
Bystolic dosages: 5 mg, 2.5 mg
Bystolic packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

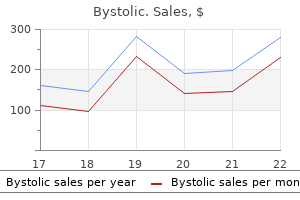
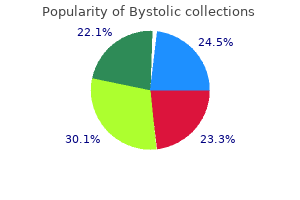
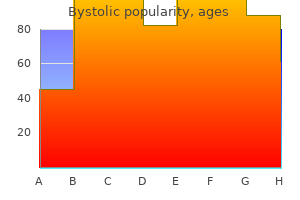
Bystolic 2.5 mg order fast delivery
In 1839 arrhythmia prognosis bystolic 2.5 mg on line, the Universite Catholique de Louvain heart attack ne demek cheap 2.5 mg bystolic free shipping, in Belgium, offered Schwann the chair of anatomy. However, his scientific productiveness during that period was restricted to one single significant paper exhibiting the essential position of bile, studied by establishing biliary fistulas in dogs. Although Schwann now not took an active half in scientific investigation, he remained an attentive observer of the advances in anatomy and physiology. Courtesy of Prentenkabinet, Centrale Bibliotheek, Katholieke Universiteit Leuven, Belgium. However, regardless of international recognition, this era was characterised by intense philosophical questioning, existential doubts, isolation, and melancholy. He however began the composition of a vast treatise, Theoria, which was supposed to be a common system of biology, ranging from cell concept, through mind operate and psychology, to theological and philosophical concerns. The sciatic nerve is the most important nerve within the lower extremity, deriving its root supply from the L4, L5, S1, and S2 spinal wire segments. It supplies motor innervation to the hamstring muscle tissue and all the muscle tissue within the decrease extremity beneath the knee. Its distal branches supply sensation to the decrease extremity below the knee, except for the medial leg and midfoot, that are provided by the saphenous nerve. The sciatic nerve consists of the medial and lateral trunks, which arise from the lumbosacral plexus and are united by a common nerve sheath as they leave the pelvis. The lateral trunk is shaped by the union of the posterior branches of the ventral rami of L4, L5, S1, and S2, and it becomes the frequent peroneal (fibular) nerve. The anterior branches of these ventral rami type the medial trunk, which becomes the tibial nerve. The sciatic nerve exits the pelvis via the larger sciatic foramen, also referred to as the sciatic notch. Here, it programs above the obturator internus muscle, and beneath the piriformis and gluteal muscle tissue. Occasionally, the sciatic nerve or certainly one of its trunks passes above or by way of the piriformis muscle. The sciatic nerve passes over the quadratus femoris muscle to enter the thigh, and it descends in the posterior thigh to reach the popliteal fossa, the place it often separates into the tibial and customary peroneal (fibular) nerves. The common peroneal (fibular) nerve divides below the fibular head into deep and superficial branches. The tibial nerve divides at the ankle degree below the lancinate ligament into the medial and lateral plantar nerves and a calcaneal department. The muscular tissues provided by the peroneal (fibular) and tibial nerve elements of the sciatic nerve are indicated in Table 1. Sciatic nerve issues check with the various situations that end in damage or dysfunction of the portion of the nerve between the sciatic notch of the pelvis and popliteal fossa. Injury within the sciatic notch region might occur after hip fracture or dislocation and also following hip surgery. The sciatic nerve may have a delayed harm after hip surgical procedure due to contact with either the wire or methacrylate cement used in the process. Injury within the gluteal region may follow Table 1 Sciatic nerve motor innervation Location of muscles provided Thigh Deep peroneal Superficial peroneal (fibular) Tibial Medial plantar Lateral plantar Short head biceps Leg a misplaced injection or a gluteal compartment syndrome resulting from gluteal muscle hemorrhage or contusion. Vascular abnormalities, such as pseudoaneurysm of the inferior gluteal artery, could compress the sciatic nerve. Whether compression by the piriformis muscle (piriformis syndrome) causes sciatic nerve dysfunction remains controversial. Acute external compression within the setting of coma, anesthesia, thigh tourniquet, positioning throughout surgical procedure or vaginal supply, and even the prolonged sitting with the thigh in opposition to a tough edge may injure the sciatic nerve. It may also be injured by direct compression from a tumor or an intrinsic nerve lesion, similar to a neurofibroma or Schwannoma. In premenopausal ladies, intermittent sciatic nerve dysfunction could occur in association with the menstrual cycle as a end result of ectopic deposits of endometrial tissue on the sciatic nerve. A gunshot wound might injure the sciatic nerve in either the sciatic notch space or the thigh. The sciatic nerve can also be injured by a systemic disorder that affects nerves in general The clinical features of sciatic neuropathy include weakness in sciatic-innervated muscular tissues and sensory symptoms in the sciatic nerve distribution. There could also be considerable individual variation in the symptoms and signs, relying on the parts of the nerve concerned and the nature and severity of the nerve damage. The weakness in sciatic neuropathy is distal predominant, involving both tibialand peroneal (fibular)-innervated muscular tissues. When severe, the affected person develops a flail foot with the complete loss of motor control. The sensory symptoms of sciatic neuropathy could include numbness, paresthesias, ache, and loss of sensation within the sciatic distribution. A complete sciatic nerve harm causes loss of sensation in the distal decrease extremity except for the medial portion, which is equipped by the saphenous nerve. The cutaneous innervation offered by branches of the sciatic nerve is summarized in Table 2. The sural nerve derives from branches of each the peroneal (fibular) and tibial nerves. In common, the peroneal (fibular) division (lateral trunk) of the sciatic nerve is extra vulnerable to injury than the tibial division (medial trunk). The higher vulnerability of the lateral trunk has been attributed to its larger fascicles and less connective tissue, and in addition its higher fixation and angulation on the sciatic notch. The analysis of a suspected sciatic nerve damage begins with a historical past and physical examination. The circumstances preceding the onset of sciatic nerve dysfunction could recommend one of the mechanisms of harm described above, which can help to establish the placement of nerve injury. The neurological deficits determined by physical examination can help point out which components of the sciatic nerve are injured. In the absence of historic data suggesting an apparent reason for sciatic neuropathy, diagnostic considerations ought to embrace other peripheral nervous system issues affecting the decrease extremity. Because the symptoms and examination findings caused by sciatic neuropathy overlap with those of lumbosacral radiculopathies, lumbosacral plexopathies, and mononeuropathies of the peroneal (fibular) and tibial nerves, it is in all probability not potential to differentiate these circumstances strictly on the basis of historical past and bodily examination. In many instances, electrodiagnostic research present the knowledge necessary to differentiate sciatic neuropathy from different situations. Magnetic resonance imaging research or computerized tomography scans of the lumbar backbone, hip, or thigh can further help to differentiate between these conditions. The sural and superficial peroneal (fibular) sensory nerve action potentials are usually absent or are of reduced amplitude. Needle electromyography typically reveals fibrillation potentials in sciatic-innervated muscle tissue and the absence of fibrillation potentials in nonsciatic-innervated muscles, including the lumbosacral paraspinal muscles. Motor unit motion potential abnormalities develop in sciatic-innervated muscle tissue when axonal regeneration results in muscle fiber reinnervation. The historical past and findings on examination and electrophysiological research might affect the decision regarding the necessity for imaging studies.
Syndromes
- Infection of the jaw or face
- Your surgeon will make a 10-inch-long cut in the middle of your chest.
