
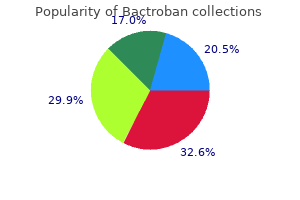
Bactroban dosages: 5 gm
Bactroban packs: 1 creams, 2 creams, 3 creams, 4 creams, 5 creams, 6 creams, 7 creams, 8 creams, 9 creams, 10 creams

Generic bactroban 5 gm fast delivery
This promotes identification of potential accidents and avoids the pitfalls of a missed harm acne keloid order bactroban 5 gm on-line, which might happen acne zeno buy bactroban 5 gm with mastercard. Cardiac and other antihypertensive medication might alter a pulse rate or have an impact on blood stress, making clinical examination tough. It is even more important than with penetrating trauma patients where decision making is commonly simpler. While there are limitations of the abdominal examination in each the conscious and unconscious patient, it offers invaluable info in the early management permitting diagnosis and prioritization. Apart from altered stage of consciousness, the variable impact of hemoperitoneum and the number of potential harm patterns with variable signs from hollow or strong viscus injury make interpretation difficult. The presence of distracting accidents in the multi-injured patient could pose a further problem. Strong suspicion of intra-abdominal harm should be considered within the following sufferers: - presence of abdominal tenderness and rebound - inflexible stomach - patients with seatbelt marking 26 � In patients with seat belt marks. The significance of seat belt marking as a predictor of intra-abdominal injury varies from series to collection. Velmahos1 has identified in motor vehicle victims that a seat belt mark is associated with an eight fold enhance in intra-abdominal trauma compared to sufferers with out seat belt mark, finding that 23% of sufferers suffered important intraabdominal organ harm notably mesenteric laceration, hepatic, duodenal and jejunal laceration. Macroscopic hematuria always needs investigation, normally indicating a major renal or bladder rupture. Tips and Pitfalls � Thirty percent of main renal injuries could exist with a normal urinalysis. Experience and amenities of the trauma middle Evaluation of Blunt Abdominal Trauma 285 26. It has the drawback nevertheless of not predicting the need for laparotomy per se and can enhance nontherapeutic laparotomy price. It is typically recommended that the white cell depend to red cell count ratio of 150 or greater, signifies a gastrointestinal tract perforation requiring surgery. Remember that 25-30 ml of blood in a patient with a standard hemoglobin will end in a red cell count of 100,000/mm3. In pelvic fractures, care must be exerted as false constructive rates of as much as 30% have been reported. It is particularly necessary to keep away from a nontherapeutic laparotomy in sufferers with pelvic trauma. Tips � Use an open method by way of umbilical wire or linea alba (at the umbilicus), just like the method for open insertion of the laparoscopic insertions of umbilical posts. This is particularly necessary in relation to identifying areas of hypoperfusion, figuring out vascular injuries and blushes. Combination of organ injury grading and blood loss estimation will enhance the prediction of requirement for surgery. Oral distinction nevertheless, does provide a nicer street map for the radiologist nonetheless, it might not enhance the detection of gastrointestinal tract perforation. Timing of Investigations 26 Prompt analysis of blunt belly trauma will improve not just the management plan however affected person outcome. Tips: � If a quantity of investigations are to be carried out, an optimum sequence ought to be thought out. Unstable Patients � � the evaluation of the unstable patient with blunt stomach trauma is a challenge requiring rapid decision making. Discussion about their college trainer, canine, favorite program on tv, or present pursuits like Pokemon playing cards, is a guaranteed means of insuring gentle evaluation. Care should be taken in ensuring the operator is credentialled and sonography of the infant must be undertaken by an obstetrician, or a suitably certified radiologist. The pelvic plain films will usually present an insight as to the potential for hemorrhage. Associated injuries are widespread and 10% of sufferers have bladder accidents, 10% spleen, 7% liver, 7% small bowel, 7% renal and other injuries in 10%. Audit and evaluation of your nontherapeutic laparotomy rate, missed damage rate and complications is important to guarantee improvement and maintenance of high requirements. Velmahos Historical Perspectives � Penetrating belly trauma was managed expectantly until the late 19th century. Anatomical Definitions � Injuries to the anterior (true abdomen) or posterior (back) stomach can cause intra-abdominal organ accidents. The Objective and the Dilemma � the objective of analysis of penetrating stomach trauma is to identify sufferers in need of operation whereas at the similar time minimizing the risks associated with pointless procedures. It is with this objective and dilemma in mind that all the following methods might be reviewed. Clinical Evaluation � Every patient with a stab wound or