
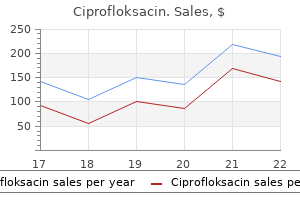
Ciprofloksacin dosages: 1000 mg, 750 mg, 500 mg, 250 mg
Ciprofloksacin packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Ciprofloksacin 750 mg generic overnight delivery
The anterior semicircular canals sense movements of your head because it moves towards your shoulder antibiotics zantac ciprofloksacin 1000 mg buy mastercard, while the posterior semicircular canals sense the movement when you transfer your head to nod "yes antimicrobial bath mat ciprofloksacin 250 mg discount free shipping. The utricle and saccule are answerable for mediating the sense of acceleration of your head in space, corresponding to in sudden motion or falling. Osseous Cochlear Labyrinth the osseous labyrinth has the appearance of a coiled snail shell ("cochlea" comes from the Greek word cochlos, that means "snail"). The cochlea coils out from its base near the vestibule, wrapping round itself two-and-fiveeighths occasions before reaching its apex. The core of the modiolus is continuous with the interior auditory meatus of the temporal bone, through which the vestibulocochlear nerve passes. In the erect human depicted in this figure the lateral semicircular canal mediates movement sensation within the horizontal plane, whereas the anterior semicircular canal will transduce data in the vertical dimension. The labyrinth is divided into two incomplete chambers, the scala vestibuli and the scala tympani, by an incomplete bony shelf protruding from the modiolus, the osseous spiral lamina. This essential construction forms the point of attachment for the scala media, which homes the sensory organ for listening to. The osseous spiral lamina turns into progressively smaller approaching the apex, such that the house between it and the other wall of the labyrinth will increase. At the apex the 2 chambers fashioned by the incomplete lamina turn into hook-like (hence the name hamulus), forming the helicotrema, the area by way of which the scala tympani and scala vestibuli communicate. The spherical window (foramen rotundum; fenestra rotundrum) supplies communication between the scala tympani and the middle ear. The oval window, upon which the stapes is positioned, permits communication between the scala vestibuli and the middle ear space. The cochlear canaliculus or cochlear aqueduct is a minute opening between the scala tympani within the area of the spherical window and the subarachnoid house of the cranial cavity. It is hypothesized that perilymph, the fluid that fills the scala vestibuli and scala tympani, passes by way of this duct, although this has not been demonstrated. To get a notion of scale, 1 mL is 1/1000 of a liter, and 1 �L is 1/1,000,000 of a liter. To summarize: � the inside ear homes the sensors for balance (the vestibular system) � � � � � and hearing (the cochlea). The osseous labyrinth is made up of the entryway to the labyrinth, the vestibule, the semicircular canals, and the osseous cochlear canal. The labyrinth is split into two incomplete chambers, the scala vestibuli and the scala tympani, by the osseous spiral lamina, an incomplete bony shelf protruding from the modiolus. The round window provides communication between the scala tympani and the middle ear area. Membranous Labyrinth the construction of the membranous labyrinth parallels that of the bony labyrinth. First, orient your self to the oval window, recognizing its hyperlink to the stapes of the middle ear. The vestibule or entryway to the inside ear is a space shared by the sense organ of hearing, the cochlea, and the sense organs of balance, the semicircular canals. The similar fluid flows by way of the entire membranous labyrinth, making steadiness and hearing intimately associated in each function and pathology. The cochlear duct forms solely a small portion of the membranous labyrinth and incorporates fluid of a barely totally different composition from that of the area surrounding the duct. The crista is the receptor organ for movement, being made up of ciliated receptor cells and a supporting membrane. From every of the 6,000 receptor cells protrude approximately a hundred stereocilia, minute hairs that sense motion in fluid, and one kinocilium. A cupola overlays the crista ampularis such that the cilia are embedded throughout the cupola. Within the vestibule lie the utricle and the saccule, housing for the otolithic organs of the vestibular system. The utricular macula is the sensory organ, which is endowed with hair cells and cilia. It is roofed by the otolithic membrane, which is invested with crystals (otoliths). The saccule lies near the scala vestibuli in the vestibule and is equally endowed with macula and otolithic membrane. The saccule and utricle talk via the endolymphatic duct, which is embedded in the dura mater. The cochlear duct creates the center area, and it houses the sensory equipment for listening to. This shelf programs the extent of the osseous labyrinth, forming the main point of attachment for the cochlear duct. Disruption of the blood supply to the cochlea, such as can happen during surgery for a cerebellar tumor, results in quick hearing loss, arising from reduced potassium output into the endolymph of the scala media (Mom, Chazal, Gabrillargues, Gilian, & Avan, 2005). The basilar membrane varieties the "ground" of the scala media, separating the scala media and scala tympani. The basilar membrane is extraordinarily thin, due to its position in supporting the touring wave. The outer three rows of hair cells, generally recognized as outer hair cells, are separated from the one row of internal hair cells by the tunnel of Corti, the product of pillar cells of Corti, also identified as rods of Corti. The vascular supply for the organ of Corti arises from the labyrinthine artery (which itself arises from the basilar artery). The cochlear department of the labyrinthine artery divides into between 12 and 14 "twigs" that serve the spiral lamina, basilar membrane, stria vascularis, and other cochlear buildings (Hackney, 2008). On the modiolar facet of the cochlear duct is found the spiral limbus, from which arises the tectorial membrane. The spiral sulcus undergirds the spiral ligament, perhaps offering stiffness to the basilar membrane (Raftenberg, 1990). The tectorial membrane overlays the hair cells and has practical significance within the processing of acoustic stimuli. The higher surface of each hair cell is graced with a sequence of approximately 50 stereocilia forming a slight "U" sample opened toward the modiolar aspect. There are three rows of outer hair cells, broadening to four rows within the apical end, numbering approximately 12,000. As with the internal cells, the stereocilia protrude from the surface of every outer hair cell, however with a "W" or "V" sample formed by approximately a hundred and fifty stereocilia. Shorter cilia are linked to the taller cilia by "tip hyperlinks," and cilia are additionally linked laterally, thus making certain that motion of one cilia involves disturbance of adjoining cilia on a hair cell. The internal hair cells are teardrop or gourd shaped, with a broad base and narrowed neck. Phalangeal processes apparently replace hair cells misplaced through acoustic trauma, thereby sustaining the delicate cuticular plate.
