
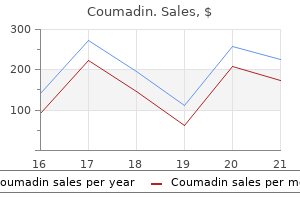
Coumadin dosages: 5 mg, 2 mg, 1 mg
Coumadin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Coumadin 5 mg trusted
The anterior and medial temporal lobes blood pressure phobia coumadin 2 mg cheap fast delivery, insular cortex prehypertension effects cheap 1 mg coumadin visa, subfrontal space, and cingulate gyri are most regularly affected (12-50A). Extratemporal, extralimbic Congenital, Acquired Pyogenic, and Acquired Viral Infections involvement occurs but is more widespread in youngsters compared with adults. Massive tissue necrosis accompanied by quite a few petechial hemorrhages and severe edema is typical. Inflammation and tissue destruction are predominantly cortical however may prolong into the subcortical white matter. Perivascular lymphocytic cuffing with diffuse neutrophil infiltration into the necrotic parenchyma is typical. It follows a bimodal age distribution, with one-third of all circumstances occurring between the ages of 6 months and 3 years and one-half seen in patients older than 50. A viral prodrome followed by fever, headache, seizures, behavioral changes, and altered mental standing is typical. Nearly two-thirds of survivors have significant neurologic deficits regardless of antiviral therapy. Hypodensity with mild mass impact in a single or both temporal lobes and the insula may be present (12-51A). Infection, Inflammation, and Demyelinating Diseases 366 demonstrate cortical/subcortical hyperintensity with relative sparing of the underlying white matter. Enhancement varies from none (early) to intense gyriform enhancement a quantity of days later (12-52D). Primary neoplasms similar to diffusely infiltrating astrocytoma often involve white matter or white matter plus cortex. Acute cerebral ischemia-infarction occurs in a typical vascular distribution, involving each the cortex and white matter. Postictal edema is transient however generally more widespread, usually involving most or the entire hemispheric cortex. Temporal lobe confluent hyperintensities with patchy foci of marked hypointensity are consistent with encephalomalacia and chronic hemorrhage. Similar findings have been current in the insular cortex and cingulate gyri (not shown). The median interval between transplantation and onset of neurologic signs is three weeks. Patients sometimes present with altered mental status, shortterm memory loss, and seizures. Note edema and mass effect, seen as hyperintensity in both cerebellar hemispheres. Postictal hippocampal hyperemia is transient, and extrahippocampal involvement is absent. The most common nonepidemic viral encephalitis, herpes encephalitis, was discussed earlier. Miscellaneous Acute Viral Encephalitides Viral encephalitis is a medical emergency. Timely, correct prognosis and immediate therapy can improve survival and scale back the likelihood of mind injury. Ischemic or hemorrhagic strokes, aneurysms, subarachnoid and parenchymal hemorrhages, arterial ectasias, and dissections have all been described. Meningitis is probably the most frequent total manifestation (50% of cases) and the commonest clinical presentation in immunocompetent patients (90%). Transmission will increase in warmer months; in the Northern hemispheres, peak activity is from July via October. Hemorrhage and enhancement are usually absent, helping differentiate rabies from Japanese encephalitis and different viral encephalitides. Onset of neurologic deterioration happens a couple of days to per week after the first indicators of influenza an infection. The morbidity and mortality are notably spectacular amongst patients with trisomy 21 (12-68). Nearly 55,000 deaths as a outcome of rabies encephalitis happen yearly, 99% of them in Asia and Africa. The virus is ample in the saliva of the contaminated animal and is deposited in bite wounds. The historical past and medical presentation are highly suggestive, however the definitive diagnosis requires laboratory confirmation of rabies antigen or rabies antibodies or isolation of the virus from biologic samples. Periventricular white matter, cerebellar, and spinal cord involvement has been reported in some instances. The midbrain, pons, cerebellum, and deep cerebral white matter are regularly involved. Miscellaneous Infectious Viral Encephalitides A host of different viral encephalitides have been identified. Arthropod-borne (ticks and mosquitoes) viruses characterize an underappreciated cause of encephalitis in older pediatric patients and adults. In this section, we briefly consider two continual encephalitides: the measles reactivation syndrome called subacute sclerosing panencephalitis and Rasmussen encephalitis. Measles virus disproportionately affects kids in areas with low measles vaccination rates. Symptom onset is commonly insidious, with behavioral and cognitive deterioration, myoclonic seizures, and progressive motor impairment. More than 95% of patients die inside 5 years, most within 1-6 months after symptom onset. Diffuse atrophy with ventricular and sulcal enlargement ensues as the disease progresses. Biopsy findings are nonspecific, with leptomeningeal and perivascular lymphocytic infiltrates, microglial nodules, neuronal loss, and gliosis. Patients are clinically normal until seizures begin, usually between the ages of 14 months and 14 years. Neurologic deficits are progressive, and the seizures usually turn into medically refractory. Treatment choices have included immunomodulatory therapy, focal cortical resection, and functional hemispherectomy. Infection, Inflammation, and Demyelinating Diseases 376 Selected References Congenital Infections Lee J: Malformations of cortical improvement: genetic mechanisms and diagnostic approach. Immigration and widespread journey have resulted in previously unique "tropical ailments" such as neurocysticercosis and different parasitic infections becoming commonplace. We first flip our consideration to mycobacterial infections, focusing totally on tuberculosis. They are divided into three primary groups, each with a unique signature disease: (1) Mycobacterium tuberculosis (tuberculosis), (2) nontuberculous mycobacteria ("atypical" mycobacterial spectrum infections), and (3) M. Each group has different pathologic features, medical manifestations, and imaging findings. We follow with a quick evaluate of nontuberculous mycobacterial infection and its uncommon manifestations within the head and neck.
