
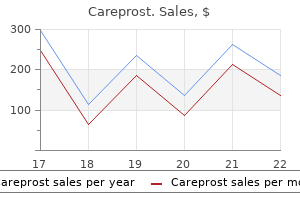
Careprost dosages: 3 ml
Careprost packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles

Careprost 3 ml generic with mastercard
Within hours of passage treatment neutropenia careprost 3 ml quality, the eggs enter an infective stage treatment episode data set careprost 3 ml generic without prescription, and they may be handed to humans by hand contact, from sheets and pillowcases, or directly onto meals and water. Once the eggs are ingested, the larvae escape from the eggs into the stomach and the duodenum, molt twice, and cross into the massive gut to full the life cycle. Sheets and pillowcases have to be cleaned totally, and all contaminated family members must be treated to prevent reinfection. At occasions, the complete household, including curtains and floors, must be cleaned to eradicate the eggs. When they migrate from the perianal space to the vagina, the worms may cause vaginitis; migration to the gut could cause appendicitis. Floch 178 Charcot-Leyden crystals may be present in sputum, and larvae also have been recovered from sputum. The grownup male measures 15 to 25 cm and is smaller than the female, which can be as giant as 35 cm. These helminths could reside for 10 to 18 months and usually copulate in the lumen of the small intestine; the mature female may produce up to 200,000 eggs every day. The life cycle begins with the eggs, that are passed into the soil and turn out to be fertilized and embryonated in 2 to 3 weeks. The eggs are ingested in contaminated meals or water, then cross into the duodenum, where they liberate a larva that penetrates the small intestine and should reach the lungs. A patient may have hypersensitivity reaction in the lung, causing the clinical manifestation of L�ffler syndrome. They mature within the small intestine, the place they copulate, and their eggs are passed into feces to complete the life cycle. Extraintestinal manifestations in themselves, nevertheless, could also be critical problems, as within the uncommon case of pancreatitis. The most necessary intervention is to prevent reinfection, particularly in areas of the world which have poor sanitation. Once the worms attain the lower intestine, symptoms might disappear, but heavier infestations may cause native disturbances, together with true intestinal obstruction. The patient could have abdominal ache, loss of urge for food, nausea, or diarrhea or constipation. At instances, the worms could cause obstruction in the appendix, or they might trigger symptoms of biliary or pancreatic illness because of the migration to bile ducts and gallbladder or pancreatic duct. Varying degrees of extraintestinal manifestations are reported, with charges as excessive as 50%. Larvae reach lung by means of pulmonary artery, penetrate alveoli and enter bronchi eight. Larvae penetrate gut wall and move to coronary heart through portal vein, liver, and inferior vena cava Fertilized 2. Worms are harbored right here, might cross to other organs (biliary tract, lung, heart) or emerge from anus, mouth, nose. Rare cases of neurologic illness have been recognized, as well as disease of almost each organ the place the larvae have migrated. The clinical picture is diversified, and the astute clinician have to be alert to suspect the infection. Obtaining epidemiologic knowledge on the infection has been troublesome as a outcome of stool analyses differ, infections can be low grade, and few larvae may be passed within the stool. However, strongyloidiasis is present in both poorly developed nations and industrialized nations. The most typical presentation is lowgrade infestation, but hyperinfection does happen and may end in severe gastroenteritis and dissemination of the organism. The larvae are then swallowed and enter the duodenum, where the adults attach to or penetrate the wall. The eggs hatch into rhabditiform larvae that migrate into the colon and are handed in the feces. A sexual cycle of development then occurs by which the rhabditiform larvae become males and females and cross eggs into the soil, which then form filariform larvae that may restart the cycle. However, a short life cycle can happen during which the rhabditiform larvae mature and penetrate the skin in the perianal area and autoinfect the host. Nevertheless, autoinfection is nicely documented, and rhabditiform larvae do develop adult sexual forms in soil. Larvae do migrate, they usually have been discovered within the heart, liver, gallbladder, mind, genitourinary organs, nervous system, and pulmonary space. Hyperinfection can happen if large numbers of organisms enter the host, usually an immunocompromised affected person or a affected person handled with corticosteroids, in whom autoinfection may turn out to be prolific. The worms are capable of regulate their very own populations, but when a number is handled with corticosteroids, the eggs produce increased amounts of ecdysteroid substances in host tissue, which permit proliferation of grownup feminine worms and eggs and an enormous variety of larvae. Hyperinfection has been related to millions of adult worms or filarial larvae within the mucosa of the small and enormous intestines. Reports point out that three stools can increase the restoration rate to 50%, and seven stools, up to one hundred pc. Many techniques are used to determine the larvae and depend on the parasitology laboratory. Several forms of serologic checks can be performed, however vary in sensitivity; cross-reactivity with other parasites occurs. The agar plate methodology now seems to be essentially the most sensitive check for identification of the larvae. Safety in kids lower than 15 kg (33 lb) or pregnant lady remains to be decided. Ivermectin is nicely tolerated in contrast with the beforehand used thiabendazole, which is no longer out there in lots of countries. An different drug, albendazole, four hundred mg twice every day for 7 days, is reported to be less efficient. In immunocompromised patients or these receiving corticosteroids, nonetheless, the autoinfection rate may improve considerably to trigger signs. Hyperinfection may cause severe, debilitating gastroenteritis, and moderate infections can cause malabsorption with chronic, debilitating illness. Relapses are reported, and remedy with ivermectin may need to be adopted with a second course of a second drug at a later date. When hyperinfection or a high-risk debilitating state develops, the outcome may be guarded. Marathe A, Date V: Strongyloides stercoralis hyperinfection in an immunocompetent patient with extreme esosinophilia, J Parasitol ninety four:759-760, 2008. The affected person could have a characteristic cutaneous lesion on the website in the perianal area by autoinfection or on the toes if the infection occurred via the soil. No other nematode has been related to such a broad vary of clinical symptoms. Patients with hyperinfection could have gastroenteritis with diarrhea and abdominal ache or large diarrhea and malabsorption. Floch 180 H ookworm illness is attributable to both of two nematodes, Necator americanus (New World hookworm) or Ancylostoma duodenale (Old World hookworm).
