genetic, molecular, and metabolomic studies, we nonetheless await the translation of many of those findings into strong clinical and randomized interventional trials to develop high-grade evidence that will confidently impression patient (including emergency) care. Thus, as we have fun and revel in these recent accomplishments, we must stay vigilant and determined to continue to increase and domesticate new proof to best serve our sufferers. Ein Fall von doppelseitigem, v� llig latent verlaufenen o Nebennierentumor und gleichzeitiger Nephritis mit Ver� nderungen am a Circulationsapparat und Retinitis. Pheochromocytoma and paraganglioma: an endocrine society scientific apply guideline. Genetic testing in the clinical care of sufferers with pheochromocytoma and paraganglioma. The management of major aldosteronism: case detection, prognosis, and therapy: an Endocrine Society Clinical Practice Guideline. Case detection, prognosis, and therapy of patients with primary aldosteronism: an endocrine society scientific practice guideline. Dietary sodium restriction increases the chance of misinterpreting gentle cases of major aldosteronism. Prevalence and clinical manifestations of primary aldosteronism encountered in main care follow. Evidence of main aldosteronism in a predominantly feminine cohort of normotensive individuals: a very high odds ratio for progression into arterial hypertension. Clinical and genetic correlates of aldosterone-to-renin ratio and relations to blood strain in a community sample. Aldosterone-stimulating somatic gene mutations are widespread in normal adrenal glands. Urine steroid metabolomics as a biomarker software for detecting malignancy in adrenal tumors. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Adrenal disaster is caused by lack of manufacturing of the adrenal hormone cortisol and/or mineralocorticoids and requires instant remedy. Symptoms of adrenal insufficiency are nonspecific and a high stage of medical suspicion is required to make the proper diagnosis. Effective continual care of major and secondary adrenal insufficiency is important, as this is a vital alternative to reduce future admissions by reiterating sick-day rules and other disaster preventative measures, improve high quality of life, and reduce morbidity and mortality. Introduction the adrenal glands are small, bilateral constructions that weigh approximately 5 g each and lie retroperitoneally on the apex of every kidney. The medulla or internal portion of the gland (which constitutes roughly 10% of each adrenal) secretes epinephrine (adrenaline) and norepinephrine (noradrenaline) and is a half of the sympathetic nervous system. The cortex forms the bulk of the adrenal gland (approximately 90%) and is liable for secreting three types of hormones: glucocorticoids, mineralocorticoids, and adrenal androgens (1). Because epinephrine and norepinephrine may additionally be derived from non-adrenal sources. Acute Adrenal Insufficiency Table - Clinical features of main adrenal insufficiency and adrenal disaster. Symptoms Signs Routine laboratory checks Adrenal insufficiency Darkened complexion/increased pigmentation/easier suntanning Hyperpigmentation (primary only), particularly of sun-exposed areas, pores and skin creases, mucosal membranes, scars, areola of breast Low blood strain with elevated postural drop Hyponatremia Hyperkalemia Uncommon: hypoglycemia, hypercalcemia Postural dizziness Anorexia, abdominal discomfort, weight loss Fatigue Adrenal crisis Syncope Abdominal ache, nausea, vomiting; may mimic acute abdomen Confusion Back pain Severe weak point Hypotension Abdominal tenderness/guarding Hyponatremia Hyperkalemia Hypoglycemia Hypercalcemia Reduced consciousness, delirium Most signs are non-specific and present chronically, usually resulting in delayed prognosis. Hyponatremia and, later, hyperkalemia are sometimes triggers to prognosis, requiring biochemical confirmation of adrenal insufficiency. Adrenal disaster is a medical emergency with hypotension, marked acute stomach symptoms, and marked laboratory abnormalities, requiring instant remedy. Additional symptoms and indicators might come up from the underlying reason for adrenal insufficiency. Cortisol is the principal glucocorticoid; aldosterone is the principal mineralocorticoid; and along with adrenal androgens constitutes the major hormones of the more than 30 produced by the adrenal cortex. All of the adrenal cortical hormones have an identical construction in that each one are steroids, and each of the steps concerned in the synthesis of the varied hormones requires a selected enzyme. The mineralocorticoids are controlled predominantly by the renin-angiotensin system. Acute adrenal insufficiency, additionally termed adrenal disaster, is a life-threatening endocrine emergency (2�4). It presents with marked signs and indicators, characteristic laboratory abnormalities, and requires instant remedy (Table 20-1). The severity of this situation is said to the Glenn Matfin Table - Clinical findings of adrenal insufficiency Finding Primary (%) Secondary/Tertiary (%) Anorexia and weight loss Fatigue and weakness Gastrointestinal symptoms, nausea, vomiting Myalgia, arthralgia Orthostatic hypotension Hyponatremia Hyperkalemia Hyperpigmentation Secondary deficiencies of gonadal, progress hormone, thyroxine, and antidiuretic hormone could happen Associated autoimmune circumstances Yes (100) Yes (100) Yes (50) Yes (10) Yes Yes (85�90) Yes (60�65) Yes (>90) No Yes (100) Yes (100) Yes (50) Yes (10) Yes Yes (60) No No Yes Yes No the numbers are representative, some symptoms and signs may be subtle.