Coumadin 2 mg lowest price
A pectoralis main musculocutaneous flap dissection in a female patient within the setting of surgical salvage heart attack risk assessment coumadin 2 mg. The pores and skin paddle is harvested from the inframammary fold on the slim denervated strip of muscle blood pressure 40 over 20 5 mg coumadin cheap with amex. Duplex ultrasound is a helpful adjunct study that confirms the vascular anatomy of the flap. This is best completed using lighted breast augmentation retractors or a head light. A laparoscopic harmonic scalpel is especially useful to achieve safe hemostasis. Salvage laryngectomy with neck dissection for chemoradiation failure of squamous cell carcinoma of the larynx. C, the radiated neck and skin of the higher chest are fully divided to stop compression of the flap pedicle and exposed muscle floor if grafted with a sheet split-thickness pores and skin graft. In many cases the whole muscle is harvested, utilizing the flap to cover vessels, a pharyngeal suture line, or other areas of defect. Careful visualization of the vascular pedicle on the deep floor of the muscle and palpation of the pulse are essential to the safety of the dissection. A tunnel is made between the chest and the neck in a subcutaneous plane to allow passage of the flap into the neck/defect. Detached from its clavicle insertion, the clavipectoral fascia varieties a fascial band, which have to be released to keep away from compression of the pedicle. Deep elements of the flap are secured to prevertebral fascia or other constructions such because the mandible to keep away from down pulling due to gravity, thus preventing dehiscence and leaks. Dehiscence of flap and postoperative fistula as a result of its bulk and pedicle attachment. Partial flap necrosis typically because of inadequate blood provide to random portion of flap 3. Introduced by Ariyan in 1979,1 the pectoralis major regional flap turned the usual and dependable technique of reconstruction of enormous defects within the head and neck till microsurgical reconstructions turned broadly obtainable. Flap physiology, flap bulk, pedicle tethering, and wound morbidity of the donor site-which communicates directly with the site of the reconstruction-may play deleterious roles. There are important physiologic differences within the blood supply of pedicled flaps and free flaps that may pertain to the prevalence of microvascular reconstructions. The reliability of such microvascular flaps and the ability of their blood supply are truly superior to traditional regional flap reconstructive surgery. Limited pedicle size and arc of rotation � Preoperative flap design and measurements are crucial. Excessive traction on the thoracoacromial pedicle � Careful design, dissection, inset of the pores and skin paddle, and suture stabilization of the muscle portion of the flap are preventive measures. Dehiscence Editorial Comment As microsurgical techniques have turn into broadly adopted and refined, free flap reconstruction has supplanted reconstruction with the pectoralis major flap. The vascular territories (angiosomes) of the body: experimental study and medical functions. A comparability of useful resource cost for head and neck reconstruction with free and pectoralis major flaps. Comparison of the rectus abdomens free flap with the pectoralis main myocutaneous flap for reconstructions in the head and neck. Which of the next is a relative contraindication to using a pectoralis major flap Pharyngeal reconstruction within the patients with vessel-depleted multiply operated necks d. A 78-year-old moribund affected person underwent a composite resection for remedy of domestically superior squamous cell carcinoma of the oral cavity; earlier palliative radiation had failed. The whole procedure was carried out on the premise of a weight-based heparin nomogram and aspirin in view of lately placed cardiac stents and symptomatic cerebrovascular illness. General "nonsurgical" oozing is famous in the lateral facet of essentially the most cephalad a part of the dissection pocket. A 69-year-old edentulous man with squamous cell carcinoma of the oral cavity invading left mandibular parasymphysis (T4 N0) underwent composite resection with bilateral neck dissection and reconstruction with an osteocutaneous free fibula flap. On postoperative day 1, the patient was taken back to the working room for venous congestion and underwent venous thrombectomy. Despite postoperative anticoagulation, necrosis of the intraoral skin paddle developed and salivary leak into freshly dissected neck ensued. The patient was again returned to the working room where the free fibula was found to be utterly necrotic. Placement of radial forearm fasciocutaneous free flap over the existent mandibular plate b. Placement of pectoralis main musculocutaneous flap to cover the existent reconstruction plate. Removal of the plate and pectoralis main musculocutaneous flap (mandibular swing) 1190. Since the introduction of this system within the Sixties, the chance of reliably transposing large volumes of vascularized tissue for reconstruction has revolutionized our capacity to resect disease and safely reconstruct defects within the head and neck. Although vital focus was positioned on the position of free flaps for reconstruction in the course of the 1980s and Nineteen Nineties, current years have introduced a rebirth of interest and enthusiasm for the use of regional flaps. An ideal reconstruction offers a patient with the best end result (in each perform and form) with the lowest donor-site and general morbidity. Flaps from the cervicofacial area include both randompattern vascular flaps (cervicofacial flaps) and axial vascular pattern flaps (cervicopectoral, supraclavicular, deltopectoral, and submental flaps). A complete understanding of regional anatomy allows for the use of a quantity of regional flaps to reconstruct defects in the head and neck. Planning for the vascular pedicle and its ultimate geometry are of key significance for flap viability and success in reconstruction. Prior treatment within the head and neck region 1) Prior head or neck surgery could affect the viability of regional reconstructive options. Medical illnesses that may have an effect on flap viability and reconstructive outcomes 1) Diabetes, particularly if poorly controlled, can affect therapeutic outcomes and flap viability. Family medical historical past 1) Coagulopathies can promote postoperative bleeding or coagulation and thus flap viability. Medications 1) Consideration of risks/benefits to discontinuing any medication that may increase the risk of bleeding. The face ought to be rigorously evaluated for any scars or evidence of prior surgical intervention, as this could disrupt blood flow for a cervicofacial development flap. The measurement of the defect ought to be measured to be positive that the planned flap is large sufficient to cover the defect. The neck must be fastidiously evaluated for any scars or proof of prior surgical intervention that may affect blood flow.