250 mg ciprofloksacin discount visa
Oral cancer typically ends in lack of oral buildings which might be invaded by cancerous cells antibiotic resistance washington post ciprofloksacin 1000 mg buy on-line, together with the mandible infection during pregnancy purchase 1000 mg ciprofloksacin with visa, maxilla, and tongue. A general rule is that removing of more than 50% of a structure will intervene with swallowing. Mandibular resection will typically result in poor bolus transit, and loss of dentition will interfere with bolus preparation (Logemann & Bytell, 1979; Pauloski et al. Glossectomy (removal of some or all of the tongue) certainly interferes with swallowing, however sufferers can often study compensatory actions. If the oropharynx is ablated, the individual will doubtless have sensory issues with initiating the swallow due to harm to the tissues. The risk of dysphagia increases dramatically if glossectomy includes the tongue base (Zuydam, Rogers, Brown, Vaughan, & Magennis, 2000). Generally, if the epiglottis is involved in the surgical procedure, the probability of dysphagia increases dramatically. If the patient has a hemilaryngectomy (removal of left or proper aspect of the larynx), the chance of a secure swallow will increase if the superior and recurrent laryngeal nerves are preserved. Radiotherapy of the top and neck causes fibrosis of the tissue, making it inelastic. Chemotherapy weakens musculature, but the patient usually will get well operate. Chapter Summary Mastication and deglutition may be seen behaviorally or as a system of reflexive responses. The behavioral stages of mastication and deglutition embody the oral (oral preparatory and oral transport), pharyngeal, and esophageal stages. In the oral preparatory stage, meals is launched into the oral cavity, moved onto the molars for chewing, and blended with saliva to type a concise bolus between the tongue and the hard palate. The soft palate and larynx elevate, and the bolus is propelled via the pharynx to the higher esophageal sphincter, which has relaxed to receive the fabric. The tongue contacts the posterior pharyngeal wall, growing pharyngeal stress and driving the bolus into the open, awaiting esophagus. The epiglottis has dropped to partially cowl the laryngeal opening, whereas the intrinsic musculature of the larynx has created a good seal to defend the airway. Sensory components of mastication and deglutition are important for the elicitation of the muscular components of chewing and swallowing, as nicely as the upkeep of the varied qualities of those processes. Taste sensors are specialized for sweet, sour, salty, bitter, and umami taste senses. Taste sense determines whether or not a bolus is ingested or faraway from the oral cavity. Oral chemesthesis refers to detection of chemical substances by means of ache and thermal sensors within the oral cavity, and stimuli eliciting these responses may be used to facilitate swallowing responses. The tactile sense (sense of touch) is mediated by mechanoreceptors that respond to deep or shallow touch. Four lessons of thermal stimulation are differentiated by human senses: warm, scorching, cool, and chilly. Pain sense (nociception) is a response to a noxious stimulus, and acts as a protecting response in opposition to the inappropriate entry of overseas objects into the gastrointestinal system. Muscle stretch is sensed by muscle spindle fibers, and muscle pressure is sensed by Golgi tendon organs, found within tendons and fascia. The sort of saliva produced varies by gland; the sublingual gland produces thick mucus secretions, the submandibular gland produces both skinny serous and mucus secretions, and the parotid gland secretes solely serous saliva. The chewing reflex involves rotatory motion of the mandible, coordinated with the movement of bolus by the tongue. The sucking reflex, which supports the developmentally earlier suckling response, is elicited by gentle contact with the inside margin of the lips and causes protrusion and retraction of the tongue, in addition to closing of the lips. The uvular elevation of the palatal reflex occurs in response to the tactile stimulation of the faucial pillars, lingual tonsils, or higher pharynx. The gag reflex is elicited by the tactile stimulation of the faucial pillars, posterior faucial wall, or posterior tongue near the lingual tonsils. Respiration happens due to inadequate oxygenation of or excessive carbon dioxide within the blood or blood acidity. List 5 of the elements of the oral preparatory stage of mastication and deglutition. The reflex includes orienting toward the course of tactile stimulation to the cheek. The reflex is elicited by delicate contact with the lower lip and ends in tongue protrusion and retraction. List two essential differences between the oral-pharyngeal anatomy and physiology of an toddler and that of an adult. The stage is the stage by which food is ready for a swallow. The stage is the stage of swallow involving the oral transit of the bolus to the pharynx. The stage is the stage of swallow involving the transit of the bolus to the esophagus and consists of numerous physiological protecting responses. The stage is the stage of swallow during which food is transported from the upper esophageal region to the abdomen. Taste from the anterior two-thirds of the tongue is mediated by the cranial nerve (name and number). Taste from the posterior one-third of the tongue is mediated by the cranial nerve (name and number). Taste from the epiglottis and esophagus is mediated by the cranial nerve (name and number). The style of bitterness is predominantly transmitted by the cranial nerve (name and number). The style of sweetness is predominantly mediated by the cranial nerve (name and number). The tastes of sourness and saltiness are predominantly mediated by the cranial nerve (name and number). Oral chemesthetic sensations are mediated by the cranial (nerve and number). Cells with endings sense stretch throughout the deep layers of the epithelium. The parotid glands launch (type of saliva) into the posterior oral cavity and pharynx. The sublingual glands release (type of saliva) into the anterior oral cavity.