gunshot wound to the abdomen ought to have a detailed medical analysis together with a rectal examination. Alternative interventional strategies to handle a gunshot wound to the abdomen exist. This patient was not operated on but had hepatic angiography with embolization of a bleeding branch of the best hepatic artery. This patient had two transpelvic gunshot wounds, no abdominal tenderness or hemodynamic instability and blood at the urethral meatus. A retrograde urethrogram confirmed contrast extravasation from the membranous portion of the urethra. Additional Diagnostic Tests � A variety of checks have been used to consider the stomach after penetrating injuries, together with diagnostic peritoneal lavage, ultrasound, contrast-injection Evaluation of Penetrating Abdominal Trauma 297. Upon exploration, the entry and exit sites to the peritoneal cavity were near each other and there was no underlying organ harm. Values of a hundred,000, 50,000, 25,000, 10,000, and 1,000 have been used with various sensitivities ranging from 99-75%. We consider that with increasing expertise, ultrasonography will turn out to be an essential software within the analysis of intra-abdominal trauma. This patient suffered a stab wound and was explored as a result of there were in depth fascial defects. Evaluation of Penetrating Abdominal Trauma 299 � the stabbogram consists of injection of distinction into the harm tract to detect attainable leakage of distinction into the belly cavity. It detects or guidelines out these accidents and divulges the presence of a functional contralateral renal unit, which is necessary when surgery for removing of the injured renal unit is a risk. The take a look at is performed by injecting intravenous contrast and taking a plain abdominal radiograph 15 to 20 minutes after injection. The check is related to a excessive price of false-positive and false-negative outcomes. Intraoperative palpation can reveal the presence of a normal-size contralateral kidney if this is deemed essential.

Buy bactroban 5 gm on-line
It extends cephalad to the umbilicus to enclose the urachus and the umbilical arteries and caudally to cover the bladder acne popping 5 gm bactroban with amex, seminal vesicles acne and birth control bactroban 5 gm buy generic online, and the prostate. Lateral condensations type the lateral true ligaments of the bladder and the puboprostatic ligaments. Sinoutricular Cord, Verumontanum, and Formation of the Prostatic Utricle As the information of the fused and canalized m�llerian (paramesonephric) ducts meet the urogenital sinus, they stimulate the sinus epithelium to form a protuberance into the sinus, the m�llerian tubercle or verumontanum. A second protuberance develops within the direction of the duct on the surface of the urogenital sinus. This projection is joined to the fused m�llerian ducts to kind the sinoutricular wire. In the male, the distal portion becomes canalized to kind the prostatic utricle or vagina masculina. A dashed line across every frontal view indicates the original degree where the wolffian duct made contact with the vesicourethral canal, defining the junction of the canal with the urogenital sinus. The widespread excretory ducts and the long run ostium of the fused m�llerian ducts enter the vesicourethral canal on the verumontanum (m�llerian tubercle). The ureteral buds department from the wolffian duct proximal to the frequent excretory duct, which is steady with the cloacal horn that was derived from the tissue of the canal. With the incorporation of the cloacal horn and the widespread excretory duct into the vesicourethral canal, the wolffian duct and the ureter enter aspect by side. The terminal portion of the m�llerian duct, now the prostatic utricle, opens between them. The progress of mesodermal wolffian tissue (crosshatched area) between the orifices of the ureter and the ejaculatory duct, combined with growth of the bladder wall, ends in the ascent and lateral displacement of the ureteral opening. In contrast, the opening of the wolffian duct is fastened in position at the verumontanum, not solely from its close embryologic affiliation with the m�llerian duct but in addition as a result of the complete lower portion of the urogenital sinus is mounted in stable mesodermal condensations so that enlargement can occur solely in a cephalic course. The terminations of the wolffian ducts do, in fact, move a small distance cephalad, leaving a symmetric pair of longitudinally disposed remnants as collicular the mesodermal widespread excretory duct is outlined as that portion of the wolffian duct distal to the ureteral bud. The tissue of the endodermal vesicourethral canal expands posteriorly toward the widespread excretory duct to type, together with the terminal piece of the common excretory duct, a funnel-shaped extrusion, the cloacal horn. As the cloacal horn becomes reincorporated into the canal, it carries the terminal piece of the frequent excretory duct into the vesicourethral canal with the ureter attached and forms part of the superficial trigone. The formation of the superficial trigone