Discount estrace 2 mg free shipping
Investigations confirmed extreme biochemical thyrotoxicosis; regular bilirubin; pulmonary edema women's health issues depression estrace 1 mg purchase on-line, and atrial fibrillation women's health north florida 2 mg estrace purchase. Because of the fever, blood cultures are drawn and she or he is admitted to intensive care unit. This could be confirmed utilizing the Burch-Wartofsky Point Scale for Diagnosis of Thyroid Storm (14). An general rating is obtained by including the scores from every of seven standards (range 0� 140). The total score of one hundred fifteen for this affected person is consistent with a prognosis of thyroid storm (45 highly likely thyroid storm). This diagnosis was also confirmed using the Japanese Thyroid Association Diagnostic Criteria for Thyroid Storm scoring system (15). Hossein Gharib Burch-Wartofsky Point Scale for Diagnosis of Thyroid Storm (14) Clinical function Scoring points Thermoregularory dysfunction Temperature F (C) <99 (37. Conclusions In order to assist our sufferers with thyroid illness, we should proceed to improve iodine dietary status; design research to determine if screening for thyroid illness, or therapy of subclinical disease, improve outcomes; develop cost-effective screening packages to detect early illness; acknowledge inflammatory thyroiditis caused by new immune therapies and leverage new insights into other thyroid conditions; encourage healthcare supply groups to present appropriate remedy for hypo- and hyperthyroidism (including thyroid emergencies); and promote public education through awareness campaigns and academic materials. This section, devoted to advanced and common thyroid emergencies, discusses pathogenesis, contributing events, prognosis, treatment and outcomes. Each chapter is written by authors with important expertise and contribution to the topic space. The chapters are well-written, up-to-date, and concise and ought to be of nice value to clinicians dealing with sufferers with thyroid disorders. Guidelines of the American Thyroid Association for the analysis and administration of thyroid illness throughout pregnancy and the postpartum. Management of thyroid dysfunction throughout pregnancy and postpartum: An Endocrine Society Clinical Practice Guideline. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules�2016 Update. Thyroid most cancers: zealous imaging has elevated detection and remedy of low threat tumours. Incidence of thyroidrelated opposed events in melanoma patients handled with pembrozilumab. Diagnostic criteria, clinical features, and incidence of thyroid storm primarily based on nationwide surveys. Hennessey Key Points r Myxedema coma is a decompensated state of hypothyroidism ensuing from extreme and prolonged depletion of thyroid hormones resulting in altered mental status and other medical options related to widespread multiorgan dysfunction. While this could be a rare situation on the spectrum of thyroid problems, myxedema coma is considered an endocrine emergency due to the hazard of increased mortality with latest rates of 20�29% reported. Treatment includes administration of hydrocortisone, levothyroxine, and consideration of liothyronine use, as properly as basic medical and cardiopulmonary support as wanted. In 1877, the time period myxedema was first utilized by William Miller Ord after Sir William Withey Gull correlated this presentation with atrophy of the thyroid gland (1). The time period myxedema coma is misleading as most sufferers are merely obtunded, but not as regularly in a real state of coma. In 1953, the term myxedema coma was used at the aspect of fatal outcomes of 4 circumstances where coma was noted in patients within the setting of typical manifestations of myxedema (2). While this can be a rare situation on the spectrum of thyroid problems, with a reported incidence rate of zero. In a examine assessing an inpatient database in Japan of 149 patients, the in-hospital mortality price was 29. Therefore, it is very important promptly recognize and deal with myxedema coma in an attempt to enhance outcomes. In this example, myxedema coma could be induced by the extra presence of widespread inciting factors similar to infections like urosepsis or pneumonia or circumstances corresponding to heart failure, exposure to a chilly environments, trauma, surgery, cerebrovascular accidents, or gastrointestinal bleeding (8�10). Medications that usually have been implicated in precipitating myxedema coma are anesthetics, sedatives, narcotics, lithium, amiodarone, sunitinib, and phenytoin (8,11). Neurological dysfunction might present as extreme hypothermia described as core temperatures <90 F (32. Altered mental status in myxedema coma is caused by underlying cerebral tissue hypothyroidism in addition to multiple mechanisms similar to decreased cerebral blood flow, hyponatremia, and hypoxemia. These also can decrease the edge for precipitation of seizures in the setting of myxedema coma (8, 9). Beside memory impairment, dysarthria, seizures, sensory and motor peripheral neuropathy have also been noted on this extreme state of hypothyroidism (12). Due to innate cardiovascular-related compensatory mechanisms within the setting of reduced availability of thyroid hormone, one can develop diastolic dysfunction and peripheral vasoconstriction which collectively might end in a reduction of circulating blood volume (13). Further, primary cardiac pump perform is instantly compromised due to decreased cardiac inotropy which may lead to cardiomegaly and negative chronotropy leading to bradycardia. Therefore, low cardiac output and hypotension can precipitate cardiogenic shock (8,9). Hypoventilation occurs within the setting of altered respiratory sensitivity to hypoxia and hypercapnia as nicely as a discount in respiratory drive. In addition, respiratory muscle dysfunction may occur which additional impairs ventilation (8,10). It has been noted in sufferers with even milder types of hypothyroidism, compared to controls, that a better prevalence of cough, sputum production, and airway inflammation may be noticed (16). In addition, an underlying anatomic course of within the setting of an infection or a manifestation of hypothyroidism, similar to pleural effusions or macroglossia, can further intervene with the lung quantity or airway measurement (10,15). There is a report of neuropathic oropharyngeal dysphagia that may contribute to aspiration and further respiratory impairment (12). The incidence of hyponatremia is based upon a diminished capacity to clear a free water load which is a consequence of the mixed results of decrease renal perfusion and the presence of elevated antidiuretic hormone levels (9,10,18,19). Due to the potential of simultaneous adrenal insufficiency and impaired gluconeogenesis, hypoglycemia can occur (8). It has been noticed that lowered intestinal motility could result in signs of higher and lower gastrointestinal distress and lowered absorptive effectivity contributing to paralytic ileus with stomach distention (9,20,21). Clinical Manifestations We can doc the everyday features of hypothyroidism previous the presentation of myxedema coma, together with fatigue, weight achieve, chilly intolerance, constipation, cool and dry pores and skin. In addition, brittle nails, Myxedema Coma macroglossia, hoarse voice, muscle cramps, menstrual disturbances, periorbital and non-pitting edema, or delayed deep tendon reflexes may be observed. The clinician ought to be especially alert to the presence of a goiter, thyroidectomy scar, or historical past of I131 remedy (8,9,22). Myxedema coma is 8-fold extra widespread in girls in comparability with men, and is a frequent explanation for hospitalization among women over 60 years of age for a diagnosis of hypothyroidism (4,19). As a consequence of this gender distinction, most circumstances of myxedema coma occur during the winter months in girls (13).