Coumadin 5 mg discount free shipping
Lateral skull base reconstruction: a comparability of the submental flap to free and regional flaps heart attack grill nyc cheap coumadin 1 mg without a prescription. Landmarks for the supraclavicular triangle embody all of the following except the a hypertension and obesity purchase coumadin 1 mg on line. The commonest dorsal surface pedicled flaps used for head and neck reconstruction are the trapezius and latissimus dorsi flaps. Thus, flap planning and final inset should take this into consideration and ensure that the vascular pedicle lies simply with out kinking, compression, or tension. The reason for the defect ought to be decided as a outcome of it could have an result on current and future reconstructive needs. For instance, a pedicled flap reconstruction may provide essentially the most rapid/ instant resolution for traumatic defect coverage. However, if a free flap would provide the most effective longterm results, a free flap could also be the popular reconstructive option regardless of the added time and complexity associated with this form of reconstruction. The extent and complexity of the defect requiring reconstruction should be decided. Thus, cutaneous tissue defects are ideally reconstructed with cutaneous tissue of similar color, thickness, and texture. Prior treatment in the head and neck area: 1) History of surgery within the neck, axilla, and back could affect viability of regional reconstructive options. Medical diseases could affect flap viability and reconstructive outcomes: 1) Diabetes, particularly if poorly controlled, can effect healing outcomes and flap viability. Family medical history: 1) Coagulopathies might have an result on postoperative bleeding or coagulation and thus flap viability. Medications: 1) Consider the dangers and benefits of discontinuing any drugs that may enhance the perioperative threat of bleeding. The neck should be fastidiously evaluated for any scars or proof of prior surgical intervention that the patient may have forgotten to point out during collection of the historical past of the present sickness or previous medical history. The axilla and extremity on the aspect thought-about for flap harvest ought to be fastidiously inspected for any proof of scars suggesting prior surgery. The range of motion and strength of the extremity on the side selected for flap harvest must be rigorously evaluated and documented preoperatively. A Doppler examination to identify and trace the vascular pedicle ought to be carried out prior to proceeding with surgery. The web site of Doppler alerts ought to be marked with a marking pen to facilitate future identification. No dedicated imaging of the neck, axilla, or again is required prior to planning or harvesting trapezius or latissimus dorsi flaps. Due to the extent of dissection and positioning needs of the surgery, general anesthesia is important for the procedure. Some surgeons choose paralysis during dissection as a end result of it relaxes muscle tissue and makes manipulation simpler. Others prefer no paralysis to aid in identification of motor nerves throughout dissection. Antibiotics should be chosen based mostly on the first website defect and related threat of infection. Scarring/cosmetic defect: It may be inconceivable to close donor websites primarily, and so they might require split-thickness pores and skin grafting. When split-thickness pores and skin grafting is used, a much less aesthetic donor site look will generally result, and a second donor site is created where the graft is harvested. Flap loss: A vital risk in any flap reconstruction surgical procedure is that of partial or total flap loss. In pedicled flaps, the commonest reason for whole flap loss is poor pedicle geometry with pedicle compression inside a tunnel, kinking, or rigidity at time of inset. Damage to surrounding constructions: During flap harvest and inset involving the trapezius flaps and latissimus dorsi flaps, there are a quantity of neurovascular buildings in danger. Damage to the brachial plexus can affect perform of the shoulder and higher extremity. Damage to the accent nerve or destabilization of key trapezius muscular insertions can outcome in shoulder droop and weak spot. Requires placement of the axillary roll and careful positioning to forestall injury of the brachial plexus 2. There is much less publicity of the again compared to a real lateral decubitus positioning. Prone positioning may be most popular if trapezius or latissimus dorsi flaps are used to reconstruct the posterior neck or occipital defects. It has insertions onto the lateral third of the clavicle, the backbone of the scapula, and the acromion. The trapezius muscle is related to three separate musculocutaneous flaps based mostly on three separate vascular pedicles. These include the superior trapezius flap, the lateral trapezius flap, and the inferior trapezius flap. Superior Trapezius Flap the superior trapezius musculocutaneous flap relies upon vascular contributions from the paraspinous muscular perforators and from branches of the occipital artery. Due to the limited arc of rotation, this flap can only reach the lateral neck for defect reconstruction and hence has been supplanted by newer reconstructive choices. Bleeding: Development of a hematoma have to be fastidiously monitored because it can cause compression of the vascular pedicle and end in flap compromise. Infection: Infection on the flap donor website is a relatively low risk, but the space may be contaminated by the defect undergoing reconstruction (especially in cases involving oral or Contraindications 1. Prior neck surgery that will have damaged the vascular supply from the occipital artery. The flap is designed by incorporating the pores and skin overlying the trapezius muscle with a superior and medial base. The superior/anterior incision is placed alongside the anterior edge of the trapezius muscle. The inferior incision is designed parallel to the anterior incision on the level of the scapular spine. The lateral extent of the flap is designed at or past the extent of the acromion. The incisions are opened and the flap is elevated in a lateral-to-medial path. Once the acromion is reached, the trapezius is elevated sharply off its bony insertions. The transverse cervical vessels are commonly recognized during this portion of the procedure and must be divided. The lengthy axis of the flap is designed between the vertebral column and the medial scapula edge. The inferior end of the flap can lengthen as much as thirteen cm distal to the trapezius muscle. A flap that extends past the trapezius muscle edge has a random-pattern blood provide. Flap elevation begins with identification of the transverse cervical vascular pedicle within the neck.
Buy 2 mg coumadin otc
Endovascular thrombectomy advantages most sufferers with acute ischemic stroke caused by occlusion of the proximal anterior circulation and provides another heart attack heartburn buy discount coumadin 5 mg on-line, probably synergistic methodology to thrombolysis arrhythmia heart rate monitor coumadin 1 mg generic online. Its advantages embrace delivering site-specific therapy and tailored thrombolytic dosage. Mechanical thrombectomy may be appropriate in patients past the therapeutic window or in whom thrombolytic therapy is contraindicated. The main goals of emergent stroke imaging are (1) to distinguish "bland" or ischemic stroke from intracranial hemorrhage and (2) to select/triage sufferers for attainable reperfusion therapies. Once intracranial hemorrhage is excluded, the second critical problem is determining whether a significant cerebral vessel is occluded. Nontraumatic Hemorrhage and Vascular Lesions 212 alternative for depicting potentially treatable main vessel occlusions. With helical acquisition, the complete protocol could be completed within 15 minutes as a single examination with separate distinction boluses. The most particular however least sensitive sign is a hyperattenuating vessel crammed with acute thrombus. It is critically necessary to determine calcified cerebral emboli, as they carry a near 50% threat of repeat ischemic stroke. M1-3 characterize the center cerebral artery cortex with each area allotted one point. The insular cortex (I), lentiform nuclei (L), caudate head (C), and internal capsule are scored with one level each. Loss of the insular cortex ("insular ribbon" sign) (8-38A) and decreased density of the basal ganglia ("disappearing basal ganglia" sign) are the most typical findings (8-37A). Cortical gyriform enhancement is uncommon in early arterial occlusion however may occur in late acute/early subacute infarction. Nontraumatic Hemorrhage and Vascular Lesions 214 occlusion with a "retrievable" intravascular thrombus present Note hypodensity of the right temporal lobe, insular cortex ("insular ribbon sign"). The core infarct includes the right frontal lobe, basal ganglia, and deep/periventricular white matter. Arterial Anatomy and Strokes the standard shade scale is graduated from shades of purple and yellow to blue and violet. Well-perfused grey matter appears red/yellow, white matter appears blue, and ischemic mind is blue/purple. Here the color scales are reversed to emphasize the abnormally extended transit time in the ischemic brain. The infarct core is seen as a dark blue/purple or black area