Order 3 ml careprost with visa
Aggressive approaches to resect a single metastasis and even multiple metastases have resulted in some success symptoms shingles buy cheap careprost 3 ml on line. Patients with untreated hepatic metastases have a median survival of approximately 10 to 11 months treatment plan for anxiety discount 3 ml careprost with mastercard. Mortality from surgery for resection of liver metastases is lower than 5%, increasing the 5-year survival rate for patients to 25% to 35%, depending on the sequence evaluated. Unfortunately, chemotherapy has not proved profitable for these sufferers; with a extensive range of reported responses, the maximum enchancment rate is 20%. New chemotherapeutic agents have been developed and others are emerging, and although therapy now includes aggressive surgical procedure, results are nonetheless unsure. Initial dietary studies reveal an increased rate of recurrence in patients who proceed to eat a Western food regimen. In Yamada T, editor: Textbook of gastroenterology, ed 4, Philadelphia, 2003, Lippincott�Williams & Wilkins, pp 1882-1913. Floch 161 present process resection for remedy had 2- and 5-year survival rates of 56% and 43%, respectively, if they underwent preoperative radiation therapy. Recent studies have confirmed the significance of preoperative chemoradiation for patients with superior disease. Chemoradiation is effective in downstaging most lesions and permits a better treatment price. Downstaging after chemoradiation may be completed in 60% to 90% of patients, with an entire resectability fee of approximately 60% and a pathologic response rate of 10% to 20%. Mortality from rectal cancer in the United States is slowly decreasing, despite the fact that the incidence is slowly rising. This indicates that early detection and therapy of rectal polyps may be stopping the formation of malignant lesions. Furthermore, there appears to be an epidemiologic distinction between rectal and colon cancer, as a outcome of the incidence of rectal most cancers is comparable for Japan and the United States but different for colon cancer. Again, early removal of easy rectal polyps appears to have decreased the incidence of rectal carcinoma. Cure relies upon largely on the extent of the lesion and whether or not metastasis has occurred. Garcia-Aguilar J, Anda E, Sirvongs P, et al: Pathologic full response to preoperative chemoradiation is associated with decrease native recurrence and improved survival in rectal cancer sufferers treated by mesorectal excision, Dis Col Rect 46:298-304, 2003. Rectal polyps can be asymptomatic however, luckily, are noted throughout most cancers screening and are eliminated via sigmoidoscopy or colonoscopy. Colonoscopy is recommended to rule out other colon lesions before initiating remedy. Ultrasound is now really helpful to evaluate the extent of the lesion, stage the lesion, and determine whether or not nodes are current. Smaller lesions that show no proof of metastasis can be excised, however most authorities imagine that any lesion larger than Dukes stage A (stage I) requires wide excision. Also, preoperative combined-modality remedy is now most popular and accepted as beneficial. Rectal tumor invades perirectal fat Perirectal fat Muscularis/fat interface Muscularis Muscularis/submucosa interface Submucosa/mucosa Mucosa/H2O balloon interface Ultrasonogram. H2O Ultrasound transducer Intact rectum sometimes shows five-banded echoic sample on ultrasound examination Hemorrhoids Martin H. When hemorrhoids are recurrent and extended, a full diagnostic evaluation is warranted. Complete blood count ought to be performed to examine for anemia, with full colonic examination to rule out any related malignancy. Computed tomography of the pelvis may be essential if an related tumor may be causing intraabdominal stress and formation of the hemorrhoid. H emorrhoids are varicose dilatations of the radicals of the superior or inferior plexus of the hemorrhoidal veins. Varicosities are accompanied, in varying degrees, by hypertrophy and spherical cell infiltration of the perivascular connective tissue. Hemorrhoids normally develop in individuals between 25 and 55 years of age, and so they seldom develop in children. Factors in hemorrhoid formation embrace (1) genetic predisposition, (2) absence of valves within the portal venous system attributed to the erect human posture, and (3) conditions that trigger transient or constant elevated pressure or stasis throughout the rectal venous plexuses, corresponding to straining from constipation, frequency of bowel movements from diarrhea, rectal tumors or strictures, being pregnant, and pelvic tumors that improve pressure. Varicosities of the inferior hemorrhoidal plexus cause exterior hemorrhoids which are located below the pectinate line and are coated by the modified skin of the anus. Formation of a thrombus within a vein, or from rupture of a vein with extravasation of blood into the cellular tissue, causes a thrombotic exterior hemorrhoid, which is an acute variety of the exterior type. This often results from straining and seems as a sudden, painful lump that can be seen as a round, bluish, tender swelling. Internal hemorrhoids are enlargements of the veins of the superior hemorrhoidal plexus. Medical remedy normally contains stool softeners, increased dietary fiber to soften stools, Sitz baths with or with out salts in warm water, astringents similar to witch hazel, and topical analgesics. Many clinicians add hydrocortisone suppositories or lotions or mesalamine suppositories to reduce the inflammatory response surrounding the interior or exterior hemorrhoids. Temporary relief of ache from exterior hemorrhoids could be obtained through the use of sprays. Surgical procedures embody rubber band ligation, injection sclerotherapy, cryosurgery, electrocoagulation, photocoagulation, and hemorrhoidectomy. Meta-analysis of controlled, randomized trials reveals that rubber band ligation is superior to sclerotherapy, and that sufferers undergoing ligation are unlikely to require remedy later. Furthermore, although it ends in higher responses than rubber band ligation, hemorrhoidectomy additionally causes extra ache and issues. Most clinicians and proctologists suggest rubber band ligation as first-line surgical remedy. However, most hemorrhoids manifest as easy rectal bleeding, with blood seen on the bathroom tissue or in the bathroom bowl. At times, the bleeding could be brisk enough to lead to bright-red blood in the toilet bowl. Often, the anal ring is too tender to permit full rectal examination, however when full examination is possible, no lesions are felt inside the anal ring. Inspection and digital examination are essential in all evaluations of exterior hemorrhoids. Proctologic or sigmoidoscopic examination is required when internal hemorrhoids are suspected: these are visualized in the rectal vault. Floch 163 P rolapse of the rectum is a condition during which a quantity of layers of the rectum or anal canal protrudes through the anal orifice.
Careprost 3 ml buy online
The time period olates usually contains all olate compounds regardless o one-carbon group or quantity o glutamate residues treatment ear infection buy discount careprost 3 ml. Natural oods largely comprise olates other than olic acid medicine x boston 3 ml careprost cheap otc, principally N5-methyl-tetrahydro olate. The intestine takes up supplementary olic acid about twice as e ciently as pure olates. The major causes or this di erence appear to be the enclosure o pure olates inside cells and the longer polyglutamate tail o natural olates that has to be removed be ore uptake. Describe the synthesis of S-adenosylmethionine and its position in methylation reactions. The Food and Nutrition Board o the Institute o Medicine within the United States recommends that adults not take greater than 1,000 �g o supplemental olic acid per day. The major concern over a excessive consumption o olic acid is that it could enable a cobalaminde cient patient to not develop megaloblastic anemia, to not seek medical consideration, and then unknowingly experience slowly progressive nerve harm (see Section 7. Folates produced by micro organism in the colon are also absorbed but correspond to solely about 10% o the olate absorption within the small intestine i the food regimen accommodates adequate olates. Accordingly, the serum and spinal uid o af ected patients have an abnormally low olate concentration. Without supplementary olate therapy, the de ect causes severe anemia, in addition to abnormal growth o the brain, which may be associated with seizures. The proximal tubules within the kidneys express transport techniques and receptors or the reuptake o ree olates, albumin, and olate-binding protein. Compared with olylmonoglutamates, olylpolyglutamates are less likely misplaced rom cells by dif usion (owing to elevated charge), less probably transported out o the cell by membrane transporters, and have a higher a nity to many o the enzymes which are concerned in olate metabolism. The anti olate methotrexate, which is used in the treatment o rheumatoid arthritis and moderate to severe psoriasis, traps cellular olates as dihydro olates (see Chapter 37). The antibiotic trimethoprim and the antimalarial pyrimethamine inhibit the dihydro olate reductase o humans less than that o bacteria, plasmodia, or oxoplasma gondii. Supplementation is especially important in women o child-bearing age (see neural tube de ects in Section 8. The degradation o ormic acid plays an important position in methanol detoxi cation (see Section three. Several one-carbon group�containing olates can readily be converted to other one-carbon group�containing olates. T ere, S-adenosyl-methionine carries a much more reactive methyl group (see Section 4). Methanol poisoning leads to a transient excessive focus o ormate in cells and blood. T us, ormate can accumulate to millimolar concentrations; this results in acidosis and injury to the optic nerve (mechanism unknown). In the treatment o methanol poisoning, it is important to stop the concentration o ormate in the blood rom rising into the toxic range. Soon a er ingestion, gastrointestinal lavage can diminish the absorption o methanol. Conversion o methanol to ormate may be slowed both with ethanol (which competes with methanol as a substrate o alcohol dehydrogenase) or with omepizole (which inhibits alcohol dehydrogenase and is also used in the remedy o ethylene glycol poisoning; ethylene glycol is utilized in cars to stop reezing or cooling o water). On common, methionine synthase remethylates about hal o the homocysteine to methionine, whereas the opposite hal is converted to cystathionine and thus enters the transsul uration pathway (see Section 9). A er a high-protein meal, extra homocysteine enters the transsul uration pathway, whereas in the asting state, extra homocysteine stays in the activated methyl group cycle. In the liver and the brain, homocysteine may also be methylated to methionine by a second reaction catalyzed by betaine-homocysteine S-methyltrans erase. In addition, S-adenosylmethionine is used or the synthesis o creatine, epinephrine, and phosphatidylcholine. The liver releases creatine into the bloodstream; mind and muscles choose it up rom there. Some people eat a day by day supplement o creatine in an ef ort to improve their