begins with the fusion of the mesoderm medial to the two ducts. Although the orifice of the wolffian duct remains in place, the mesoderm that was originally a half of the common excretory duct turns into energetic and enlarges. This mesodermal development displaces the ureteral orifices cranially and laterally, shifting them from close to the midline at the junction of the vesicourethral canal with the urogenital sinus right into a lateral place within the bladder. The entire superficial trigone, a structure that extends from the verumontanum to the ureteral orifices, is formed by this mesodermal (wolffian) progress. The dashed line exhibits the extent at which the wolffian duct initially made contact with the vesicourethral canal. The size of the collicular folds is an indication of the distance that the ducts and verumontanum have moved cephalad. In the mature stage, the tissue from the wolffian duct varieties the superficial trigone. Distally, in the preprostatic urethra, the verumontanum is found holding the ejaculatory ducts and prostatic utricle. Thus developmentally the muscular tissues of the superficial trigone are continuous with these of the ureter, all being of wolffian origin. Ductal Incorporation in Male and Female Male the ductal mesoderm (cross-hatched area) that was included into the vesicourethral canal moves cranially and laterally and carries the ureteral orifices with it. As described previously, this tissue turns into distributed as the superficial trigone within the area between the ejaculatory ducts distally and the ureteral orifices proximally. The fused m�llerian ducts enter the canal at the verumontanum, which lies at the junction of the vesicourethral canal and the urogenital sinus. The ureters penetrate the bladder wall by a straight course; later improvement supplies an oblique tunnel. Instead of resulting in a prostatic utricle, canalization of the sinoutricular wire in the feminine varieties the terminal portion of the vagina. The whole feminine urethra develops from the urogenital sinus because the homologue of the posterior urethra of the male. The equal of the verumontanum containing the m�llerian prostatic utricle could be considered as lying at the introitus. Remnants of the wolffian ducts turn into the epo�phoron and paro�phoron, and are additionally represented within the grownup because the Gartner ducts that extend the size of the vagina. An inadequate response of the renal blastema to the stimulus arising from the branching ureteral bud may also lead to a discount of renal tissue. They may be related to obstruction however can happen in inheritable syndromes in the absence of obstruction. Or the bud may develop in a comparatively irregular place so that it attempts induction of a poor area of the renal blastema. Evidence for that is that dysplasia is usually discovered related to a displaced secondary ureteral bud that empties laterally or distally into the urethra. Anomalies on the Ureteric Hiatus Paraureteral diverticula (saccules) arise at the upper extremity of the trigone simply above the ureteric orifice as a transhiatal herniation of the bladder mucosa. Deficient development of the hiatus and of the muscle of the superficial trigone is the possible trigger in infants. Many are probably secondary to a weak internal longitudinal layer of the bladder musculature on the ureterovesical angle and to poor help from the outer longitudinal layer. With obstruction or neurogenic bladder, elevated detrusor stress could trigger transhiatal herniation of the vesical mucosa to form the so-called saccule of mucosa compelled via an overstretched hiatus. Hiatal diverticula disturb the submucosal course of the terminal ureter and, subsequently, are associated with reflux. They may be duplications consequent on the formation of a second bud on the wolffian duct or they could be ureteral ectopia from late arrival or vesicoureteral reflux from early arrival of the ureter at the vesicourethral canal. Even if the ureteral bud forms at the correct place and time, it could be unduly large and result in formation of a dilated upper tract corresponding to is seen in the nonrefluxing nonobstructed megaureter. One clarification is delayed rupture of the occluding epithelial membrane normally lying at the junction of the ureter and the urogenital sinus within the sixth week of gestation, when nephrogenic operate is in abeyance; persistence of the membrane leads to obstruction at that web site. Another explanation is delay in the absorption of the immature ureter into the vesicourethral canal. A third principle is that arrest in muscular development of a ureter located too far caudally ends in distention of the terminal portion. A easy ureterocele, during which the cystic formation happens at the site of the normal orifice, is uncommon in children and may actually be acquired somewhat than congenital. A distinction is made between an intravesical ureterocele, in which the orifice is within the bladder, and an ectopic ureterocele extending distal to the bladder neck, though its orifice could lie within the bladder.
