
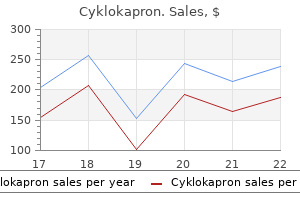
Cyklokapron dosages: 500 mg
Cyklokapron packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Buy cyklokapron 500 mg visa
There is nothing attribute within the radiologic or histologic findings of the first lesion treatment under eye bags cyklokapron 500 mg safe, including the presence of blood vessel invasion that can reliably predict the development of pulmonary implants in a affected person with typical giant cell tumor treatment 5th finger fracture cyklokapron 500 mg cheap without prescription. There is usually no recurrence after easy curettage, and it can be managed by systemic remedy with steroids. Ancestors of those families have been traced to the southern Italian city of Avellino in the Campania area. B, Higher magnification of A exhibiting typical (nonmalignant) cytoarchitectural options of large cell tumor in pulmonary implant. C, Formation of reactive osteoid associated with pulmonary implants of standard big cell tumor. D, Pulmonary implant of large cell tumor delineated by a reactive shell of bone and peripheral scarring. B and C, Higher magnification of A showing nicely defined nodules of standard giant cell tumor with peripheral scarring in lung. D, Small (miliary) implant of conventional giant cell tumor in subpleural lung related to distinguished reactive bone forming an incomplete peripheral shell. E, Higher magnification of D exhibits a pulmonary implant predominantly composed of mononuclear cells with distinguished reactive bone. A and B, Pulmonary implants of typical giant cell tumor with outstanding reactive bone. C and D, Higher magnifications of A and B showing prominent interconnecting bone trabeculae. The tumor is composed predominantly of mononuclear histiocytic cells with stromal fibrosis obscuring, along with reactive bone, the classic microscopic architecture of giant cell tumor. C, Oblique view of thoracic backbone with partial collapse of bodies of T5 and T6 at web site of giant cell tumor (arrows). D, T1-weighted sagittal magnetic resonance picture reveals tumor (arrows) with low sign compressing dural sac. Note mosaic sample of cement lines, in addition to outstanding osteoclastic resorption and osteoblastic rimming. C, Electron micrograph of nucleus of large cell containing viruslike filamentous inclusion. D, Higher magnification of filamentous inclusion physique resembling paramyxovirus particles. Inset, Inclusions could be identified by light microscopy as eosinophilic our bodies inside giant cell nuclei. They resemble paramyxovirus inclusions, but the precise nature of these structures stays to be determined. In such cases, an examination of extra biopsy materials may be required to solve this diagnostic dilemma. Occasionally, a florid reactive proliferation of fibroblasts with high mitotic activity might mimic fibrosarcoma. In such instances, attention must be directed towards the gradual blending of such suspicious areas with clearly benign reactive tissue to avoid a false diagnosis of sarcomatous change. However, reactive bone is almost at all times present at the periphery of the lesion and at times can prolong inside it for a substantial distance. The diagnosis of osteosarcoma complicating a conventional giant cell tumor requires the presence of a malignant bone-forming tumor. Secondary Malignant Giant Cell Tumor Malignant change usually occurs after multiple native recurrences of a traditional large cell tumor. Sarcomatous change is extra likely to occur in a beforehand irradiated lesion, often 5 years or extra after the preliminary radiation exposure. Sarcomatous change also can develop a few years and even a long time after removal of the primary lesion. However, these features are incessantly observed in a locally superior typical large cell tumor. In extraordinarily rare circumstances, a phenotypic change to epithelial malignancy with squamous differentiation has been reported. Reactive bone can be current focally and must be appropriately identified as not being an integral a part of the lesion. There is excessive mitotic activity of each stromal and tumor large cells, with multiple atypical mitoses current. In reference to focal adjustments, it may be troublesome in some cases to distinguish between main malignant large cell tumor and secondary malignant change in a conventional large cell tumor. In cases with outstanding atypia and quite a few atypical mitoses, the analysis of malignancy is straightforward. The diploma of biologic aggressiveness will increase as stromal cells become more prominent and show an increase in mitotic activity. Grade 1 corresponds to a standard, microscopically benign large cell tumor, and grade three is Text continued on p. A, Anteroposterior radiograph of a recurrent giant cell tumor presenting as a big expansile lesion, which destroyed the cortex of distal femoral epiphysis. B, Microscopic features of the tumor in A displaying a conventional element of this giant cell tumor. C and D, High-grade undifferentiated sarcomatoid component of the lesion proven in A and B with pronounced atypia and brisk mitotic activity (B-D, �200. A, A part of the tumor exhibiting cytoarchitectural features according to a conventional big cell tumor. B, Higher magnification of A exhibiting mononuclear histiocytic cells and scattered multinucleated large cells. C, Sarcomatoid part of the tumor exhibiting proliferation of atypical spindle cells. D, Higher magnification of C showing disorganized proliferation of undifferentiated sarcomatoid cells with pronounced atypia. B, Computed tomogram of lesion in A exhibits eccentric, sharply demarcated defect with focally destroyed cortex. C and D, Areas of typical osteosarcoma with outstanding tumor osteoid have been current in addition to standard big cell tumor. A, A element of the tumor with options resembling typical big cell tumor. B, Sarcomatoid part of the tumor composed of undifferentiated mesenchymal cells in confluent growth. C, Higher magnification of B exhibiting sarcomatoid plump, spindle, and oval undifferentiated mesenchymal cells. B, Higher magnification of A showing pronounced atypia and mitotic activity in sarcomatoid cells. C, Undifferentiated sarcomatoid cells with pronounced atypia and focal clear cell change in one other area of the tumor proven in A and B. D, Higher magnification of C showing pronounced atypia and focal clearing of the cytoplasm in sarcomatoid cells.
Ceanothus intermedius (New Jersey Tea). Cyklokapron.
- Dosing considerations for New Jersey Tea.
- Cough, spasms, bleeding, gonorrhea, syphilis, colds, fever, chills, and other conditions.
- How does New Jersey Tea work?