bodily per ormance. The methylation o cytosine occurs to inactivate retrotransposons (a class o movable genetic elements), the second X chromosome in emales, imprinted areas o the genome (to silence choose maternal or paternal genes; see Chapter 5), and gene expression at varied levels o development (see Chapter 6). The amino group o the side chain o lysine residues may be methylated as much as three old, and the guanidino group o the aspect chain o arginine residues as a lot as two old (yielding as a lot as three dif erent isomers). Cobalamin is a vitamin principally acquired rom eating oods which may be derived rom animals. Institute o Medicine recommended daily allowance o cobalamin or folks aged 14 years or older is 2. No tolerable higher consumption stage or cobalamin is ready as a result of no adverse ef ects have been reported in wholesome persons. Because o their food plan, strict vegans must take a supplement o cobalamin; this is particularly necessary or pregnant girls and nursing moms to keep away from cobalamin de ciency in their in ants (see also Section 7. Cobalamin accommodates a substituted corrin ring with a cobalt (Co3+) ion in its midst. Cyanocobalamin is probably the most generally used orm o cobalamin in orti ed oods and vitamin supplements. The human body converts cyanocobalamin to the co actors methylcobalamin and 5-deoxyadenosylcobalamin (see below). E cient uptake o cobalamin requires a abdomen that secretes acid, pepsin, and intrinsic actor; a pancreas that Table 36. As a low pH and proteases within the stomach ree dietary cobalamin rom the ood matrix, haptocorrin, secreted by salivary glands and the gastric mucosa, binds to cobalamin. In the small gut, as chyme reaches a near-neutral pH, proteases rom the pancreas degrade haptocorrin, and cobalamin leaves haptocorrin and as an alternative binds to intrinsic actor (shown in abbreviated orm in. In the terminal portion o the ileum, the intrinsic actor-cobalamin complex binds to cubam (a heterodimer o cubilin and amnionless); this binding requires Ca2+, which is normally supplied by the pancreas. Cubam is also expressed within the proximal tubules o the kidneys or the reabsorption o a quantity of proteins. These enable cubilin to bind not only the intrinsic actor-cobalamin complicated but in addition albumin, vitamin D�binding protein, trans errin, and apolipoprotein A1. Cobalamin is then either methylated or 5-deoxyadenosylated to become methylcobalamin or 5-deoxyadenosylcobalamin, respectively. Me thylmalo nyl-Co A Mutas e Methylmalonyl-CoA mutase requires 5-deoxyadenosylcobalamin and catalyzes a reaction within the conversion o propionyl-CoA to succinyl-CoA. A cobalamin de ciency leads to an increase in the concentration o methylmalonic acid within the blood, which is use ul or a prognosis (see Section 7. This impairs replication o rapidly dividing cells and thus results in megaloblastic anemia and diarrhea. Cobalamin def ciency results in a largely irreversible destruction o the myelin sheaths o the nervous system; as properly as, by inactivating methionine synthase, a cobalamin def ciency could lead to a secondary olate def ciency. Furthermore, regular olate stores (which are mainly in the liver) equal solely a ew weeks o olate needs. In flip, this explains the principal ef ects o olate de ciency on the body: megaloblastic anemia (also referred to as macrocytic anemia; see. An inadequate provide o deoxythymidine triphosphate (d P) also limits the speed o pink blood cell manufacturing and results in cells o extremely variable measurement, many o which are destroyed within the bone marrow as a substitute o being released into the bloodstream (hence the anemia).
3 ml careprost purchase mastercard
Inactive scientific symptomatic disease may replicate full remission medicine cabinets recessed order 3 ml careprost overnight delivery, with no evidence of a pathologic situation or with a low-grade treatment zinc poisoning careprost 3 ml purchase fast delivery, continual situation. Depending on patient tolerance and doctor preference, topical remedy in the form of enemas or suppositories is commonly effective for acute and maintenance therapy. Although nutritional remedy is slower, significant studies have proven that it works. Therefore, conjugated, unconjugated, and rectal varieties at the second are out there, in addition to a formulation that could be given once daily. Corticosteroids are also rapidly effective in topical form, when disease is restricted to the rectum or the distal colon. Doses are variable, and sufferers should be checked carefully for any hematologic problems. Cyclosporine can induce a remission of signs, and patients could also be placed on oral cyclosporine or different immunosuppressive brokers. However, that is drastic remedy, and these sufferers are near present process complete colectomy or surgical procedure. Because allergic and possible hematologic adverse effects could develop, infliximab must be used with warning. However, its broad use in rheumatoid arthritis has given gastroenterologists confidence about its safety. Natalizumab, an 4-integrin, was proven in early trials to be effective in inducing remission and bettering high quality of life. Natalizumab has now been positioned back in the marketplace and joins infliximab, adalimumab, and certolizumab as different organic therapy selections. An increased incidence of lymphoma has been suspected with using infliximab, however latest evaluations indicate the immunomodulator could additionally be incriminated. Intensive evaluation is forthcoming, wise, the effectiveness of these drugs is comparable, and remission and maintenance rates of 35% to 95% have been reported. Many patients with chronic or extreme disease require long-term corticosteroid therapy and should develop the associated complications. Great effort must be made to use an immunomodulator to replace corticosteroids if patients turn out to be dependent on their use. Placebo All the acute and chronic trials with biologicals have been matched towards placebo. Classifications change with the latest data out there; therefore, the being pregnant class of a drug should be checked with the physician prescribing and the pharmacy delivering the drug to a pregnant affected person. Francella A, Dyan A, Bodian C, et al: the security of 6-mercaptopurine for childbearing sufferers with inflammatory bowel disease: a retrospective cohort examine, Gastroenterology 124:9-17, 2003. The precise illness process is related to solely a slight improve in spontaneous abortion. Statistical information reveal that sulfasalazine, mesalamine, and corticosteroids seem secure during pregnancy. Floch one hundred fifty five icroscopic colitis is a syndrome in which sufferers have (1) continual diarrhea, (2) normal findings on colonoscopy and a normal-appearing mucosa, (3) histologic proof of elevated cellular infiltrate in the lamina propria, and (4) both (a) fullblown lymphocytic colitis with intraepithelial lymphocytes and increased infiltrate in the lamina propria or (b) collagenous colitis with a collagen band below the epithelium larger than 10 m. M Microscopic colitis has been difficult to outline, but numerous stories have clarified the syndrome. Initially described as "collagenous" colitis, with watery diarrhea and deposition of collagen, it was later famous that many sufferers with chronic watery diarrhea have a lymphocytic infiltrate and a definite intraepithelial lymphocytic infiltrate. During the previous decade, many sufferers have been described with watery diarrhea responsive to remedy and with increased infiltrate solely in the lamina propria. It is Lymphocytic colitis Low-power microphotograph of lymphocytic colitis that exhibits increased lymphocytic and spherical cell infiltration in the lamina propria. High-power microphotograph of lymphocytic colitis (same patient and biopsy as in determine at left). Collagenous colitis Colon biopsy specimen displaying collagenous colitis (trichrome stain [blue]). High-power microphotograph of collagenous colitis that exhibits an enlarged (pink) collagen layer and an elevated lymphocytic infiltrate in the lamina propria. The arrow indicates a cellular component (fibroblast nucleus) entrapped within the enlarged collagen layer. Histologic examination of the biopsy specimen reveals no distortion of the crypts, as seen in ulcerative colitis. Almost 30% of sufferers with celiac disease have been reported to have some form of microscopic colitis; thus an analogous cause is suspected. Some consultants choose a 4- to 8-week trial of bismuth subsalicylate before administering mesalamine. It may be necessary to use prednisone to induce remission if bismuth subsalicylate and mesalamine fail to do so. The course of microscopic colitis is benign, and most sufferers reply to mesalamine, budesonide, bismuth subsalicylate, and if needed, corticosteroids or an experimental therapeutic agent. Other patients, however, expertise relapse and require repeat remedy after being in remission. Fernandez-Banares F, Salas A, Esteve N, et al: Collagenous and lymphocytic colitis: analysis of medical and histologic options, response to treatment, and long-term follow-up, Am J Gastroenterol 908:340-347, 2003. Robert M: Pathology of microscopic, lymphocytic, and collagenous colitis, J Clin Gastroenterol 38:S17-S26, 2004. Schiller L: the medical spectrum of microscopic colitis, J Clin Gastroenterol 38:S27-S30, 2004. Less than 50% of patients have stomach ache along with diarrhea, and less than 33% experience weight reduction. The results of watery diarrhea may be severe, and a lot of patients turn out to be hypokalemic. Often, a patient with low-grade watery diarrhea receives a diagnosis of irritable bowel syndrome on the premise of regular gross colonoscopy findings, but no biopsy specimen was taken as a outcome of the mucosa seemed regular. Mucosal biopsy of the colon should be performed to decide whether or not a affected person with watery diarrhea has microscopic colitis. More detailed research will permit a willpower of the incidence and prevalence of the illness. An preliminary criterion was "increased collagen deposition," and then the "presence of intraepithelial lymphocytes" was added as a criterion. It is now accepted that increased levels of lymphocytes and plasma cells, with the risk of eosinophils within the lamina propria, correlating with the scientific image and resolving with treatment, make the analysis. The drugs most often used are mesalamine and budesonide, with the latter favored in a latest study. Trials have been carried out utilizing bismuth subsalicylate, antibiotics, Neoplasms of the Large Bowel: Colon Polyps Martin H. High-grade dysplasia in a polyp is usually referred to as "intermucosal carcinoma (malignant)," or carcinoma in situ. Nonneoplastic polyps include mucosal, hyperplastic, and inflammatory (pseudopolyps) varieties, hamartomas; and different uncommon sorts. Submucosal polyps are lipomas, lymphoid collections, leiomyomas, hemangiomas, fibromas, and rare presentations of endometriosis, pneumatosis cystoides intestinalis, colitis cystica profunda, or metastatic lesions. The prevalence of colorectal neoplasia varies worldwide: 30 to forty per one hundred,000 inhabitants within the United States; 15 to 30 per a hundred,000 in Europe; and fewer than 5 to 10 in South America and Asia.