Diseases
- Familial porencephaly
- Vitamn B6 deficiency
- Anorchidism
- Osteogenesis imperfecta retinopathy
- Craniofacial dysynostosis
- Optic atrophy polyneuropathy deafness
- Toni Debre Fanconi maladie
- Hyperprolactinemia
Bactroban 5 gm purchase line
In this mechanism acne extractions bactroban 5 gm buy discount online, a lateral directed drive is applied on the iliac wing acne near mouth 5 gm bactroban with mastercard, such as would occur when a car from the facet strikes a pedestrian. If the magnitude of the forces is high, a pivoting happens across the sacral body and thus causes the posterior sacroiliac ligament to be positioned underneath tension and thus failing or a fracture through the iliac wing can happen. Essentially, on this mechanism, there are either accidents to the posterior sacroiliac ligaments or fractures of the iliac wings and pubic rami that lead to complete vertical instability. Indications of a pelvic injury could embody leg length inequality, scrotal hematoma or swelling, or hematomas around the iliac wings or lower again. If suspected, palpation of the iliac wings will present useful details about the gross stability of the pelvic ring. More subtle instability can be assessed afterward with specific radiographic views and stress views. These lesions are closed degloving accidents where the subcutaneous tissue is torn or sheered away from the underlying fascia forming a cavity crammed with hematoma and liquefied fats. Open drainage and debridement, adopted by dressing modifications and packing finest handle these lesions. Despite the widening, the posterior sacroiliac ligaments were intact in this case. It is very common for these patients to also maintain accidents to abdomen, chest and head. If a diagnostic peritoneal lavage is contemplated, it ought to be carried out utilizing a supraumbilical method to stop a possible entry into the retroperitoneal space by way of the reflection of the peritoneum that follows the spherical ligament below the umbilicus. Signs of genitourinary damage embrace hematuria, blood on the meatus, and a high using prostate in a man. The presence of blood at the meatus or a high riding prostate in a man is extremely indicative of a urethral damage and is a sign for a retrograde urethrogram prior to Foley insertion in a hemodynamically secure patient. In a hemodynamically unstable affected person, a single try to place a catheter is made by a qualified urologic specialist. Bladder injuries in each men and women correlate with the number of pubic rami fractures. Pelvic Fractures and the General Surgeon 453 � Injuries to the pelvic ring frequently are associated with injuries to the peripheral nerves. The L5 root enters the pelvis beneath the L5 transverse course of and crosses the sacral ala approximately 2 cm medial to the sacroiliac joint and joins the sacral plexus. Frequently sufferers with pelvic fractures requires early intubation and as such, require early examination and documentation of their neurologic status so as to to not lose this baseline information. Examination ought to embrace sensation and motor testing to the lower extremity in addition to perianal sensation. Examination of this film ought to allow an excellent estimation of the mechanism of injury, determine fractures and allow inferences of ligamentous injury. Control of such bleeding can be achieved by avoiding coagulopathy and providing tamponade. Coagulopathy can be secondary to the dilutional effects of resuscitation fluids and blood merchandise in addition to hypothermia. In a affected person with an intact pelvis, the potential retroperitoneal area can maintain a volume of roughly 2 liters. In the appearance of a pelvic harm in which the pubic symphysis is widened by 2 cm greater than regular, the potential retroperitoneal area has been estimated to improve to 6 liters. It stands to reason then that controlling the displacement of the pelvic ring can facilitate tamponade. In the absence of lower extremity damage, internally rotating each limbs may also serve to lower pelvic displacement. It will also enable a affected person to be transported from division to division without concern of further displacement. External fixation has been proven to decrease the mortality rate in unstable pelvic injuries and has decreased transfusion requirements. Multiply injured affected person with a fracture of the left acetabulum and a subtrochanteric femoral shaft fracture. The conventional frame is an anterior frame utilizing Schantz pins inserted between the internal and outer tables of the anterior iliac wings and attached to a trapezoidal body. This body has the advantage of being simple to apply and has a low complication fee. In sufferers with a big posterior lesion, it tends to offer less inflexible management of the posterior lesion. This was extra of a difficulty when external fixation was the one known means of definitively treating these lesions to union. This frame can be utilized anteriorly to management an anterior lesion or may be applied posteriorly to shut a posterior lesion. Some authors have instructed that these frames be applied beneath radiographic control, and thus may be much less useful in the emergency department. Ideally, a means of elimination can determine these patients, the place different sources of bleeding have been dominated out. Interestingly, in a latest sequence of hemodynamically unstable patients with unstabilized pelvic injures in which Pelvic Fractures and the General Surgeon 455 thoracic and abdominal sources of bleeding had been ruled out, only 30% had angiographically treatable lesions, thus supporting the assumption that hemodynamical instability is a results of venous bleeding. A concern concerning angiography has been raised in sufferers with acetabular fractures that will require an extended illiofemoral approach for open reduction. If the inner iliac artery or superior gluteal artery is embolized, and a adequate time period has not occurred to permit for revascularization, the viability of the flap may be jeopardized. In this group of patients, embolization ought to only be undertaken when a treatable lesion has been identified. An ideal alternative occurs when a patient has a widened pubic symphysis or a parasymphyseal fracture and undergoes exploratory laporotomy for an belly injury. At the completion of the laparotomy, the midline incision is prolonged to the pubis and plate fixation of the symphysis is undertaken. Performing this fixation imparts vital stability to the pelvic ring, permits instant removal of the exterior fixator, and simplifies later supplemental posterior fixation. Once the affected person is secure to undergo additional diagnostic studies, pelvic inlet and outlet views are obtained. These additional views permit the classification of the acetabular fracture and thus allowing one to arrive at a surgical tactic for joint reconstruction. Judet views are primarily 45� internal and exterior rotation views of the acetabulum and are taken with the pelvis rotated along its longitudinal axis and centering the x-ray beam on the acetabulum. Evaluation of those films is past the scope of this review and the reader is referred to traditional works for further information. Stability is defined as the flexibility of the pelvis to resist regular physiologic forces. Stability could also be inferred primarily based on the fracture pattern, bodily examination and serial radiographs. Fractures of the acetabulum are evaluated based mostly on the steadiness of the hip joint, the presence of intra-articular fragments and joint congruity.