- What is New Jersey Tea?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96575
Cyklokapron 500 mg discount free shipping
The incision is transmural and is taken into account enough when periureteral fats is visualized endoscopically medicine net 500 mg cyklokapron sale. The benefits of endopyelotomy are these inherent in minimally invasive surgical procedures medicine q10 generic cyklokapron 500 mg without prescription, including decreased cost, shortened hospitalization, and shortened recuperative interval. In addition, the effectiveness of endopyelotomy as a remedy for major ureteral strictures is comparable to that of open surgical procedures. Finally, endopyelotomy has a bonus over open surgery in the remedy of secondary strictures, for which follow-up open surgical procedures are complicated and less commonly end in adequate resolution of strictures. Other endoscopic procedures which are less generally carried out embody transrenal inspection and biopsy of the renal amassing system and the ureter. This is mostly performed in patients with filling defects or strictures when the underlying tissue prognosis is unknown. Endoscopic procedures could be performed as a substitute for open surgical inspection or surgical procedures for biopsy access. A transrenal approach is seldom used for this software because most ureteral and pyelocalyceal lesions may be reached in a retrograde trend with a flexible ureteroscope, thus avoiding the need to create a transrenal tract. The only absolute contraindication for this process is an uncorrected coagulopathy. In addition, if rigid nephroscopy is deliberate, large-bore tract creation is topic to length limitations. Most normal rigid endoscopes have a working length of 20 cm or much less, which is barely longer than the standard nephrostomy sheaths provided by manufacturers. This tube should be left in place for no less than 7 days before making an attempt transrenal endoscopy with no nephroscopic sheath. Because many sufferers with a large stone burden will harbor infection-based stones, antibiotic prophylaxis is essential. Again, a posterior calyx must be chosen for transrenal puncture and tract creation. As entry to a certain area throughout the pyelocalyceal system or the ureter is desired, site choice for puncture is essential. For nephrostolithotomy, an upper-pole calyx usually permits for endoscopic entry to the largest segment of the intrarenal amassing system. To minimize problems, transrenal puncture should be performed under the 12th rib when possible. For the upper pole, puncturing between the eleventh and twelfth ribs is often required and should be considered protected. Because the pleural reflection commonly extends to the eleventh rib or lower, puncturing above the eleventh rib ought to be averted due to the high risk of transpleural tract passage and ensuing pleural effusion, hemothorax, empyema, or presumably pneumothorax. However, after placement of a heavy-duty guidewire and a security guidewire, the tract is dilated to 9 F with a fascial dilator. The subsequent dilatation could be carried out with a high-pressure balloon dilatation catheter. The inflated diameter ought to be 10 mm, and the balloon size must be 10 to 12 cm. B, Following needle puncture of a lower-pole calyx, this film demonstrates development of the guidewire into the renal pelvis, around the stone. C, Following catheter manipulation to steer the tip of the guidewire into the ureter, a fascial dilator (arrow) is superior over the guidewire to dilate the tract before passing the balloon dilatation catheter. Using the balloon dilator the tract may be quickly dilated from eight to 30 F with a single inflation. This radiograph also demonstrates a second safety guidewire via the nephrostomy tract, which was positioned as a precaution. After dilatation of the tract, the balloon catheter is eliminated and placement of a 10-mm sheathed dilator is attempted. If balloon dilatation incompletely dilates the whole tract, smaller semirigid fascial dilators may be used to dilate the tract steadily to the utmost diameter of 10 mm. The sheathed dilator can then be placed over the guidewire, the dilator removed, and the guidewires and nephroscopy sheath left in place. Endoscopy may be carried out through this sheath instantly, or a drainage catheter can be handed via the sheath if endoscopy is deferred. Placing a security catheter over the protection guidewire is advisable after placement of a large-bore drainage catheter. A commonplace 5-F angiographic catheter can serve as a security catheter; it ought to be advanced over the safety wire in order that its tip is in a steady place, ideally inside the bladder. At the tip of the procedure each nephrostomy catheters must be sutured to the skin and the large-bore tube must be left to external drainage to allow for outflow of urine and residual blood clot. The affected person should be visited day by day for a minimum of three days, if hospitalized, to guarantee tube perform and to identify potential nephrostomy issues early. Hematuria routinely lasts so long as 72 hours, however hematocrit ranges ought to be monitored if hematuria is extreme. With meticulous and thorough endoscopic techniques, stone-free rates of 85% or higher could be achieved with percutaneous nephrolithotomy. In cases involving complex-shaped stones, multiple transrenal nephrostomy tracts could additionally be required to attain fragments clustered in isolated segments of the kidney. These infusion methods make the most of an influx and outflow catheter for the infusion of agents that bathe and slowly dissolve the residual stone fragments. In addition, preoperative identification of anomalous vessels could affect a surgeon to choose open surgical stricture repair rather than endopyelotomy. The identification of aberrant vessels of great dimension (4 mm in diameter) implies a substantial danger of large bleeding if the vessel is inadvertently incised during endopyelotomy. Once targeted, the stone is treated with repeated shock-wave bursts generated extracorporeally however focused internally on the stone. The stone fragments typically pass spontaneously in an antegrade fashion with voided urine. This coalescence of fragments is described as a stein strasse, translated as stone avenue. Rarely, extra complex interventions are required to deal with these obstructing stone casts. These interventions embody ureteral dilatation, stone flushing, or long-term ureteral stenting. Complete dialogue of those methods is beyond the scope of this chapter, however the essential components shall be described. B, Intraoperative radiograph following creation of a large-bore percutaneous tract with a sheath in place. C, Nephrostogram carried out 6 weeks following endopyelotomy demonstrating marked lower in the renal pelvic dilatation in comparability to the preoperative look.
Order cyklokapron 500 mg free shipping
In typical circumstances medications emt can administer buy cyklokapron 500 mg free shipping, the distinctive morphologic traits of well-developed small glands of prostate carcinoma are easy to acknowledge in metastases treatment guidelines 500 mg cyklokapron buy overnight delivery. The small cell carcinomas of the prostate are microscopically indistinguishable from other small cell carcinomas, such as those of lung origin. In such circumstances, the metastatic foci predominantly consist of sclerotic bone with scattered small clusters of tumor cells. It is postulated that prostate carcinoma stimulates new bone production by secretion of a number of ubiquitous kinins and pro-osteoblastic factors that drive osteoblast differentiation and bone formation. In such circumstances, documentation of the epithelial nature of those cells with epithelial markers such as cytokeratin can assist the diagnosis. In addition to radiotherapy and bisphosphonates, a selection of radiopharmaceuticals have lately been identified to specifically treat prostate carcinoma bone metastases by homing in on bone lesions whereas limiting native toxicity, thus providing each palliative and survival advantages. Cytologic preparations from properly or moderately differentiated prostate most cancers might contain recognizable microglandular structures that resemble small rosettelike formations with nuclei on the periphery and a middle shaped by amorphous cytoplasmic materials. Carcinoma of the Kidney Renal cell carcinoma is a prototype of a tumor that regularly presents as a skeletal (often solitary) metastasis with a clinically occult primary tumor. Note that nuclei of tumor cells are uniform in dimension and show solely minimal atypia. Inset, Higher magnification of tumor cells showing particulars of nuclear morphology, which comprise distinguished nucleoli and evenly distributed chromatin. C and D, Metastatic clear cell carcinoma of the kidney shows loosely organized clusters of tumor cells with ill-defined clear and finely granular cytoplasm. Note gentle atypia of tumor cells characterized by the presence of spherical to oval nuclei with clearly visible nucleoli (A-D, �400; Inset A, �600; Inset D, �400) (A-D and insets, hematoxylin-eosin. Renal cell carcinomas are known to metastasize to uncommon distant websites such because the pores and skin, tongue, eye, heart muscle, acral skeleton, and breast. Renal cell carcinomas preferentially metastasize to the femur, humerus, pelvis, and spine; though osteoblastic lesions have been described,128 the vast majority are lytic. Approximately 10% of renal cell carcinomas dedifferentiate into high-grade spindle-cell or pleomorphic sarcomatoid carcinoma. Some of those lesions can have features suggesting an undifferentiated spindle-cell or pleomorphic sarcoma, and may be misdiagnosed as primary bone lesions. Review of medical knowledge and identification of the epithelial nature of cells with appropriate immunohistochemical markers are useful for classifying the lesion as a metastasis. Cytologic preparations from the metastatic sarcomatoid variant of renal cell carcinoma present malignant spindle and pleomorphic cells organized in massive sheets, small clusters, or singly that might be very deceptive. Nuclei present pronounced atypia characterised by irregular chromatin clumping and distinguished nucleoli. In general, the cytologic options of metastatic sarcomatoid carcinoma are indistinguishable from these of primary malignant fibrous tumors of bone. Immunohistochemical stains for keratin and vimentin, combined with a scientific history of major renal carcinoma, are helpful to set up the correct prognosis. Welldifferentiated thyroid carcinoma can current clinically as skeletal metastases (either solitary or a number of