Order careprost 3 ml amex
Zheng M medications migraine headaches cheap careprost 3 ml online, Chen Y treatment lupus 3 ml careprost trusted, Bai J, et al: Transjugular intrahepatic portosystemic shunt versus endoscopic remedy within the secondary prophylaxis of variceal rebleeding in cirrhotic sufferers: meta-analysis replace, J Clin Gastroenterol 42(5):507-516, 2008. Previous research have proven that a portosystemic gradient (difference between portal and hepatic venous pressures) higher than 12 mm Hg is related to an increased threat for bleeding varices. Variable-sized stents of 10 and 12 mm are available to increase the dimensions of the shunt. Balloon deflated and removed; stent stays to keep patency of portosystemic shunt Liver Biopsy Kris V. Kowdley 229 would occur within the vascular compartment and would be related to a lower risk for intraabdominal bleeding. Percutaneous liver biopsy is generally carried out using native anesthesia alone, although many hepatologists have begun using a mild sedative to reduce anxiety. After native anesthesia with lidocaine, a trocar is used to create a tract to facilitate passage of a 16-gauge needle. Different forms of needles are available for liver biopsy; the Klatskin needle is often used. Hematoxylin and eosin stain is used to consider for inflammation and necrosis; trichrome stain is used to assess the presence and diploma of fibrosis; and stains such as reticulin can be utilized to consider the structure. In addition, particular stains are helpful to display screen for particular liver diseases, such as periodic acid�Schiff with diastase for 1-antitrypsin deficiency, Perls Prussian blue stain for iron, and a particular stain for hepatitis B core antigen. Biochemical measurement of iron or copper can be performed from fresh or paraffin-embedded tissue to establish a selected analysis of hemochromatosis or Wilson disease, respectively. However, liver biopsy stays an important process for determining the prognosis and prognosis of liver disease. More importantly, liver biopsy remains the best method for establishing the presence or absence of cirrhosis. In many liver diseases, together with alcoholic liver disease, hemochromatosis, and hepatitis C, the risk for hepatocellular carcinoma is associated primarily with the presence of cirrhosis. Therefore, identification of cirrhosis can facilitate choices about screening for liver most cancers. Furthermore, findings on liver biopsy are essential for making remedy decisions in lots of persistent liver diseases, including hepatitis B and hepatitis C. Liver biopsy remains the criterion for the prognosis of persistent hepatic ailments corresponding to Wilson illness, nonalcoholic steatohepatitis, and autoimmune hepatitis. Liver biopsy occasionally identifies sudden findings that will change administration. Evaluating the minute construction of the liver is crucial for assessing sufferers with drug-induced hepatitis or fulminant liver failure. Managing patients after liver transplantation also largely depends on liver biopsy, significantly in situations related to a high rate of recurrence, such as hepatitis C and hepatitis B. Pain may be localized over the biopsy web site, diffusely unfold over the abdomen, or more typically, referred to the right shoulder from irritation of the diaphragm. Bleeding is extra severe and will end in hepatic capsular hematoma and even intraabdominal bleeding, although that is uncommon. Other complications embrace infection, pneumothorax or hemothorax, and perforation of the gallbladder or the bile ducts. Risk factors for issues of liver biopsy embody coagulopathy and increased number of passes. Most facilities require that the affected person lie on the proper side for several hours after the biopsy to allow internal compression of the liver against the rib cage. Contraindications to liver biopsy include lack of affected person cooperation, bacterial cholangitis, extrahepatic bile duct obstruction, and vital coagulopathy or thrombocytopenia. Some advocate avoiding liver biopsy in sufferers with cystic liver lesions because of an infection risk and in those with amyloidosis because of hemorrhage threat. This location is marked, and the biopsy is subsequently carried out at the bedside, usually in a day-surgery or ambulatory setting. This method is normally selected when biopsy is performed to research focal lesions, corresponding to suspected hepatocellular carcinoma or adenoma. Liver biopsy can be accomplished using laparoscopy, though usually solely when the affected person is already present process laparoscopic surgery. In addition to the percutaneous approach, liver biopsy may be carried out utilizing transjugular techniques, typically by interventional radiologists and for patients with a higher threat for bleeding, corresponding to these with thrombocytopenia or coagulation abnormalities. A catheter is introduced into the right internal jugular vein and then handed into the liver by way of the hepatic vein. Breath held in expiration, whereas needle pushed to most depth with quick rectilinear motion with out rotation; aspiration maintained 7th to ninth intercostal space in midaxillary line (Biopsy specimen recovered by expelling saline from syringe) 2. Alternate Techniques the most important limitation of liver biopsy is sampling variability, particularly in liver diseases with focal involvement, similar to cystic fibrosis and primary sclerosing cholangitis. This has led to active investigation into other strategies to assess the presence or absence of cirrhosis. In the longer term, the mix of structural imaging studies and dynamic serum or plasma markers of fibrosis might reach enough reliability to substitute liver biopsy within the analysis of cirrhosis. However, liver biopsy will probably remain essential for diagnostic purposes in some sufferers for whom serologic testing has not established the cause for liver illness. Kowdley 230 hypoxemia (low atmospheric pressure), or both, because this a half of the hepatic lobule is most delicate to situations of hypoxia. Periportal or peripheral necrosis signifies damage to periportal hepatocytes and in the adjoining peripheral zone of the parenchymal lobule. Extensive zonal, primarily central, necrosis usually outcomes from exposure to varied poisons, toxins, or medicine however is also observed after infection or shock. If central necrosis becomes more intensive, bridges develop that connect the central zones or the portal and central zones (bridging necrosis). This could proceed further to virtually complete lack of liver cells in a lobule (massive necrosis). Massive necrosis in a substantial a half of the liver produces hepatic insufficiency, generally fatal, that traditionally has been termed acute yellow atrophy or acute purple atrophy of the liver. The regular architecture of the liver may be troublesome to acknowledge in huge necrosis. The time period cell dropout has also been used to describe some circumstances of hepatocellular necrosis. Necrosis implies not solely the death of cells, but in addition the phenomena following cell death, particularly, the disappearance of cells and frequently the accompanying inflammatory response. The ultimate and irreversible stage of degeneration, hepatic necrosis, involves only the liver cells in most types, whereas Kupffer cells and stroma stay intact. Kupffer cells reply to most forms of hepatocellular degeneration and necrosis with reactive proliferation. Acute viral, poisonous, or drug-induced hepatitis is normally the trigger of hepatocellular necrosis, but any course of leading to a systemic inflammation or a liver-specific damage can lead to hepatic necrosis, as can a variety of insults that cause hepatic ischemia or hypoxemia.