Buy estrace 1 mg otc
Whenever acute zoledronic acid is supplied in these emergency conditions womens health for life lima ohio generic estrace 2 mg free shipping, it is important to menopause diagnosis 1 mg estrace purchase mastercard guarantee that patients are both vitamin D- and calcium-sufficient to keep away from hypocalcemia. Serum calcium corrected for levels of serum albumin must be monitored within the setting of acute therapy. With immobilization the elevated bone resorption continues and will even enhance, whereas bone formation, previously well coupled to resorption, decreases, and hypercalcemia can develop. Fink the potential for an increased vascularity in the bone, as has been described earlier, and in some instances have been proven to have will increase in cardiac output as a consequence. Epidemiologic studies recommend an growing prevalence worldwide, the trigger is of unsure etiology however may be attributable to changing dietary practices (including calcium supplementation), migration from cooler rural settings to hotter urban settings, and even world warming. Obesity, hypertension, metabolic syndrome, and diabetes at the second are acknowledged as necessary risk factors. The term "renal colic" is widely used to describe the pain resulting from passage of kidney stones by way of the urinary tract. This "colicky" renal pain is among the commonest symptoms resulting in emergency care presentation, and infrequently prompts intensive differential diagnosis and work-up. In most cases, the etiology of hypercalciuria stays unexplained and is usually termed idiopathic hypercalciuria. Uric acid stones are associated with the metabolic syndrome, obesity, and diabetes, all of which lead to impaired ammoniagenesis and acid urine. Laboratory evaluation should include a urinalysis, full (full) blood count, and complete metabolic profile. Kidney stone prevention is relatively inexpensive, cost-effective, and sometimes practiced. Goldfarb Introduction the term "renal colic" is extensively used to describe the pain resulting from the passage of kidney stones through the urinary tract. The extreme intermittent flank ache that radiates to the lower stomach, genitalia, and groin, could also be related to different gastroenterological or urological symptoms. This "colicky" renal pain is likely considered one of the commonest signs resulting in emergency care presentation, and infrequently prompts in depth differential prognosis and work-up. In this text we focus on the pathophysiology of renal colic, the analysis and acute administration of kidney stones, and the measures taken to forestall stone recurrence. Pathophysiology the ache of renal colic may simply be thought to come up from the muscular contraction of the ureter in response to the irritating, descending stone. The ureteral easy muscle contracts in a peristalsis-like manner, which may expel the stone. However, extended isotonic contraction leads finally to elevated manufacturing of lactic acid which irritates the sub-mucosal nerve endings positioned within the higher urinary tract. Pain radiates to , and could be perceived in, any organ with similar innervation such as the gastrointestinal organs and different elements of the genitourinary system (7). Denervation due to kidney transplant surgery makes the event of typical renal colic unlikely. More than 50% of kidney transplant patients with de novo or donor-gifted stones current with no particular symptoms. In animal models of acute unilateral uppertract obstruction, renal pelvic stress and renal blood circulate both improve initially within 1�2 h, doubtless from the elevated stage of prostaglandin E2 (8). Over the following several hours, renal blood flow starts to decline, initially because of efferent arteriolar vasoconstriction. Both renal pelvic strain and renal blood move start to decline, and a progressive discount ensues in glomerular filtration fee, renal plasma flow, and renal oxidative metabolism (8�10). These reductions happen within hours, and reach a nadir by 2 weeks of complete unilateral ureteral occlusion. Although kidney stones have gotten more frequent in women, there continues to be a gender prevalence difference, with a male:feminine ratio of about 2:1. This ratio appears to be consistent with that noticed in different international locations as properly (3). This rising prevalence is of uncertain etiology but could also be attributable to altering dietary practices, increasing prevalence of diabetes and weight problems, migration from cooler rural settings to hotter city settings, and even global warming. These growing prevalence charges are additionally associated with an increase in the value of kidney stone management to an estimated $2. Acute Medical Aspects Related to Kidney Stones Calcium Stones the most common crystal composition of kidney stones is calcium oxalate (11). Calcium phosphate stones should lead to consideration of primary hyperparathyroidism, if serum calcium is on the high end of the normal vary or high; and renal tubular acidosis, in which case, serum bicarbonate focus is low. Uric Acid Stones Uric acid stones happen as the results of low urine pH; hyperuricosuria is much less important as a risk issue (13). Uric acid stones have lately been related to the metabolic syndrome, obesity, and diabetes, all of which result in impaired ammoniagenesis and acid urine (14). The growing prevalence of diabetes and metabolic syndrome, leading to increasing prevalence of uric acid stones, likely contributes to growing kidney stone prevalence. Occasionally the diagnosis of diabetes is first made or suspected when uric acid stones current; measurement of glycosylated hemoglobin could also be appropriate. Struvite stones Struvite stones are composed of "triple phosphate" crystals composed of calcium ammonium magnesium phosphate. Struvite stones are extra common in girls because girls are extra usually affected by urinary tract infections. Cystine Stones Cystinuria is a genetic reason for stones, accounting for 1% of all stones, and as much as 7% of stones in youngsters (16). It is as a outcome of of mutations in two genes liable for expression of the cystine transporter in the nephron. Pathology New concepts in regards to the origins of calcium stones have recently resulted from a sequence of examinations of renal pathology obtained from renal papillary biopsies throughout endoscopic stone management (17). One possible mechanism by which hypercalciuria occurs and causes urinary supersaturation, selling stone formation, is the reduction of proximal tubular calcium reabsorption (18). The etiology of this decreased reabsorption is unclear however has been linked to effects of insulin. Differential Diagnosis Kidney stones are the most frequent explanation for flank ache in an emergency room. A number of different urinary tract and extrarenal causes should also be considered when evaluating a patient with acute flank pain. The the rest, 20�35%, had a non-urinary explanation for pain, such as appendicitis, diverticulitis, unsuspected bowel obstruction, or twisted ovarian cyst. Risk Factors Evaluation of a affected person with attainable kidney stones ought to tackle a number of necessary danger factors. About 40% of sufferers with renal colic in an emergency room have a first degree relative with stones.