Order 5 gm bactroban with mastercard
The starting dose of everolimus is 5 mg daily and of itacitinib is 300 mg every day with treatment planned for two years or till progression/intolerance acne treatment for men cheap bactroban 5 gm visa. This quantified the significantly raised dangers of breast cancer skin care nz bactroban 5 gm purchase online, notably those treated with high dose radiotherapy to the breast round menarche. It is hoped de-intensification of therapies will attenuate danger of these long-term effects but this has not yet been definitively demonstrated. Once complete, this would be the much the largest cohort of its type worldwide, to enable excessive power analyses of threat elements for a variety of great late effects in Hodgkin Lymphoma. Basophil Neutrophil Eosinophil Lymphocyte Monocyte Leukocytes There are 5 different varieties of leukocytes: 1. Monocyte Neutrophil Eosinophil Basophil Lymphocyte Three of those could be additional divided into granulocytes (Neutrophil, Eosinophil and Basophil) as a result of they include visible granules throughout the cell. White blood cell types Eosinophil (left) and Basophil (right): combat parasitic infections and allergic reactions Lymphocyte: acknowledge antigens, produce antibodies, and destroy contaminated cells Thrombocytes Thrombocytes, or extra generally generally identified as platelets, are small blood cells that shed off of a bigger cell referred to as a "Megakaryocyte". The time period used to describe the creation of thrombocytes is identified as "Platelet shedding". Red Blood Cell Diseases Sickle Cell Disease Anemia Red blood cell in the "sickle" shape due to a genetic mutation. Decrease in the variety of red blood cells as a end result of an underlying trigger or deficiency. A lower or lack of platelets in the blood that might be brought on by an autoimmune disease. Leishmania and Dirofilaria coinfection in canine in Greece Dirofilaria immitis and Angiostrongylus vasorum in dogs from southern Portugal. The northward unfold of leishmaniasis in Italy: proof from retrospective and ongoing research on the canine reservoir and phlebotomine vectors. Rapid identification of causative species in patients with Old World leishmaniasis. Human dirofilariasis as a outcome of Dirofilaria (Nochtiella) repens: an replace of world literature from 1995 to 2000. Clinical and laboratory observations in 91 dogs infected with Dirofilaria immitis in northern Greece. Canine heartworm disease (dirofilariosis): pathogenesis and prognosis of a multidimensional illness. Bradford: If definitive radiation or chemoradiation resulted in an entire locoregional response and 6 months later a major web site recurrence occurred, I would carry out the initially planned surgical resection and reconstruction (see #4 above). Clearly, in this instance free tissue switch is really helpful due to the poor wound healing anticipated 6 months after radiation and/or chemoradiation. Futran: At this juncture, surgical extirpation is the only potential healing modality left. The defect would be reconstructed with an osteofasciocutaneous sensate radial forearm free flap. The delicate tissue attributes of the radial forearm flap make it a perfect choice for this defect. Since this affected person is a excessive danger for additional recurrence, once the wounds have sufficiently healed, consideration would be made for using weekly methotrexate remedy for 4�6 months. All of the consultants agree that chemoradiation treatment regimens ought to be performed in a protocol setting. Factors which may be felt to predict radiation responsiveness are tumors restricted to the tonsillar fossa, superficial or exophytic tumors, and poorly differentiated or lymphoepithelioma histology. Anterior pillar lesions with retromolar trigone extension, important tongue base extension, or trismus are preferably treated surgically (Dr. The authors range considerably of their remedy method for this explicit patient. He emphasizes the necessity for close monitoring for an objective response after two cycles of chemotherapy or 50 Gy of radiation with instant salvage for insufficient responses. His rationale for this approach is that the most effective practical consequence is achieved with out compromising oncologic management. Bradford favors surgical resection followed by radiation therapy and probably adjuvant chemotherapy based mostly on histopathologic parameters. She feels that combined modality remedy to both the primary website and necks provides superior locoregional management compared with definitive radiation therapy, provides objective histopathologic standards for entry into adjuvant remedy protocols, and that sophisticated reconstruction of the defects have decreased the surgical morbidity. Futran favors external beam radiation therapy with commonplace fractionation, along with a planned modified radical neck dissection. He feels that radiation therapy will present a excessive likelihood of local control for this affected person, and that the practical end result will be higher than primary surgical procedure. A lately published randomized trial comparing radiation versus concomitant chemoradiation7 demonstrated a significant enchancment in local