Careprost 3 ml purchase with mastercard
The lateral phase corresponds to the basic descriptions of the left lobe medications prescribed for depression 3 ml careprost cheap with amex, whereas the facet of the medial section on the visceral live surface corresponds to the quadrate lobe symptoms enlarged prostate careprost 3 ml quality. The four bile ducts of the second order type these of the third order, which drain both the superior or the inferior corresponding phase. Thus, the bile ducts and the accompanying vessels could be designated based on the lobes, segments, and areas to which they belong. The anatomically distinct caudate lobe has a vascular association that divides it right into a left portion, drained by the left lobar duct, and a proper portion, drained by the best lobar duct. The caudate course of, connecting the caudate lobe with the proper lobe of the liver, has a separate web of vessels, which often communicates with branches of the proper lobar duct. Neither the caudate lobe nor other components of the liver present effective communication between the best and left lobar duct systems. The distribution of draining bile ducts and afferent blood vessels, as schematically depicted here, is legitimate generally, however individual variations are abundant, particularly in the lateral superior vessel and ducts for the appendix fibrosa. Segmental bile duct variation happens extra typically on the best aspect, whereas variation in segmental arteries is extra widespread on the left aspect. Kowdley 214 ertain studies, particularly the painstaking dissections of Michels, have disclosed appreciable variations (see Chapter 215) in the arterial provide of the liver, biliary system, and pancreas. According to the traditional description, present in solely 55% of examined specimens, the celiac artery or celiac axis is a brief, thick trunk that originates within the aorta just under the aortic hiatus in the diaphragm. It extends horizontally and forward above the pancreas and splits into the left gastric, hepatic, and splenic arteries. An inferior phrenic artery, usually ranging from the aorta, or a dorsal pancreatic artery (see later), in any other case departing from the splenic artery, the hepatic artery, or the aorta, might exceptionally derive from the celiac axis. The left gastric (or coronary) artery, the smallest of the three celiac branches, starting at the cardia, extends along the lesser curvature of the abdomen to anastomose with the best gastric artery. The splenic artery, the biggest of the three celiac branches (in the adult), takes a somewhat tortuous course to the left, alongside and behind the higher border of the pancreas. At a variable distance from the spleen, it breaks up into numerous terminal branches that enter the hilus of the spleen. The left gastroepiploic artery and the quick gastric arteries usually have their origins in one of these terminal branches. As the hepatic artery turns upward, it provides origin first to the gastroduodenal artery (see later), then often to the supraduodenal artery, and at last to the proper gastric artery. The supraduodenal artery, which may also originate from the best hepatic or the retroduodenal artery, descends to supply the anterior, superior, and posterior surfaces of the primary inch (2. The right gastric artery passes to the left along the lesser curvature of the stomach to anastomose with the left gastric artery. The continuation of the hepatic artery beyond the origins of these vessels is known as the widespread hepatic artery (arteria hepatica propria). It ascends and divides into several branches, most often the proper hepatic and left hepatic arteries; the middle hepatic artery often arises from the left hepatic artery. The proper hepatic artery generally passes behind the widespread hepatic duct to enter the cystic Calot triangle, formed by the cystic duct, the hepatic duct, and, cephalad, the liver. Occasionally, however, the best hepatic artery crosses in front of the bile duct (see Chapter 215). In general, the arterial provide to the pancreas, common bile duct, and adjacent parts of the duodenum comes from branches of the gastroduodenal, superior mesenteric, and splenic C arteries. The gastroduodenal artery, after its origin from the frequent hepatic artery, passes downward to course behind the first portion of the duodenum and in front of the pinnacle of the pancreas. Before or immediately after passing behind the duodenum, it gives origin to the posterior superior pancreaticoduodenal artery, which has been renamed (Michels) the retroduodenal artery. At the lower border of the pylorus, the gastroduodenal artery divides into a larger proper gastroepiploic artery and a smaller anterior superior pancreaticoduodenal artery. The right gastroepiploic enters the greater omentum to comply with the higher curvature of the stomach. The anterior superior pancreaticoduodenal artery continues downward on the anterior surface of the head of the pancreas as far as its decrease border, the place it turns upward to unite with the anterior branch of the inferior pancreaticoduodenal artery, also referred to as the anterior inferior pancreaticoduodenal artery. In roughly 40% of the circumstances, no frequent inferior pancreaticoduodenal artery exists, and the anterior and posterior vessels originate individually from the superior mesenteric artery. The head of the pancreas and the second and third parts of the duodenum are thus supplied by two arcades, an anterior and a posterior arch. The posterior arch is fashioned by the posterior superior pancreaticoduodenal (retroduodenal) artery uniting with the posterior inferior pancreaticoduodenal artery. The anterior arch is fashioned by the gastroduodenal and anterior superior pancreaticoduodenal arteries uniting with the anterior inferior pancreaticoduodenal artery. Both give off branches that anastomose with each other through and around the pancreas, supplying that organ and the duodenum. Branches of the splenic artery are the chief suppliers to the neck, physique, and tail of the pancreas. Some of these are small twigs given off by the splenic artery because it programs along the upper border of the pancreas. Three branches, nonetheless, are normally larger than the others and have achieved the distinction of individual names. The dorsal pancreatic artery, also called the superior pancreatic artery, although normally originating from the beginning of the splenic artery, can also arise from the hepatic or celiac artery or the aorta. It runs downward behind and within the substance of the pancreas, dividing into left and right branches. The proper branches constitute an anastomotic vessel to the anterior pancreatic arch and also a branch to the pancreatic lingual. The great pancreatic artery originates from the splenic additional to the left and passes downward, dividing into branches that anastomose with the transverse or inferior pancreatic artery. The artery for tail of pancreas (arteria caudae pancreatis) originates from the splenic artery, or from its terminal branches at the tail of the pancreas, and divides into branches that anastomose with the terminal twigs of the transverse pan- creatic artery. The transverse pancreatic artery, normally the left branch of the dorsal pancreatic, programs behind the physique and tail of the pancreas close to its decrease border. The different branches of the splenic artery are variable terminal branches to the spleen, the left gastroepiploic artery, the short gastric arteries to the fundus of the stomach, and normally branches that anastomose with the left inferior phrenic artery. Kowdley 215 n more than 40% of dissections, variations were found in the origin and course of the hepatic artery or its branches (Michels). These contain, with equal incidence, the proper and left hepatic arteries and are of greater than passing surgical significance, primarily as a result of their unintended ligation results in liver necrosis. A changed hepatic artery originates from a different source than in the standard description and substitutes for the standard vessel (see Chapter 214). An accessory artery is a vessel extra to those originating in accordance with standard descriptions. An instance of alternative is the origin of the common hepatic artery from the superior mesenteric artery. The common hepatic artery passes via or behind the pinnacle of the pancreas, and its ligation during a pancreaticoduodenal resection deprives the liver of its arterial blood supply. Under these circumstances, only the left gastric and splenic arteries come up from the celiac axis.