- Rapid breathing (tachypnea)
- Chromosome studies
- Blood vessel abnormality
- Decreased alertness or orientation
Bystolic 5 mg cheap visa
Selective brokers that both block or improve activity at particular nicotinic receptor sites may result in arterial insufficiency discount bystolic 2.5 mg online more promising therapies for cognitive dysfunction blood pressure and pulse rates 5 mg bystolic purchase, particularly these conditions involving attention, similar to attention-deficit dysfunction, and varied dementias, particularly frontal lobe dementias. More is known about nicotinic receptors than perhaps another receptor in the brain. However, this knowledge demonstrates the complexities that methods neuroscience exposes by method of understanding interactions amongst medication and receptors in numerous neural methods. Colquhoun D, Unwin N, Shelley C, Hatton C, and Sivilotti S (2003) Nicotinic acetylcholine receptors. Diagnosis in these latter cases is commonly missed, notably in the absence of a household history. Interstitial lung disease is common and a supply of main morbidity in patients with kind B disease, in whom survival to adulthood can happen. Lipid alterations, together with the accumulation of sphingolipids, likely affect the membranes of various subcellular compartments of neurons and glial cells, and result in anomalies in signaling pathways, neuronal polarization, calcium homeostasis, synaptic plasticity, myelin manufacturing, or immune response. In severely affected cases, ascites and severe liver disease could additionally be evident in the neonatal period. Other infants could present with extended jaundice, followed by hypotonia and developmental delay that manifest during early childhood. The classic presentation occurs in mid- to late childhood with the insidious onset of ataxia and the next development of dystonia and seizures. Ultimately, sufferers manifest with dysarthria and dysphagia, making oral feeding unimaginable. Careful considerations should be given in instances the place the diagnosis relies only on molecular evaluation as a end result of the importance of a sequence alteration could also be uncertain in the following circumstance: mutations not previously reported or not supported by expression studies that present functional impairment of the cognate protein. Analysis may be performed on chorionic villous sampling or amniocytes for prenatal diagnosis, and the same method could be applied for preimplantation genetic testing. Gene remedy is also under investigation, but at current solely preclinical studies (in animal models of the disease) have been conducted. Most typically the dream emotion is anxiousness but other emotions like disappointment, anger, and disgust could be main options of a nightmare. The most typical nightmare themes are being chased, falling, being paralyzed, being late, and demise of shut persons. On awakening, the person is totally awake, oriented to the surroundings, and in a position to give a full account of the nightmare. Recent findings indicate that treating particularly nightmares in patients with depression who suffer from nightmares regardless of their normal remedy (pharmacological or psychotherapeutic) successfully reduced nightmare frequency. Posttraumatic reenactments are replays of traumatic events experienced in their waking lives. Interestingly, the therapeutic strategy to cope with nightmares (imagery rehearsal therapy) is effective for each forms of nightmares (idiopathic nightmares and posttraumatic reenactments). Nocturnal panic assaults have their peak after awakening (usually accompanied by demise anxiousness and the somatic symptoms of a panic assault such as hyperventilation, paresthesias (numbness or tingling sensations), and sweating), whereas the misery from a nightmare decreases on awakening. It should be famous, however, that nightmares can set off nocturnal panic assaults in sufferers with panic disorder. A careful psychiatric interview ought to be thought of, as nightmare frequency is increased in mental disorders corresponding to depression and anxiety disorders. A history of drug use should be elicited, as nightmares are related to a broad number of compounds, corresponding to serotonin reuptake inhibitors, cholinesterase inhibitors, and antihypertensive medicines. Nightmares and Sleep Quality Even though nightmares are categorized as a parasomnia, a number of researchers conceptualize nightmare disorder as a type of insomnia as a outcome of sleep high quality is drastically reduced in these patients, presumably as a end result of the direct effect the nightmare has on returning back to sleep and indirect effects as a result of worries that nightmares could occur after falling asleep. Differential Diagnosis Nightmares should be differentiated from night time terrors, posttraumatic reenactments, and nocturnal panic attacks. There is a gender distinction in nightmare frequency, with ladies tending to 592 Encyclopedia of the Neurological Sciences, Volume three doi:10. This distinction is most pronounced for adolescents, and younger and middle-aged adults, and virtually nonexistent for youngsters younger than 10 years or within the elderly (older than 60 years). In different words, even when the circumstances that originally triggered the nightmares Therapy Indications for treatment are sophisticated by the frequency of nightmares in the common inhabitants and lack of a clear definition of pathological nightmare dysfunction. Cognitive-behavioral remedy approaches, corresponding to systematic desensitization have been very efficient. The first step is confrontation, which is just carried out by writing down the dream. In the second step, the affected person makes use of lively creativeness to produce a new ending for the dream, i. Ideally, the therapist encourages energetic methods to enhance creation by the affected person and refrains from giving recommendations. If the affected person suggests avoidance habits (hiding or flying away), the therapist asks whether there are further choices to cope with the situation current in the nightmare. In view of those theories, new endings that embody communication with threatening dream characters are inspired. Children are requested to complement the dream drawing with the elements that they create and are helpful. Interestingly, scientific expertise signifies that if nightmares persist, the impact of the intervention often generalizes to affect different nightmare conditions. Several randomized controlled trials indicate that imagery rehearsal therapy is very effective in lowering nightmare frequency. Etiology Many hypotheses have been formulated relating to the origin of nightmares ranging from furry beasts sitting on the chest of the dreamer, oxygen scarcity during sleep attributable to externally impaired respiration (bedspread over the face), or heavy and spicy meals eaten late within the night. Findings clearly assist a disposition-stress mannequin explaining nightmare etiology. A large-scale Finnish twin examine showed that the concordance rate for frequent nightmares is considerably higher in monozygotic than dizygotic twins, supporting a genetic factor in nightmare etiology. Although trait anxiousness was not constantly associated with nightmare frequency in adults, findings in children clearly indicate that trait anxiety is related to elevated frequency. In addition, acute stressors corresponding to relationship issues, work-related stress, and loss of close family members can improve nightmare frequency. This is in line with the so-called continuity hypothesis of dreaming that asserts that desires mirror waking life experiences, such that the anxiety, or other unfavorable feelings of the day, are carried into dreams. In brief, the prevalence of nightmares is explained by a mixture of vulnerability and current stressors. In addition to these two elements, nightmares are often an anxiety phenomenon (like phobias and panic disorder), and avoidance habits tends to become entrenched. Interestingly, most studies indicate that the reduction of nightmares also improves different clinical symptoms, together with depressive mood, daytime functioning, and sleep quality. Schredl M (2010) Nightmare frequency and nightmare matters in a representative German sample. Schredl M and Reinhard I (2011) Gender differences in nightmare frequency: A meta-analysis.