lesions) with an occult major tumor. Thyroid carcinomas that affect younger people and youngsters are extra aggressive and have a higher propensity to metastasize to the skeleton and lungs, though age higher than 55 years is a powerful predictor of dying following disseminated illness. Aspirates from metastatic thyroid follicular carcinoma show a uniform population of small cells lying singly in three-dimensional clusters, typically forming follicles with central colloid. Intranuclear cytoplasmic inclusions and nuclear "creases" are commonly seen in the spherical nuclei. Colloid can be seen as an amorphous substance dispersed in a background of the smear or could be present inside the core follicles. Cytologic features of metastatic thyroid follicular cell carcinoma are very distinctive and allow the identification of thyroid origin in the majority of instances. Carcinoma of the Pancreas Carcinoma of the pancreas is understood for its poor prognosis. The lesion is low signal depth on T1-weighted pictures (A) and high-signal depth on T2-weighted pictures (B). C, An axial computed tomography scan exhibits the massive lesion in the proper ilium in addition to a second lesion close to the left sacroiliac joint. A, Anteroposterior radiograph shows a solitary lytic lesion within the proximal humeral diaphysis. B, Radioisotope scan shows a solitary focus of uptake similar to the lesion seen in A. C and D, Microscopically, the lesion consists of nests of clear cells with intervening nice capillaries, typical of renal cell carcinoma (C, �100; D, �400) (C and D, hematoxylin-eosin). C, Gross photograph of bisected rib reveals intramedullary gray-tan lesion with cortical disruption. D, Photomicrograph reveals attribute follicular progress pattern with colloid of metastatic follicular variant of papillary carcinoma of thyroid. A and B, Low power photomicrographs present a predominantly spindle-cell neoplasm with abundant collagenous stroma, interpreted on limited needle biopsy as undifferentiated carcinoma. C, the sarcomatoid part adjoining to a focus with overt epithelial differentiation. D, the epithelial element resembles the follicular variant of papillary carcinoma. Melanoma most commonly metastasizes to regional lymph nodes, but skeletal metastases also occur, most often involving axial websites such because the ribs, jaw, pelvis, and backbone; appendicular metastases are encountered less incessantly. Tumor cells can differ from epithelioid to spindled in look, and should or might not include melanin pigment. In the setting of an unknown major tumor, metastatic melanoma must be distinguished from poorly differentiated carcinoma; amelanotic tumors may be mistaken for poorly differentiated carcinoma or even sarcomas when predominately spindled in appearance. Patients with appendicular metastases seem to have barely better survival than these with axial metastases, owing in part to a shorter interval to metastasis for the axial lesions. In addition, they more often involve the appendicular skeleton in contrast with the axial skeletal involvement seen in adults. Rhabdomyosarcoma, neuroblastoma, and clear cell sarcoma of the kidney are the three most notable examples of pediatric malignancies which have a very high propensity for metastasizing to the skeleton, a characteristic that represents an integral part of the clinical conduct of these tumors. Rhabdomyosarcoma Rhabdomyosarcoma can be categorized into a quantity of completely different subtypes. Embryonal and alveolar rhabdomyosarcoma are seen primarily in the pediatric inhabitants, whereas pleomorphic rhabdomyosarcoma, a comparatively rare tumor, happens primarily within the grownup population. One subtype of embryonal rhabdomyosarcoma that affects adolescents and is more incessantly located in the spermatic wire is the spindlecell variant. Overall, the head and neck region, genitourinary organs, and soft tissue of the extremities are probably the most incessantly affected websites. The alveolar variant of rhabdomyosarcoma, which extra generally arises in the extremities, has a poorer prognosis than both embryonal rhabdomyosarcoma or fusion-negative alveolar rhabdomyosarcomas193 (see below).
Cyklokapron 500 mg purchase on line
D medicine 44-527 cyklokapron 500 mg buy lowest price, Computed tomogram shows well-circumscribed lytic tumor containing foci of mineralized bone matrix in base of pedicle medicine 8 letters generic 500 mg cyklokapron visa, lamina, and body. A, Nineteen-year-old man who reported pain at site of previously extracted decrease tooth. Well-circumscribed radiolucent area with central opacity represents benign bone-forming tumor. B, Bone-forming mass with ill defined punctuated mineralization sample on the root of bicuspid. C, Twenty-two-year-old man with tumor arising adjoining to root of first molar tooth. D, Gross photograph of tumor shown in C; tumor consists of agency, gritty mass attached to tooth root. A and B, Plain lateral and anteroposterior radiographs of osteoblastoma arising in left frontoparietal region of cranium of 18-year-old lady. Double contour of margin is caused by unequal destruction of inside and outer tables of calvarium. C, Computed tomogram exhibits shell of reactive bone peripherally and smaller intracranial bulge. D, Gross photograph of resected specimen exhibiting well-circumscribed, tan exterior surface of osteoblastoma. Note sharp circumscription and larger destruction of outer desk than of inside cortex. The cortex may be at least focally destroyed with or with out periosteal new bone formation. These options are liable for the radiologic confusion with malignant tumors that will occur in approximately 20% of osteoblastomas. The atypia is of a degenerative sort much like that more typically seen in historical schwannomas. The absence of mitotic exercise and specifically of atypical mitoses is helpful in distinguishing such lesions from an osteosarcoma. The distinguishing options of osteoid osteoma and osteoblastoma have been discussed within the opening paragraph of this chapter. The primary differences of dimension, ache pattern, and perilesional sclerosis are usually sufficient to separate these two entities, which are histologically indistinguishable. Osteoblastomas that attain sizes exceeding 4 cm and that present distinguished or exuberant periosteal new bone formation present issues of their radiographic differentiation from osteosarcoma. This group of osteoblastomas may present histologic features that can be misinterpreted as indicators of malignancy by the pathologist. These options embody foci of lacelike osteoid deposition, excessive cellularity, and quite so much of scattered mitotic figures. This could also be further difficult by the rare finding of small foci of cartilage in in any other case benignappearing osteoblastomas. Fortunately, these distinctive disturbing features often occur separately and focally in a tumor that otherwise represents a conventional benign osteoblastoma. A tumor that reveals all of the talked about atypical features is finest considered an osteosarcoma. Moreover, primary aneurysmal bone cysts not related to underlying lesions have a predilection for a similar anatomic websites as osteoblastomas. This is particularly true with regard to their occurrence within the posterior neural arch of vertebrae. Aneurysmal bone cysts may include microscopic zones of reactive osteoid and new bone that differ from the small, irregular, anastomosing trabeculae of nidus tissue. Similar to osteoid osteomas, osteoblastomas specific transcription elements controlling osteoblastic lineage differentiation, similar to Runx2 and Osterix. Because of its wealthy stromal vasculature, the tissue is granular, friable, and reddish and may bleed profusely when curetted. The nidus is nicely demarcated at its periphery and can be easily separated from the encompassing bone. There could additionally be gross proof of hemorrhage and cystic degeneration with blood-filled spaces characteristic of secondary aneurysmal bone cyst. The hemorrhage and secondary reparative adjustments are notably frequent in bigger lesions and should considerably alter the gross appearance. At low magnification the nidus tissue consists of an interlacing community of bone trabeculae evenly distributed in a unfastened fibroblastic stroma with a outstanding vasculature. The osteoid shaped may be deposited in coarse trabeculae or sparsely cellular sheets. Prominent rimming osteoblasts and multinucleated osteoclast-like giant cells are present. Although the lesion is grossly properly demarcated, microscopically the osteoid trabeculae merge gradually with the adjacent regular bone. When the tumor extends beyond the cortex, the soft tissue margin usually has a clearly recognizable shell of reactive bone. Large, expanded lesions normally have gross and microscopic proof of secondary aneurysmal bone cyst with a number of cystic areas filled with blood. In rare cases stromal cells in osteoblastoma may show pronounced atypia, such lesions are referred Treatment and Behavior Osteoblastomas have a higher growth potential than osteoid osteomas and should often attain considerable dimension. Lateral radiograph of femur with surface lesion (arrow) attached to posterior cortex. B and C, Sagittal and axial magnetic resonance T1-weighted pictures show subperiosteal location with cortical erosion. D, Radiograph of 15-year-old boy with knee pain, who was found to have eccentric lytic lesion of distal femoral metaphysis. E, Computed tomogram shows encapsulation by peripheral shell of subperiosteal bone and cortical erosion. A, Axial computed tomogram of pelvis displaying well-circumscribed osteoblastoma involving the iliac bone in the neighborhood of the sacroiliac joint. B, Low power photomicrograph of osteoblastoma exhibiting irregular unwell defined trabeculae of woven bone in hypercellular stromal tissue. C, Intermediate power photomicrograph of osteoblastoma with irregular bony trabeculae surrounded by outstanding rims of osteoblasts. B, Irregular, ill defined sheets of osteoid with entrapped osteoblastic cells (�100). D, Higher power view exhibits outstanding osteoblastic cells bordering irregular poorly mineralized bony trabeculae. A, Irregular haphazardly arranged bony trabeculae of woven bone surrounded by plump osteoblastic cells in a extremely mobile spindle cell stromal tissue with dilated vessels. C, Small focus of lacelike poorly mineralized osteoid with entrapped osteoblastic cells. D, Small focus of sick defined osteoid deposition with entrapped osteoblastic cells. A, Unusual case of osteoblastoma with space of well-developed cartilage in in any other case typical osteoblastoma.