Diseases
- McArdle disease
- Appendicitis
- Vocal cord dysfunction familial
- Rectal neoplasm
- Wilkes Stevenson syndrome
- CDG syndrome type 1A
- Strumpell Lorrain disease
- Familial m Familial w
Careprost 3 ml online
The infra-anal fascia overlaying the iliococcygeus muscle roofs the ischiorectal house medications januvia generic careprost 3 ml amex. The coccyx and the sacrospinous and sacrotuberal ligaments medicine to stop vomiting order 3 ml careprost amex, overlapped by the gluteus maximus muscle, constitute the bottom or posterior wall of the fossa. These buildings thus confine the posterior extension of the ischiorectal house, which has, posteriorly to the anal canal, no medial walls. The fossae of each aspect communicate with each other by what is named the deep postanal house, which lies above the anococcygeal ligament or posterior extension of the exterior anal sphincter and beneath the levator plate. This deep postanal house is also known as the posterior communicating house because the proper and left ischiorectal spaces talk by way of it. The deep postanal house is thus the identical old pathway for purulent infections to unfold from one ischiorectal house to the other, resulting in the semicircular or "horseshoe" posterior anal fistula. The ground of the ischiorectal house behind the urogenital diaphragm is the transverse septum of the ischiorectal fossa. Large fat globules lying in a matrix of skinny collagenous fibrils fill the ischiorectal house. Interior hemorrhoidal (rectal) vessels and nerves cross each house obliquely from its posterior-lateral angle en route from the pudendal vessels and nerves in Alcock (pudendal) canal to the anal canal. Superficial and deep compartments of the urogenital diaphragm occupy the area inside the pubic arch and include the urogenital musculature, which is in shut useful relationship to the pelvic diaphragm and the anorectal sphincters. Rosenthal 74 fibers, is current in the complete length of the anterior wall of the canal. For roughly the lateral one fourth to one third of the canal, fibers of the internal indirect muscle, which come up from the inguinal ligament and the related iliac fascia, form the anterior wall of the canal deep to the external indirect aponeurosis. The flooring of the canal is formed in its medial two thirds to three fourths by the rolled-under portion of the external indirect aponeurosis, along with the lacunar ligament, forming a shelf on which the spermatic cord rests. The transversalis fascia is current for the whole size of the posterior wall of the inguinal canal. Toward the medial end of the canal, reinforcing the part of this wall posterior to the superficial inguinal ring, is the reflected inguinal ligament. The tendon of the rectus abdominis muscle fuses with the posterior facet of the conjoined tendon. The subserous fascia and the peritoneum are posterior or deep to the transversalis fascia and proceed behind the deep inguinal ring. At the lateral end of the canal, the inferior epigastric artery and vein are posterior to the canal within the subperitoneal fascia. Overlying these vessels, thickening within the transversalis fascia could appear, known as the interfoveolar ligament. A slight melancholy within the parietal peritoneum, as seen from within, could also be current at the web site of the deep inguinal ring. The roof of the inguinal canal is formed by the most inferior fasciculi of the interior indirect muscle as they gradually move in a barely arched trend, from a position at their origin anterior to the canal to a place at their insertion posterior to the canal. At the lateral end of the canal, the lower fasciculi of the transversus abdominis arch similarly cowl the canal. The weakest area in the anterolateral wall in relation to the inguinal canal is the area of the superficial inguinal ring, which is strengthened by the reflected inguinal ligament, the conjoined tendon, and the growth laterally and inferiorly from the tendon of the rectus muscle to the pecten pubis. This generally weakened space, by way of which direct inguinal hernias move, is commonly described as a triangle bounded superolaterally by the inferior epigastric vessels, superomedially by the lateral margin of the rectus, and inferiorly by the inguinal ligament, generally known as the inguinal (Hesselbach) triangle. Preperitoneal hernia restore has allowed a brand new view of the anatomy of the inguinal canal. The preperitoneal space is bordered posteriorly by the peritoneum and anteriorly by the transversalis fascia. External iliac vessels run on the medial aspect of the psoas muscle before passing under the iliopubic tract and the inguinal ligament and changing into the femoral vessels. Five major nerves in the preperitoneal space are responsible for innervation of the lower abdominal wall, inguinal, and genital areas: the iliohypogastric, hypogastric, ilioinguinal, genitofemoral, and lateral femoral cutaneous nerves. The inguinal canal is an oblique tunnel, three to 5 cm long, by way of the muscular and deep fascial layers of the anterior belly wall, parallel to and superior to the inguinal ligament. The canal extends between the interior inguinal ring, situated within the transversalis fascia approximately halfway between the anterior superior spine of the ilium and the pubic symphysis, and the exterior inguinal ring, positioned in the aponeurosis of the external stomach indirect muscle simply superior and lateral to the pubic tubercle. In the male, the canal conveys the spermatic twine, comprising the vas deferens and the vessels and nerves of the testes. The anatomy of the inguinal canal is similar in the female but is considerably much less well developed. The canal in the female accommodates the round ligament of the uterus because it travels toward its termination within the labia majora. The inside inguinal ring, a funnel-shaped opening within the transversalis fascia, is the site at which the transversalis fascia turns into the innermost overlaying of the spermatic cord, the inner spermatic fascia. Inferior epigastric vessels are just medial to the interior inguinal ring, and probably the most lateral level of the inferior border of the transverses muscle is just lateral to this ring. The exterior inguinal ring is shaped by a division of the fibers of the exterior belly oblique aponeurosis with fibers that pass superomedial to the ring attaching to the pubic symphysis. This portion of the external indirect aponeurosis is called the superior crus of the exterior (superficial) ring. Fibers of the exterior oblique aponeurosis that cross inferolateral to the superficial inguinal ring are referred to as the inferior crura of the ring. The decrease border of the exterior oblique aponeurosis is folded under itself, with the sting of the fold forming the inguinal ligament. The fascia lata on the anterior side of the thigh is closely blended to the full size of the ligament, and its lateral half is fused with the iliac fascia because the iliacus muscle passes into the thigh. Fibers of the aponeurosis form the medial half of the inguinal ligament, rolling underneath in such a method that the fibers forming the inferolateral margin of the exterior inguinal ring become probably the most inferior fibers on the attachment to the pubic bone, thus attaching most interiorly on the pubic tubercle, whereas fibers originally more inferior connect higher up on the tubercle, in sequence alongside the medial a part of the pecten pubis for varying distances. The portion of the aponeurosis that runs posteriorly and superiorly from the folded fringe of the ligament to the pecten pubis known as the pectineal a half of the inguinal ligament, or the lacunar ligament. The inguinal canal and related constructions could be viewed as a tubular tunnel having a roof, a floor, and anterior and posterior walls. The two openings are the deep inguinal ring in the transversalis fascia at the inner (lateral) finish of the canal and the superficial inguinal ring in the aponeurosis of the exterior oblique muscle on the external (medial) finish of the canal. In Bendavid R, editor: Prostheses and abdominal wall hernias, Austin, Texas, 1994, Landes Medical, pp 82-103. A easy view shows two imaginary planes passing through the umbilicus, one vertically and the opposite horizontally. The abdomen is thus divided into four quadrants: a proper and a left higher quadrant and a proper and a left lower quadrant. A division of the abdomen for descriptive purposes uses two vertical and two horizontal planes that divide the stomach into 9 regions (tic-tac-toe board).