Cheap 5 mg bystolic
Subsequent experiments showed that sympathetic nerve stimulation additionally released a humoral factor that could mimic the consequences of nerve stimulation blood pressure chart standing discount bystolic 2.5 mg visa. During the intervening many years blood pressure standards cheap bystolic 2.5 mg free shipping, the factors for neurotransmitter status have been developed and revised, further neurotransmitter candidates have been recognized, mechanisms for neurotransmitter launch and inactivation have been elucidated, and neurotransmitter receptors and transporters have As the function of acetylcholine as a neurotransmitter, especially in the autonomic nervous system and at the neuromuscular junction, began to acquire broad acceptance, the possibility was entertained that different transmitters existed as nicely. First, neurotransmitters should be present in nerve terminals in order that they can be released in response to stimulation. In the case of acetylcholine, the precursor is choline, which is converted to acetylcholine via the enzymatic action of choline acetyltransferase. A corollary of the requirement for neurotransmitter localization to nerve terminals is that the enzymes responsible for transmitter synthesis should also be found there. Because the power of neurons to talk rapidly requires a preformed pool of transmitter molecules, nerve terminals should also possess websites for storing these molecules, and these sites often take the form of membrane-bound vesicles. It is now identified that such stimulation prompts sodium channels, which admit extracellular sodium into cells, leading to the depolarization of the neuronal membrane. Depolarization, in turn, leads to the opening of calcium channels, and the extracellular calcium that enters the nerve terminal through these channels triggers neurotransmitter release. Release happens at specialized, lively zones of the neuronal membrane and outcomes from the fusion of neurotransmitter-containing vesicles with the cell membrane, adopted by exocytosis of their contents. Each numbered step within the strategy of neurotransmission also represents a possible target for drug motion, as detailed within the textual content for particular person neurotransmitter methods. Dale was the primary to present that a given neurotransmitter (acetylcholine) could act through different receptors (nicotinic and muscarinic), and a number of receptors for a single transmitter at the second are recognized to be the rule. Neurotransmitter receptors are categorized into two classes: ionotropic receptors, which modulate ion fluxes, and metabotropic or G proteincoupled receptors, which activate chemical second messengers (Table 1). In some instances, receptors for a neurotransmitter could be discovered on the identical neuron from which the transmitter is launched. Fourth, neurotransmitters must be able to inactivation to restrict their actions in time and house, and subsequently mechanisms for inactivation must exist at or near their sites of launch. Acetylcholine is inactivated by enzymatic breakdown, during which acetylcholinesterase is employed to regenerate choline. However, other transmitters are inactivated by removing from the synaptic cleft by way of reuptake into neurons or glia. Numerous medicine and a variety of other neurological disorders have an effect on these transmitter techniques (Tables 2 and 3). Acetylcholine Acetylcholine is synthesized from choline and acetyl coenzyme A by the motion of choline acetyltransferase. Acetylcholine is degraded extracellularly by acetylcholinesterase, which generates choline and acetate, the previous of which undergoes reuptake into neurons, offering the precursor for the resynthesis of acetylcholine. Norepinephrine and Epinephrine Norepinephrine and epinephrine (as nicely as dopamine) are catecholamines, and are synthesized from the precursor amino acid tyrosine by a sequence of enzymatic steps. Released norepinephrine binds to a- or b-adrenergic receptors, and its action is terminated by reuptake. Norepinephrine is the transmitter of sympathetic postganglionic fibers and of central pathways that originate within the locus coeruleus and project to the cerebral cortex, cerebellum, spinal wire, and other areas. A defect in norepinephrine synthesis has been implicated in pure autonomic failure. Drugs that alter adrenergic neurotransmission embrace agents that stimulate norepinephrine launch and which are used to treat narcolepsy (methylphenidate and dextroamphetamine) and antimigraine agents that inhibit norepinephrine reuptake (tricyclic antidepressants) or that block b-adrenergic receptors (propranolol). Dopamine receptor antagonists are used to treat chorea and other hyperkinetic motion disorders (haloperidol and phenothiazines) and migraine (metoclopramide). The most prominent serotonergic pathway originates in the brainstem raphe nuclei and projects diffusely all through the mind and spinal wire. A dysfunction of central serotonergic transmission has been proposed to underlie the pathophysiology of migraine. Histamine Dopamine the synthesis of dopamine was mentioned previously, and its enzymatic breakdown proceeds as described for norepinephrine, except that the most important metabolite is homovanillic acid. Histamine-containing neurons within the central nervous system are concentrated primarily in the hypothalamus and project extensively to the mind and spinal twine. Histamine H1 receptor antagonists (antihistamines), such as meclizine, promethazine, and dimenhydrinate, are used to treat vertigo. Glutamic Acid Glutamic acid, or glutamate, is the most ample excitatory transmitter in the central nervous system. Following its launch, the action of glutamic acid is terminated by reuptake, predominantly into astrocytes. Glutamic acid interacts with both ionotropic and G protein-coupled, or metabotropic, receptors. Glutamic acid-containing neurons are distributed extensively all through the central nervous system, and embrace pyramidal cells of the cerebral cortex and cerebellar granule cells. Domoic acid, a toxin current in blue mussels, is assumed to produce symptoms via its interplay with glutamic acid receptors. Glycine release is impaired in tetanus, and glycine receptor blockade is liable for the signs of strychnine poisoning. Others Several extra molecules have been proposed as typical (amine or amino acid) neurotransmitters, including adenosine, aspartic acid, and taurine. Nonclassic Neurotransmitters Several molecules have a task in communication between neurons, though they differ from classically outlined neurotransmitters in important respects. Thus, whereas basic transmitters are synthesized in nerve terminals, packaged in synaptic vesicles, launched by exocytosis involving the fusion of synaptic vesicles with the cell membrane, and bind to receptors on the postsynaptic membrane, nonclassic neurotransmitters depart from a number of of these options. In some instances, a basic neurotransmitter and a neuropeptide coexist in and are released together from the same neuron. Neuropeptides embrace endocrine hormones and releasing elements similar to corticotrophin-releasing hormone, gastrointestinal hormones such as cholecystokinin, neurokinins corresponding to substance P, and opioid peptides such because the enkephalins and endorphins. Amino Acids As discussed in Classic Neurotransmitters, a number of amino acids seem to operate as basic neurotransmitters, however a extra moderen amino acid transmitter candidate, D-serine, is unconventional in certain respects. The most notable of those is that D-serine is launched from glia quite than from neurons. In greater mammals, most amino acids happen in the L-isoform, whereas most sugars happen within the d-isoform, perhaps explaining why D-serine has been completely missed in the past years. The pathway for its manufacturing and launch from Glycine Glycine is a major inhibitory transmitter within the spinal cord. Classic amine and amino acid transmitters are synthesized in nerve terminals, saved in and released from vesicles, act on membrane-bound receptors, and are inactivated by metabolic breakdown and reuptake. When glutamate is released into the synapse, it activates metabotropic glutamate receptors in the close by glia. Drugs that alter D-serine production may represent a model new avenue of therapy for these illness states.
Buy bystolic 5 mg with mastercard
The cells of those rosettes encompass a central lumen outlined by a basement membrane analogous to the external limiting membrane of the retina wide pulse pressure in young adults bystolic 5 mg visa. However pulse pressure 74 discount 5 mg bystolic visa, photoreceptor differentiation is demonstrable by characteristic immunopositivity of the luminal membrane for retinal S-antigen. Ependymal rosettes are present in benign to intermediately aggressive ependymal tumors such as conventional ependymoma, anaplastic ependymoma, and angiocentric ependymal tumor (also known as angiocentric glioma). Ependymal rosettes are additionally occasionally found deep to the traditional ependymal lining of the brain. In no much less than some instances, these symbolize outpouchings or branches of the ependymal lining of the ventricular system. These outpouchings could also be partially obliterated throughout brain development, much like the partial obliteration of the central canal of the grownup spinal twine, ensuing within the formation of benign isolated small canals that seem as rosettes on cross-section. The central lumen of the ependymal rosette is commonly immunoreactive Encyclopedia of the Neurological Sciences, Volume four doi:10. Similar flower-like buildings missing a central lumen occurring within a retinocytoma or retinoblastoma are referred to as fleurettes and are thought to be much more differentiated and will predict a much less aggressive scientific course in retinoblastomas. To distinction them from perivascular pseudorosettes, ependymal rosettes are moreover generally recognized as true ependymal rosettes. The terminal bar and intra-lumenal cilia are seen within the bigger rosette to the left. Note hyperchromatic nuclei, pseudostratification of cells and multiple intra-rosette mitotic figures (arrows). Myxopapillary ependymomas are typically benign tumors that happen in the cauda equina space of the spinal cord inside the subarachnoid house. This is believed to be the result of myxoid degeneration of the ependymal cell processes projecting onto the central, normally hyalinized, capillary, presumably secondary to poor blood supply to the tumor. Astroblastomas are uncommon glial tumors largely composed of one other unique kind of perivascular pseudorosette. The skinny tapering cell processes projecting toward the central blood vessel are tightly packed and troublesome to distinguish. Note the relatively clear space containing scant delicate mobile processes (myxoid degeneration) between the cells and hyalinized central blood vessel. Note the easily identifiable nucleoli of the monopolar astroblastoma cells and the way a variety of the cell endfeet flare out wider as they contact the vessel basement membrane (arrows). Certain properties of rotenone make it best to be used as an agricultural insecticide. It is a multicarbon ring steroid-like compound that, like many such chemical compounds, is susceptible to photodecomposition by ultraviolet mild. Rotenone absorption by way of the gastrointestinal tract is minimal, and the small quantities are readily degraded by the liver. Mode of Toxicity the poisonous nature of rotenone derives from its high affinity to the complex I holoenzyme (complex I) of mitochondria and resulting inhibition of mobile respiration. Complex I is positioned in the inner membrane area of mitochondria and protrudes into the matrix, serving as the primary web site of access for electrons into the respiratory chain. Thus, the positioning of action for rotenone has been discovered to be at the catalytic site for the reduction of ubiquinone to dihydroubiquinone, which is the final stage of electron transfer in complicated I. The gradient established by complex I may participate within the regulation of the mitochondrial permeability transition pore, which is a big calcium-dependent pore situated within the inner membrane of the mitochondria. Opening this pore, which can