Safe 250 mg ciprofloksacin
Firing pattern of human genioglossus motor units throughout voluntary tongue movement virus that causes cervical cancer cheap ciprofloksacin 250 mg overnight delivery. An investigation of compensation and adaptation to auditory perturbations in people with acquired apraxia of speech virus encrypted files purchase ciprofloksacin 750 mg fast delivery. Functional identification of the perioral neuromuscular system: A signal move diagram. The components of regular motion in the course of the first yr of life and abnormal motor motion. Systematic analysis in experimental phonetics: A theory of the speech mechanism as a servosystem. Lip and jaw motor control during speech: Responses to resistive loading of the jaw. Movements of the upper and decrease lip throughout speech: Interactions of the lips with the jaw fastened at totally different positions. Neural modeling and imaging of cortical interactions underlying syllable manufacturing. A theoretical investigation of reference frames for the planning of speech movements. A child with signs of developmental apraxia of speech with whom a palatal raise prosthesis was used to manage palatal dysfunction. Anticipatory coarticulation in the speech of adults and younger children: Acoustic, perceptual, and video data. Functionally particular articulatory cooperation following jaw perturbations during speech: Evidence for coordinative buildings. The problem of flexibility, fluency, and speed-accuracy trade-off in expert habits. An examination of the levels of freedom of human jaw movement in speech and mastication. Distinct representations of phonemes, syllables, and supra-syllabic sequences in the speech production network. Mandibular motor management through the early improvement of speech and nonspeech behaviors. Acoustic and articulatory options of diphthong manufacturing: A speech clarity research. Development of vocal tract length throughout early childhood: A magnetic resonance imaging study. Anatomic improvement of the oral and pharyngeal parts of the vocal tract: An imaging study. Developmental sexual dimorphism of the oral and pharyngeal portions of the vocal tract: An imaging study. Reflex responses in human jaw, lip, and tongue muscle tissue elicited by mechanical stimulation. A kinematic description of the temporal traits of jaw motion for early chewing: Preliminary findings. Humans have done a fabulous job of taking the anatomical buildings and their physiology and capitalizing on these functions for speech. In some ways, the physiology of mastication (the process of preparing food for swallowing, also called chewing) and deglutition (the processes of swallowing) offers an beautiful view of those built-in techniques we use so effortlessly in speech. As we talk about these very fundamental and elementary processes, you will notice how we invoke the respiratory, phonatory, articulatory, and nervous methods. Furthermore, keep an eye fixed on the Clinical Notes we provide in bins to see just how problematic it could be when the anatomy and physiology of any one of these methods is disrupted. Deglutition refers to swallowing, which is a fancy process of transferring the bolus into the pharynx and propelling it into the esophagus. These two biological processes require the combination of lingual, velar, pharyngeal, and facial muscle motion (see Chapter 7) with laryngeal changes (see Chapter 5) and respiratory control (see Chapter 2). All intrinsic and extrinsic muscle tissue of the tongue are referred to as into motion to move the food into place for chewing and preparation of the bolus (either liquid or a mass of food) for swallowing. We have lengthy recognized that feeding expertise are both preparatory and supportive of the speech act, and insufficient development of feeding displays instantly on speech growth. In this text, we first discuss developmental and grownup mastication and deglutition patterns as they relate to the underlying anatomy and physiology, after which we focus on the neuroanatomical underpinnings of these processes in an try and integrate these important capabilities with their management mechanisms. Articulator perform measures of force are the same as those mentioned in Chapter 7, but in this context they could signal the potential for swallowing deficit. Remember that the articulators have the first accountability of mastication, and that speech is a secondary pursuit. To look at the advanced kinematics of oral and pharyngeal constructions, researchers depend upon visualization methods that end in three-dimensional representations, similar to multi-slice computer-aided tomography. These limitations are more than made up for by the fact that the clinician or researcher can instantly detect aspiration and more precisely assess pharyngeal residue. A final tool is ultrasound, which also provides a way of observing motion during swallow, although the presence of bone impedes visualization. Anatomical and Physiological Developmental Issues As we mentioned in Chapter 7, maturation of the infant nervous system provides a secure base of trunk, neck, and head upon which mastication and deglutition are developed. The maturation process of the bodily and physiological methods units an essential stage for the adult swallowing perform. It has been observed as early as 10 weeks gestational age, and most fetuses display nonnutritive sucking by 15 weeks; suckling is stimulable at this point in growth as nicely. The infant positive aspects vitamin by way of the rooting reflex (Glodowski, Thompson, & Martel, 2019), which entails orienting towards the course of tactile contact with the mouth area (perioral region). In the first 6 months of life, this reflex is manifest as a suckling sample, which is the piston-like motion of the tongue (Arvedson & Brodsky, 2002). This sample is replaced by sucking, a extra complex process in which the tongue raises and lowers, which, in combination with stronger labial seal, causes a negative stress that attracts liquid into the mouth. This growth is dependent on the increased dimension of the oral cavity, which permits the superiorinferior movement of the tongue. Although both suckling and sucking are supported by mandibular movement, the sample of the tongue motion and diploma of lip occlusion are the primary variations. Nonnutritive suckling experiences are gained by use of pacifiers, which assist the toddler arrange the oral habits. Early on, infants could take up to three sucks before swallowing and have an apneic interval between suck�swallow runs (Arvedson & Brodsky, 2002). As the infant develops, the ratio of sucks to swallows moves from 3:1 to 1:1, with respiration occurring after between 10 and 30 suck�swallow sequences (Arvedson & Brodsky, 2002; Lau, Smith, & Schanler, 2003). If you look intently at these figures, you want to notice that there are marked variations between these two techniques. The larynx is markedly elevated at birth however descends over the course of the primary 4 years. An absent or weak suckling reflex requires intervention by a feeding specialist who might help to stimulate it, and different forms of nutrient intake may be required until the reflex is established. This reflex is elicited by the tactile stimulation of the lips and perioral space, as properly as via the visual presentation of a meals source in older infants (Miller, 2002), and entails protrusion of the tongue with sufficient pressure to initiate the flow of milk from the breast.