Buy 500 mg cyklokapron mastercard
In one massive study medications bipolar disorder buy cyklokapron 500 mg cheap, exome sequencing of diffuse massive B-cell lymphomas detected recurrent mutations in 322 genes symptoms rotator cuff injury purchase 500 mg cyklokapron with visa. The kinds of mutations included copy quantity alterations, intergenic mutations, and mutations of coding and regulatory areas of various genes. These genes include epigenetic modifiers, genes involved in immune surveillance, and genes that regulate signaling pathways (Table 12-5). Inactivating mutations of 2 microglobulin (B2M) are seen in approximately 30% of diffuse giant B-cell lymphomas, resulting in the incapability of cytotoxic T cells to acknowledge lymphoma cells. In the setting of lymphoma, aberrant somatic mutation may be seen as a main event or could additionally be related to transformation to a extra aggressive lymphoma. The translocation associate is an immunoglobulin gene in additional than half of circumstances, with the remaining translocation partners represented by nonimmunoglobulin genes. The t(14;18) is present in small numbers of B cells in normal germinal middle B cells. It is characterised by the presence of quite a few, largely nonrecurrent, genetic abnormalities and atypical cytologic features with marked nuclear irregularity. The acute and lymphomatous varieties characterize aggressive illness, in which bone lots could additionally be current. The acute form accounts for 60% of circumstances and presents with lymphadenopathy, a leukemic picture, and a monoclonal absolute T lymphocytosis in addition to atypical morphology. The lymphomatous kind, accounting for 187452695 854 12 Hematopoietic Tumors Chr 14 thirteen eleven. The translocation ends in two derivative chromosomes, chr der(14) and chr der(18). Both of these varieties are associated with elevated lactate dehydrogenase and will usually contain the liver, spleen, pores and skin, or bone. Hypercalcemia is a characteristic medical finding, current in 70% of sufferers with the acute kind, not all of whom have lytic bone lesions. Recent research have proven that the acute, smoldering, and chronic varieties have a greater response to antiviral therapy with interferon alfa-2b and zidovudine than to chemotherapy. A recent scientific trial evaluating front-line antiviral therapy with chemotherapy for the acute form of grownup T-cell lymphoma/leukemia resulted in a 5-year survival fee of 28% for the antiviral arm versus 10% for the chemotherapy arm. Antiviral therapy of the continual kind resulted in a 100% 5-year survival fee in contrast with less than 20% with no therapy in one other examine. Microscopic Findings Adult T-cell lymphoma/leukemia might show significant variation in morphology from case to case. The continual and smoldering forms are usually composed of small lymphocytes with delicate pleomorphism. Acute and lymphomatous forms may display small lymphocyte morphology but are extra probably to show marked pleomorphism. The acute type typically shows marked pleomorphism, with circulating T cells with characteristic deeply lobulated nuclei often identified as flower cells. The differential prognosis consists of diffuse massive B-cell lymphoma, different T-cell lymphomas, and myeloid sarcoma. Adult T-cell lymphoma/leukemia has a characteristic though not particular immunophenotype. Other T-cell lymphomas, particularly peripheral T-cell lymphoma not otherwise specified are additionally thought-about in the differential analysis and should have the same immunophenotype. The hypercalcemia related to adult T-cell lymphoma/leukemia is a result of increased osteoclast exercise. Adult T-cell lymphoma/leukemia cells overexpress Wnt5, which has been proven to transform granulocyte/ monocyte precursors into osteoclasts. It is thought that activation of Wnt5a/Ror (receptor tyrosine kinase-like orphan receptor) -catenin independent noncanonical signaling ends in a shift towards osteoclastic bone resorption and decreased osteoblastic bone formation. The 5-year survival price is 85%, with most disease-related deaths occurring in patients over age 55 years. Overall, with modern therapy, radiographically identifiable bone involvement is extraordinarily unusual in the course of the course of the disease because most patients (90%) are disease-free for a really very long time and are sometimes thought-about cured. B, Radioisotopic bone scan showing multiple foci of elevated uptake throughout the skeleton. D, Axial computed tomography scan exhibiting a destructive lesion involving the thoracic vertebral physique. A, Photomicrograph of adult T-cell lymphoma displaying lytic bone lesion with osteoclasts (�200). C, Photomicrograph of adult T-cell lymphoma exhibiting lymphocytes with pleomorphic nuclei (�200). In the appendicular skeleton, the proximal components of main tubular bones, such as the femur and humerus, are preferentially involved. The putting characteristic is the presence of homogenous acidophilic, inclusion-like nucleoli that approximate 25% of the dimensions of the nucleus. The cellular microenvironment includes T cells, histiocytes, plasma cells, eosinophils, neutrophils, and fibroblasts. The classical lymphocyte-rich variant is the exception and is associated with a background of mantle zone B lymphocytes and variable numbers of histiocytes and T cells. The immunophenotype of the cellular surroundings listed above is attribute of nodular sclerosis and mixed cellularity subtypes, which characterize the majority of cases. The sorts that are frequently present in bone have options of nodular sclerosis and combined cellularity subtypes. In addition, the background cells may often be polymorphous, with plasma cells and eosinophils inflicting frequent confusion with osteomyelitis. To keep away from confusion with reactive or inflammatory problems corresponding to osteomyelitis, it is essential to consider the complete clinicopathologic picture. The appropriate analysis relies on identification of Reed-Sternberg cells or variants and demonstration of the appropriate immunophenotype by immunohistochemical stains. D, Photomicrograph of lacunar cells with cytoplasmic retraction artifact and lots of background eosinophils (�400). A, Photomicrograph of lacunar cells with cytoplasmic retraction artifact and many background eosinophils. Most studies require microdissection of Reed-Sternberg cells from the cellular microenvironment. In addition to translocations involving immunoglobulin genes common to many B-cell lymphomas, Reed-Sternberg cells have been found to have complex genetic abnormalities, including aneuploidy, positive aspects and losses of multiple chromosome loci, and a quantity of translocations and mutations (Table 12-7). Some of those genetic abnormalities result in deregulation of crucial signaling pathways. ReedSternberg cells have direct and oblique interactions with the surrounding cells and secrete varied cytokines and chemokines that entice the assorted constituents of the mobile microenvironment.