occur during rotenone inhibition of advanced I, results in mitochondrial dysfunction, the release of proapoptotic factors corresponding to cytochrome c, and subsequent cell dying. The ingestion of diluted rotenone answer could lead to stomach irritation or vomiting. Inhaling rotenone results in elevated respiration adopted by depression and convulsions. Rotenone could additionally be extra poisonous when inhaled and has been reported to induce dermatitis, ulcers in the nostril, and irritation of mucous membranes. Chronic exposure to rotenone in rats leads to growth retardation and vomiting and will produce changes in the liver, where rotenone is metabolized. Rotenone, deguelin, and tephrosin are all thought to work through inhibition of complicated I in the mitochondria. The use of rotenone in fisheries is often restricted to utility earlier than stocking the fishery so as of get rid of undesirable fish that would compete with the specified species. In both situations, the exposure of the handler is anticipated throughout application of the rotenone, and of people in close proximity to the body of water where rotenone is utilized. The application of rotenone is achieved with the utilization of varied forms of gear, ranging from helicopters for spraying lakes, boats with oversurface booms or underwater hoses, and people using backpack sprayers. Therefore, exposure to rotenone might occur by way of inhalation, dermal absorption, and the ingestion of fish collected from areas the place rotenone has been utilized. Owing to the comparatively short half-life of rotenone toxicity, exposure risk is taken into account to be largely acute and short-term. Common symptoms following publicity are eye irritation, dermal irritation, throat irritation, and nausea. This has led to the examination of the potential threat that advanced I-inhibiting pesticides, corresponding to rotenone, might pose to the final inhabitants. Rotenoids Rotenoids are naturally occurring compounds which are chemical cousins of rotenone and that share a capability to inhibit complicated I of the electron transport chain. They are often synthesized in the identical vegetation as rotenone and thus are present in extracts containing rotenone. For example, both rotenone and deguelin are present within the dice resin of Lonchocarpus utilis. Deguelin is a chemical that has insecticide and piscicide activity and displays anticancer properties. Like rotenone, deguelin administration may cause neurodegeneration, the lack of dopamine cells in the brain, and parkinsonian signs in rats. Neurological Effects Few neurological signs have been reported from rotenone publicity, but they embody peripheral neuropathy, numbness, and tremor. No deaths have been reported during normal use of rotenone, although fatalities from intentional ingestion of rotenone have been reported. Therefore, intravenous publicity allows for rotenone to reach the central nervous system, the place its inhibition of mitochondrial perform could be toxic. The rubella virus specializes in infecting people as a outcome of Homo sapiens are the exclusive natural host. The virus savors crowded situations as a end result of unfold occurs by way of inhaled infected droplets. Once the contaminated droplets are inhaled, replication occurs within the buccal mucosa adopted by infection of the lymphatic tissue within the nasopharynx and higher respiratory tract. The lymphatic system performs an necessary position in establishing systemic infection, however viremia disseminates the disease extra shortly. Rubella reigns all through the world and recrudescence of infection continues to occur when new unprotected generations are uncovered to the virus.
Discount bystolic 5 mg free shipping
The medical phenotype of 4-hydroxybutyric aciduria is notably heterogeneous hypertension prevention buy 5 mg bystolic with mastercard, even inside sibships heart attack from stress bystolic 2.5 mg low cost. Neuropsychiatric signs and behavioral problems are prominent and embrace sleep issues, inattention, hyperactivity, and anxiousness. It has been proposed that N-acetyl-L-aspartate might function as a molecular water pump in myelinated neurons, transporting water in opposition to its gradient from neurons to oligodendrocytes. Progressive macrocephaly, hypotonia with outstanding head lag, seizures, and the loss of beforehand acquired expertise are often discovered. As the illness progresses, affected kids develop optic nerve atrophy, pyramidal signs, and finally a decerebrate state. Neuroimaging studies show symmetrical leukodystrophic changes with lack of arcuate fibers of the cerebral white matter, and neuropathological studies present spongiform degeneration, significantly of the cortex and subcortical white matter. Lithium citrate, which induces a mild decrease in mind N-acetylasparte concentrations, may be beneficial. Dietary acetate supplementation with glyceryl triacetate is presently evaluated as novel remedy technique. Furthermore, L-lysine can be elevated demonstrating secondary impairment of the saccharopine pathway of mitochondrial lysine oxidation, which requires 2-oxoglutarate as cosubstrate. Most patients with L-2-hydroxyglutaric aciduria observe a characteristic disease course. In infancy and early childhood, mental and psychomotor improvement appears regular or solely slightly retarded. Thereafter, seizures, progressive ataxia, pyramidal tract signs, slight extrapyramidal signs, and progressive psychological retardation become the most obvious medical findings. Sometimes psychological deterioration is quickly progressive, and a single affected person with fatal neonatal consequence has been described. In some patients, various varieties of malignant mind tumors, similar to medulloblastoma, glioblastoma multiforme, astrocytoma, and primitive neuroectodermal tumor, have been reported. The use of riboflavin therapy has been used in a few patients resulting in partial enchancment of neurological symptoms and decreased urinary excretion of L-2-hydroxyglutarate. D-2-Hydroxyglutaric Aciduria L-2-Hydroxyglutaric L-2-hydroxyglutaric Aciduria aciduria is a uncommon autosomal recessive illness of unknown prevalence first described in 1980, which is characterized by progressive lack of myelinated arcuate fibers and a spongiform encephalopathy. The chromatographical separation of these enantiomers can be performed using derivatization with a chiral reagent or a chiral stationary section. Prenatal analysis has been successfully carried out by correct willpower of D-2-hydroxyglutarate in amniotic fluid in addition to by molecular diagnosis. Patients with D-2-hydroxyglutaric aciduria exhibit a more variable phenotype than sufferers with L-2-hydroxyglutaric aciduria. Most patients endure from a extreme early onset epileptic encephalopathy, though a considerable subgroup showed gentle signs or have been even asymptomatic. Severely affected patients typically current with extreme muscular hypotonia, intractable seizures, irritability, cortical blindness, extreme improvement delay, and cardiomyopathy. Less severely affected Organic Acid Disorders 691 sufferers exhibit principally mild neurological symptoms together with slight developmental delay, delayed speech, and febrile convulsions. Mevalonic Aciduria Mevalonic aciduria, first described in 1986, inherited as an autosomal recessive trait, is a dysfunction of the peroxisomal ldl cholesterol and nonsterol isoprene biosynthesis attributable to mevalonate kinase deficiency. Mevalonate kinase catalyzes the phosphorylation of mevalonic acid, the product of the reduction of 3-hydroxy-3-methylglutaryl-CoA to 5-phosphomevalonic acid. Pathogenesis of mevalonic aciduria stays unclear, however scientific symptoms seem associated to lack of ldl cholesterol and other isoprenoids quite than to accumulation of mevalonic acid. The most severely affected patients die in infancy with profound developmental delay, dysmorphic features, cataracts, hepatosplenomegaly, lymphadenopathy, anemia, thrombocytopenia, diarrhea, and malabsorption. A characteristic feature of mevalonic aciduria is recurrent crises with fever, lymphadenopathy, improve within the size of liver and spleen, arthralgia, edema, and morbilliform rashes without metabolic derangement. In between crises, standard chemical investigations are normal except for elevated serum creatine kinase in most sufferers. Patients with full lack of enzymatic function usually have a less extreme illness course as though having considerable residual activity suggesting that the nonenzymatic operate of the faulty protein is important for the mechanisms underlying neurodegeneration. Heterozygous women could additionally be asymptomatic or may have variable stationary psychomotor retardation with impaired hearing. The prognosis is mostly poor, with death in early childhood in severely affected sufferers. Branched-Chain Organic Acid Disorders Metabolic derangement on this illness group results from inherited defects of specific enzymes involving the catabolism of branched-chain amino acids. Neurological symptoms are particularly frequent however other organs, similar to kidneys, liver, pancreas, skeleton, and coronary heart muscle, may be concerned as nicely. Methylmalonic Aciduria Methylmalonic aciduria is the biochemical hallmark of a heterogeneous group of inborn errors of metabolism with a cumulative prevalence of no much less than 1:50 000 newborns. Elevations of 2-ethylhydracrylic acid and 3-hydroxyisobutyric acid in urine may be discovered. Affected boys usually develop truncal 692 Organic Acid Disorders epilepsy, usually happen. In these sufferers, as a substitute of having a neonatal decompensation, neurological symptoms may progress slowly over several years. Some accumulating organic acids and CoA esters, such as 2-methylcitric acid, propionyl-CoA, and methylmalonic acid, are thought-about to inhibit mind energy metabolism and hepatic ammonia cleansing, thus inflicting neuronal harm (see Propionic Aciduria). Metabolic remedy is based on dietary restriction of protein and supplementation of L-carnitine. The prognosis of methylmalonic aciduria is uncertain and depends on many parameters such because the age at onset of first symptoms, cobalamin responsiveness and the underlying enzymatic defect, and the extent of residual exercise. Neurological signs and signs are frequent, together with the event of chorea and dystonia related to basal ganglial hypodensities in neuroimaging studies, suggesting selective vulnerability of basal ganglia, mostly affecting the putamen. Furthermore, affected patients show developmental delay and psychological retardation and seizures. Metabolic treatment is predicated on the dietary restriction of isoleucine, valine, methionine, and threonine as well as supplementation with L-carnitine. Furthermore, development of propionate-producing gut micro organism is limited by intermittent utility of metronidazole or colistin. Elevated propionyl-CoA and propionic acid interfere with quite a lot of metabolic pathways. Pathophysiologically, relevant actions are an inhibition of carbamoyl phosphate synthetase 1, an enzyme of the urea cycle, and limited manufacturing of its cofactor, N-acetylglutamate secondary to 2-oxoglutarate-requiring glutamate synthesis resulting in hyperammonemia throughout metabolic crises. Furthermore, propionyl-CoA inhibits pyruvate dehydrogenase complex and 2-methylcitric acid inhibits Krebs cycle enzymes, leading to hyperammonemic encephalopathy, lowered adenosine triphosphate synthesis and elevated manufacturing of lactic acid and ketone bodies. Van Schaftingen E (2009) L-2-hydroxyglutaric aciduria, a disorder of metabolite repair. Millions of individuals worldwide are uncovered to organic solvents, primarily in the occupational setting, as these compounds are used as degreasers, constituents of paints, lacquers, inks, dyes and adhesives, intermediates in chemical synthesis, parts of fuel additives, and in dry cleaning. This is followed by a last stage of dementia, with marked international deterioration in mind and reminiscence, which is poorly reversible but typically nonprogressive on termination of publicity. Although its acute toxicity is low, persistent dermal or inhalation exposures trigger a sensorimotor polyneuropathy that resembles a dyingback neuropathy (a distal axonopathy).