Purchase ciprofloksacin 750 mg with mastercard
During charging antibiotic resistant gonorrhea 2015 generic ciprofloksacin 750 mg without prescription, the system continues to monitor individual beats and label them as "T" or "S bacteria growth temperature order ciprofloksacin 750 mg on-line," but now particular person intervals myopotentials, Twaves, and Rwave double counting. The ventricular rate is determined continuously by calculating the average of the last 4 certified beats. As lengthy as this is below the therapy zone(s), those beats will be labeled "S" (denoting sensed beats). Once the average fee is larger than the programmed threshold, tachycardia is asserted within the shock zone and a tachycardia detection counter (referred to as the "X counter") might be superior. For average charges within the conditional zone, mor phological evaluations are carried out on each beat, and beats deemed treatable might be labeled with "T" and the tachycardia detection counter might be incremented. The gadget makes use of a rolling 24 certified beat buffer to determine the X Counter Value. In gen eral, as treatable or "T" beats enter the 24 certi fied beat buffer and "S" beats exit the 24 beat buffer, the X Counter is increased. At the onset of tachycardia detection, the first certified treatable beat (T) will seed the X Counter to a value of 5 to account for the averaging of the last 4 inter Tachycardia Counter 18 counts of T Intervals using the counting guidelines of the 24 certified beat buffer = tachycardia detection Persistence Criteria Nominal Value is 2 Each consecutive T beat advances the counter. Shock Confirmation Shock Confirmation threshold (dynamic � it adjusts primarily based on T and S beats during charging) should equal Shock Confirmation quick interval counter by or after the top of cost. The yellow space denotes the 18 tachycardia (treatable) intervals (marked by T) that resulted in satisfaction of the initial criteria. The blue, green, and purple areas mark the prolonged analysis of the arrhythmia due to persistence. In this example, persistence has been increased to 11 because of three previous nonsustained occasions. Following this event, the persistence value will further increase to 14, further lowering the danger for inappropriate shocks and unnecessary cost cycles. This threshold defines the variety of consecutive quick intervals that have to be met on the end of the cost cycle. Redetection in the conditional zone, all morphologybased discrim ination nonetheless applies. Episode end shall be declared if any of the following happen: 1 Twentyfour consecutive intervals extra the forty ms slower than the therapy zone. Programming Redetection follows the identical roles as preliminary detection with the exception that the preliminary duration criteria are 14 rather than 18. As most algorithms are preset, the principle choices left to the practitioner are selecting between one or two ther apy zones and setting the edge rate for each of them. All intervals are fast and meet the "treatable" necessities, and subsequently labeled "T. Detection in this zone is outlined solely by the number of certified intervals above the set threshold. In this zone, arrhythmia discrimination algorithms are energetic and are carried out in a stepwise method. Poorly matched morphology will be further evaluated using a dynamic waveform evaluation that checks for uniformity. Consecutive beats are in contrast with each other, and if deemed to be polymorphic they will be labeled "T. The "dose" is a operate of the frequency of resynchronization pacing and of the effectiveness of each resynchronized beat. The impact of those parameters, and their optimization, is reviewed in Chapter 2 (Hemodynamics of Cardiac Pacing), and briefly mentioned within the following. Lastly, optimized resynchronized pacing must be delivered practically constantly (>92�98%)98 in order to have a clin ical impression. The elevated fre quency of ventricular pacing has a minimal effect on the average heart fee. The latter issue is important, as a outcome of inappropriately rapid pacing itself could depress ventricular systolic function. Bottom: hospital telemetry shows pacing throughout quickly conducted atrial fibrillation because of an algorithm designed to maximize cardiac resynchronization pacing. Randomized con trolled study of detection enhancements versus rateonly detection to stop inappropriate remedy in a dual chamber implantable cardioverterdefibrillator. Optimizing implantable cardioverterdefibrillator treatment of rapid ventricular tachycardia: antitachycardia pacing remedy during charging. Prevention of inappropriate therapy in implantable cardio verterdefibrillators: outcomes of a prospective, randomized research of tachyarrhythmia detection algorithms. Dual chamber versus singlechamber detection enhancements for implantable defibrillator rhythm analysis: the detect supraventricular tachycardia study. Underdetection of ventricular tachycardia by algorithms to enhance specificity in a tieredtherapy cardioverterdefibrillator. A trial design for analysis of empiric programming of implantable cardioverter defibrillators to improve affected person administration. This is mentioned additional in Chapter 2 (Hemodynamics of Cardiac Pacing: Optimization and Programming to Enhance Cardiac Function). With a thor ough understanding of device operation perform, it could certainly be optimized to provide lifeprolonging therapy with minimal morbidity. Effect of failed defi brillation shocks on electrogram amplitude in a noninte grated transvenous defibrillation lead system. Differences in tachyarrhythmia detection and implantable cardioverter defibrillator therapy by major or secondary prevention indication in cardiac resynchronization therapy sufferers. Optimal combination of discriminators for differentiating ventricu lar from supraventricular tachycardia by dualchamber defi brillators. Combined use of morphology discrimination, sudden onset, and stability as discriminating algorithms in single chamber cardioverter defibrillators. Discrimination of ventricular tachycardia from sinus tachycardia and atrial fibrillation in a tieredtherapy cardioverterdefibrillator. Underdetection of ventricular tachycardia by algorithms to improve specificity in a tiered therapy cardioverterdefibrillator. Enhanced detection criteria in implantable cardioverter defibrillators to avoid inappropriate remedy. Preliminary clinical expertise with the first twin chamber tempo maker defibrillator. Clinical expertise with the model new detection algorithms for atrial fibrillation of a defibrillator with twin chamber sensing and pacing. Ventriculoatrial con duction in sufferers with implantable cardioverter defibril lators: implications for tachycardia discrimination by dual chamber sensing. Ventriculoatrial conduction capability and prevalence of 1:1 retrograde conduction throughout inducible sustained monomorphic ventricular tachycardia in 305 implantable cardioverter defibrillator recipients. Discrimination between ventricular and supraven tricular tachycardia by twin chamber cardioverter defibril lators: importance of the atrial sensing perform.