Cheap estrace 2 mg
Patients often current hemodynamically unstable with life-threatening injuries that require emergent intervention breast cancer 9 lymph nodes 1 mg estrace with mastercard. The variability of these accidents results in womens health 33511 cheap estrace 2 mg with visa additional uncertainty for surgeons in how to best manage these patients. The airway should be secured shortly and systematically, sufficient respiration and air flow stabilized, life-threatening hemorrhage located and controlled, large-bore intravenous entry obtained for resuscitation, vital indicators measured, and apparent neurologic deficits recognized because the patient is uncovered. This standard major survey in the context of the underlying mechanism of injury helps establish life-threatening injuries and permits fast treatment and hemorrhage control to be effectively initiated. In general, patients who present with hemodynamic instability and shock following a penetrating damage require emergent surgical intervention. Left thoracotomy for management of descending Resuscitative endovascular balloon occlusion of aorta for extreme pelvic and abdominal hemorrhage via left femoral access. In addition, lung parenchymal bleeding can be compressed, air leaks from bronchial injuries controlled, and the pericardium opened to launch any tamponade. This maneuver can be applied to patients with tense hemoperitoneum to control inflow to the stomach. These gadgets permit the affected person to endure both repair of concomitant accidents. Inserting a vascular shunt, although seemingly simple, has the potential to cause harm if not carried out correctly. The steps for shunt placement are well-outlined in Chapter fifty two (Extremity Vascular Trauma). Technically, entry could be gained on the femoral or axillary artery beneath ultrasound guidance or direct cutdown. The 5-Fr sheath is exchanged for a 12-Fr sheath and a 32mm Coda Balloon Catheter (Cook Medical Inc. Exactly how long the balloon can be occlusive with out causing irreversible important organ or neurologic harm is unknown. Up to one-third of patients undergoing surgical exploration for traumatic hemorrhage also require a pulmonary resection due to related parenchymal damage. The first concern is to decide probably the most appropriate incision to use; the second is to determine what process to perform. Whichever method is used, it ought to be versatile enough to tackle potential accidents in adjoining locations together with the neck and stomach. If the damage caused a large pericardial defect, the patient could exsanguinate into the left pleural cavity with an enormous hemothorax. Tamponade could forestall a massive hemothorax and paradoxically produce a short protecting interval. However, if not rapidly corrected, tamponade will trigger cardiac failure and dying. Cardiac harm have to be ruled out in any affected person with a penetrating harm to the "box" area, outlined as the world inferior to the clavicles, superior to the costal margin, and medial to the midclavicular line. Stable sufferers can endure a structured workup, while unstable patients ought to go on to the operating room. Those in cardiac arrest require quick intervention and should benefit from a salvage emergency thoracotomy. The left anterolateral thoracotomy is the incision of alternative for sufferers in extremis. If needed, this incision can be prolonged throughout the sternum right into a clamshell thoracotomy that gives complete publicity of the mediastinum, pericardium, and bilateral thoracic cavities. Atrial accidents may be managed with a vascular clamp and repaired with 4-0 polypropylene suture, while the right ventricle can be digitally managed and repaired with a horizontal mattress suture. Repair sutures must be positioned beneath the coronary vessel, in a horizontal mattress fashion, and tied. However, a proximal coronary artery injury, especially the left anterior descending artery, which is related to severe cardiogenic shock, may require emergent bypass. Mild cardiac dysfunction associated with coronary harm may be managed with an intraaortic balloon pump to provide afterload discount and improved cardiac output in the hope of avoiding an emergent coronary artery bypass. Rarely, a septal defect is created and in such circumstances elective restore is often attainable. This is the most common method for the unstable affected person present process an emergent resuscitative process. It provides rapid entry to the thorax with good exposure to the hilum and avoids the time-consuming positioning related to the standard posterolateral thoracotomy. Limited exposure of the center, complete lung, and posterior mediastinum, particularly the esophagus, are its drawbacks. The inner mammary artery and vein are in shut proximity medially and must be preserved if possible. It supplies glorious exposure of the anterior mediastinum, and both lungs and pleural cavities. In slicing across the sternum, a Lebsche knife, sternal saw, or Gigli saw could additionally be used followed by ligation of the inner mammary vessels bilaterally. It should solely be used if the affected person is hemodynamically stable and the injury is confined to the ipsilateral hemithorax. Singlelung isolation is often desired and obtained by way of placement of either a double-lumen endobronchial tube or bronchial blocker by anesthesia. The normal incision is carried down from the suprasternal notch to the xiphoid course of. The sternal midline is recognized and divided with a sternal noticed; a retractor is positioned after controlling sternal edge bleeding. Some patients arrive with stable hemodynamics and often stay steady throughout their workup. The inner mammary artery should always be inspected to rule out injury as a explanation for hemorrhagic shock. This minimally invasive option eliminates the need for an intensive open surgical procedure together with its associated dangers. Factors in opposition to utilizing an endovascular approach embrace: insufficient proximal or distal landing zones; hemodynamic instability; different injuries in the same region requiring exploration; and vascular occlusion or transection preventing guidewire traversal of the traumatic lesion. A final consideration is the use of an endovascular proximal artery occlusion balloon at the facet of open surgical procedure. This strategy permits speedy proximal hemorrhage management with minimal dissection to facilitate a regular open restore. On the best, distal management of the right widespread carotid artery is supplied by a purple vessel loop, while within the background the right subclavian artery is managed by a red vessel loop. The damage itself is managed instantly with either major restore, patch angioplasty, or interposition grafting. Options for an interposition graft embody prosthetic graft or autologous vein, which is preferred within the setting of a contaminated wound. Patients may be further resuscitated within the intensive care unit and returned to the working room for definitive repair after their physiology has been optimized.
Ava Root (Kava). Estrace.
- How does Kava work?
- Anxiety in women going through menopause.
- Stress, insomnia, restlessness, social anxiety, attention deficit-hyperactivity disorder (ADHD), epilepsy, psychosis, depression, chronic fatigue syndrome (CFS), headaches, colds, respiratory tract infections, tuberculosis, rheumatism, chronic bladder infections, sexually transmitted diseases, menstrual problems, cancer prevention, and other conditions.
- Is Kava effective?
- What is Kava?
- Anxiety.
- Are there safety concerns?
- Dosing considerations for Kava.