Careprost 3 ml cheap overnight delivery
Apoptosis could be divided into an extrinsic pathway that is dependent upon plasma membrane receptors and an intrinsic pathway that is dependent upon mitochondria treatment ulcerative colitis discount 3 ml careprost overnight delivery. The intrinsic pathway is dependent upon the permeabilization o the outer mitochondrial membrane and the discharge o cytochrome C rom the intermembrane space o mitochondria treatment uterine fibroids order careprost 3 ml. Cytochrome C within the cytosol then avors the ormation o an apoptosome, activation o an initiator caspase, and activation o ef ector caspases. These alterations additionally render tumor cells immune to chemotherapy-induced apoptosis. The Cip/Kip amily includes p21Cip1, p27Kip1, and p57Kip2 (noted as p21, p27, and p57). Obesity is a risk actor or a restricted quantity o cancers, notably cancer o the endometrium. Isolation and evaluation o circulating tumor cells maintain promise in making a prognosis and figuring out the optimal therapy. Overexpression o cyclins Cancer is the consequence o multiple abnormalities o the genome o somatic cells. Most o the mutations seen in tumors are single nucleotide substitutions, and most o these are missense mutations. Some o the clinically signi cant mutations improve proli eration, and others inhibit apoptosis. In a simple binary classi cation, driver mutations are key to neoplasia, whereas passenger mutations have ew consequences. Oncoproteins could additionally be regular proteins which are expressed in uncommon abundance as a end result of o gene ampli cation or a chromosome translocation that hyperlinks the gene to a promoter that leads to an elevated rate o transcription. In neoplasms, the tumor suppressor unction could be lost by mutation or epigenetic ef ects. Mutations might cause a loss o unction because o missense mutation, loss o heterozygosity (see Section 4. Mutations in tumor suppressors, proto-oncogenes, or oncogenes can each be driver mutations. Most o the main cancer-causing mutations af ect the unction o one out o a couple of dozen pathways. Some o these inhibitors are used to impair the unction o oncoproteins, similar to protein kinases. For essentially the most half, no medication are available to remedy loss o tumor suppressor unction instantly. However, the loss o tumor suppressor exercise generally results in elevated exercise o one other protein downstream in the pathway that can sometimes be inhibited with a drug. In heritable most cancers syndromes, the illness is de ned as an unusually early onset and an unusually high probability o developing a selected neoplasm. In a person who has just one allele to lose to inactivation, cancer occurs sooner than in a person who has two alleles to lose; therefore the dominant pattern o inheritance. In act, tumors in kids usually include ewer mutations than those in older adults. Furthermore, even normal, aged pores and skin incorporates a signi cant raction o tumorigenic driver mutations. A large portion o the age-dependent most cancers risk is associated with the quantity o stem cell divisions, presumably because o related replication errors. Records of ~5 million folks in the United Kingdom (~9% of all inhabitants) from 1987�2012 have been analyzed. For occasion, non-small-cell lung carcinomas rom smokers have ~10 occasions the quantity o mutations ound in the identical tumors rom nonsmokers. Among the many everlasting mutations, some lead to the ormation o an oncogene and others lead to the loss o tumor suppressor unction. For a comparable quantity o nicotine consumed, smoke rom a water pipe incorporates ~10 instances more benzo[a]pyrene than smoke rom a cigarette. Chewing tobacco incorporates N-nitrosamines that give rise to most cancers o the oral cavity. The primary dif erence between an obese and a lean person is the mass o adipose tissue. The obesity-induced, elevated focus o estrone avors the growth o estrogen-dependent tumors. Other proposed explanations or an obesity-induced improve in cancer threat state that the obesity-induced increased concentration o insulin or hormones released rom the adipose tissue. The ef ect o ethanol (alcohol) consumption alone (and together with smoking) on the danger o cancer in the mouth, pharynx, larynx, and esophagus is described in Section 4. Circ ulating Tumo r Ce lls Circulating tumor cells (C Cs) are cells which were shed by a tumor or its metastases and entered the bloodstream. In the laboratory, C Cs are enriched and identi ed on the basis o the presence and absence o sure cell sur ace proteins. A blood sample that exams positive or C Cs usually accommodates more than our cells per 7. Currently, C Cs can be utilized to make a prognosis and choose a remedy or most cancers o the breast, prostate, or colon. Many tumors o the lung take a look at positive or the overexpression o kinases that can be inhibited pharmacologically. Prostate tumors are genetically very numerous and o en comprise a translocation that places a promoter with an androgen response factor next to a transcription actor. Accordingly, sufferers with advanced prostate most cancers are commonly given androgen deprivation remedy. About hal o the instances o amilial melanoma are caused by mutations in a gene that encodes an inhibitor o cell cycle progression. Much o the element we all know concerning the genetic modifications that occur in varied tumors relies on huge parallel sequencing (next era sequencing; see Section 5. Such sequencing is now gaining entry into medical use, most o en within the orm o select most cancers gene panels. The major present challenges are to study to interpret the implications o noticed mutations and to decide the most ef ective therapies. It is now apparent that there are a couple of dozen pathways that consistently unction abnormally in cancer (see Section 2. Hence, a amily history o most cancers in a single organ may be attributable to a number of dif erent heritable most cancers syndromes; af ected amily members there ore must be examined or mutations in a number of pathways. Increasingly, gene panels and large parallel sequencing are used to screen or multiple genetic alterations (see Section 6 in Chapter 4). Currently, essentially the most success ul remedy o most cancers is elimination o the tumor by surgical procedure. However, some premalignant circumstances can success ully be detected, similar to adenomatous colon polyps by colonoscopy and cervical dysplasia by colposcopy.
Careprost 3 ml mastercard
Treatment of acute assaults is supportive and consists of administration of the associated pain symptoms urinary tract infection careprost 3 ml generic mastercard. Marked tenderness is variable; peritoneal signs similar to rebound tenderness happen frequently; and guarding is often seen treatment using drugs is called buy 3 ml careprost with visa. Patients even have leukocytosis (left shift on differential), nausea, vomiting, and constipation. Abdominal pain sometimes precedes fever by a couple of hours and continues for 24 to 48 hours after the fever resolves. Other manifestations embody aseptic meningitis, pericarditis, febrile myalgia, and vasculitis. Livneh A, Langevitz P, Zemer D, et al: Criteria for the diagnosis of familial Mediterranean fever, Arthritis Rheum 40:1879-1885, 1997. Ozen S: Familial Mediterranean fever: revisiting an ancient disease, Eur J Pediatr 162:449-454, 2003. Diagnosis and management of most of these accidents are comparatively easy and direct. Injury to the small bowel secondary to blunt trauma, nonetheless, can current a much greater diagnostic dilemma. The importance of early diagnosis stems from the excessive morbidity and mortality rates seen in sufferers with delayed prognosis of these injuries. Associated morbidity is often secondary to the identification and immediate therapy of small-bowel harm. This distinction is important in resection secondary to the completely different digestive capabilities of the ileum and jejunum. The ileum is responsible for the absorption of vitamin B12 and the reabsorption of bile salts into the enterohepatic circulation. Location of the wound is also necessary in that the distal small bowel has the next anaerobic bacterial load. Therefore, distal small bowel injuries pose larger danger for postoperative infection. This is especially true with blunt belly trauma, which regularly has multiple related injuries that distract from refined abdominal findings. Injury to the small bowel should be dominated out in patients with penetrating belly injury. The small gut is the most incessantly injured intraabdominal viscus in sufferers with penetrating trauma as a end result of it occupies most of the abdominal cavity and is very mobile. Therefore, injury with penetration may happen in virtually any area of the peritoneal cavity. Evaluation of the complete size of the small bowel begins with the ligament of Treitz and continues to the ileocecal valve. Inspection includes examination of the complete mesentery and identification of hematoma or potential injury to the blood supply of the bowel. This technique eliminates additional trauma when changing the bowel within the peritoneal cavity, and it permits the surgeon to look at surrounding tissue to determine whether or not easy repair or resection is important. For small lacerations, closure should be accomplished in a transverse trend to the long axis of the bowel to forestall narrowing of the lumen. Resection should be carried out for a number of injuries in a brief segment or for a short phase with huge tissue destruction. For injuries involving bowel ischemia in a brief phase, easy resection with reanastomosis can be carried out. If a large section of the bowel is ischemic or if associated accidents are severe, resection should be limited and ought to be adopted by a deliberate