that contrasts with the usually perfused red/yellow mind (837B). Ischemia-induced vascular injury predisposes to two highly morbid and probably fatal postischemic complications, i. With large vessel occlusions, loss of the expected "circulate void" in the affected artery can generally be identified. Also look fastidiously for the presence of multifocal parenchymal microbleeds in older patients. In this age group, "blooming black dots" are mostly brought on by persistent hypertension or amyloid angiopathy. The presence of cerebral microbleeds may be an unbiased danger factor for subsequent anticoagulation-related hemorrhage. Aquaporins are transmembrane proteins-water channels-that facilitate bidirectional selective water transport in and out of the cell. Arterial Anatomy and Strokes to intraarterial thrombolysis or mechanical thrombectomy. Clot location and size may be precisely decided and collateral circulation delineated. Frequent findings embrace an abrupt vessel "cut-off" (8-42A), "meniscus" signal, tapered or "rat-tail" narrowing, or "tram-track" appearance with a trickle of contrast across the intraluminal thrombus. Other common angiographic findings embody a "bare" or "naked" space of nonperfused brain (8-42B) (8-42C), slow antegrade filling with delayed washout of distal branches (seen as intraarterial contrast persisting into the capillary or venous phase), and pial collaterals with retrograde filling throughout the cortical watershed (8-42D) (8-42E) (8-42F). Less widespread signs are hyperemia with a vascular "blush" across the infarcted zone (so-called luxury perfusion) (8-42F) and "early draining" veins (arteriovenous shunting with contrast showing in veins draining the infarct while the remainder of the circulation continues to be within the late arterial or early capillary phase). Mass effect is rare in hyperacute stroke however very common within the acute/late acute levels. A "hyperdense vessel" signal may be simulated by elevated hematocrit (all the vessels appear dense, not just the arteries), arterial wall microcalcifications, and hypodense brain parenchyma. Nontraumatic Hemorrhage and Vascular Lesions 218 (8-41A) Acute stroke in a 47y man exhibits patchy hyperintensity in left caudate nucleus, lateral putamen, and parietal cortex. Arterial Anatomy and Strokes Subacute Cerebral Infarcts Terminology Strokes evolve pathophysiologically with corresponding changes reflected on imaging studies. Frank tissue necrosis with progressive inflow of microglia and macrophages round vessels ensues with reactive astrocytosis around the perimeter of the stroke. Ischemiadamaged vascular endothelium turns into "leaky," and blood-brain barrier permeability increases. When reperfusion is established-either spontaneously or following treatment with tissue plasminogen activator-exudation of purple blood cells through the broken blood vessel partitions causes parenchymal hemorrhages. Petechial hemorrhages are extra frequent than lobar bleeds and are most common within the basal ganglia and cortex. Mass effect initially will increase, then begins to lower by 7-10 days following stroke onset. Patchy or gyriform enhancement seems as early as 2 days after stroke onset, peaks at 2 weeks, and usually disappears by 2 months. Signal intensity in subacute stroke varies depending on (1) time since ictus and (2) the presence or absence of hemorrhagic transformation. Signal intensity decreases with time, reaching isointensity at 1-2 weeks (the T2 "fogging impact") (8-47). Nontraumatic Hemorrhage and Vascular Lesions 222 can typically be identified as a well-delineated hyperintense band that extends inferiorly from the infarcted cortex alongside the corticospinal tract. The intravascular enhancement often seen within the first forty eight hours following thromboembolic occlusion disappears within three or four days and is changed by leptomeningeal enhancement attributable to persisting pial collateral blood circulate. Patchy or gyriform parenchymal enhancement can happen as early as 2 or three days after infarction (8-46) and may persist for 2-3 months, in some instances mimicking neoplasm (8-48). Arterial Anatomy and Strokes Chronic Cerebral Infarcts Terminology Chronic cerebral infarcts are the end result of ischemic territorial strokes and are additionally called postinfarction encephalomalacia. A cavitated, encephalomalacic brain with strands of residual glial tissue and traversing blood vessels is the standard gross look of an old infarct (8-49A). The adjoining sulci and ipsilateral ventricle enlarge secondary to volume loss within the affected hemisphere (849A). Look for atrophy of the contralateral cerebellum secondary to crossed cerebellar diaschisis. Multiple Embolic Infarcts Brain emboli are less widespread however essential causes of stroke. Simultaneous small acute infarcts in a number of different vascular distributions are the hallmark of embolic cerebral infarcts (8-51).
Generic 2 mg coumadin overnight delivery
In these instances hypertension disorder 2 mg coumadin purchase fast delivery, striking foci with irregular rim enhancement are frequently-but not invariably-present arrhythmia game 1 mg coumadin amex. Corticosteroids significantly lower the prevalence and intensity of enhancement. Chronic "burned out" lesions show elevated diffusion due to disorganized cellular structure (14-28). Increased choline, consistent with myelin destruction, and a lipid-lactate peak from necrosis are sometimes current. Retinitis and myelitis with radiculitis are the two most frequent extracranial displays. Mortality approaches one hundred pc, and median survival is measured in days to a couple of weeks. In-hospital parasitemia, renal impairment, and clinical deterioration are common in these coinfected patients, so early identification of both infections is essential for management. Both differ in clinical expression, illness management, and prognosis though their imaging manifestations are similar. Here brain parenchyma is broken by each the replicating pathogen and the incited immune response. The recovering immune response targets persistent pathogenderived antigens or self-antigens and causes tissue harm. More than 90% are supratentorial, with preferential location in the basal ganglia and deep white matter abutting the lateral ventricle. Toxoplasmosis is more generally a quantity of, and lesions typically exhibit the "eccentric target" signal, i. Overall, the commonest site is the skin (14-42), followed by mucous membranes, lymph nodes, and viscera. We then turn our consideration to postinfection and postvaccination inflammatory syndromes. The recent recognition of autoimmune encephalitis and autoantibodymediated diseases as necessary issues with overlapping neurological and imaging features is then addressed. The chapter concludes by discussing three important inflammatory-like disorders of unknown or uncertain etiology: neurosarcoidosis, idiopathic inflammatory pseudotumors, and continual inflammatory demyelinating polyneuropathy. Proinflammatory cytokines and T-cell-mediated macrophage and resident microglia activation play a crucial function in inflammatory demyelination, each in the preliminary and sustained immune responses to myelin antigens. It is influenced by a posh interplay of genetic susceptibility and epigenetic and postgenomic events. Environmental elements with various, population-specific ranges of prevalence-latitude gradient additionally play a prominent function. Note the characteristic perpendicular orientation of the lesions on the callososeptal interface along penetrating venules. Ovoid plaques demonstrate the attribute perpendicular orientation along medullary veins. Acute lesions are sometimes hypercellular, with foamy macrophages and outstanding perivascular T-cell lymphocytic cuffing. Normal-appearing white matter also regularly demonstrates adjustments, together with microglial activation, T-cell infiltration, and perivascular lymphocytic cuffing. Less than 10% happen in the posterior fossa though infratentorial lesions are comparatively more widespread in children. Between 50-90% of all supratentorial lesions happen at or close to the callososeptal interface and adjacent to the lateral ventricles (15-2) (15-3). Centripetal perivenular extension is widespread, inflicting the appearance of "Dawson fingers" radiating outward from the lateral ventricles. Other commonly affected areas embrace the subcortical Ufibers, brachium pontis, brainstem (15-4), and spinal cord. Chronic inactive plaques have more distinctly outlined borders and are grayish in colour with scarred and excavated, depressed centers (15-6). It is the commonest persistent nontraumatic neurologic illness among younger and middle-aged individuals within the developed world. Perivascular persistent irritation and scattered stellate reactive astrocytes are current. Caucasians of Northern European descent living in temperate zones are essentially the most commonly affected ethnic group. Clinical presentation varies with heterogeneous neurologic manifestations, evolution, and incapacity. The interaction between inflammatory and neurodegenerative processes sometimes leads to intermittent neurologic disturbances adopted by progressive accumulation of disabilities. Attacks ("relapses" or "exacerbations") are followed by periods of partial or full restoration. Approximately