Cyklokapron 500 mg order on-line
Stroma is minimal and confined to few delicate fibrous tissue strands and blood vessels treatment variable cyklokapron 500 mg order. D when administering medications 001mg is equal to discount cyklokapron 500 mg visa, Higher magnification of C exhibits uniform tumor cells with minimal quantity of cytoplasm. Inset, High energy photomicrograph of Homer Wright rosette consisting of a central fibrillar core bounded by concentrically organized tumor cells. Note the presence of apoptotic darkish cells at the interphase of viable and necrotic tumor. D, Higher magnification of the interphase between viable and necrotic tumor tissue showing distinguished darkish apoptotic cells. In a small variety of tumors, the microscopic look of tumor cells might deviate from the so-called basic pattern. These options are extra usually seen in recurrent and treated lesions but can be present in primary tumors. A delicate, finely granular chromatin pattern and clearly identifiable small to medium nucleoli are characteristic. Immunohistochemical and molecular research allowing differential analysis with different small cell malignances may be performed on materials obtained for cytologic preparations. The cellularity is high, and the tumor cells are densely filled with nearly nonexistent stroma. Two kinds of cells as defined by gentle microscopy-a principal type (light with open intact chromatin) and a secondary sort (dark with condensed chromatin)-can even be acknowledged at the ultrastructural degree. Minimal quantities of stromal components related to endothelial-lined capillaries and occasional larger vessels are seen focally. Centrally positioned nuclei are oval to round and have outlines with occasional indentations of the nuclear membrane. Some intracytoplasmic reticulum and poorly developed small Golgi centers are present. The ultrastructure of the dark cells may present all the options of nuclear condensation and segmentation described for apoptosis. Before the appearance of chemotherapy, the prognosis was dismal, with a 5-year survival rate of less than 20%. The use of multimodality therapy plans of irradiation and multidrug chemotherapy plus surgical procedure has significantly changed this survival price. Those patients who initially have localized, resectable disease and are handled with multidrug chemotherapy along with surgery have a 5-year survival price of approximately 70%. A-D, Fine-needle aspirate containing undifferentiated spherical cells with occasional nucleoli and vague cytoplasm, occasionally forming rosette-like constructions (arrows). Inset, Rosettelike construction fashioned by circumferential association of tumor cells around central core containing delicate fibrillar cytoplasmic material. A and B, Undifferentiated mesenchymal cells containing sparse cytoplasmic organelles and outstanding deposits of glycogen. Note fantastic, evenly dispersed, granular chromatin of tumor cell nuclei (A, �5000; B, �14,000). A, Undifferentiated tumor cells containing sparse cytoplasmic organelles and regular round nuclei with freely dispersed chromatin on occasional nucleoli. Similar to osteosarcoma, it has been proven that surgical removal of the resectable lung metastases improves survival. The incidence of disseminated disease on the time of diagnosis is excessive, and roughly 15% to 28% of sufferers initially have metastatic illness. In addition, lesions in the latter websites are significantly bigger at presentation and show in depth gentle tissue involvement. Extensive spontaneous necrosis of untreated lesions is a predictor of more aggressive clinical behavior and is linked to lower survival rates. Its presence is considered by some authors to be synonymous with invasion into gentle tissue and may signify the next stage and quantity of lesions. Favorable response, which is outlined as total or subtotal (90% to 100%) necrosis, appears to be a robust predictor of long-term survival. The hyperlink between favorable prognosis and good chemotherapy response has been persistently proven in several unbiased studies. Moreover, the diploma of postchemotherapy necrosis seems to correlate with the rate of disease-free survival. In a research from the Rizzoli Institute, the 5-year disease-free survival rate was 90% for patients with complete necrosis, 53% for those with microscopic residual tumors, and 32% for these whose lesions had gross proof of residual tumor. Immunohistochemical features of overexpression of the genes concerned within the improvement of drug resistance, such as P glycoprotein, present some promising results, but too few instances have been studied to assess the sensible application of these findings. Sparse neurosecretory granules are associated with each growing Golgi centers and cell processes. The outer perimeter of the cells forming the rosette can generally be delineated by an incomplete basal lamina�like material. In a latest interinstitutional examine involving a quantity of facilities within the United States and Europe, the analysis of 315 instances showed no affiliation between neural differentiation and more aggressive conduct. In the unique report, the authors postulated that this lesion had a definite pathogenesis and apparently arose within the ribs, predominantly within the periosteum, however may additionally come up in the delicate tissue, and possibly throughout the lung. The lesions are incessantly constructive for one or several of the so-called neural markers, including neuron-specific enolase and neurofilaments of 70 kD, and may specific neuroendocrine markers corresponding to chromogranin. The unique options appear to be frequent primitive neural or neuroendocrine differentiation, in addition to focal epithelial differentiation. A, Tumor cells with sparse cytoplasmic organelles as seen on low power magnification. B, Centrally positioned cytoplasmic processes correspond to core of rosette (asterisk). A, Axonal differentiation of tumor cells with formation of interconnecting cytoplasmic processes (arrows). These two antibodies establish the antigen in formalin-fixed, paraffin-embedded tissue. It can be optimistic in pediatric lymphomas, lymphocytic lymphoma, and sometimes in rhabdomyosarcoma and even synovial sarcoma. Positivity for neuron-specific enolase is usually disregarded as a specific marker of neural differentiation. On the opposite hand, if its expression can be correlated with other features of neural differentiation, it provides a useful tool with which to assess the diploma of neural phenotypic expression. A, Intermediate energy view of small round-cell tumor with sparse stromal elements. C and D, Tumor cell displays strong positivity for periodic acid�Schiff stain, which is diastase sensitive (A-D, �400). Scattered positivity of particular person tumor cells for keratins may be seen in roughly 10% of these tumors. In general, the differential analysis of small round-cell tumors of bone include not only the entities described in this chapter, but also a selection of mesenchymal and epithelial (primary and metastatic) tumors that will occur in youngsters, adolescents, and adults.
Syndromes
- Blindness
- Cut down on salt, whether it is table salt, or flavor intensifiers that contain salt such as monosodium glutamate (MSG).
- ECG
- Abdominal pain - severe
- Increase fluid intake, especially cold milk products. Gargle with cool water or try eating popsicles. Avoid hot beverages and citrus fruits.
- MRI scan of the brain, brainstem, or spinal cord
- Anemia of chronic disease
- The most common type of air leak occurs when air gets into the space between the lung and inner chest wall. This is called a pneumothorax. This air can be removed with a tube placed into the space until the pneumothorax heals.
Generic cyklokapron 500 mg online
Trias A medications 2 times a day 500 mg cyklokapron cheap mastercard, Quintana O: Synovial chondrometaplasia: evaluate of world literature and study of 18 Canadian cases keratin treatment best 500 mg cyklokapron. Geldyyev A, Koleganova N, Piecha G, et al: High expression level of bone degrading proteins as a attainable inducer of osteolytic options in pigmented villonodular synovitis. Gonzalez-Campora R, Salas Herrero E, Otal-Salaverri C, et al: Diffuse tenosynovial large cell tumor of soppy tissues: report of a case with cytologic and cytogenetic findings. Mertens F, Orndal C, Mandahl N, et al: Chromosome aberrations in tenosynovial large cell tumors and nontumorous synovial tissue. Nakashima M, Uchida T, Tsukazaki T, et al: Expression of tyrosine kinase receptors Tie-1 and Tie-2 in giant cell tumor of the tendon sheath: a potential position in synovial proliferation. Nilsonne U, Moberger G: Pigmented villonodular synovitis of joints: histological and medical problems in diagnosis. Nilsson M, H�glund M, Panagopoulos I, et al: Molecular cytogenetic mapping of recurrent chromosomal breakpoints in tenosynovial large cell tumors. Ohjimi Y, Iwasaki H, Ishiguro M, et al: Short arm of chromosome 1 aberration recurrently present in pigmented villonodular synovitis. Berger I, Weckauf H, Helmchen B, et al: Rheumatoid arthritis and pigmented villonodular synovitis: comparative analysis of cell polyploidy, cell cycle phases and expression of macrophage and fibroblast markers in proliferating synovial cells. Dal Cin P, Sciot R, Samson I, et al: Cytogenetic characterization of tenosynovial giant cell tumors (nodular tenosynovitis). Fiocco U, Sfriso P, Lunardi F, et al: Molecular pathways involved in synovial cell irritation and tumoral proliferation in diffuse pigmented villonodular synovitis. Fujita S, Iizuka T, Tuboi Y, et al: Synovial chondromatosis of the temporomandibular joint with immunohistochemical findings: report of a case. Seki K, Hirose T, Hasegawa T, et al: Giant cell tumor of tendon sheath: an immunohistochemical observation on the traits and the capability of proliferation of tumor cells. Shinjo K, Miyake N, Takahashi Y: Malignant large cell tumor of the tendon sheath: an