Buy ciprofloksacin 250 mg fast delivery
Note the the vertebrobasilar supply arises from the paired vertebral arteries anastomosing to turn out to be the basilar artery bacteria zar buy ciprofloksacin 1000 mg on line. The vertebrobasilar supply branches to turn out to be the posterior cerebral arteries and cerebellar arteries light antibiotics for acne 1000 mg ciprofloksacin discount amex. The internal carotid supply arises from the internal carotid artery, and serves the middle and anterior cerebral arteries. The circle of Willis offers a way of equalizing pressure, in addition to offering redundant vascular supply within the case of cerebrovascular accident. Regions of lateral and medial cerebrum served by the interior carotid and vertebrobasilar provide. Note that the middle cerebral artery serves the entire language, speech and hearing territory. The medial cerebral cortex is served predominantly by the anterior cerebral artery, with the occipital lobe being served by the posterior cerebral artery of the vertebrobasilar system. The venous system is the system of blood vessels referred to as veins that provides the technique of draining carbon-dioxideladen blood to the lungs for reoxygenation. Venous drainage is accomplished via a sequence of superficial and deep cisterns. Superficial drainage empties into the superior sagittal sinus and transverse sinus. Deep drainage is by means of the inferior sagittal sinus, the straight sinus, transverse sinuses, and the sigmoid sinus. Blood returns to the final bloodstream via the jugular veins, and spinal wire drainage is via radicular veins. A thrombus is a international body (such as a blood clot or bubble of air) that obstructs a blood vessel, and such obstruction is called a thrombosis. If the thrombus breaks free from its web site of formation and floats via the bloodstream, it becomes an embolus, or floating clot. An embolism is an obstruction of a blood vessel by that international physique delivered to the point of occlusion by blood circulate. When an intracranial aneurysm ruptures, the blood is launched into the house surrounding the brain, generally as a end result of most aneurysms occur in arteries rather than capillaries. The strain associated with both the development of the ballooning aneurysm and the sudden launch of blood into the cranial cavity is life-threatening, with websites of neural harm being associated to the situation of the rupture. Occlusion of the anterior cerebral artery is infrequent, however could lead to hemiplegia, lack of some sensory function, and personality change. Occlusion of the center cerebral artery is the most typical and can end result in severe disability due to the important nature of the areas served. Posterior cerebral artery occlusion produces variable deficit that may include reminiscence dysfunction. The circle of Willis is a collection of communicating arteries that provides redundant pathways for blood flow to areas of the cerebral cortex, equalizing strain and move of blood. A foreign body throughout the blood vessel (thrombus) creates an obstruction to blood circulate (thrombosis) or becomes an embolus when released into the bloodstream. An aneurysm is a ballooning of a blood vessel, and rupture of an aneurysm leads to blood being released into the area of the brain. The middle cerebral artery is the most common web site of occlusion; the end result could additionally be significant language and speech deficit if the occlusion includes the dominant cerebral hemisphere. Cerebellum the cerebellum is the most important element of the hindbrain, resting throughout the posterior cranial fossa, instantly inferior to the posterior cerebral cortex. The cerebellum is the heavy hitter of the nervous system when it comes to neurons: While the cerebral cortex is residence to 18 billion neurons, the cerebellum has sixty nine billion neurons, which is 80% of the entire number within the brain (Azevado et al. Needless to say, this neuron density speaks to the important nature of the cerebellum as an integration middle. The cerebellum is answerable for coordinating motor instructions with sensory inputs to management motion, and it communicates with the brain stem, spinal wire, and cerebral cortex by means of superior, center, and inferior cerebellar peduncles. The cerebellum additionally performs a major role as reminiscence for motor function and even cognitive processing (Akshoomoff & Courchesne, 1992). It has connections with the limbic system, reticular activating system, and cortical affiliation areas; and medical studies of individuals with cerebellar lesions verify its function in cognitive govt perform and reminiscence. From behind, one can see that the cerebellum is composed of two hemispheres and is prominently invested with horizontal grooves. The anterior lobe is often referred to as the superior lobe, and the middle lobe is known also because the inferior lobe. The vermis separates the two hemispheres and aids in defining the intermediate and lateral cerebellar areas of the posterior floor. The anterior surface reveals the third lobe of the cerebellum, the flocculonodular lobe, made up of the best and left flocculi and central vermis: L. The prominent center cerebellar peduncle is between the superior and inferior cerebellar peduncles. The flocculonodular lobe is functionally referred to because the vestibulocerebellum (or archicerebellum), whereas the spinocerebellum (or paleocerebellum) is the anterior lobe and the portion of the posterior lobe related to the arm and leg. The posterior lobes and the intermediate vermis make up the neocerebellum (or pontocerebellum). At the center of the white fibers is a sequence of nuclei serving as relays between the cerebellum and the speaking regions of the physique. The outer molecular layer incorporates basket, stellate, and Golgi cells (not proven in figure), and the intermediate layer accommodates Purkinje cells. Purkinje cells are large neurons forming the boundary between the molecular and granular layers of the cortex. Excitation of a Purkinje cell causes inhibition of the nucleus with which it communicates. Golgi cells project their dendrites into the molecular layer and their axons into the granular layer. Their soma obtain enter from both climbing fibers and Purkinje cells, and the axons synapse with granule cell dendrites. Climbing fibers arising from the inferior olivary nuclei pass via the inside granular layer to communicate with the Purkinje cells. Granule cells within this inside layer project axons to the outer layer where they divide right into a T-form. The branches course at roughly proper angles to the bottom of the axon, synapsing with the dendritic arborization of the Purkinje cells. Activation of those granule cells excites basket and stellate cells but inhibits Purkinje cells. Projections from non-cerebellar regions (spinal cord, mind stem, cerebral cortex) terminate in mossy fibers. Projections from this nucleus route by way of the superior cerebellar peduncle to synapse in the ventrolateral nucleus of the thalamus and from there ascend to the cerebral cortex by the use of thalamocortical fibers.