one-third have an preliminary episode followed by normal or near-normal function. Although most are small-between 5 and 10 mm-large lesions can reach several centimeters in diameter. Enlarged ventricles and sulci with white matter volume loss and a thinned corpus callosum are typical findings. T1 hyperintensity is an independent predictor of atrophy, incapacity, and advancing illness. A faint, poorly delineated peripheral rim of delicate hyperintensity secondary to lipid peroxidation and macrophage infiltration often surrounds sharply delineated hypointense "black holes. Chronic and extreme circumstances typically show average volume loss and generalized atrophy. Larger lesions usually show a really hyperintense center surrounded by a barely less hyperintense peripheral space (15-15B) and variable amounts of perilesional edema. Note triangle form and perpendicular orientation of lesions following the course of deep medullary veins. A outstanding incomplete rim ("horseshoe") of enhancement with the "open" nonenhancing section facing the cortex can be present, especially in large "tumefactive" lesions (15-16) (1517) (15-18). Leptomeningeal enhancement occurs in some circumstances and may be a surrogate marker for cortical demyelination. Steroid administration considerably reduces lesion enhancement and conspicuity and will render some lesions just about invisible. Myoinositol ranges are elevated in acute lesions and are additionally increased in normal-appearing white matter. Volume loss with multiple hypointense ovoid and triangular lesions in the deep periventricular white matter is present. The broad bases of the triangles are oriented towards the ventricular surface with the apices pointing toward the cortex. Note triangle-shaped occipital lesions with broad bases at the ventricular floor. The left parietal lesion with incomplete ("horseshoe") rim enhancement exhibits diffusion restriction within the periphery surrounding a nonrestricting hypointense core. The left hemisphere lesions reveal a extra hypointense middle surrounded by a less hypointense rim.
Collard Greens (Cabbage). Coumadin.
- Are there any interactions with medications?
- Stomach pain, stomach and intestinal ulcers, bladder cancer, excess stomach acid, asthma, morning sickness, preventing osteoporosis and cancer, and other uses.
- Dosing considerations for Cabbage.
- Relieving breast engorgement (hard, painful breasts) in breast-feeding women, when applied to the skin of the breasts.
- Are there safety concerns?
- How does Cabbage work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96208
Discount 5 mg coumadin amex
Postextubation narcotic withdrawal occurs frequently in patients who require sedation and air flow and ought to be appropriately recognized and treated heart attack songs 1 mg coumadin generic free shipping. For delicate stenosis with limited symptoms hypertension kidney disease symptoms 1 mg coumadin order with amex, conservative administration has been proven to be protected. For sufferers too critically ill for surgical repair, temporizing measures with endoscopically placed stents could be utilized. Biodegradable stents should be considered over permanent stents, that are associated with a better rate of probably devastating issues. When symptoms of tracheal stenosis are current, the luminal stenosis is estimated to be at the following, respectively: a. Other common findings have been dermoids in 21%, ranula in 10%, and the remaining were inflammatory lesions. The thyroid tissue begins to descend from the foramen cecum anterior to the hyoid bone and laryngeal cartilages to lastly reach its regular adult pretracheal place. The proximal portion of the diverticulum that connects the thyroid gland and foramen cecum sometimes obliterates and atrophies over time. Other places embody the suprahyoid location in as much as 20% to 25% of the cases and at the stage of the hyoid in 15% to 50% of the circumstances. However, practically one-third of the instances occurred in patients of their third decade or older. Similarly, recent stories recommend a bimodal incidence with the most common common age in children to be 6 years and in adults to be 41 to 45 years. Indications for excision of a midline mass within the neck mass include diagnosis, cosmetic appearance, prior an infection, and possibility of malignancy. The Sistrunk process has been shown to lower the speed of recurrence to approximately 5%. The majority of the patients current with the historical past of a quickly enlarging midline mass in the neck and oftentimes report a history of a previous upper respiratory illness. Some may present with recurrent infections which were beforehand handled and improved on antibiotics. Patients may be completely asymptomatic or can have dysphagia, odynophagia, and a feeling of obstruction if severely enlarged. The mass is characteristically described as transferring with swallowing or protrusion of the tongue due to its attachment to the hyoid bone. Some sufferers could have a draining tract from the site of a prior incision and drainage, recurrence as a outcome of incomplete excision, or a ruptured cyst. Excision of ectopic thyroid gland with no functioning thyroid gland elsewhere will result in hypothyroidism. At instances, the presence of proteinaceous fluid can give a pseudosolid appearance, whereas prior an infection and hemorrhage might give a heterogeneous look. In the setting of prior an infection, there may be a thickened cyst wall, increased fluid attenuation, and loss of tissue planes. However, the diagnosis of carcinoma is often made by the way on histologic examination of pathology specimens following surgical excision. Primary care doctor for medical clearance when significant comorbidities present 2. Midportion or physique of the hyoid bone: A 1- to 2-cm part, depending on patient age/size, of the central portion of the hyoid bone is removed. Thyroid notch within the thyroid cartilage: this landmark can be used to mark the midline of the neck. Cricoid cartilage: In very young children, this might be fairly high in the neck and mistaken for the hyoid bone. Recurrence from incomplete resection � Goal of the surgery: Remove the cyst and any associated ductal remnants and secretory tissue. Intraoperative hemorrhage from the lingual artery � If the dissection within the tongue base strays from the midline, the lingual artery could also be encountered. Postoperative hematoma or infection � these problems may be mitigated by placing a drain. Pharyngocutaneous fistula � May end result from a breakdown of the closure of the tonguebase mucosa. The hyoid bone could be cut with a needle-tipped cautery in small children and bone cutter or hyoid scissors in bigger patients. Soft tissue attachments to the superior facet of the hyoid bone are left undisturbed. To accomplish this, the now free-floating part of hyoid bone is grasped with an Allis or Leahy clamp and pulled anteroinferiorly, and a cylinder of tissue on the base of the tongue is created via a superiorly aimed dissection with an insulated needle-tipped cautery. Exposure may be facilitated by using the first suture placed as a traction suture and slicing it after later sutures have been placed. The tongue is grasped with a perforating towel clip, and an assistant pulls the tongue anteriorly. The surgeon locations a protracted 18-Ga spinal needle via the pores and skin overlying the physique of the hyoid bone and advances the tip by way of the tongue mucosa on the foramen cecum. The stylet is removed and a #2 braided polyester suture is advanced through the needle, the top is grasped in the mouth with a tonsil clamp, and the needle is withdrawn. The traction suture is divided and the intraoral part removed by the anesthesiologist. The pharyngotomy is fastidiously closed in layers with interrupted absorbable suture over a Penrose drain. Pressure on the retractor brings the bottom of the tongue into the wound, facilitating the excision of the block of tissue on the foramen cecum. Dermal attachments or irritation could require removal of a fusiform section of overlying pores and skin. The cyst is elevated and a airplane is developed posterior to the body of the hyoid bone. B, the cyst is recognized, the strap muscular tissues are retracted, and the cyst is pedicled on the hyoid bone. The vallecula is entered posterior to the hyoid bone: Only a skinny layer of tissue might separate the mucosa from the posterior floor of the hyoid. The dissection might stray from the midline: Landmarks must be checked frequently. Too little tongue tissue could also be removed: � Surgeons have reported low recurrence charges with removal of solely a really restricted cuff of tissue above the physique of the hyoid. The strap muscles should be brought together medially to assist fill the useless house created by the loss of the midportion of the hyoid bone and the superficial delicate tissues. Routine pain management with acetaminophen, ibuprofen, and oxycodone may be began immediately. Placement of a traction suture to guide the tongue-base resection by way of the foramen cecum. Use of a traction suture to ship the upper part of the tongue base into the wound to improve exposure of the upper a half of the resection. When untreated, recurrent infections, fistulas to skin, and signs of obstruction from increasing size of the lesion can occur.