Meadow Routs (Marsh Marigold). Bystolic.
- How does Marsh Marigold work?
- Dosing considerations for Marsh Marigold.
- Pain, cramps, problems related to menstruation or "periods," bronchitis, liver problems, constipation, fluid retention, high cholesterol, low blood sugar, cleaning skin sores, and other conditions.
- Are there safety concerns?
- What is Marsh Marigold?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96645
2.5 mg bystolic effective
The pterygopalatine ganglion neurons innervate the lacrimal glands heart attack get me going extended version 2.5 mg bystolic order overnight delivery, the blood vessels of the attention blood pressure and caffeine bystolic 2.5 mg buy low price, the blood vessels and secretory glands of the nasal cavity and palate, and the cerebral blood vessels. Parasympathetic Output to Cranial Effectors the cranial parasympathetic neurons are situated in the common visceral efferent column of the midbrain, pons, and medulla. The parasympathetic fibers run superficially within the inferior subdivision of the oculomotor nerve through the cavernous sinus and then the superior orbital fissure to reach the orbit where they synapse on the ciliary ganglion, located in opposition to the surface of the optic nerve. There are a quantity of microganglia in association with the Encyclopedia of the Neurological Sciences, Volume three doi:10. Vagal Pathways General Features the vagus nerve (cranial nerve X) supplies the most widespread parasympathetic output to the visceral organs, including the airways, coronary heart, proximal part of the gastrointestinal tract, pancreas, and liver. There are several subpopulations of ganglion neurons that receive preganglionic inputs from the vagus nerve. Vagal influence decreases in the course of the inspiratory section and increases during the expiratory section of respiration, resulting in respiratory sinus arrhythmia. Heart rate variability is inversely correlated with age in resting regular subjects. The vagus also reduces atrioventricular conduction and will increase the ventricular refractory period. Vagal stimulation additionally reduces contractility of the atria and to a much lesser extent the ventricles. Respiratory Tract the vagal management of the respiratory tract entails two outputs (1) branchiomotor outputs from neurons within the nucleus ambiguous to striated muscle tissue of the pharynx, larynx, and higher esophagus and management swallowing and phonation and (2) parasympathetic outputs control airway resistance and secretions. The vagal parasympathetic control of the airways is mediated via microganglia associated with the pulmonary plexus. Most neurons are cholinergic and stimulate bronchial constriction by way of M3 muscarinic receptors. Gastrointestinal Tract Vagal inputs to the alimentary tract affect primarily the esophagus and abdomen. The importance of vagal control decreases dramatically in the small bowel and colon, the place motility and secretion are primarily managed by native reflexes. The esophageal branches are positioned above and under the pulmonary branches and form the esophageal plexus. The vagus could elicit both contraction or relaxation of the decrease esophageal sphincter. In the abdomen, the vagus causes leisure of easy muscle in the proximal stomach (receptive relaxation) to accommodate the meal and stimulates motility in the distal stomach and thus gastric emptying. However, the vagus may also inhibit gastrin secretion through a postganglionic cholinergic stimulation of D cells that release somatostatin. During micturition, descending inputs from the pontine micturition center elicits coordinated activation of the sacral preganglionic neurons (promoting bladder detrusor contraction) and inhibition of Onuf motoneurons (and thus relaxation) of the exterior sphincter. Vagal preganglionic branches to the celiac and superior mesenteric plexuses reach small ganglia within the pancreas. The vagus stimulates a resting secretion of bicarbonate, but its major impact is to increase enzyme secretion via cholinergic muscarinic mechanisms. Vagal inputs improve secretion of somatostatin and pancreatic polypeptide which, in turn, inhibits enzyme and bicarbonate secretion. Colon and Rectum Preganglionic neurons of the sacral spinal cord project through the pelvic nerve and plexus to neurons located either in myenteric plexus in the wall of the descending and sigmoid colon and rectum or extramural neurons located in ganglia distributed within the distal end of the pelvic nerves. These extramural neurons each innervate the graceful muscle immediately and project to the myenteric plexus. Many extramural neurons receive inputs from distension-sensitive myenteric neurons and project again by way of the pelvic ganglia to the spinal cord. Parasympathetic Control of the Pelvic Organs General Features the sacral parasympathetic outflow is crucial for evacuation of the bladder and rectum and reflex vasodilatation of the erectile tissue in sexual organs of women and men. There are advanced interactions among the parasympathetic, sympathetic, and somatic outputs to the pelvic organs. The sympathetic system promotes emission of sperm and contributes to psychogenic erection. The easy muscle of the vas deferens, seminal vesicles, and prostate gland receive excitatory noradrenergic innervation from neurons within the pelvic plexus that receive preganglionic inputs via the hypogastric nerves. Erection requires vasodilatation of penile arteries and relaxation of venous sinusoids in the erectile tissue, resulting in enhance in blood move and enlargement of the sinusoidal areas. Very delicate weak point or paresis will not be recognized by formal manual muscle testing of isometric strength, however it could lead to actions that are abnormally sluggish or clumsy. The time period paresis is derived from the Ancient Greek word, paresB, which suggests neglecting or disregarding. The time period paresis is often modified by a prefix indicating the placement of the weak spot, as proven in Table 1. This system of classification relies on isometric energy testing and due to this fact fails to recognize the mildest forms of paresis with normal isometric strength however irregular motility. The cause of paresis should be identified and handled before it might possibly cause frank weak point. Tests that may detect delicate paresis include the pronator sign for the higher extremity and heel strolling for the decrease extremity. The pronator signal is elicited by asking sufferers to maintain their arms outstretched in front of them, with the palms up, while keeping their eyes closed. A positive signal is elicited when the hand tends to pronate and sometimes the elbow tends to turn into slightly flexed. Heel strolling will facilitate the recognition of gentle paresis within the leg by enhancing the difference between the two toes, with the weak one displaying foot dorsiflexion weak point that may not be appreciated in common gait or by isometric guide testing. Some of the extra frequent etiologies are listed in Table three, based on the kind of onset and website of involvement. Lesions in the proprioceptive pathways of the higher extremities also can trigger clumsiness of movements of the affected limb, which may mimic the paresis attributable to lesions of the corticospinal tract. The Sylvian fissure forms the inferior boundary of the parietal lobe, a border that becomes increasingly obscure within the zone shared by the parietal, temporal, and occipital lobes. On the outer floor of the hemisphere, these embody the postcentral gyrus, the supramarginal gyrus, the angular gyrus, and the superior parietal lobule. The intraparietal sulcus separates the superior parietal lobule from the supramarginal and angular gyri. On the inner surface of the hemisphere, the paracentral lobule straddles the central sulcus. The postcentral gyrus receives afferent projections from the ventral tier of thalamic nuclei. These fibers, conveying somatosensory information from the contralateral body, terminate somatotopically on the posterior bank of the central sulcus. Somatosensory information from this space tasks to association cortex within the superior parietal lobe.