250 mg ciprofloksacin order otc
The first four years reveal extraordinarily speedy development oral antibiotics for acne doxycycline purchase 250 mg ciprofloksacin with visa, but that tapers off in all circumstances antibiotic 4 days ciprofloksacin 250 mg cheap amex. As you examine these figures, also discover the distinction between men and women in this development: There is a striking divergence between vocal tracts at puberty (around 11 years). During the first 24 months of life, the onerous palate will increase nearly 1 cm in length, while the velum will increase solely about 0. Males are represented by the open circles and darkish dashed development line, females by the triangles and solid trend line. Notice that the most speedy development occurs between delivery and 4 years, with one other improve within the 12- to 16-year range. Notice the speedy enhance in vocal tract size distinction starting at puberty (around 11 years). Males are represented by the open circles and dashed pattern line, while females are represented by the triangles and stable pattern line. Note that the rate of growth plateaus at around 4 years of age however increases once more between 12 and sixteen years. Development of the pharyngeal house is a big contributor to total vocal tract size. Top: Length of the horizontal vocal tract (lips to pharyngeal wall, identified within the figure as Vocal tract-oral distance) as a operate of age. Males are represented by the open circles and dashed pattern line, and females are represented by the triangles and strong development line. Notice that development patterns for the vocal tract are basically the same for males and females, with the best development between start and four years. Notice that males have higher growth than females between 4 and 6 years, and then present the pubertal increase over females beginning round 11 years. It ought to now be pretty clear that the maturation of the motor speech system governs, in massive part, the speech sounds a baby is capable of making. A child of 2 or three years of age is quite able to the basic valving motion of opening and closing the mouth (/ba/), and raising and decreasing the tongue on the alveolar ridge (/da/) or near the velum (/ga/). However, managed manufacturing of the stops requires the power to differentiate labial, mandib- t ular, and lingual movements, and thus, mastery of the stops might occur as late as 6 years. The "raspberry" you hear in the preverbal baby is very probably the precursor to the fricatives that develops later. With graded management of lingual strain comes the flexibility to make minute changes of an articulatory posture, corresponding to these made with the dorsum of the tongue to differentiate /s/ and // by way of widening of the tongue groove and tongue tip elevation. The depth of the mandible increases to accommodate the tongue, producing a steady improve within the oral cavity dimension. The tongue undergoes a similar progress, filling the area created by the expansion of the mandible, and attaining about 75% of adult measurement by 7 years. We see a corresponding fee of descent of the larynx (about three cm of drop over the 7-year period), in addition to of the hyoid (about 2 cm). The first line characterizes the fast development between delivery and 1 to 2 years of age, whereas the second line characterizes the extra steady growth through the subsequent interval. Needless to say, these adjustments have a big influence on the resonant characteristics of the vocal tract throughout speech, and an actual impact on mastication and deglutition. To summarize: � A neonate is decided by reflexive responses for protection and to meet fundamental needs. Tongue size exhibits a rapid improve through the first 12 months of life and then reaches 73% of adult dimension by 7 years. Mandibular depth and length show a more regular increase in size over the identical time interval, reaching 90% of grownup dimension by 7 years. Note that the blue triangles characterize males and the red, upward pointing triangles denote female participants. Coordinated Articulation Theories of motor management for speech have undergone a great deal of evolution but are centered typically around the notions of locus of management, the necessity for consistency for the motor act, and task specification. Consider the next hierarchical elements of speech, as implied by MacKay (1982). Within the initial, conceptual system, we should first develop the proposition, or thought to be expressed, and that concept represents the sentence to be spoken. This idea or proposition should be mapped into a syntactical system to set up the language varieties acceptable to match the concept, and acceptable phrases must be chosen to match the syntax and to match the proposition. Thus, if the concept "Tomorrow is Monday" is the chosen proposition, the syntax for that proposition must be chosen, and the words chosen to match the syntax and the proposition. In the phonological system, syllable construction is parsed from the lexical alternatives. Phonological rules are applied to establish the right phoneme combinations to meet the needs of the phrases chosen previously, and the person features of these phonemes are parsed from the phonological specs. Thus, on the phonological system stage, the chosen phrases ("Tomorrow," "is," "Monday") are further broken into syllables, chosen phonemes, and options for the phonemes. For occasion, the /t/ in "tomorrow" is outlined as lingua-alveolar, stop, and voiceless. Note that, all through all of this, there was no point out of muscular tissues of articulation. In the muscle movement system, muscles are activated to meet the needs of the characteristic selection course of. The /t/ of the phonological system was broken into options, such as lingua-alveolar, and that is now translated into the motion of the muscle tissue of the tongue that will produce that linguaalveolar gesture (such because the superior longitudinal and genioglossus muscles). By this principle, the associated chain principle, the manufacturing of /t/ required only that the speaker be taught the entire motor sequences leading as much as elevation of the tongue to the alveolar ridge, the broadening and tensing of the tongue to produce a seal, the retraction of the tip to launch the /t/, and then motion to the following phoneme. We may hyperlink a sequence of reflexive actions and entrain them in a sequential activation sample. Once the motor act was discovered, the speaker would forever be prepared to produce a word with /t/ in it. Future theories would have to account for the fluidity of speech production, the inherent variability of articulation based on context, and the flexibility of the articulators to achieve their phonetic goal regardless of unpredictable alteration of the context of the production. In probably the most extreme case, the command system could be oblivious to the state of the articulators at any second and would administer the muscle instructions with out regard for the articulator circumstances of the second. The great factor about such a model is the direct entry that the motor system has to the language processor. Individual phonemes can be represented by a burst of neural excitation, so that the plan for a /t/ could be expertly executed with devoted precision. This mannequin elegantly addresses a major drawback: the articulatory act for any phoneme requires precise activation of an overwhelming number of neurons and muscle fibers, and the activation have to be correct, well timed, and result in right motion. Thus, simply activating a program that your brain is aware of will produce a /t/ is way simpler than having to micromanage your articulatory system.