Syndromes
- Parasitic infections such as malaria
- Parkinson disease
- If your own tissue is being used to make your new ACL, your surgeon will make a larger cut. Then, your surgeon will remove this tissue through the larger cut.
- Suck on hard candies or throat lozenges. Young children should not be given such products because they can choke on them.
- Have you breathed in or swallowed any irritating substances?
- Location of the tumor
- Exercise tolerance test (stress test or treadmill test)
- Electrolyte abnormalities
Coumadin 2 mg buy discount line
Wound an infection or pin site infection-This is a comparatively common complication arrhythmia update 2014 coumadin 5 mg purchase with amex, which can be minimalized by adhering to strict pin site care heart attack in men purchase coumadin 1 mg fast delivery. For sufferers with very mild symptoms, watchful ready and residential monitoring may be thought of. In this technique, the mandible is uncovered with either an exterior or internal approach; osteotomies are carried out close to the angle of the mandible. Two transcutaneous pins are fixated on either facet of the osteotomy and secured to the exterior distraction gadget. Distraction and consolidation section care is just like the internal device method, except that the affected person must put on the exterior distractor during the consolidation part. Postoperatively, decreased costs have been also principally associated to decreased charges of inpatient pneumonia care and emergency room visits. However, the cost of hospital stay, residence nursing, home-care gear, hospital charges for subsequent tracheostomy evaluations, and elevated emergency department visits make tracheostomy an costly intervention when considering complete price per patient. As this is a relatively new software, dad and mom should be cautioned that there are restricted information on the long-term dental and orthodontic outcomes related to this procedure. However, the inverted-L osteotomy described above, should, theoretically, minimize the potential trauma to the molars. Data does help using mandibular distraction to improve both sleep apnea and dysphagia in sufferers with mandibular distraction. Readers ought to note that this chapter primarily focuses on internal distraction gadgets, that are utilized in a large number of centers. Mandibular distraction osteogenesis for the treatment of neonatal tongue-based airway obstruction. Tracheostomy versus mandibular distraction osteogenesis in Canadian youngsters with Pierre Robin sequence: a comparative cost evaluation. Economic benefits to a distraction choice tree model for management of neonatal upper airway obstruction. New surgical tools and techniques often provide elegant solutions to longstanding issues doubtlessly at vital increased price relative to current requirements of care. This is the first description of distraction osteogenesis rules to lengthen the mandible. Mandibular distraction to relieve airway obstruction in kids with cerebral palsy. Other indications embody a need for time for further re-evaluation (such as imaging) and/or when there shall be a delay in initiating definitive surgical remedy. This is done first to acquire a stat Gram stain to slender the antibiotic options as a substitute of starting double or triple remedy and, second, to discontinue or change the previously initiated antibiotics. This is more generally the case if the mucosal folds between the stapes, incus, and malleus restrict communication between the epitympanum and mesotympanum. Any secondary acquired (from perforation) or major acquired (from a retraction pocket) cholesteatoma growing on the posterosuperior quadrant will pose a better danger of ossicular erosion, listening to loss, extension to the attic and into the mastoid, and different problems. In an infectious situation the place number of the correct antibiotic as shortly as possible has important importance, accurate identification is secured by tympanocentesis or myringotomy. This process also narrows the spectrum of antibiotics by getting a stat Gram stain, which not only differentiates between gram positives and gram negatives but also factors to traits of the organisms that will help in narrowing down the probabilities, thus helping to determine the choice of antibiotic. To release the purulent effusion beneath pressure in the center ear, in the presence or suspicion of an otologic comuntil imaging is carried out and/ or the patient/ operating room/ surgical staff are ready, tympanocentesis or myringotomy should buy time and also lessen the danger for progression of complications until definitive remedy may be administered. In the absence of concern for a complication, the only justification is extreme pain and the goal of relieving it. Performing tympanocentesis or myringotomy safely requires nearly complete immobility of the affected person. This is achieved by restraining the kid with the assistance of oldsters or support workers. Additional restraint may be achieved through the use of a papoose or by swaddling a newborn or an infant with a sheet. Any sudden movement, even of some millimeters, can lead to inadvertent ear canal trauma and bleeding, making instrumentation even more challenging. Otitis Media, Myringotomy, Tympanostomy Tube, and Balloon Dilation within the Pediatric Population 1431 � When the patient and/or mother and father have beforehand experienced related procedures underneath restraint, it could be inconceivable to persuade them of the necessity of tympanocentesis or myringotomy. The use of phenol may pose a danger for spilling or spreading inadvertently and therefore could also be dangerous in a noncompliant youngster. Therefore the necessity and timing of those procedures may be adjusted in accordance with the circumstances. The choices are performing the process beneath basic anesthesia, with topical anesthesia, or with no anesthesia but potential analgesia. These decisions shall be made based on the indications, alternatives, risks, and the timeline of deliberate analysis and remedy. Based on the indications, situations, and limitations, one of many previously talked about options could also be most well-liked. Pars flaccida Short process Manubrium of Malleus Positioning � Supine: the affected person is positioned supine with the pinnacle turned away from the surgeon for each ear. It is important to determine the landmarks to be capable of carry out tympanocentesis or myringotomy in the correct location and to avoid problems. A, the speculum is held as shown for the proper ear for a right-handed surgeon; the third finger is placed within the concha to retract the pinna in the posterosuperior course so that the ear canal can be straightened with one hand. B, the speculum is held as proven for the left ear for a right-handed surgeon; the third finger is handed inferior to the speculum and positioned within the concha to retract the pinna in the posterosuperior path so that the ear canal could be straightened with one hand. D, To deal with the myringotomy knife, the thumb and index finger hold the handle whereas the third finger stabilizes the shaft of the knife, releasing up the fourth finger to be anchored on the speculum edge and the fifth finger to be anchored on the top if attainable. Instruments are held as described earlier, each fourth fingers anchored on the speculum and both fifth fingers anchored on the pinnacle for stabilization. Complications � Trauma to the exterior ear canal is normally because of inadequate restraint. Inadequate securing of the phenol bottle might end in spillage and a chemical burn at the spilled website. Initiation of antibiotic treatment without obtaining an effusion sample for culture and sensitivity is an choice. Similarly, more optimum pain management could obviate the need for tympanocentesis or myringotomy. When a long-lasting tube is inserted, at least half of the shaft of the T-tube is cut off. Holding the flanges straight with the alligator forceps, slowly release the forceps when the tips of the flanges are previous the incision in order to permit opening of the flanges in the different way. Secure the proper positioning of the angle of the tube and flanges for optimum operate and surveillance. A Rosen needle is usually needed to insert or align the flanges and the shaft within the desired course. B, Advancement of the guide catheter via the nasal passage is achieved after enough decongestion, with the steerage of endoscopes. D, A balloon is inserted to the extent of a yellow ring, and the pressure is elevated by inflating the special syringe to the specified stress for the specified duration. Whereas myringotomy/tympanocentesis is presently performed mainly for extra acute circumstances, tympanostomy tube insertion has, since its introduction within the Fifties, become the commonest outpatient surgical procedure in children.