management charges and disease-specific survival in a series of a hundred sufferers with squamous cell most cancers of the top and neck. However, subsite evaluation revealed these variations to be significant for the larynx and hypopharyngeal sites, with no distinction in local management or disease survival for patients with orophyaryngeal cancer. If surgical procedure were the given possibility, all the consultants would method this tumor via a lip splitting incision and median or parmedian mandibulotomy and preserve the mandible until concerned with tumor. This supplies one of the best publicity, and preservation of mental nerve and possibly lingual nerve perform. None of the authors would perform a selective neck dissection sparing level V for a solitary 4-cm nodal metastasis. Futran advocates planned, post-therapy neck dissection in all sufferers with N+ illness on the time of main remedy planning. Bradford recommends a planned neck dissection for all sufferers with nodal illness initially 3 cm or higher. In the occasion of a neighborhood recurrence 6 months after therapy, all of the authors are in settlement with a lip splitting approach, neck dissection, and free flap reconstruction. Bradford and Peters would spare the mandible if uninvolved via a mandibulotomy method. Bradford and Futran would resect a minimal of the volume of the unique tumor with margins. The management of tonsillar carcinoma stays challenging and with no uniform consensus. Many other factors combine into the choice making process, corresponding to affected person preferences and biases, surgeon and institutional philosophies, geographical distances and social restrictions concerned with a quantity of visits to a tertiary care middle, notably in patients from a rural setting. In addition, definitive prospective research comparing oncologic outcomes, prices, useful outcomes, and quality of life are needed. Limitations of radiotherapy in the definitive therapy of squamous carcinoma of the tonsillar fossa. Surgery versus radiation therapy as a single-modality treatment of tonsillar fossa carcinoma: the Roswell Park Cancer Institute experience. Effectiveness of salvage neck dissection for superior regional metastases when induction chemotherapy and radiation are used for organ preservation. They digest the particle and "present" peptides on their surface (antigen presenting cell). Normal Range: 20 � 40% Lymphocytes make up the second main group of leukocytes and are primarily concerned in immune reactions. Upon goal recognition, they secrete cytotoxic compounds that may lyse the cell and/or induce apoptosis.
5 gm bactroban with visa
Notice also the bilateral pleural fluid collections acne scar removal bactroban 5 gm without prescription, consistent with bilateral hemothoraces acne girl purchase bactroban 5 gm amex. Esophagus � Usually seen in penetrating trauma however may happen in blunt chest trauma. Extraluminal gas adjoining to the positioning of damage might result in the suspicion of damage to the esophagus. May be positioned in the left superior intercostal vein, often from a left subclavian vein method. May even be placed within the subcutaneous tissues, which is in all probability not recognized on a standard frontal radiograph. Tears of the trachea and primary bronchi brought on by blunt trauma: Radiologic findings. Endotracheal tube in the best mainstem bronchus, the commonest place for a misplaced endotracheal tube. There is resulting left lung collapse with a left chest tube and left rib fracture. Asensio and Kuen-Jang Tsai Introduction � Indications for the use of the Emergency Department thoracotomy that seem in the literature vary from imprecise to fairly particular. It has been utilized in a selection of settings together with penetrating and blunt thoracic and/or thoracoabdominal accidents, cardiac and exsanguinating belly or extremity vascular injuries. Historic Perspective � Schiff in 1874 promoted the concept of open cardiac massage. Physiology Objectives Resuscitation of agonal sufferers with penetrating cardiothoracic injuries. To perform open cardiopulmonary resuscitation which might produce up to 60% of the conventional ejection fraction. Effects of Thoracic Aortic Cross Clamping-Negative Affects � � � � � � Decreases blood circulate to the stomach viscera to approximately 10%. Effects of Thoracic Aortic Cross Clamping-Unknowns � Length of safe cross clamp time. This procedure must be used as an adjunct to definitive restore of the stomach vascular injury. It should be strictly limited to those who arrive with vital signs at the trauma heart and experience a witnessed cardiopulmonary arrest. Pericardium is grasped between 2 Allis clamps and a pointy incision is made anterior to the phrenic nerve. At this time the trauma surgeons should evaluate the extent of hemorrhage current inside the left hemithoracic cavity. Note the place of the nasogastric tube, as the esophagus is superior to the aorta. A nasogastric tube beforehand positioned can function a guide in distinguishing the esophagus from the customarily considerably empty thoracic aorta. The descending thoracic aorta is bluntly dissected and a Crafoord-DeBakey cross clamp is applied. Results � the literature