- Reducing withdrawal symptoms in people who need to stop taking anti-anxiety and sleep medicines called benzodiazepines.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96842
Discount 2 mg estrace amex
The literature reports mortality rates <5% pregnancy hip pain buy 1 mg estrace free shipping, which could be larger in emergency settings women's health york pa 1 mg estrace order with amex. On physical examination, she was discovered to have a 3-cm pulsatile mass in her right groin and 1+ pedal pulses. Postoperatively, the affected person did properly and was discharged home on postoperative day four. The black arrow points to the aneurysm; notice that the left femoral artery is occluded from a prior tried revision. Given its redo nature, anastomotic aneurysm restore is related to a better incidence of native wound problems than could be expected. Arterial dimensions in the decrease extremities of sufferers with abdominal aortic aneurysms: no indications of a generalized dilating diathesis. The present management of isolated degenerative femoral artery aneurysms is too aggressive for their natural historical past. Anastomotic aneurysms after vascular reconstruction: issues of incidence, etiology, and treatment. The related limb ischemia may be secondary to acute or persistent thrombosis of the aneurysm or secondary to distal embolization of a mural thrombus. Some patients can present with compressive signs if the aneurysm is large sufficient, such as ache or lower extremity edema, or even a deep vein thrombosis. The most feared complication is irreversible leg ischemia because of sudden aneurysm thrombosis or extensive distal embolization, with a major danger of subsequent amputation. Duplex ultrasonography may also be used to evaluate nonvascular plenty of the popliteal fossa and for mapping superficial veins to put together for remedy of the aneurysm. Open surgical repair can traditionally be performed via certainly one of two totally different strategies, a medial or posterior method, each with their own advantages. The aneurysm is bypassed and ligated both proximally and distally to exclude it from the circulation. Geniculate arteries require ligation if they come up from the aneurysmal popliteal section and have the potential to retrograde perfuse the excluded aneurysm sac. Computed tomography angiogram depicting bilateral, partially thrombosed but patent popliteal aneurysms. Posterior strategy 271 For the medial approach, the patient is positioned supine with the leg externally rotated, with a bump positioned under the knee. The popliteal artery is then exposed above and under the knee joint; this is sometimes accomplished through the identical incisions used for vein harvest. Arterial exposure may be troublesome due to arteriomegaly, venous engorgement, kinking, tortuosity, or vessel displacement. A tunnel is then usually created from the above-the-knee to the below-the-knee area between the heads of the gastrocnemius muscle. Careful attention to the anatomy of the gastrocnemius muscle is important to identify and release any attainable entrapment by irregular slips of muscle, if it exists. After controlling the vessels proximally and distally, arterial bypass is carried out in normal trend with a saphenous vein bypass graft from above-the-knee to below-the-knee. The bypass anastomosis could be carried out in either an end-to-end or an end-to-side trend. If the aneurysm is patent, the inflow and outflow arteries to the sac additionally have to be ligated. A completion arteriography, angioscopy, or duplex ultrasonography must be thought of earlier than closure. The medial method is familiar to vascular surgeons due to its similarity to femoropopliteal bypass. This widespread publicity presents a bonus of this strategy over the posterior strategy. The medial strategy additionally offers quick access to the saphenous vein and permits the process to be performed at a distance from the diseased vessel itself, lowering the chance of injury to adjoining constructions. The primary disadvantage of this strategy is that the aneurysm is left intact without decompression. Some surgeons will open the aneurysm sac by way of the aboveor below-knee incision and suture-ligate back-bleeding branches to forestall this complication. The proximal extent of the incision is used to expose the nice saphenous vein, which can be harvested to use as a bypass conduit. The popliteal artery is recognized proximally and uncovered by separating the semimembranosus and semitendinosus muscular tissues medially from the long head of the biceps femoris muscle laterally. Dissection is sustained distally along the artery to avoid injury of the tibial and peroneal nerves coursing laterally and posteriorly to the aneurysm. The bypass may be carried out as an interposition graft with end-to-end anastomosis or as a standard end-to-side bypass. Angiography is initially performed; surgical procedure is performed during the same admission. If the aneurysm is occluded, however a distal outflow vessel is identified on angiography, bypass is carried out as described beforehand. If the limb is immediately threatened, and the patient has sensory and motor dysfunction, emergent thromboembolectomy is carried out. The distal popliteal artery is uncovered and managed below the knee, exposing the area of the trifurcation. An arteriotomy is then made and a Fogarty catheter is handed into all three runoff vessels. After bypass, these sufferers might develop signs of reperfusion harm, like rhabdomyolysis, and so they may require fasciotomy. Those who offered with important limb ischemia solely had a 59% limb salvage rate at 5 years. They additionally found 1-year patency rates to be 96% in sufferers reconstructed with saphenous vein versus 67% for those reconstructed with prosthetic graft. The excellent limb salvage and patency charges are the explanation why aneurysms >2 cm are treated in any affected person who can tolerate open surgical repair. The pain was a relentless, severe, aching ache within the left foot and posterior calf, and started about 2 hours before presentation. Before growing fixed pain, the affected person had been experiencing ache in his left lower leg, even when walking a brief distance. He had a palpable dorsalis pedis and posterior tibial artery pulses in his right decrease extremity, however no palpable pedal pulses in his left decrease extremity. There was a small, firm mass palpated behind his left knee with no palpable popliteal pulse. The affected person was taken urgently to the working room where a left decrease extremity angiogram was carried out. He had a thrombosed popliteal artery with reconstitution of the peroneal and posterior tibial arteries near the ankle.