Coumadin 5 mg buy discount
Because of the pharyngeal pouch element of a 3rd branchial anomaly blood pressure medication od generic 5 mg coumadin with amex, thymic tissue may be present within the cyst walls; some think about cysts of the third branchial pouch to be synonymous with thymic (thymopharyngeal) cysts hypertension knowledge test order coumadin 2 mg visa. Second Branchial Anomalies A second branchial anomaly may present as a cyst, sinus tract, or fistula tract. Isolated branchial cysts mostly originate from the second branchial system. On histopathologic examination, lymphoid tissue is characteristically discovered inside the cyst walls. Fourth Branchial Anomalies Fourth branchial anomalies likewise manifest solely as sinus tracts or cysts. An inner sinus tract arising from the apex of the pyriform sinus would pierce the cricothyroid membrane to enter the neck, theoretically coursing inferiorly and deep to the superior laryngeal nerve and superficial to the recurrent laryngeal nerve. This course would deliver the tract into close proximity to the superior pole of the ipsilateral thyroid gland. Given the anatomic course of third and especially fourth branchial anomalies, abscess formation or recurrent an infection of the thyroid gland should elevate suspicion of a 3rd or extra likely fourth branchial pouch remnant. An inside communication to the ipsilateral pyriform sinus should be dominated out in such instances. Particularly any medicines that would complicate anesthesia or increase the risk of hemorrhage 5. A history of alcohol and/or tobacco use is of significance in adults owing to the possibility of cystic cervical neoplastic metastases. A detailed examination of the ear is especially essential if there are any periauricular sinus tract openings. When and how did the anomaly first current (cervicofacial cutaneous opening, evident neck mass, or both) Has there been any evidence of secondary an infection such asfluctuationinsize,ache,orerythemaoftheoverlying pores and skin Has there been any proof of compromise to the aerodigestive tract, similar to dysphagia or stridor Previous surgical intervention such as needle aspiration or incision and drainage Bleeding disorders or antagonistic reactions to common anesthesia (in preparation for surgical excision) The ultrasonographic characteristics of a branchial cyst include uniform low echogenicity and lack of internal septation with no acoustic enhancement. Three-dimensional ultrasonography has been used to diagnose giant branchial cysts prenatally. It is particularly useful with respect to lesions within the parotid gland area to help outline the relationship of the mass to the facial nerve. Disadvantages include the comparatively excessive expense, study length, and frequent want for sedation and presumably general anesthesia in youngsters. If at all attainable, this should be prevented in order to stop disruption of the cyst wall and formation of fibrosis with a view to future excision. Patients are sometimes supine, and a shoulder roll and rotation of the head are often used to improve publicity. Antimicrobial coverage might need to be broadened within the event of a latest or concurrent an infection. Key Anatomic Landmarks � S eethesectionstitled"Preoperative Period"and"Surgical Technique. C, Contrast swallow examine revealing a communication from the left pyriform sinus into the neck. The aim of surgery for kind I first branchial anomalies is full excision of the sinus tract and/or cyst. The sinus tract may be outlined with a lacrimal probe or injection of methylene blue. Since sort I lesions are at all times superficial to the parotid gland, the parotid and temporalis fasciae serve as best landmarks with respect to the depth of excision. Superficial to these tissue planes, a cuff of sentimental tissue surrounding the sinus tract and cyst may be excised in a circumferential style toward the exterior ear canal. A shave excision of tragal or external ear canal perichondrium and cartilage is often necessary at the termination web site of the tract. The tract, doubtlessly demarcated as described for kind I lesions, is fastidiously dissected with a surrounding cuff of skin and gentle tissue towards the parotid gland. The superficial parotidectomy permits initial identification of the facial nerve trunk and subsequent clarification of the course of the tract relative to the branches of the facial nerve. A portion of the cartilaginous canal might should be excised to take away the tract completely. The wound is irrigated and the incision closed in a layered style, typically over a small suction drain. A cyst of suspected second branchial origin is managed similar to any isolated mass within the neck. An incision is positioned in a pores and skin crease both overlying or simply inferior to the mass. The cystic mass, as soon as clearly defined, is dissected in circumferential style, care being taken to keep away from disruption of the cyst. A large mass may profit from decompression utilizing needle aspiration to facilitate atraumatic removal. Oncethemasshasbeenremoved,thewoundisirrigated and the incision closed in a layered style, sometimes over a small suction drain. For sinus or fistula tracts of suspected second branchial cleft origin with a cutaneous opening, an elliptical incision is outlined across the website of the sinus/fistula. A cuff of connective tissue surrounding the tract is excised so as to make sure that every one epithelial components have been removed. The majority of second branchial cleft remnants are sinus tracts that finish blindly. An ipsilateral tonsillectomy is typically necessary in such instances to enable for sufficient entry to the pharyngeal communication in order that it can be closed. They are managed in equivalent fashion to second branchial cleft anomalies, with the important proviso of preparation for the potential for longer, deeper tracts following the embryologic anatomy described earlier on this chapter. Third and fourth branchial pouch anomalies pose a means more significant operative challenge. Historically these lesions have been approached through a lateral-tomidline curvilinear incision designed to permit adequate exposure of the ipsilateral facet of the laryngotracheal airway. Both the thyrohyoid (third pouch) and cricothyroid (fourth pouch) membranes must be recognized to decide the origin of the branchial pouch tract.