Bystolic 5 mg discount overnight delivery
Neurosyphilis is simply the incidence of neurological problems due to heart attack 36 cheap 5 mg bystolic with amex infection with T blood pressure of 100/60 order 5 mg bystolic. The spectrum of clinical sickness related to neurosyphilis is exceptionally broad. The most typical form of neurosyphilis presently diagnosed is asymptomatic neurosyphilis. Among the symptomatic problems of neurosyphilis, the earliest to manifest is syphilitic meningitis. Syphilitic meningitis usually occurs inside the first 12 months of an infection and may be accompanied by options of secondary syphilis. Confusion, lethargy, seizures, aphasia, and hemiplegia could additionally be noticed in association with syphilitic meningitis. Focal neurological findings are believed to be the consequence of associated vascular harm. The neurological manifestations include aphasia, hemiparesis, hemianesthesia, diplopia, vertigo, dysarthria, and a variety of brainstem syndromes. Many of the eponymous stroke syndromes of the brainstem described in the nineteenth century In contrast to atherosclerotic cerebrovascular illness, these lesions had been often very discrete due to the involvement of an isolated artery. A giant spectrum of spinal cord problems are seen in affiliation with syphilis (Table 1). The most distinctive and often heralding symptom is lightning-like pains that may be triggered by touch and most often have an result on the legs and stomach. The gait is ataxic with a foot-stomping character due to an related impaired position sense. Lower extremity reflexes are absent, and sexual and sphincter dysfunction are noticed. Syphilitic meningomyelitis is maybe the commonest spinal syndrome currently complicating syphilis. It is characterised by slowly progressive weak point of the decrease extremities accompanied by paresthesia. Spastic paraparesis or paraplegia and impaired sensory perception (disproportionate loss of vibratory and position sense) are found on bodily examination. An acute infarction in the territory of the anterior spinal artery secondary to a syphilitic arteritis results in paraplegia with lack of ache and temperature sensation under the level of the lesion, with preservation of vibratory and place sense. In the preantibiotic period, basic paresis accounted for a considerable Table 1 Syphilis of the spinal twine Syphilitic meningomyelitis Syphilitic spinal pachymeningitis Spinal twine gumma Syphilitic hypertrophic pachymeningitis Spinal vascular syphilis Syphilitic poliomyelitis Tabes dorsalis Miscellaneous Syringomyelia Syphilitic aortic aneurysm Charcot vertebra with compression of the spinal twine proportion of psychiatric sickness. Dementia and psychiatric disturbances, together with emotional lability, paranoia, delusions of grandeur, hallucinations, and inappropriate habits, are the hallmarks of general paresis. Tremors of the tongue and extremities, hyperreflexia, hypomimetic facies, dysarthria, chorioretinitis, optic neuritis, and pupillary abnormalities, including Argyll Robertson pupils, are seen. On cranial magnetic resonance imaging, frontal and temporal atrophy, subcortical gliosis, and elevated ferritin in the basal ganglia have been seen in sufferers with general paresis. Progressive focal neurological manifestations, seizures, and increased intracranial pressure complicate gummas of the mind. Brain computed tomography and cranial magnetic resonance often present a dural-based, enhancing lesion with related mass effect. Gummas affecting the cervical spinal cord lead to progressive quadriparesis, and those within the thoracic space end in progressive paraparesis. Syphilis is more aggressive and may be more difficult to treat in the setting of immunodeficiency. In addition to the Argyll Robertson pupil, other ophthalmological conditions related to T. The latter is usually unilateral and should happen with or with out associated basilar meningitis. Otitic syphilis results in listening to loss (either acute or steadily progressive) and vertigo. Syphilitic damage of the eighth cranial nerve is a late manifestation of congenital syphilis, however it may occur with acquired illness. In patients with neurosyphilis, the diagnosis is mostly dependent on serological research. The treponemal exams include the fluorescent treponemal antibody absorption take a look at, microhemagglutination assay, hemagglutination treponemal test for syphilis, and the treponemal immobilization test. The take a look at is simply too insensitive, nonetheless, to exclude the prognosis of neurosyphilis on the basis of a adverse study. Its frequency of reactivity seems to vary with the clinical form of neurosyphilis, and its presence in asymptomatic neurosyphilis could also be considerably lower than in symptomatic disease. However, a cardinal requirement for the analysis of neurosyphilis is a reactive serum treponemal check. Newer technology exams for syphilis and neurosyphilis, particularly these using the polymerase chain response and monoclonal antibodies, may clear up this dilemma, however additional research is required before widespread software. Although not diagnostic of neurosyphilis, radiological research may be useful in excluding other pathologies. Gummas are avascular, dural-based plenty with surrounding edema that on magnetic resonance imaging are characteristically isointense, with grey matter on T1-weighted pictures and hyperintense on T2-weighted photographs. The penicillin ought to be administered at no less than 4-h intervals to maintain the consistent levels at or above treponemicidal values. The successful use of intravenous ceftriaxone, 2 g day by day for 10 days, and oral doxycycline, 200 mg twice day by day for 21 days, has been reported. An alternative therapeutic course is the administration of a 30-day course of 200 mg doxycycline twice daily following the completion of intravenous remedy. Although secondary prophylaxis is extensively employed, further studies are warranted earlier than secondary prophylaxis or some permutation of it can be broadly beneficial. Unless the disease recrudesces, as may be seen in early latent syphilis and which is the reason for its distinction from late latent syphilis, neither latent nor tertiary syphilis is considered contagious. In these individuals with main, secondary, or latent syphilis, the manifestations of neurosyphilis may be avoided by the timely administration of sufficient doses of penicillin. Monitoring Therapy Determining the adequacy of remedy depends on careful follow-up of the patient. This delay to reversion from a seropositive status displays the duration and severity of the illness. Persistent seropositivity suggests persistent infection, reinfection, or a organic false-positive test. The fixed neurological deficits of neurosyphilis might fail to enhance with treatment, and some abnormalities, corresponding to tabes dorsalis and optic atrophy, could worsen regardless of enough remedy. The cell count should return to regular within 1 yr of remedy (usually 6 months) and the protein concentration within 2 years. Hollander H (1988) Cerebrospinal fluid normalities and abnormalities in people infected with human immunodeficiency virus. The research and apply of neurotology serves the clinical frontiers of neurology and otolaryngology and mainly considerations auditory and vestibular dysfunction.