Ciprofloksacin 500 mg cheap amex
The tensile energy of the fibrous tissue is often larger than that of the vessel or cardiac wall antibiotic resistance reversal ciprofloksacin 250 mg, leading to antibiotic resistance lab activity ciprofloksacin 250 mg buy line shearing or avul sion with software of extra drive. Similarly, in leads with low tensile energy, any signal of separation of the lead or insulation harm ought to immediate cessation of straightforward traction. Removal of the lead without helix retraction is more of a priority in the atrium, the place the wall is considerably thinner. If traction fails, our subsequent strategy is to transect the lead just beyond the connector pin in a nonisodiamet ric portion of the lead, attempting to go away as a lot as pos sible with which to work. A locking stylet placed in the internal conduction coil is used to maintain lead integrity and transmit traction forces to the lead tip. In the unique Cook locking stylet, after the lead was sized and the appropriately sized locking stylet chosen, the stylet was advanced as far as possible, ideally the length of the lead, and counterclockwise turning of the stylet "locked" it into place (left panel). The lead is passed via the loop at the end, and a steel sleeve passed over the lead to lock it. We also advocate tying a securing suture to the outer insulation and main it back by way of the loop in the locking stylet, particularly when operating through a sheath the place at the initial levels the lead could not be capable of be grasped instantly. This aids in inserting pressure along the whole lead rather than just on the inner or outer parts. This is assumed to cut back the chances of "snowplowing" or tearing of the insula tion, which can make the passage of sheaths tough. The subsequent step is usually the development of nonpow ered telescoping sheaths over the lead, which acts as a rail. Countertraction is applied to the sheath as traction is being applied to the result in break adhesions at every binding site. Adequate traction on the lead and coaxial alignment of the sheath over the lead ought to be maintained to maxi mize the elimination of fibrotic adhesions and decrease trauma to vascular constructions. Inadequate traction may find yourself in the sheath passing outside the line created by the lead itself and laceration of cardiovascular buildings. If countertraction using nonpowered sheaths is unsuccessful, powered sheaths are used. Powered sheaths have suggestions that can minimize through fibrous tissue, which considerably reduces the amount of traction and countertraction wanted to extract the lead. The electro surgical dissection sheath makes use of radiofrequency power from two tungsten electrodes on the tip of a Teflon sheath. Because the dissection airplane from the radiofre quency energy is restricted to a small arc along the radius of the sheath, catheter rotation may be required to free the lead circumferentially. Use of electrosurgical dissec tion sheaths has been related to similar success rates to the laser sheath. Both sheaths use an outer sheath for support, countertraction against the endo cardium, and serve as a work station. If bunching of insulation or "snowplowing" is assumed to be the issue, upsizing to a bigger French sheath is commonly useful. The Evolution sheath has a handletriggerdriven, stainlesssteel treaded barrel rotational tip at the end of a versatile sheath designed to drill via fibrosis, calcification, sleeve, and suture material. Approach to extraction nearly all of leads are extracted through the vein by way of which the lead was implanted. Lead extraction using multiple venous access websites, such as the interior jugular vein and vein of implantation, have also been described. Because traction is utilized from an inferior method, the femoral strategy is believed to have lower propensity for perforation, venous tear, and cardiac avulsion. There are numerous instruments at present out there for femoral lead extraction, together with the Byrd Femoral Workstation (Cook Medical). If the lead tip has been freed, the femoral venous sheath is positioned in the proper atrium. The free end is snared in the proper atrium or in the inferior vena cava after pulling the lead into the inferior vena cava. If the lead tip remains to be connected to the endocar dium, the femoral venous sheath is positioned in the best atrium and a loop of the lead is snared and introduced into the sheath. The proximal finish is amputated and the lead tip freed with traction and countertraction. Prospective examine of axillary vein puncture with or with out contrast venography for pacemaker and defibrillator lead implanta tion. Prospective rand omized comparability of the protection and effectiveness of placement of endocardial pacemaker and defibrillator leads utilizing the extrathoracic subclavian vein guided against this venography versus the cephalic strategy. Safety and efficient ness of placement of pacemaker and defibrillator leads within the axillary vein guided in contrast venography. A new trick to a routine process: tak ing the concern out of the axillary vein stick utilizing the 35� cau dal view. Clinical expertise of distinction venography guided axillary vein puncture in biventricular pacing R1. A new approach to percutaneous subclavian venipuncture to keep away from lead fracture or central venous catheter occlusion. Transiliac everlasting pacemaker implantation after extraction of infected pectoral pacemaker techniques. Permanent transfemoral pacemaker: a singlecenter series carried out with a better and safer surgical technique. Surgical extraction by thoracotomy is at present reserved for larger vegetations or for circumstances where surgi cal intervention is required for different causes. If lead revision or reimplantation is planned comply with ing extraction, and the vein of implantation is discovered to be occluded, the operator has certainly one of several options: (i) venoplasty of the vein of implantation; (ii) implantation of the model new lead on the opposite aspect with or without tunneling of the lead; (iii) alternate venous entry, such as the iliac vein; and (iv) maintenance of venous access by passing a guidewire through the laser sheath used for extraction. At occasions, a combination of strategies is required to impact full lead extraction. At this level, a femoral route can be used to snare the heel of the lead and apply traction from this femoral route. Any stylets that have been positioned in the lead from above are eliminated and the leads cut in the infraclavicular pocket. With continued traction, the lead can typically be removed in its entirety via the femoral vein. Another example of combined approaches is the applica tion of radiofrequency power through a standard abla tion catheter for portions of retained lead fragments or intramyocardial adherent portions of the lead the place laser is inaccessible. Although clinical expertise remains restricted regarding extraction of chronically implanted leads within the coronary venous system, a number of techniques have been employed. For now and the foreseeable future, this procedure have to be approached with nice respect by personnel dedicated to developing expertise. Present understanding of shock polarity for internal defibrillation: the apparent and nonobvious medical implications.