5 mg coumadin buy free shipping
Patient with Graves orbitopathy hypertension jama purchase coumadin 2 mg mastercard, optic neuropathy in the right eye arrhythmia powerpoint presentation order coumadin 2 mg with visa, visual acuity of 20/50 in the best eye, and Ishihara colour imaginative and prescient of 1. Indications � Urgent decompression throughout energetic phase of inflammation (for Graves): � Compressive optic neuropathy � Corneal ulceration � Elective decompression after the disease is quiescent (for Graves): � Proptosis � Sensation of strain or pain � Dryness of the eyes � Subluxation of the globe Contraindications � Active sinus an infection. Adequate medical or surgical administration of sinus an infection is critical earlier than orbital surgical procedure because of the risk of infection spreading to the orbital tissues. If an optic nerve decompression is planned at the similar time, navigation is helpful to establish the course of the optic canal and inside carotid artery. Strabismus surgical procedure could additionally be carried out for unresolved diplopia, and eyelid surgical procedure (either correction of retraction or blepharoplasty) could also be required after that. Drilling of bone must be along the axis of the optic canal to keep away from harm to the carotid artery. A relative benefit of performing the medial wall decompression first is that the orbital contents are beneath higher strain and herniation of orbital adipose tissue into the sinus cavity is facilitated with exterior orbital therapeutic massage. Orbital Decompression 1041 � the sphenoid sinus is opened, and the sphenoidotomy is maximally enlarged with Kerrison rongeurs. Residual septations are then removed in a posterior-to-anterior course along the cranium base. The nasofrontal recess is exposed, however additional dissection of the frontal sinus is pointless and should predispose to stenosis. Bone fragments are carefully elevated from the underlying periorbita with a Cottle elevator or ball-tipped probe. The bone on the junction of the medial and inferior partitions may be very thick and will require drilling. If the affected person is undergoing decompression for visual loss, extra bone is removed posterior to the entrance of the optic canal. The blade can be bent 30 degrees towards the orbit approximately 1 to 2 cm from the tip to provide a larger attain. Multiple parallel horizontal incisions (at least three) are made from the ethmoid roof to the floor of the orbit. Intervening strands of periorbita are cut to allow complete herniation of the orbital contents. Gentle external strain on the eyelids with the hand highlights remaining strands of periorbita and facilitates herniation of orbital adipose tissue into the ethmoid defect (Video 151. The periosteum should be elevated from both the interior and exterior surfaces of the lateral wall of the orbit. The bone should be identified as far superiorly because the fossa of the lacrimal gland and inferiorly to simply above the level of the zygomatic arch. Careful elevation along the exterior surface proceeds in a posterior path and then turns medially in the temporal fossa. Once the periosteum has been elevated from the bone, a large ribbon retractor is inserted between the periorbita and bone by an assistant. A reciprocating bone saw is used to minimize by way of the lateral wall, parallel to the zygomatic arch; the tip of the saw blade is positioned within the inferior orbital fissure, and the ostectomy is created from medial to lateral. Frequent pauses to assess the position and adequacy of safety of the orbital contents are essential. The second osteotomy is made just superior to the zygomaticofrontal suture with the tip of the noticed blade inside the orbit. It is necessary to have good publicity of the lateral wall externally to gauge the depth of the saw blade and avoid slicing into the anterior or center cranial fossa. It might be essential to elevate the remainder of the temporalis muscle from the posterolateral floor of the bone with electrocautery. Bone wax is utilized as needed, and any remaining small fragments of bone are eliminated with the same instrument. The sharp surfaces of the remaining zygomatic and frontal bones are smoothed with a burr or rongeur. Further bone could additionally be eliminated superiorly and inferiorly and posteriorly until the sphenoid bone begins to widen. A short-bladed knife, similar to a sickle knife, is now utilized to the periorbita in a really superficial manner, directed posteriorly to anteriorly, to slit the fibrous septa and permit the orbital contents to prolapse into the temporal fossa. Careful closure of the wound is achieved by exact realignment of the upper and decrease grey traces of the eyelid with a single horizontal sew of 6-0 absorbable material, such as polyglactin, buried laterally. The deep tissues are reapproximated with inverted 6-0 suture and the skin closed rigorously with running 7-0 nylon or interrupted chromic gut suture. Stevens or similar scissors are used to reduce the lateral canthal ligament and deepen the incision to bone. The periosteum is incised vertically along the apex of the rim with a scalpel or needle-tipped electrocautery. A Cottle elevator is then used to elevate the periosteum from the Common Errors in Technique � Preservation of the center turbinate limits expansion of the orbital contents and predisposes to synechiae. A speedy taper of oral steroid treatment is adequate for most patients; those decompressed in an acute setting require a a lot more aggressive routine and longer taper. One week after balanced decompression, visual acuity in the best eye was 20/25 and Ishihara colour vision was regular (17/18 plates). Complications � the dangers related to endoscopic medial and inferior orbital decompression are just like these after any endoscopic sinus surgery. Excessive elimination of bone at the posterior margin of the maxillary antrostomy can injure the descending palatine nerve, resulting in numbness of the palate. This must be recognized and managed expeditiously based on intraorbital pressures. It could additionally be essential to further detach the lateral canthal ligament and delay closure of the lid incision. Placing the noticed blade too deep can injure the dura and brain with the superior lateral wall osteotomy. The diplopia is usually transient but may require corrective surgical procedure if it persists past 6 months. Orbital Decompression 1043 Alternative Management Plan � Irradiation of orbital tissues � Some sufferers with shallow orbits and/or principally proliferation of orbital adipose tissue (more so than muscle) might profit from adipose tissue�only decompression of the orbits. A giant meta-analysis of research since 1990 confirmed a lower in proptosis of as much as 6 mm, with a form of balanced decompression (lateral and medial walls), with a 9% complication price. Decompression of only the lateral wall decreased the effectiveness of the decompression by 50% (about 3 mm). Surgically, the variety of decompressed partitions correlates directly with the discount in proptosis, and with a balanced medial and lateral wall decompression, the common discount in proptosis is between 4 and 5 mm. Errors in approach are usually related to incomplete and nonmaximal removal of the orbital bone, harm to the ethmoid arteries, or incomplete openings of the sphenoid or frontal sinuses that can turn out to be obstructed from the prolapsing orbital contents. Die Druckentlastung der Augenh�hle durch Entfernung der �u�eren Orbitalwand bei hochgradigen Exophthalmus (Morbus Basedowii) and konsekutiver Horn hauterkrankung.