1 mg estrace order amex
There has been some interest in the literature about allowing use in the hospitalized pediatric population menstruation 3 times in one month 1 mg estrace with amex, but no information on security of the units on this population is out there (28) women's health magazine running tips 1 mg estrace purchase fast delivery. A key think about minimizing errors and adverse occasions in these conditions is a collaborative relationship between the patient and hospital employees. In addition, because of the continual advances in diabetes units and applied sciences, enough ongoing education of all key stakeholders about insulin pumps and other evolving tools is warranted. Management of Insulin Pumps in Hospitalized Patients Hospitalizations for folks with Type 1 and Type 2 diabetes in contrast with the nondiabetic inhabitants of Tayside, Scotland: a retrospective cohort examine of useful resource use. Patients with kind 2 diabetes had greater charges of hospitalization than the general inhabitants. Use of continuous subcutaneous insulin infusion (insulin pump) therapy within the hospital setting: proposed pointers and outcome measures. Current views on the use of steady subcutaneous insulin infusion within the acute care setting and overview of therapy. Continuous subcutaneous insulin infusion (insulin pump) therapy may be safely used within the hospital in select sufferers. Outpatient to inpatient transition of insulin pump remedy: successes and persevering with challenges. Insulin pump patient traits and glucose management within the hospitalized setting. Society for Ambulatory Anesthesia consensus statement on perioperative blood glucose management in diabetic patients undergoing ambulatory surgical procedure. Comparison of insulin pump remedy (continuous subcutaneous insulin infusion) to alternative methods for perioperative B. Experiences of continuous subcutaneous insulin infusion in pregnant ladies with type 1 diabetes throughout supply from four Italian centers: a retrospective observational examine. Cultivating high quality: a program to practice inpatient pediatric nurses in insulin pump use. Continuous subcutaneous insulin infusion providing better glycemic management and high quality of life in Type 2 diabetic topics hospitalized for marked hyperglycemia. Continuous infusion of subcutaneous in comparability with intravenous insulin for tight glycaemic management in medical intensive care unit patients. Management of Diabetes and/or Hyperglycemia during Enteral and Parenteral Nutrition Aidar R. The development of hyperglycemia during vitamin help is associated with elevated threat of issues and mortality. Insulin therapy ought to be considered for blood glucose more than a hundred and eighty mg/dL (10 mmol/L). Introduction Malnutrition, widespread in hospitalized patients, is related to longer length of stay, poorer outcomes and survival, and increased price of care. In general, the dietary assessment, indications for vitamin assist, and estimate of nutrition requirements for critically ill sufferers with hyperglycemia are just like those of nondiabetic sufferers (1). Studies which have demonstrated a helpful affect of dietary help on clinical outcome have supplied diet for a minimal of 1 week. Metabolic derangements in electrolytes, minerals (especially hypophosphatemia), and water-soluble vitamins are widespread and may be delicate or extreme. Organ compromise can manifest as pulmonary, cardiac, neuromuscular, and hematologic complications. Appropriate monitoring includes day by day weight, fluid balance, and indicators of oedema till steady. Levels of serum potassium, phosphorus, and magnesium ought to be measured daily, and any deficiencies changed. Hyperglycemia is regularly noticed in hospitalized patients receiving specialised nutritional support. The glycemic strategies also needs to follow widespread sense in selecting acceptable therapeutic approaches that not solely control hyperglycemia but additionally have low hypoglycemia risk. Common causes of hyperglycemia in hospitalized patients include insufficient insulin dosing, overfeeding, medications, as properly as stress, irritation, and infection. In addition, extreme delivery of glucose and gluconeogenic substrates by way of the enteral or parenteral route in hospitalized sufferers also can contribute to hyperglycemia. In basic, diabetic sufferers experiencing inpatient hyperglycemia are at larger danger of complications and mortality (3), although evidence is missing if interventions designed to reduce hyperglycemia do improve medical outcomes, at least in non-critically ill sufferers (4). This is particularly necessary for sufferers with type 1 diabetes mellitus who should proceed a minimal of basal insulin remedy. Standard enteral formulation include 1� 2 cal/ml and, in general, consist of protein, lipid in the form of long-chain triglycerides, and carbohydrates. Current proof and opinions within the field argue for delayed and permissive underfeeding. Often, continuous feeding is utilized in critically sick sufferers and intermittent (gravity) feeding is used in medically stable patients. By distinction, jejunal feeding ought to at all times be continuous (nocturnal or 24-hour infusion). The format of the feeding routine has a serious impact on the design of insulin management applications. Increases in the tube feeding infusion price should be averted until adequate glucose control has been achieved by acceptable insulin management. For sufferers with hyperglycemia without prior analysis of diabetes and no prior use of insulin or oral diabetic brokers, initially suggest remedy with short-acting insulin until tube feeding is nicely tolerated. Once the tube feeding infusion fee has reached 30�40 ml/hr, using intermediate-acting insulin is usually protected. Although some sufferers receiving gravity feedings may be managed with a couple of times daily intermediate-acting insulin alone, others will need combined intermediate and short-acting insulin remedy. Most sufferers will require only a once-daily administration of intermediate-acting insulin (alone or mixed with a short-acting insulin preparation) previous to the onset of tube feeding. Continuous feeding over 24 hours: Scheduled administration of intermediate-acting insulin, usually given every 8 hours, could also be required. If the feeding tube is removed or dislodged, the potential for prolonged hypoglycemia is larger if long-acting insulin is used. Also, reliance on intermediate insulin requires a extra frequent dose-adjustment than use of long-acting insulin, ensuing in the potential for more speedy achievement of glucose management. For sufferers on tube feeding, the commonest explanation for hypoglycemia is unexpected discontinuation of tube feedings. The incidence of hypoglycemia reported in these retrospective studies diversified between zero. The rationale for the conservative method to insulin intensification in these sufferers is justified by the fact that it might take several days to obtain the desired vitamin objectives due to the potential gastrointestinal intolerance during early optimization of enteral feeding. Significant diabetic gastroparesis is commonly present in sufferers with long-standing kind 1 diabetes. Demonstration of delayed gastric emptying establishes the prognosis of gastroparesis. Accurate analysis of diabetic gastroparesis is important, because it avoids the faulty attribution of gastrointestinal signs to tube feeding or to different factors capable of slowing intestine motility. Most sufferers with diabetic gastroparesis intolerant of gastric feedings are able to tolerate isoosmolar jejunal tube feedings when initiated at a low price and advanced slowly.