post-mortem report and evaluation of the literature. Tashiro H, Iwasaki H, Kikuchi M, et al: Giant cell tumors of tendon sheath: a single and a quantity of immunostaining analysis. Uchibori M, Nishida Y, Tabata I, et al: Expression of matrix metalloproteinases and tissue inhibitors of metalloproteinases in pigmented villonodular synovitis suggests their potential position for joint destruction. Ushijima M, Hashimoto H, Tsuneyoshi M, et al: Giant cell tumor of the tendon sheath (nodular tenosynovitis): a examine of 207 cases to examine the large joint group with the common digit group. Yoshida W, Uzuki M, Kurose A, et al: Cell characterization of mononuclear and giant cells constituting pigmented villonodular synovitis. Hallel T, Lew S, Bansal M: Villous lipomatous proliferation of the synovial membrane (lipoma arborescens). Salik Y, Akmee R, Yildiz Y, et al: Lipoma arborescens occurring in each knees at totally different instances: a case report. Siva C, Brasington R, Totty W, et al: Synovial lipomatosis (lipoma arborescens) affecting a number of joints in a patient with congenital quick bowel syndrome. Bruns J, Eggers-Stroeder G, von Torklus D: Synovial hemangioma: a rare benign synovial tumor-report of 4 circumstances. Busa R, Adani R, Marcuzzi A, et al: Acute posterior interosseous nerve palsy attributable to a synovial haemangioma of the elbow joint. [newline]In this chapter, we describe a few of these situations that may often simulate a neoplasm and should require microscopic examination to verify the prognosis or to rule out a neoplastic process. In the radiologic literature, these conditions are grouped into two major classes: those related to abnormal enchondral ossification and people primarily affecting the websites of membranous bone formation. It is usually accepted that the common characteristic of the conditions described in this chapter is that all of them come up from defects in bone resorption or formation in the course of the strategy of skeletal improvement, maturation, and transforming. A summary of medical shows, radiographic characteristics, and genetic alterations implicated within the improvement of hereditary bone dysplasia is offered in Table 21-2. The polyps of the gastrointestinal tract are adenomatous and sometimes contain the colon but can be present within the duodenum and abdomen. The adenomatous polyps of the gastrointestinal tract have a excessive propensity for malignant transformation. In reality, colon most cancers develops in all affected people until prophylactic colectomy is performed. The gentle tissue fibrous lesions vary from aggressive fibromatosis at one finish of the spectrum to a lesion which is histologically much like nuchal-type fibroma. They could be divided into (1) calvarial and mandibular ivory exostoses; (2) osteomas of the paranasal sinuses, facial bones, and orbit (sino-orbital osteomas); (3) enostoses or bone islands; and (4) surface (juxtacortical) osteomas of long bones. Lesions categorized microscopically as osteomas can be separated into a number of distinct clinicopathologic variants; ivory exostosis, sinoorbital osteoma, bone island, and surface osteoma of lengthy bones. Modified and used with permission from Greenspan A: Skelet Radiol 20:561�583, 1991. The most typical location is within the again and paraspinal region followed by the top and neck and extremities. They usually develop intraabdominally spontaneously or more usually after surgery. Microscopically, ivory exostoses are button-like excrescences of mature lamellar bone restricted to the cortical surfaces and normally continuous with the outer table of the skull or the mandibular cortex. The dense cortical lamellar bone making up these exostoses accommodates osteons with haversian canals. Rare cases of compact floor osteoma have been reported in different flat bones in addition to on long bones. A, Lateral radiograph of skull shows frontal area with buttonlike floor osteoma. B, Specimen radiograph of excised, ivory-like excrescence faraway from frontal regions of cranium. Compact bone with fibrous stroma shows focal osteoclastic resorptive activity (C, �25) (C, hematoxylin-eosin. Sometimes the latter areas show energetic reworking, with mobile fibrous tissue filling the interstices, osteoblastic activity, and osteoclastic resorption. For this reason, we choose to regard the sporadic osteomas that arise within the orbit, paranasal sinuses, and facial bones, particularly those that contain osteoblastoma-like foci or options of energetic bone manufacturing and reworking, as benign bone-forming neoplasms quite than as hamartomas or dysplasias. Occasionally, they attain a bigger dimension (giant osteoma) that compresses adjoining structures and trigger a disfiguring deformity. We also have seen a giant bone island that was misinterpreted microscopically as a low-grade intraosseous fibroblastic osteosarcoma. Surface Osteoma of Long Bones Surface osteoma that includes the clavicle, pelvic, or long bones of the extremities is the rarest type of osteoma. Similar to other osteomas, this lesion consists of mature lamellar bone organized into osteons and haversian canals. No continuity between the lesion and the underlying medullary cavity may be seen grossly or on radiographs. Osteoma that entails the floor of an extended bone must be radiographically and microscopically differentiated from parosteal osteosarcoma, melorheostosis, and osteochondroma. Moreover, the bone in osteoma is mature and types stable areas with recognizable haversian canals, that are usually not current in parosteal osteosarcoma. The distinction from melorheostosis relies primarily on the radiographic sample of the bone surface lesion.
Cyklokapron 500 mg purchase overnight delivery
There is loosely textured edematous chondroid and fibrous intervening tissue with vascular proliferation and a granulation-like tissue appearance symptoms gerd cheap cyklokapron 500 mg without prescription. An autosomal dominant sample of inheritance with variable clinical expressivity is postulated in familial circumstances medicine 7 buy generic cyklokapron 500 mg line. In a few of the bigger calcified nodules, cystic changes with fluid levels could be documented using these techniques. Gross Findings Tumoral calcinosis consists of an encapsulated firm mass of multiple calcified nodules that focally coalesce into larger, lobulated plenty. The nodules are filled with yellow-gray, pasty lots or a milky fluid that can be washed out from individual lesions. Chemical and ultrastructural analysis of this substance reveals calcium crystals consistent with hydroxyapatite. Incidence and Location Tumoral calcinosis may be very uncommon and appears to affect Africans and African-Americans predominantly, but it could additionally affect other ethnic teams. Calcifications are often positioned within the periarticular gentle tissue in the vicinity of main joints, such as the hips, shoulders, and posterior elbows. The inactive or mature section merely shows calcified deposits in a dense fibrous stroma. Differential Diagnosis Similar tumoral calcifications may be present in patients with a number of underlying metabolic calcium problems, such as continual renal illness or secondary hyperparathyroidism. Lesions much like tumoral calcinosis can occur in sufferers with main hyperparathyroidism, hypervitaminosis D, milk-alkali syndrome, and scleroderma. The phrases chondrocalcinosis and calcium pyrophosphate crystal deposition arthropathy were independently applied to the identical situation, which is characterised on radiographs by distinguished multifocal calcification in the cartilages of joints and intervertebral disks. The term encompasses pseudogout, chondrocalcinosis, and pyrophosphate arthropathy. A, Lateral radiograph of elbow exhibits coarse deposits of calcific material in area of olecranon bursa. B, Massive calcinosis in delicate tissue round parascapular area and axilla in teenage boy. C, Low power photomicrograph exhibits circumscribed foci of calcific material with central cystification and peripheral foreignbody giant-cell response in tumoral calcinosis. D, Higher power magnification exhibits calcified bodies and more finely dispersed, noncrystalline calcifications. The temporomandibular joint was involved in three patients, and the metatarsophalangeal joint of the great toe was concerned in two sufferers. Long-standing swelling of the affected area was famous in two patients with temporomandibular joint involvement. Two patients had a painful mass of the nice toe, which was clinically thought of to be gouty tophus. Rapid, progressive myelopathy at an upper cervical level developed in another patient. One patient was asymptomatic, and the lesion was discovered incidentally on imaging research carried out for other causes. None of the sufferers in our collection had radiographic evidence of chondrocalcinosis or medical signs in any other joints. Gross Findings the lesion is a circumscribed, white-gray mass with a kind of chalky appearance. The cellular tissues comprise giant numbers of histiocytes and foreign body�type large cells surrounding the calcified areas and representing a international body granulomatous reaction, whereas the much less cellular tissues include metaplastic chondroid tissues. The chondroid cells can be atypical, with variable nuclear dimension and shape, and may mimic a malignant cartilage tumor. The calcium pyrophosphate dihydrate crystals are detachable by decalcification, and their basophilic features are misplaced in demineralized sections. Differential Diagnosis the metaplastic chondrocytes found in our sequence of sufferers sometimes confirmed cytologic atypia (three patients) analogous to that seen in some sufferers with synovial chondromatosis and superficially resembled chondrosarcoma. Particularly in decalcified sections from which calcium pyrophosphate dihydrate crystals are misplaced, atypical options in metaplastic chondrocytes and the presence of myxoid stroma may result