5 mg bystolic generic with mastercard
Location of Adrenergic Receptors Although adrenergic receptors are found throughout the body in tissues innervated each by the peripheral and central nervous techniques arrhythmia facebook discount 2.5 mg bystolic free shipping, a couple of locations are of particular interest arrhythmia nursing care plan order 2.5 mg bystolic. In the center, b1-receptors predominate, whereas in the clean muscle tissue of the lungs, some blood vessels, and the uterus, b2-receptors are relatively abundant. Effects Mediated by the Central Nervous System In the central nervous system, the cell bodies of noradrenergic neurons are discovered primarily in the locus coeruleus within the brainstem. Although adrenergic receptors are discovered throughout the brain, a2receptors are of specific importance as a outcome of they assist regulate the release of norepinephrine as properly as many other neurotransmitters. The final (postganglionic) nerves in the sympathetic system are adrenergic and thus launch norepinephrine at finish organs. The adrenal medulla, which can also be a part of the sympathetic system, releases epinephrine into the circulation. Activation of the sympathetic system, as happens in response to perceived danger, ends in the release of huge portions of norepinephrine and epinephrine. Drugs that evoke responses just like sympathetic nerve stimulation are referred to as sympathomimetic drugs. They produce their effects either instantly, by stimulating adrenergic receptors (adrenergic receptor agonists), or not directly, by promoting the release of norepinephrine or by blocking its reuptake. Table 1 provides examples of various sympathomimetic medicine, with their mechanisms of action, the consequences they produce, and common therapeutic indications. Table 2 provides examples of adrenergic receptor antagonists, with their receptor selectivity, the results they produce, and customary therapeutic indications. Grassi G (2009) Assessment of sympathetic cardiovascular drive in human hypertension: Achievements and perspectives. Hokfelt T, Johansson O, and Goldstein M (1984) Central catecholamine neurons as revealed by immunohistochemistry with particular reference to adrenaline neurons. Ilias I and Pacak K (2005) Diagnosis and administration of tumors of the adrenal medulla. When each the eyes and the visible scene are shifting, it also maintains the percept of a stable world, stopping oscillopsia (the false notion of motion). Saccades are quick eye actions that redirect the eyes from one target to another. Oscillation could end result when one or more of those subsystems turn into unstable as a outcome of congenital, developmental, or acquired circumstances. Alternatively, when the saccadic system is flawed or unstable, saccadic intrusions and oscillations end result. The presence of either nystagmus or saccadic instability could indicate neurological abnormalities or may replicate nonsymptomatic congenital circumstances. The differential analysis of those possibilities requires accurate identification and characterization of the actual instability present. Eye-movement recording can differentiate nystagmus types, as properly as saccadic intrusions and oscillations. When continuous runs of saccadic intrusions happen, they turn into saccadic oscillations. Infantile Nystagmus Several kinds of nystagmus may appear at delivery or during infancy. Fortunately, they can be identified by their distinctive waveforms, characteristics, or interocular section relationships. Unfortunately, a person could have a couple of sort of infantile nystagmus, producing complex waveforms. This interaction facilitates target acquisition and maintained foveation, permitting good visible acuity despite the ocular oscillation. These traits may be exploited therapeutically either optically, via using prisms, or surgically. Afferent stimulation of the ophthalmic division of the trigeminal Definitions Nystagmus could be divided into two broad categories, pendular and jerk. Pendular nystagmus is a sinusoidal oscillation with no distinguished saccadic quick phases. Jerk nystagmus consists of an preliminary sluggish phase followed by a corrective saccadic fast part. In addition, the relative amplitudes and phases of the nystagmus within the two eyes or the circumstances that elicit nystagmus assist differentiate them. Saccadic intrusions are initiated by a Encyclopedia of the Neurological Sciences, Volume 3 doi:10. This is at present being accomplished by tenotomy of the four horizontal recti tendons and reattachment at their authentic factors of insertion on the globe. It is a jerk nystagmus (of both eyes) that beats in the direction of the fixating eye, whatever the gaze angle and whether one eye is occluded or each are viewing (only one shall be fixating because of the strabismus). The quick phases take the eye previous the goal and the sluggish phases then decelerate the attention toward the target, allowing the fixation subsystem to preserve goal foveation on the low-velocity ends of the slow phases. Finally, infants sometimes have mixtures of uniocular, grossly disconjugate, and variable-phase-difference pendular nystagmus. However, the same kind of nystagmus could also be indicative of a mind tumor and imaging is usually required. It is absent within the primary position and is current solely as the gaze is directed laterally, it has fast phases that beat within the direction of the gaze, and its amplitude grows with gaze eccentricity. Eccentric position signals leak exponentially toward zero (primary position), causing the eyes to comply with the same course. Acquired pendular nystagmus can also be widespread and is usually is accompanied by oscillopsia. It may be current in multiple aircraft, with one predominating, or may be dissociated in the two eyes. In excessive cases, the actions could additionally be completely disconjugate, resulting in a pendular vergence nystagmus. It is thought to end result from impaired visible connections to the cerebellum, resulting in instability in reciprocal connections from the brainstem. It could symbolize a dynamic dysfunction related to the static disorder of dissociated vertical deviation. A mannequin simulation demonstrated that loss of retinal information and transient reconstructed error produced staircase saccadic intrusions. Square-wave oscillations have been reported in progressive supranuclear palsy and bought immunodeficiency illness. Saccadic dysmetria is a postsaccadic, damped saccadic oscillation (hypermetria) or collection of less-than-adequate saccades (hypometria). Hypermetria results from an increased gain (greater than 1 however less than 2) in the saccadic subsystem inflicting every saccade to overshoot by a onerous and fast proportion of the desired amplitude till the required corrective saccade falls inside a useless zone.
Bystolic 5 mg discount
If the reasoner recognizes parallels between a novel downside and a familiar solved one blood pressure medication making blood pressure too low buy bystolic 5 mg otc, then the earlier solution could also be tailored to fit the new problem arrhythmia management plano bystolic 5 mg with mastercard, eliminating the necessity for intensive search in the issue space. Numerous studies utilizing each neuropsychological and neuroimaging strategies have now confirmed that prefrontal cortex is critical in analogy for each the comparison process. If neither direct prior knowledge nor an analogy is available, heuristic search methods could also be used. The apparent difference between the current state and the objective state is that the automotive is unwashed. Second, an preliminary aim can lead to subsequent subgoals that successfully decompose the issue into smaller elements. Shallice conducted a research that particularly examined the way during which frontal lobe patients approach novel issues requiring planning and arranged sequential action. He tested sufferers with varied types of mind injury, in addition to management subjects, on their ability to solve varied variations of the Tower of London puzzle. This puzzle consists of three differently colored disks and three pegs of different lengths. The experimenter places the disks in a beginning configuration, and the topic must then transfer them into a new configuration outlined by the experimenter in a minimum variety of moves. Recent evidence suggests that the previously mentioned findings ought to be interpreted cautiously. The same research discovered that several posterior regions of the mind, especially these related to the era of visible images, additionally play vital roles in chess taking half in. Using functional magnetic resonance imaging, Koechlin and colleagues employed a task that might be modified to manipulate working reminiscence load in addition to aim use. However, when individuals have been required to maintain a main aim whereas concurrently utilizing subgoals, frontopolar prefrontal cortex was additionally recruited. Numerous neuroimaging studies have now implicated frontopolar cortex as being necessary for relational integration. Evidence additionally 980 Problem Solving seems to suggest that extra relationally complex a problem, larger the involvement of extra anterior areas of prefrontal cortex. Thus, frontopolar prefrontal cortex ought to turn into progressively extra important because the variety of subgoals will increase. Although laboratory research often give attention to problems that are novel for the participant, skilled real-world problem fixing frequently includes evoking a related drawback schema and utilizing specialized problem-solving strategies. There is increasing proof that the development of problemsolving talent includes other brain areas in addition to prefrontal cortex. This finding suggests that the basal ganglia (or at least the frontostriatal circuit) are necessary for the event of problem-solving expertise. Recently, researchers have begun to move beyond merely contemplating how separate areas of the brain are involved in drawback solving to develop an understanding of how brain networks allow problem fixing. New analysis strategies for neuroimaging data in cooperation with efforts to build neutrally plausible computational models of downside fixing to assist analyze these information, will hopefully yield a much clearer picture of how the mind solves problems in the future. Acknowledgments Preparation of this entry was supported by a grant from the American Federation of Aging Research and the Illinois Department of Public Health. Koechlin E, Basso G, Pietrini P, Panzer S, and Grafman J (1999) the position of the anterior prefrontal cortex in human cognition. The future anatomist, physiologist, embryologist, and ophthalmologist studied philosophy in Olomouc from 1765 to 1767. He studied medication in Vienna from 1770 to 1776, working first with Austrian physician Anton de Haen from 1774 to 1776, who recognized his ability in anatomical drawing. Prochaska turned a professor of anatomy and ophthalmology at the University of Prague in 1778 however left in 1791 for Vienna, the place he remained till 1819 as professor of anatomy and ophthalmology. Prochaska proposed that a latent nervous force, the vis nervosa, coordinates all impressions passing alongside nerves to the person nerve centers. The different kind of nerve fiber conducts mirrored impulses from the sensorium commune to the muscle tissue and other effector organs. In doing so, he has been thought-about to have advanced a primordial idea of localization of perform inside the mind. Kneipa within the gallery of the Dean and Professors of the Medical Faculty of Prague). Primary infections could happen through oropharyngeal or respiratory routes, or alternatively from contaminated meals or drinks. The virus is then thought of to be latent or persistent in kidney or lymphoid organs such as the spleen, tonsils, and bone marrow. The virus may flow into through blood vessels in affiliation with peripheral lymphocytes. In individuals with immunosuppression, the circulating virus may enter the mind and induce the demyelinating disease. The viruses seem as icosahedral structures roughly forty nm in diameter or as filamentous varieties. The viruses form clusters preferentially situated on the inner periphery of the nucleus (as surrounded by arrows). The genome shows a tripartite group with early and late coding areas and a regulatory area. Rheumatic diseases had been additionally present, and systemic lupus erythematosus was some of the common underlying illnesses. Recently, virus reactivation associated with immune modulatory medicine has also been a problem. In some cases, nonetheless, pathological examination of biopsied mind tissues or post-mortem can also be required for a final analysis. This may be partly due to the expanded medical spectrum of underlying diseases and prolonged clinical time course. Computed tomography of the brain reveals hypodense lesions of the affected white matter with out mass effect. Contrast enhancement is rare and, if observed, is often faint and located within the periphery of the lesions. Although a number of white matter lesions are characteristic, isolated lesions may be noticed. Cranial magnetic resonance imaging also shows hyperintense lesions on T2-weighted imaging within the affected areas. Frontal lobes and parieto-occipital areas are most commonly affected, although involvement of the cerebellum or brainstem and the spinal cord can also be seen. Isolated or related involvement of the basal ganglia could also be noted as nicely, and such a divergent distribution of the demyelinating lesions may trigger diagnostic confusion. In contrast, these of the neurotropic sorts are markedly divergent and likely are derived from the archetypal sequence on account of deletion and duplications.