Ciprofloksacin 750 mg order with mastercard
Adhesions could outcome virus check 750 mg ciprofloksacin fast delivery, by which parts of the parietal pleurae adhere to the visceral pleurae antibiotic in food ciprofloksacin 750 mg discount free shipping. When you contract the diaphragm, the pleural lining of the diaphragm maintains its contact with the visceral pleurae of the two lungs above it, causing the lungs to increase. Likewise, when you increase the thorax transversely by elevating the rib cage, you discover that the lungs comply with faithfully. In this manner, the lungs are in a place to comply with the action of the muscular tissues with out actually being hooked up to them. Because the mating surfaces of the two linings are infused with a serous secretion, the friction of motion of the two linings is tremendously decreased, making respiration rather more environment friendly. When this fluid is misplaced or lowered, as within the dysfunction often known as dry pleurisy, the friction is significantly increased and pain outcomes. If the lining of one lung is damaged via disease or trauma, we nonetheless have the other lung in reserve. There is a level of floor pressure arising from the presence of fluid and highly conforming surfaces that helps hold the sheets collectively. This surfactant reduces the surface rigidity within the lungs and offers a slippery interface between the lungs and the thoracic wall, allowing simple, low-friction gliding of the lungs throughout the thorax. The two surfaces conform to each other on account of the fluid bond between them, and a adverse stress is maintained by lack of contact with the skin environment. This house is occupied primarily by the center, as well as by the trachea, the most important blood vessels, nerves, the thymus gland, lymph nodes, and the conducting portion of the gastrointestinal tract often recognized as the esophagus. The mediastinum lies deep to the bony thorax and its muscular coverings and is nestled deep in the lungs. Its central location in the physique betrays its significance to all areas, and its critical placement surrounded by lung tissue ensures environment friendly switch of gasoline to (and from) the blood pumped by the guts. In the posterior are the vertebrae and the large muscles of the back, and the anterior-lateral side of the thorax is a powerful wall of bone and muscle. The heart is nicely protected in opposition to most trauma, aside from romantic disappointment! The organs and constructions of the mediastinum are encased by a continuation of the parietal pleurae. This lining provides a low-friction mating surface between the lungs and the middle house. The visceral pleural lining of the lungs adjacent to the mediastinum is termed the mediastinal pleura. The left and right phrenic nerves serving the diaphragm move anterior to the foundation constructions of the lungs, coursing along the lateral surfaces of the pericardium (the membranous sac enclosing the heart) to innervate the diaphragm. The left and right vagus nerves enter the posterior mediastinum to innervate the heart, first passing behind the basis structures of the lung, coursing inferiorly to the anterior and posterior surfaces of the esophagus. They descend by way of the diaphragm adjacent to the esophagus through the esophageal hiatus to innervate the belly viscera. The vagal pulmonary branches provide a parasympathetic nerve supply for the lungs, with nerve fibers discovered even in the smallest bronchioles. Muscles of respiration may be divided into muscle tissue of inspiration and expiration (Table 2�3). It is also wise to explain initially that expiration could be either forced or passive but is much more often a passive process. A second, essential notice is that identification of origin and insertion are decided by function. This reality reflects just how ingenious we humans have been at making the fundamental human physiology work for speech, language, and listening to. Muscles of Inspiration As with many voluntary bodily features, inspiration is a graded exercise. We enlist the help of increasingly larger numbers of muscular tissues as our respiratory wants enhance. If the lungs are to expand and fill with air, the thorax must increase in size as nicely. The first approach to increase the thorax is to enhance its vertical (superior-inferior) dimension, a course of that occurs for each quiet and forced inspiration. A skinny however sturdy muscle placed throughout the bottom margin of the rib cage, configured like a drumhead, would be an economical means of increasing the scale of the rib cage without having to manipulate the bony portion in any respect. The thorax and stomach cavity under are separated by one of the important muscles of the physique, the diaphragm. The diaphragm takes the form of an inverted bowl, with its attachments alongside the decrease margin of the rib cage, sternum, and vertebral column. It varieties an entire separation between the upper (thoracic) and lower (abdominal) chambers; and when it contracts, the drive of contraction is directed downward toward the stomach viscera. This contraction leads to elongation of the cavity shaped by the ribs, in order that the lungs increase and air enters by way of the respiratory passageway. Primary Inspiratory Muscle of the Thorax: the Diaphragm the first muscle of inspiration is the diaphragm. The edges attach alongside the inferior boundary of the rib cage, to the xiphoid process, and to the vertebral column in the posterior side. The intermediate area is made up of a big, leafy aponeurosis known as the central tendon. When the muscle contracts, muscle fibers shorten and the diaphragm pulls the central tendon down and ahead. The muscle fibers of the diaphragm radiate from the central tendon, forming the sternal, costal, and vertebral attachments. The anterior-most sternal attachment is made at the xiphoid course of, with fibers coursing up and again to insert into the anterior central tendon. Lateral to the xiphoid, the fibers of the diaphragm attach to the inner border of ribs 7 by way of 12 and to the costal cartilages to kind the costal attachment. In the posterior side, the vertebral diaphragmatic attachment is made with the corpus of L1 via L4 and transverse processes of L1. Notice that the diaphragm programs markedly down from the sternum to the vertebral attachment, fully separating the thorax from the stomach. The posterior vertebral attachment also offers assist for the esophageal hiatus. The right crus arises from attachment at L1 by way of L4, by which the fibers ascend and separate to encircle the esophageal hiatus. Fibers of the left crus additionally arise from L1 through L4, passing to the left of the hiatus. Although the diaphragm separates the thorax from the stomach, the necessity for nutrients dictates that there be communication between the oral cavity and belly region. The region below the diaphragm also has vascular needs, and these require supply routes via the diaphragm. The esophageal hiatus, via which the esophagus passes, is discovered immediately anterior to the aortic hiatus, while the inferior vena cava traverses these two cavities via the foramen vena cava (which is within the right-central aspect of the diaphragm as viewed from above).