2 mg estrace generic mastercard
Case research A 35-year-old man women's health garcinia cambogia generic estrace 2 mg visa, who was beforehand in good well being menstrual ovulation calculator cheap 1 mg estrace fast delivery, was admitted to the intensive care unit after a motor vehicle accident, throughout which he suffered extreme head damage with loss of consciousness, necessitating intubation. On the third hospital day, the patient was found to be hyponatremic (serum sodium: 129 mmol/L [normal, 135�145], urine sodium: 60 mmol/L and urine osmolality: 450 mOsm/kg). Hyponatremia resolved inside two days after the institution of glucocorticoid alternative in stress doses, confirming the central function of glucocorticoid deficiency within the pathogenesis of hyponatremia in this patient. Hypopituitarism Conclusions Hypopituitarism is attributable to all kinds of pathologies affecting the hypothalamic pituitary unit. Prompt establishment of glucocorticoid substitute and careful attention to fluid and electrolyte steadiness could be lifesaving in acutely sick sufferers. Despite substantial advances in the analysis and administration of pituitary issues, hypopituitarism stays a severe condition and has been associated with extra mortality, because of inadequately handled hypoadrenalism, long-term excess threat of cardiovascular and cerebrovascular illness, and probably increased threat of malignancy in irradiated sufferers (2. Further enhancements in the accuracy of diagnostic testing and replacement therapies are wanted so as to enhance the long-term outlook of these patients. Deaths among grownup patients with hypopituitarism: hypocortisolism throughout acute stress, and de novo malignant mind tumors contribute to an increased mortality. Hypophysitis secondary to cytotoxic T-lymphocyte-associated protein 4 blockade: insights into pathogenesis from an autopsy series. Hypopituitarism and central diabetes insipidus: perioperative diagnosis and Management. Ipilimumab-induced hypophysitis: an in depth longitudinal analysis in a large cohort of patients with metastatic melanoma. Clinical evaluation: current state and future perspectives in the prognosis of diabetes insipidus. Hormonal substitute in hypopituitarism in adults: an Endocrine Society Clinical Practice Guideline. Pituitary dysfunction following traumatic mind injury or subarachnoid haemorrhage: endocrine administration in the intensive care unit. Factors predicting postoperative hyponatremia and efficacy of hyponatremia management methods after more than one thousand pituitary operations. Improved cortisol exposure-time profile and consequence in patients with adrenal insufficiency: a prospective randomized trial of a novel hydrocortisone dual-release formulation. Evaluation and treatment of grownup growth hormone deficiency: an Endocrine Society Clinical Practice Guideline. Hypothalamic/pituitary perform following high-dose conformal radiotherapy to the base of cranium: demonstration of a dose-effect relationship using dose-volume histogram analysis. American Association of Clinical Endocrinologists and American College of Endocrinology. Disease state scientific evaluation: a neuroendocrine strategy to sufferers with traumatic mind injury. Disease state clinical evaluation: update on progress hormone stimulation testing and proposed revised cut-point for the glucagon stimulation test in the analysis of adult progress hormone deficiency. Signs of meningeal irritation or altered consciousness might complicate the prognosis. Corticotropic deficiency with adrenal insufficiency may be life threatening if left untreated. Nowadays, conservative management is more and more utilized in selected patients (those without necessary visual acuity or area defects and with regular consciousness), as successive publications present converging proof that a "wait-and-see" method provides similar outcomes by means of oculomotor palsy, pituitary perform, and subsequent tumor growth. Headache of sudden and extreme onset is the main symptom, generally related to visible disturbances or ocular palsy. Between 2% and 12% of patients with all kinds of pituitary adenoma expertise apoplexy, and the prognosis of pituitary adenoma was unknown at time of apoplexy. The vascularization of adenoma is predominantly supported by the direct arterial blood supply quite than portal system for the conventional pituitary gland. Pituitary adenomas are 5 times more susceptible than other intracranial tumors to bleed and bear infarction and necrosis, presumably as a outcome of the pituitary gland has an distinctive rich vascular structure or as a end result of pituitary tumors might outgrow their blood provide or as a end result of ischemia (and thus infarction) occur following compression of infundibular or superior hypophyseal vessels towards the sellar diaphragm by the increasing tumor mass with intrinsically poor vascularity. Clinical Presentation Headache is the most outstanding symptom of acute apoplexy and is present in more than 80% of patients (18,19). Headache can be typically the preliminary symptom, with sudden and extreme onset described "like a thunderclap in a transparent sky" (20). It is usually related to vomiting and nausea and may mimic migraine or meningitis (21). Middle row: At 24 hours: T1W sequences present peripheral and central areas of spontaneous sign hyperintensity (top), while T2W sequences show mainly central hypointense areas (bottom); observe also the typical thickening of the sphenoid sinus mucosa on both T1W and T2W sequences (arrows). Right row: At 36 hours: T1W (top) and T2W (bottom) sequences show a rise in the hyperintense and hypointense areas (asterisk) and further thickening of the sphenoid sinus mucosa (arrows). Variable degrees of visual-field impairment may be observed, bitemporal hemianopsia being most typical. Signs or signs of meningeal irritation, fever, and discount of the extent of consciousness not often happen (25). Endocrine Dysfunction Acute endocrine dysfunction may be present, additional complicating the medical image. By revealing a pituitary tumor, even when no necrosis or hemorrhage is discovered, these imaging strategies provide confident diagnostic affirmation. This explains why imaging hardly ever reveals pure hemorrhage or infarction however somewhat blended features. It is also the most life-threatening hormonal complication, doubtlessly inflicting extreme hemodynamic problems and hyponatremia (27,28). After administration of distinction medium, the pituitary tumor shows inhomogeneous enhancement, occasionally with ring enhancement (3). Discrete hypodensity of a pituitary mass and thinning of the sellar flooring (white arrow). In the very first hours after onset, frank hyperintensity on T1W could additionally be absent, either due to infarction or as a outcome of the hemorrhage is still in the type of deoxyhemoglobin (31). It is generally used to detect deposits of hemosiderin even later after a hemorrhagic event. A histological examine confirmed that the subepithelial layer of the sphenoid sinus mucosa was markedly swollen. Histological features may be necessary for prognostication: easy tumor infarction alone tends to produce much less extreme clinical features at presentation and have a better outcome than hemorrhagic infarction or frank hemorrhage (38). Recovery of neurological, ophthalmological, and endocrine operate is very variable. If altered consciousness improves after decompression, altered visible fields and acuity additionally are inclined to improve, but permanent visible sequelae may happen, notably in case of optical nerve atrophy. The treatment goals are to enhance symptoms and relieve compression of native constructions, particularly the optic pathways. Much of this, nevertheless, is secondary to injury to the normal gland from the initial apoplectic event. Conservative Approach Reports of spontaneous medical improvement and shrinkage (or disappearance) of apoplectic pituitary adenomas suggest that a conservative approach may be appropriate in selected cases.