Cheap bystolic 5 mg amex
Causes embrace anterior spinal artery thrombosis blood pressure medication harmful bystolic 5 mg cheap free shipping, vasculitis arrhythmia high blood pressure cheap 2.5 mg bystolic with mastercard, dissecting aortic aneurysm, embolism, systemic hypotension, and aortic surgical procedure. Because the anterior spinal artery additionally provides the ascending spinothalamic tracts, patients have a lack of pain and temperature sensation beneath the extent of the lesion. Vibration and proprioception sensation, nevertheless, are preserved as a result of the posterior columns are provided by the posterior spinal arteries. Initial symptoms are painless and progressive weak spot, corresponding to a foot drop or arm weak point. The symptomatic weak limbs usually exhibit a mix of each higher and lower motor neuron findings, together with brisk reflexes and atrophy with fasciculations. A number of medical trials looking for simpler therapies are underneath way. Spinal Cord Diseases with Prominent Lower Motor Neuron Findings Poliomyelitis Poliomyelitis, as quickly as the leading cause of an acute flaccid paralysis, presents as uneven weak point, atrophy, extreme cramps, and fasciculations due to the lack of anterior horn cells, that are preferentially affected by the virus. The leukodystrophies and different metabolic problems have an effect on the spinal twine and could also be accompanied by a peripheral neuropathy as well as cognitive impairment. Patients with borderline values ought to bear evaluation of the extra delicate methylmalonic acid and homocysteine ranges, which are elevated in most sufferers with a true deficiency. Other notable metabolic issues related to myelopathy are copper, folate, and vitamin E deficiencies as nicely as publicity to nitrous oxide and zinc overdose. Tabes Dorsalis and Infectious Myelopathy the late results of neurosyphilis can involve the posterior columns, resulting in a extreme gait abnormality due to loss of proprioceptive info (sensory ataxia). The dorsal nerve roots are also concerned, resulting in extreme radicular-type ache. The examination reveals a profound lack of vibration and proprioception and a slapping gait. Infectious myelopathy can also be because of tuberculosis, fungal agents, and parasites corresponding to Schistosoma in endemic areas. Spinal Cord Diseases with More Prominent Sensory Findings Syringomyelia and Central Spinal Cord Syndromes Central cavitation of the cervical spinal cord usually presents with lack of pain and temperature sensation in both arms and shoulders as a outcome of involvement of the spinothalamic tracts as they cross in the central spinal twine. If the cavitation extends into the medulla, bulbar signs of dysarthria and dysphagia also can develop (syringobulbia). This can have a similar look to a spinal cord tumor that develops in the heart of the cord, corresponding to an astrocytoma or ependymoma. Posterior Spinal Artery Occlusion Occlusion of the posterior spinal artery leads to a sudden loss of vibration and proprioception sensation beneath the extent of the lesion. Patients have problem strolling as a end result of a severe loss of proprioception and sometimes stroll with a slapping or stomping gait to decide the position of the legs in area. The disorder is extraordinarily rare as a end result of the posterior spinal arteries receive a number of feeders, and some authorities doubt that it ever occurs. Conclusion Damage to the spinal wire and its pathways could additionally be devastating and cause considerable disability. Recent major breakthroughs in understanding the pathophysiology underlying many syndromes have led to improved diagnosis and highly efficient and disease-specific remedies. Management of the affected person with spinal wire pathology requires a multidisciplinary method and intensive rehabilitation. Vitamin B12 Deficiency Vitamin B12 deficiency can lead to a subacute mixed degeneration, which means degeneration within the spinal twine (pyramidal tracts and posterior columns) and in the peripheral nerves. Patients incessantly present with a gait abnormality because of severe lack of proprioceptive sensation. Evidence of posterior column dysfunction (vibration and proprioception loss) is current and is typically the most distinguished abnormality found on examination. Other neurological (optic neuropathy, cognitive adjustments, and dysgeusia) and nonneurological manifestations (glossitis, vitiligo, prematurely grey hair, anorexia, and megaloblastic anemia) can also be present. Upper Motor Neuron Lesions Further Reading American Academy of Neurology (2011) Spinal twine, Root, and plexus issues. Depending on the diploma of injury to the spinal cord, sufferers could have permanent deficits or might get well fully. Although any spinal stage may be involved, the cervical spine is most frequently affected adopted by the thoracic and lumbosacral spine, in that order. The purpose is unknown, however it may be related to the relative hypermobility of the backbone in children and to their immature bones, which permit extra laxity during direct trauma and make fractures less prone to occur in contrast with more occurrences in mature people. To stop secondary damage to the spinal wire because of ischemia in response to the loss of autoregulation, hypertensive remedy administered within the first few days after damage appears to improve total neurological outcomes in patients with acute spinal twine injury. The most important factors in improving outcomes appear to be early analysis and immobilization. Results of the third National Acute Spinal Cord Injury randomized controlled trial. Introduction Spinal cord transection is a devastating situation, leading to permanent disability. Spinal cord transection affects largely active younger people and is associated with substantial monetary costs for acute remedy and lifelong supportive therapy. Spinal wire transection is a complete interruption of white matter tracts, segmental gray matter, and associated nerve roots within the spinal wire at any level between the cervicomedullary junction and tip of the conus medullaris. Symptoms of spinal cord transection mirror the level at which the spinal wire is affected. Similar clinical outcomes are related to spinal hemorrhage, infarction, tumors, infections, a quantity of sclerosis, or idiopathic myelitis. The pathophysiology of spinal wire transection consists of several timed and well-characterized phases. The primary part, which is attributable to the mechanical drive to the spinal wire, affects cellular constructions and microvasculature. Secondary harm ultimately leads to the lack of adjoining spinal twine tissue, often with the formation of cavities via the stumps. The secondary response is split into several phases that reflect key pathophysiological mechanisms. Hemorrhage, edema, ischemia, neural tissue disruption, and loss of spinal wire perform under the harm characterize the quick phase. Disruption of communication between the brainstem and autonomic nervous system is liable for medical presentation. Furthermore, microvascular disturbances result in ischemia and cell dying in spinal wire tissue distant from the precise site of injury. Besides native microvascular modifications, pulmonary and cardiac components contribute to ischemia. During the instant part, histological changes in distant areas of the spinal cord are often not apparent. Astrocytes, T cells, microglia, neutrophils, and monocytes are liable for inflammation. During the intermediate part (14 days to 6 months after injury), the lesion stabilizes and scar tissue and cysts continue to type.