second-look process and delayed anastomosis. The diagnosis of small-bowel trauma secondary to blunt harm is a controversial area. The presence of free fluid in the peritoneal cavity in the absence of solid-organ damage is extremely suggestive of small-bowel harm. Small intestinal harm could also be missed on radiologic research, particularly if the study is carried out within the early postinjury interval. Diagnostic laparoscopy has been used for analysis of peritoneal penetration after stab wounds and diaphragmatic penetration after thoracoabdominal penetrating accidents. Recent studies have supplied laparoscopy as an possibility for evaluating the small gut and mesentery for blunt trauma harm. Management of small-bowel accidents secondary to blunt trauma is just like the administration of penetrating accidents mentioned earlier. Postoperative management of sufferers with small-bowel injuries is usually dictated by the related accidents. However, this could be difficult in the patient who has sustained extended shock or a large mesenteric injury. Pikoulis E, Delis S, Psalides N, et al: Presentation of blunt small intestinal and mesenteric injuries, Ann R Coll Surg Engl eighty two:103-106, 2000. Rossi P, Mullins D, Thal E: Role of laparoscopy in the evaluation of belly trauma, Am J Surg 166:707-710, 1993. In North America, trauma is the leading explanation for demise in persons youthful than forty four years. The colon is the second most typical abdominal organ injured in penetrating trauma. Nonetheless, colonic damage after blunt stomach trauma is related to the next threat for complications and increased hospitalization. Furthermore, no diagnostic modality or mixture of findings can reliably exclude blunt injury to the colon. Therefore, a surgical strategy is really helpful early in the evaluation of stomach trauma suspected to contain the colon. From the Civil War to the Vietnam War, the mortality fee from colonic damage declined from more than 90% to less than 10%. Several components have contributed to the significant enchancment in survival in this affected person population, together with using a diverting colostomy, fluid resuscitation, availability of blood products, and broad-spectrum antibiotics. Preoperative antibiotics against cardio and anaerobic flora must be initiated early after the damage. Infection rates are considerably lowered when prophylactic antibiotics are given earlier than surgical procedure quite than throughout surgical procedure (7% vs. Moreover, advances in anesthesia and intensive care management continue to contribute to the general lower in morbidity and mortality. The mechanism of damage is usually one of the few elements distinguishing military from civilian damage. Combat lesions frequently outcome from high-velocity weapons and explosive gadgets, whereas civilian injuries usually end result from handguns, stab wounds, and blunt trauma. The degree of tissue damage is proportional to the kinetic power delivered by high-velocity weapons. Therefore, the overall prognosis for civilian trauma is better than for war-related accidents as a end result of civilian accidents are often a results of low-velocity weapons. Penetrating wounds involving the intraperitoneal parts of the colon incessantly happen in multiples, in distinction to lesions involving the ascending or descending colon. However, lesions within the retroperitoneal portions of the colon are often overlooked, resulting in severe anaerobic infection because of the vulnerability of the retroperitoneal house.
Careprost 3 ml buy mastercard
If the patient has diarrhea symptoms anxiety careprost 3 ml order amex, colonoscopy will doubtless reveal the traditional aphthous ulcerations of the bowel and "skipped" areas medicine side effects effective careprost 3 ml. Biopsy can be carried out on that space to confirm or rule out a analysis of terminal ileitis. If the affected person has perianal or anal illness, anoscopy should be performed in addition to colonoscopy to determine the websites of fistulization and fissures. Serologic markers are now obtainable and have been useful in confirming, and at occasions making, the diagnosis. Capsule endoscopy is gaining broad acceptance and can demonstrate ulceration and stricture of the small bowel. Doubleballoon enteroscopy could additionally be helpful in unsure cases, and biopsy materials may be obtained. Approximately 40% of sufferers have a pattern that entails the small and huge intestines, 30% have solely small bowel involvement, and 25% have massive bowel involvement. In Western nations, the incidence now ranges from 6 to 10 per one hundred,000 population, with a prevalence price of one hundred thirty per one hundred,000, and stories indicate the incidence is rising. Often, nonetheless, the illness goes undiagnosed or is delicate till a complication develops later in life. When the terminal ileum is concerned, the major presenting symptom is normally right decrease quadrant ache, which may be confused with appendicitis. At occasions, the abdominal ache could additionally be diffuse, but it varies with the area of the bowel involved. Physical examination may reveal no findings or a mass in the proper decrease quadrant. The most dramatic extraintestinal manifestations are pyoderma gangrenosum and perianal tags (skin), uveitis, iritis, and conjunctivitis (eye), and peripheral arthritides, sacroiliitis, and osteoporosis (bones). However, laboratory test outcomes and endoscopy can differentiate these ailments readily. However, most sufferers can obtain remission with one of the therapeutic medical regimens. When surgery is necessary, patients regularly obtain remission (see Chapter 152). When repeated surgical procedures and resections are necessary, quick bowel syndrome could develop. Diligent medical and dietary therapy can keep good quality of life in most sufferers. Surgical management is discussed in Chapter 152 and dietary administration in Section X. The decision to stick with medical therapy when the disease is insidious and causes modifications within the actions of every day residing is difficult. Surgery could be effective and might cause remission of signs, but surgical intervention has limits. Fistulae are more frequent and develop in 20% to 40% of sufferers, and most are enteroenteric or enterocutaneous. Antibiotic and medical therapy could additionally be useful and in some studies have proved efficient, however surgical therapy is usually essential. Obstruction is a typical complication, and although stents and dilatation are attempted, surgical intervention is critical to relieve progressive obstruction, which is commonest within the small bowel. Antibiotics, bowel relaxation, and intensive medical remedy, including anti�tissue necrosis issue, differ in T their capability to heal fistulae. These knowledge are several decades old, however, and new, more dramatic medical therapies may have the ability to avert the necessity for surgery in some patients. Nevertheless, the list of indications for surgery is lengthy, and its necessity turns into apparent in particular person sufferers (Box 152-1). Endoscopic evidence for recurrence ranges from 28% to 73% at 1 year and 77% to 85% at three years after ileal resection. Unfortunately, if repeat surgery is necessary, short bowel syndrome and malabsorption may develop. Older studies report recurrence in roughly 75% of sufferers at 10 years; again, long-term studies of the newer therapies are wanted to determine whether repeat surgical treatment is important. Unfortunately, some patients with indeterminate colitis inadvertently bear total colectomy with an ileoanal process only to expertise a recurrence of ileitis. Early studies reveal that laparoscopic surgery ends in lower incidence of minor complications and shorter periods of postoperative recovery. At times, however, there are "skipped" areas, and several segments should be resected. Severe recurrent obstruction results in vital resection and short bowel syndrome (see Chapter 115). Fistulization of the pores and skin, bladder, or vagina might require a extra aggressive or a surgical method because different organ methods are involved. However, if the abscess can no longer be managed, surgical drainage and resection are needed. If screening demonstrates dysplasia, cautious consideration have to be given to resection. The goal of remedy in perianal disease is aid of local ache and preservation of the sphincter. Local cleansing, Sitz baths, suppositories, and cleaning ointments to the area all are important. Metronidazole has been efficient in as many as 75% of patients, but several months of remedy are required, and illness does are inclined to recur. Lesions additionally heal with enough disease management; therefore, vigorous immunosuppression or biological remedy is indicated. If medical therapy fails, surgical drainage and placement of setons and mushroom catheters could additionally be needed. If perianal illness is severe and incontinence develops, proctectomy is necessary. A easy pores and skin tag may be enlarged and painless but could be rectally disfiguring ("elephant ears"). It is necessary to take a look at for native tenderness and look for discharge from a fistula. At instances, it could be too troublesome to carry out a rectal examination, but the anal ring could be teased, and sometimes a small fissure may be demonstrated with out coming into the anal ring. It is important to rule out any malignant lesion throughout early presentation in a patient who has not undergone endoscopic examination of the anal ring, and anesthesia could also be necessary to consider the rectum. Hereditary polyposis syndromes show that colorectal neoplasia has a genetic part (see Chapter 158). The genetic component is complex; the involved reader is referred to the Additional Resources.