Estrace 2 mg order otc
The redundant aneurysm sac is sutured over the aortic prosthesis within the abdomen and chest women's health xmas kekse 1 mg estrace generic mastercard. As the left kidney is returned to its anatomic position breast cancer mortality rate estrace 1 mg purchase otc, the perinephric fats usually suffices to provide sufficient protection of the aortic graft within the region of the visceral aortic section. A single pleural tube is placed and a closed suction drain could additionally be left within the retroperitoneum if hemostasis is in query. Renal failure Minimizing renal ischemic occasions, utilizing chilly perfusate, avoiding intraoperative hypotension, and treating stenotic lesions aggressively with both bypass or open stent placement scale back renal harm. The creator reserves dialysis for particular medical indications like quantity overload, hyperkalemia, or acidosis. When wanted, steady venovenous hemodialysis is preferred because it offers for a smoother hemodynamic course than typical hemodialysis. Preoperative renal insufficiency is essentially the most powerful predictor of postoperative renal failure; postoperative renal dysfunction negatively impacts short- and long-term survival. Indeed, if strict standards are used, some 40% of sufferers endure a respiratory complication. Contributing elements include paralysis of the left hemidiaphragm and pain from the extensive chest wall incision that impedes pulmonary hygiene. For sufferers who fail extubation, the creator favors early placement of a tracheostomy (required in <10% of patients). Postoperative care Postoperatively, patients should be monitored in an intensive care unit setting. Oxygen supply is essential in the early section of restoration and the creator rarely extubates sufferers within the early postoperative interval. It is important to monitor the hematocrit for signs of ongoing bleeding and all coagulation issues ought to be aggressively corrected. Most late aortic events are the results of native aneurysmal disease in distant (or noncontiguous) aortic segments. Several reports have emerged validating that almost all operative survivors return to their preoperative impartial residing standing. Contemporary management of descending thoracic and thoracoabdominal aortic aneurysms: endovascular versus open. In addition, late aortic events happen in about 10% of patients, but few of those are graft-related. The aortic wall is 3�4 instances thicker and more inflexible than degenerative aneurysms, and the inflammatory process is limited to the anterior and lateral aortic wall. These options improve the incidence of damage to each vascular and visceral retroperitoneal structures during aneurysm restore. As a outcome, the special issues within the open reconstruction for inflammatory aortic aneurysms are still worthy of examine and evaluation for each vascular surgeons and trainees. The chance of those technical difficulties will increase as the extent of the aneurysm and measurement of the inflammatory mass enhance. Inflammatory aortic aneurysms occur at a younger age, have a stronger familial tendency, and happen extra predominantly in males compared to noninflammatory aneurysms. The majority are symptomatic at presentation with stomach or back pain, weight reduction, and elevated erythrocyte sedimentation fee as frequent scientific findings. The analysis is made preoperatively with 90% sensitivity using computed tomography angiography or magnetic resonance angiography. Inflammatory aortic aneurysms are normally isolated to the infrarenal phase of the abdominal aorta. The anterior, through a midline celiotomy utilizing a xipho-pubic incision, affords particular advantages in treating aneurysmal and occlusive illness. The lateral approach may be from a thoracoabdominal incision involving two physique cavities or a direct left lateral approach from a flank incision with the affected person turned in a 90-degree place. The anterior method provides the benefit of ease and facility in addressing the aorta and its branches from the renal artery stage to past the femoral bifurcation in these with juxtarenal or infrarenal aortic aneurysms. Operating room preparation is simpler and easily reproducible for emergent procedures. Fluorescent ureteral stents are placed before skin incision to stop injury in the occasion of ureteral adhesion to the inflammatory aneurysm. A midline incision that extends from the xiphoid course of to simply above the pubis creates the space required to safely expose the proximal aorta at the renal and mesenteric degree all the means down to the iliac bifurcations. For added exposure, the xiphoid course of may be resected and the pores and skin incision carried additional cephalad. As the exposure is created, shallow blades are transitioned to longer blades for retraction of the posterior peritoneal tissues, the abdominal wall, and the decrease chest wall. The retractor system have to be correctly positioned to obtain lateral and superior retraction of the higher abdominal cavity. The hinge lock mechanism and arms are elevated 15�20 cm above the horizontal floor of the chest and abdomen. This permits the drive vector generated by the retractors to be at a 45-degree angle from the horizontal aircraft of the anterior belly wall directed upward and outward. After the stomach has been opened, the nasogastric tube placement has been confirmed, and the stomach has been explored, the falciform ligament is taken down between heavy ties. This is followed by division of the triangular ligament towards the dome of the diaphragm. The mid-transverse colon and splenic flexure are pulled up and over the stomach and positioned under the diaphragm with dry laparotomy pads. In the setting of an inflammatory aneurysm, the duodenum is mostly adherent to the anterior proper lateral aneurysm wall. This section ought to be left undisturbed till the proximal dissection is full. The ligament of Treitz is mobilized completely earlier than finishing the complete size of the posterior retroperitoneal incision. The duodenum adherent to the aneurysm is allowed to escape the enclosed towel; the remaining duodenum and small bowel are held. The long retractor blades are superior deeper and the posterior peritoneal constructions are hooked by the blades and retracted to the proper and left. Operative management 231 the upper abdominal wall and lower rib cage are unfold extensively aside. Proximally, a transverse posterior peritoneal incision is made at the base of the pancreas in the avascular plain perpendicular to the longitudinal incision over the aneurysm. A Harrington blade is placed in the midline over the central mesenteric root for proximal mild retraction of the body of the pancreas. The branches are taken down sequentially between 3-0 silk ties, to embody the adrenal vein, accent renal branches, and the lumbar-renal vein. A renal vein retractor may be positioned anterior to the pararenal aorta to retract the vein superiorly by several centimeters.