in the histologic misdiagnosis of chondrosarcoma. Grossly, tophaceous pseudogout is a calcified, chalky mass not like the calcification seen in chondrosarcoma. A international body�type granulomatous reaction containing histiocytes and big cells is a useful discovering to distinguish it from chondrosarcoma. More necessary, however, is the identification by polarized light microscopy of birefringent crystals characteristic of calcium pyrophosphate dihydrate. The exact nature of those crystals could be decided by radiographic diffraction or electron probe analysis. Synovial chondromatosis and chondromas in gentle tissue are the other lesions that could be confused with tophaceous pseudogout, particularly within the circumstances during which a heavily calcified cartilage matrix may obscure the cartilaginous nature. Indeed, radiographic diffraction studies in each synovial chondromatosis and chondroma of soft tissue show that the mineral deposits symbolize hydroxyapatite. Treatment and Behavior Tophaceous pseudogout could recur after complete or incomplete surgical excision. A, Radiograph of proper hip reveals calcified mass in delicate tissue adjoining to acetabular margin; this mass represents deposits of calcium pyrophosphate dihydrate in capsule of hip joint (arrows). The crystals are brief rhomboid or, hardly ever, needle shaped, just like urate crystals. A and B, Anteroposterior and lateral radiographs of foot present large calcification of soft tissue round metatarsophalangeal joint of nice toe resulting from localized deposit of calcium pyrophosphate dihydrate crystals. B, Computed tomogram of cervical backbone of patient shown in A reveals extradural calcific mass compressing dural sac (arrows). A, Calcified tophaceous deposit from plantar aspect of foot shows whitish chalky appearance much like that seen in monosodium urate tophus. B, Metaplastic chondroid change surrounds islands of basophilic calcified crystalline calcium pyrophosphate dihydrate. C, Some basophilic calcified deposits provoke international body�type, giant-cell reaction without chondroid metaplasia. D, Compensated polarization microscopy demonstrates constructive birefringence of rhomboid calcium pyrophosphate dihydrate crystals. C, Photomicrograph of decalcified specimen displaying lobules of myxoid material corresponding to areas of metaplastic cartilage and crystalline materials deposits. D, Higher magnification of C exhibiting an interface between hypercellular stroma and myxoid areas with distinguished plump histiocytic cells exhibiting nuclear atypia. This description is restricted to the tophaceous form of gout and the basic microscopic features which might be helpful in distinguishing this metabolic dysfunction from a neoplasm. Clinical Data In basic, gout is characterised by hyperuricemia and the deposition of monosodium urate crystals in synovial tissues. It is rare in women, however when it does have an effect on a female patient, the onset of signs usually occurs in the postmenopausal interval. Approximately 50% of the sufferers with gouty arthritis have nodular deposition of monosodium urate crystals which might be referred to as tophi. Radiographic Imaging the formation of tophi happens three to 40 years (average, 12 years) after the first assault of gout.
500 mg cyklokapron order with amex
They represent a heterogeneous group of neoplasms with various biologic behaviors 3 medications that cannot be crushed purchase cyklokapron 500 mg mastercard. They range from low-grade symptoms of ebola cyklokapron 500 mg buy cheap line, locally aggressive malignancies (grade 1) to extremely aggressive tumors with a excessive propensity for metastases (grade 3). Most skeletal myxoid chondrosarcomas are grade 2 lesions and are pathogenetically distinct from soft tissue myxoid chondrosarcomas. A small subset of bone myxoid chondrosarcomas are high-grade lesions and may be pathogenetically just like extraskeletal myxoid chondrosarcomas. Central and particularly secondary peripheral chondrosarcomas evolve via distinct molecular pathways. They catalyze the oxidative decarboxylation of isocitrate into -ketoglutarate of the Krebs tricarboxylic acid cycle. The progression mechanisms of chondrosarcoma are largely unknown, but high-grade lesions are characterised by aneuploidy and multiple chromosomal abnormalities. On the opposite hand, high-grade lesions most likely develop via a multistep mechanism that includes a quantity of reworking and tumor suppressor genes. In basic, aneuploidy and overexpression of Aurora kinases are adverse prognostic components. In chondrosarcoma, a number of genetic alterations (altered genes) correlate with the clinical aggressiveness of the lesion, and most high-grade tumors are aneuploid. Karyotyping research indicate that alterations involving a quantity of chromosones are frequent in chondrosarcoma of bone. Dedifferentiation can also occur in low-grade intramedullary osteosarcoma, parosteal osteosarcoma, big cell tumor, and chordoma. The growth of a similar, extremely deadly sarcoma in several distinct precursor conditions might in reality represent a pathogenetically related course of that has widespread molecular pathways of development. The bcl-2 protein is typically present within the low-grade precursor conditions however is absent within the sarcomatous part. Our knowledge point out that in depth losses of genetic materials on chromosome 17p play a job within the improvement of dedifferentiation. Chordoma the signature molecular mechanism concerned in the improvement of chordoma is chromothripsis. In reality, chordoma is the prototypic tumor in which this novel mechanism of cancer growth has been recognized. It instantly binds to nearly 100 target genes and influences the expression patterns of a myriad of downstream targets. It has been proven that brachyury, in reality, acts as a master regulator of an elaborate oncogenic network involving diverse pathways affecting the cell cycle and mobile interactions with matrix components. A, Chromosomal location and exonal structure of the brachyury (T) gene as nicely as the functional domains of the encoded protein. Variation within the websites of chromosomal breakpoints results in a quantity of fusion sorts (bracketed region). These biologically pushed therapeutic interventions open some new avenues for focused therapies, but their medical software stays to be confirmed. Abe E, Shiina Y, Miyaura C, et al: Activation and fusion by 1,25dihydroxyvitamin D3 and their relation in alveolar macrophages. Akatsu T, Takahashi N, Debari K, et al: Prostaglandins promote osteoclast-like cell formation by a mechanism involving cyclic adenosine 38,58-monophosphate in mouse bone marrow cell cultures. Akatsu T, Takahashi N, Udagawa N, et al: Role of prostaglandins in interleukin-1�induced bone resorption in mice in vitro. Amizuka N, Davidson D, Liu H, et al: Signalling by fibroblast progress factor receptor three and parathyroid hormone-related peptide coordinate cartilage and bone growth. Ducy P, Zhang R, Geoffroy V, et al: Osf2/Cbfa1: a transcriptional activator of osteoblast differentiation. Brehme M, Hantschel O, Colinge J, et al: Charting the molecular network of the drug goal Bcr�Abl. International Human Genome Sequencing Consortium: Finishing the euchromatic sequence of the human genome. International Human Genome Sequencing Consortium: Initial sequencing and evaluation of the human genome. Kolch W, Pitt A: Functional proteomics to dissect tyrosine kinase signalling pathways in cancer. Meyerson M, Gabriel S, Getz G: Advances in understanding cancer genomes through second-generation sequencing. National Research Council: Mapping and sequencing the human genome, Washington, D. The Cancer Genome Atlas Research Network: Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Wu W, Choudhry H: Next generation sequencing in cancer research, vol 2, Decoding the cancer genome, Springer, 2013, New York. Abe E, Miyaura C, Tanaka H, et al: 1,25-Dihydroxyvitamin D3 promotes fusion of alveolar macrophages each by a direct mechanism and by a spleen cell�mediated indirect mechanism. Dy P, Wang W, Bhattaram P, et al: Sox9 directs hypertrophic maturation and blocks osteoblast differentiation of growth plate chondrocytes. Katagiri T, Yamaguchi A, Ikeda T, et al: the non-osteogenic mouse pluripotent cell line C3H10T1/2 is induced to differentiate into osteoblastic cells by recombinant human bone morphogenetic protein-2. Komori T, Yagi H, Nomura S, et al: Targeted disruption of Cbfa1 results in a complete lack of bone formation owing to maturational arrest of osteoblasts. Loveridge N, Farquharson C: Studies on progress plate chondrocytes in situ: cell proliferation and differentiation. Muir H: the chondrocyte, architect of cartilage: biomechanics, structure, perform and molecular biology of cartilage matrix macromolecules. Taga T, Hibi M, Hirata Y, et al: Interleukin-6 triggers the association of its receptor with a attainable sign transducer, gp130. Tamura T, Udagawa N, Takahashi N, et al: Soluble interleukin-6 receptor triggers osteoclast formation by interleukin-6. Udagawa N, Takahashi N, Akatsu T, et al: Origin of osteoclasts: mature monocytes and macrophages are able to differentiating into osteoclasts beneath an appropriate microenvironment prepared by bone marrow�derived stromal cells. Dobashi Y, Sugimura H, Sato A, et al: Possible association of p53 overexpression and mutation with high-grade chondrosarcoma. Fujita J, Yoshida O, Yuasa Y, et al: Ha-ras oncogenes are activated by somatic alterations in human urinary tract tumors. Halevy O, Michalovitz D, Oren M: Different tumor-derived p53 mutants exhibit distinct biological actions. Harashima H, Dissmeyer N, Schnittger A: Cell cycle control throughout the eukaryotic kingdom. Yamada Y, Horton W, Miyashita T, et al: Expression and structure of cartilage proteins. Antill�n-Klussmann F, Garc�a-Delgado M, Villa-Elizaga I, et al: Mutational activation of ras genes is absent in pediatric osteosarcoma.
Cyklokapron 500 mg buy
C medications given for migraines purchase cyklokapron 500 mg without a prescription, Photomicrograph exhibiting proliferation of myofibroblastic cells with out cytologic atypia medications starting with p 500 mg cyklokapron cheap with mastercard. D, Proliferation of fibroblast-like spindle cells in fibrous stroma resembling fibromitosis incessantly seen in this reactive course of. A-C, Proliferation of myofibroblastic cells without cytologic atypia in dense fibrous stroma resembling fibromatosis (A-C, �100) (A-C, hematoxylin-eosin. A and B, Anteroposterior and lateral radiographs of tibia in baby show posterior cortical disruption in higher third of shaft, with periosteal new bone formation and surrounding bone sclerosis. It is mostly postulated that trauma and osteopenia are the 2 major predisposing components. Development of fracture, fragmentation, or both incessantly occur later in the course of the disease. Virtually all lesions eventually develop calcification (sclerosis) inside lytic areas of the affected bone and within the adjoining gentle tissue. Occasional binucleate chondrocytes, a high degree of cellularity, and myxoid adjustments are seen inside cartilaginous areas. Bone metaplasia is also regularly current with the production of ample immature woven bone. The bone metaplasia is equivalent to that seen in lesions of exuberant callus formation secondary to fracture therapeutic or in energetic myositis ossificans. The risk of misdiagnosis is compounded if this fracture callus extends into soft tissue. The osteocartilaginous materials can also show focal bone necrosis, fibrosis of the marrow, and proliferation of capillary vessels with hemosiderin deposits. The angiomatoid pattern of granulation tissue would possibly suggest angioma, but this is usually seen in fracture healing. Neuropathic change is typically recommended by the occasional presence of fragments of necrotic bone and cartilage particles that result from fragmentation of the fracture site. The intervening stromal tissue exhibits histiocytic and multinucleated giant-cell reaction. Microscopically, early lesions comprise polymorphonuclear (neutrophilic) leukocytic infiltrate in the marrow. Prominent formation of new reactive bone is usually a dominant feature in later phases of the disease. Results of bacterial, viral, and fungal cultures, in addition to special stains for infectious organisms, are constantly adverse. Some sufferers could have associated recurrent pores and skin lesions (pustolosis palmoplantaris). They include palmoplantar pustulosis, psoriasis, acne fulminans, neutrophilic eccrine hidradenitis, acute febrile netrophilic dermatosis, and pyoderma gangrenosum. Marginal erosions of tarsal bones and metatarsals are sharply outlined and completely radiolucent (arrows). Microscopic Findings Microscopically, monosodium urate crystals are needle shaped and reveal strongly negative birefringence under compensated polarization microscopy. Monosodium urate crystals are additionally present in tophi, where they form multicentric, radially oriented deposits surrounded by a matrix of amorphous materials, lipids, and proteinaceous particles. A and B, Anteroposterior and lateral views of knee of affected person with longstanding gout present bone erosion by tophaceous deposits of monosodium urate (arrows). Note radiolucent defects with sclerotic borders in femoral condyle, tibial plateau, patella, and fibular head. Clinical consequence of sufferers with persistent recurrent multifocal osteomyelitis is usually good, but some patients may have persistent disease after a protracted follow-up. Biopsy of the lesions is performed to verify the inflammatory nature of the process, and the lesions are hardly ever confused with a nonhematologic neoplasm. However, the late phases of the process, characterized by the predominant lymphoid infiltrate, may be confused with lymphoma of the bone. It is useful to consider in the differential diagnosis the whole scientific image and radiographic presentation of the lesion. Lymphoma of the bone almost by no means happens in young sufferers whose illness presents with multifocal involvement of metaphyseal elements. Primary amyloidosis, with no related generalized disorder, is very rare within the skeleton. The most frequent form of amyloidosis involving the skeleton is related to multiple myeloma. It can affect the skeleton diffusely as a half of disseminated multiorgan disorder. Olecranon deposit of monosodium urate crystals (tophus) reveals adequate calcium deposits to render it radiopaque. This phenomenon happens in only one third of gouty tophi, which are normally radiolucent. Less frequently diffuse or tumoral amyloidosis could be related to chronic autoimmune disorder. In older textbooks, secondary amyloidosis, such as that associated with tuberculosis or chronic infectious osteomyelitis, has been emphasised. A new form of skeletal amyloidosis has been described in patients receiving long-term dialysis. Several instances of tumorlike amyloidosis related to Bence Jones proteinuria and other laboratory parameters of plasma cell dyscrasias have been described. Extremely rare circumstances of tumoral amyloid deposition in bone with out another related disorders have been also described within the skeleton. Tumoral deposition of amyloid in bone is frequently related to cystic degeneration. Minimal quantities of amyloid deposit is most likely not recognizable on conventional histologic preparations. The presence of amyloidosis in such instances could be disclosed by all or a variety of the mentioned special stains. Note that tophaceous deposit of chalky materials erodes bone and disrupts joint surfaces. D, Higher power magnification of C depicts tophaceous deposit and disruption of interphalangeal joint surface and deposition of fabric in adjacent medullary cavity. A, Plain radiograph of right hand reveals a quantity of lytic periarticular defects with overhanging edges typical of tophaceous gout. B, Nodular (tophaceous) deposition of monosodium urate crystals surrounded by fibrosis with reactive changes such as mononuclear cells and multinucleated giant cells. C, Polarized microscopy of tissue processed and glued in nonaqueous solution reveals robust birefringence of needle-shaped monosodium urate crystals. D, Higher energy photomicrograph under compensated polarization microscopy exhibits negatively birefringent needle-shaped monosodium urate crystals. A, Lytic and sclerotic modifications in proximal metaphysis of tibia in patient with episodes of fever and bone ache. B, Radioisotopic bone scan exhibits elevated uptake in both femoral and tibial metaphyses.