abounds with retrospective sequence describing the use of emergency division thoracotomy. Emergency Department Thoracotomy 279 � In the evaluate of over 7,335 sufferers present process emergency division thoracotomy there were 551 survivors. None of the patients subjected to Emergency Department thoracotomy for blunt cardiopulmonary arrest, noncardiac thoracic injuries or exsanguinating stomach vascular injuries survived. Proceedings of the American Association for the Surgery of Trauma 58th Annual Meeting, Baltimore, Maryland 1998; 20. Penetrating cardiac accidents: Prospective one-year preliminary report; An evaluation of assorted predicting outcome. Progressing via the centuries Hippocrates and Claudeus Galinus made transient references to stomach evaluation. In basic the liver and spleen are mostly injured in blunt stomach trauma, Table 26. For instance within the presence of an apparently isolated splenic injury, 10% will have related damage involving both the diaphragm or small bowel. In the presence of minor splenic injuries nevertheless such as a Grade 1 damage, one could anticipate less than 4% having diaphragmatic or bowel injury. Abdominal injury sustained throughout football or other contact sports activities may give rise to isolated splenic or renal accidents. Often deal with bar injuries transmit such drive as to resemble a penetrating injury. In the analysis of patients falling from heights and "jumpers", remember retroperitoneal accidents are a significant source of hemorrhage. Patients with transpelvic trajectories, gluteal gunshot wounds, and proximity stabbings must be evaluated by sigmoidoscopy. The check is frequently exhausting to interpret due to the lack of bowel preparation. Blood discovered should be interpreted as a optimistic check, no matter whether or not the precise harm is visualized or not. It offers exact information on the bullet trajectory as properly as on the situation of intra-abdominal organs, notably retroperitoneal ones. Its indications, though not yet absolutely explored, probably are: - Patients with equivocal medical indicators. It is greatest performed within the working room but can be done on the bedside with 300 Trauma Management enough local anesthesia. However, in chosen circumstances it might possibly present a crude idea of the wound-tract direction. About 40% of sufferers with penetrating trauma of the left thoracoabdominal space have diaphragmatic accidents, and amongst those, the damage is "occult" in one-third. Because no other take a look at can reliably rule out diaphragmatic accidents, laparoscopy is an important tool in the analysis of left penetrating thoracoabdominal trauma. The value of laparoscopy in different kinds of penetrating stomach trauma is unsure. False unfavorable outcomes occur frequently, particularly with retroperitoneal or small bowel injuries. Intensive monitoring, extra testing and a low threshold for laparotomy are applicable. Routine Exploration or Selective Management: Resolution of the Dilemma � There is settlement that stab wounds must be managed selectively. About one-third of patients with anterior and two-thirds with posterior stomach gunshot wounds may have no scientific important intra-abdominal harm. In giant prospective studies, it predicted the necessity for operation with a sensitivity of 95-100%. If medical examination is reliable for stab wounds, it must be reliable for gunshot wounds as well.
Bactroban 5 gm purchase with visa
A higher understanding of the biology and frequency of this phenomenon may be of appreciable value acne 12 weeks pregnant bactroban 5 gm cheap visa, each because of its intrinsic therapeutic impression and potential synergy with immunotherapy skin care routine quiz bactroban 5 gm order with visa. Results: A complete of 162 patients have been analysed and categorized by age into group A (28 to 55 y; n=46), B (56 to sixty four y; n= 87) and C (65 to 71 y; n=29). Martynkevich Hematology Clinic, Russian Research Institute of Hematology and Transfusiology, Saint-Petersburg, Russian Federation; 2Clinic, Military Medical Academy named after S. Kirov, Saint-Petersburg, Russian Federation; 3Clinic, North-Western State Medical University named after I. Mechnikov, Saint-Petersburg, Russian Federation Background: Studies over the past decade, have significantly improved our understanding of the molecular basis of multiple myeloma and mechanisms of disease development. The division of sufferers into varied risk groups primarily based on the chromosomal markers is being utilized by many facilities for select and optimize of therapeutic strategy. However, such molecular risk-stratification systems are repeatedly updated in accordance with the emergence of new information about the prognostic impact of anomalies. The role of complicated karyotype and mixture of genetic abnormalities remains unclear. Methods: the research included 159 sufferers (median age sixty three years, range 28 - eighty three; male: feminine ratio � 1:1. We additional searched the t (4;14), t(6;14), t(11;14), t(14;16) and t(14;20) in sufferers with IgH translocation. The dose of 140 mg/m was used in 13%, 15% and 30% of sufferers in group A, B and C, respectively. Conclusion: Combination two aberrations and complicated abnormalities are unfavorable prognostic markers. Baseline patient traits, disease and therapy related variables were reported utilizing descriptive statistics (frequency, median and percentage). Disease subtype was IgG kappa or lambda in 45%, gentle chain kappa or lambda in 28%, IgA kappa or lambda in 18% and others in 9%. Normal cytogenetic was seen in 57% while the remaining comprised of hyperdiploidy in 22%, advanced cytogenetic in 12%, t (11:14) in 6% and 1. Background: Multiple myeloma remains an incurable illness regardless of the emergence of new medicine. The search of optimal therapeutic strategy to improve life expectancy and remission in sufferers with this disease is continues. This is facilitated to the achievement of the utmost attainable response and eradication of residual tumor load. Aims: To determine the influence of autologous stem cell transplantation on efficiency of remedy and tumor load in patients with multiple myeloma. Schmidt 1 Hematology Clinic, Russian Research Institute of Hematology and Transfusiology, Saint-Petersburg, Russian Federation; 2Clinic, Military Medical Academy named after S. Kirov, Saint-Petersburg, Russian Federation; 3Clinic, North- Western State Medical University named after I. Acalabrutinib is a highly selective, potent, covalent Bruton tyrosine kinase inhibitor with minimal off-target actions. For patients with relapsed/refractory mantle cell lymphoma, acalabrutinib demonstrated an general response fee of 81%, with 40% of sufferers reaching a complete response (Lancet. Patients must be aged 65 years, have treatment-naive mantle cell lymphoma, and never be meant for stem cell transplant. Approximately 546 sufferers might be randomized 1:1 to receive oral acalabrutinib a hundred mg twice every day or placebo twice day by day plus 6 cycles of bendamustine (90 mg/m2 on days 1 and 2) and rituximab (375 mg/m2 on day 1 of each 28-day cycle). Patients attaining partial or complete responses will obtain maintenance rituximab every 2 cycles for as much as 12 additional doses plus acalabrutinib or placebo. The primary endpoint is unbiased evaluation committee-assessed progression-free survival per the Lugano Classification. Secondary endpoints embody total response fee (partial response), length of response, time to response, overall survival, and security. Exploratory endpoints embrace pharmacokinetic and pharmacodynamic assessments, minimal residual illness, patient-reported outcomes, and medical useful resource utilization. Disclosures: Wang, M: Consultant Advisory Role: AstraZeneca, Janssen, and MoreHealth; Board of Directors or advisory committees for Celgene and Janssen; Honoraria: Acerta Pharma, Celgene, Dava Oncology, Janssen, and Pharmacyclics; Research Funding: Acerta Pharma, 16 9 D. Louis, United Background: Mantle cell lymphoma is an aggressive B-cell nonHodgkin lymphoma that remains incurable with current therapies, together with commonplace first-line bendamustine and rituximab. There is a medical want for novel strategies to improve disease control in 554 � 2019 the Authors. Belada, D: Consultant Advisory Role: Gilead Sciences, Roche, Takeda; Research Funding: Takeda; Other Remuneration: Gilead Sciences, Roche. Dreyling, M: Honoraria: Bayer, Celgene, Gilead, Janssen, Roche, Acerta, Bayer, Celgene, Gilead, Janssen, Novartis, Roche, Sandoz; Research Funding: Celgene, Janssen, Mundipharma, Roche; Other Remuneration: Celgene, Janssen, Roche, Takeda. Goy, A: Consultant Advisory Role: Acerta Pharma, Celgene, Kite/Gilead, Pharmacyclics/J&J, and Takeda; Honoraria: Celgene, Pharmacyclics/J&J, and Takeda; Research Funding: Acerta Pharma, Celgene, Genentech, Kite/Gilead, Pharmacyclics/J&J, and Seattle Genetics; Other Remuneration: Acerta Pharma, Celgene, Pharmacyclics/J&J, and Takeda. Yin, M: Employment Leadership Position: Acerta Pharma; Stock Ownership: Acerta Pharma. Chen, T: Employment Leadership Position: Acerta Pharma; Stock Ownership: Acerta Pharma. Checkpoint inhibitors have revolutionised remedy for a quantity of strong tumours and induce frequent responses in Hodgkin lymphoma. The primary goal is to document durable anti-tumour activity of R-GemOx-Atezo, assessed by progression free survival at 1 12 months. Secondary goals are to decide safety, response rate and general survival rates. The trial opened recruitment in May 2018 and is scheduled to full recruitment in March 2020. Griffiths, G: Research Funding: Hold academic trial grants from quite a few firms including Roche. The study opened to enrollment in December 2018 with roughly 80 world sites deliberate. Buske, C: Honoraria: Roche, Janssen, Pfizer, Celltrion, Hexal; Research Funding: Roche, Janssen, Bayer. Abrisqueta, P: Consultant Advisory Role: Janssen, Abbvie, Roche; Honoraria: Janssen, Abbvie, Roche; Other Remuneration: Speaker: Janssen, Abbvie, Roche. A steady dosing schedule resulted in delayed (>cycle 2) grade 3 adverse events of diarrhea and pores and skin rash in ~1/3 of sufferers, likely associated to on-target effects on T-regs leading to immune-mediated toxicity. The part I part of the research was performed, based on continual reassessment methodology, from September 2014 to July 2017, and 21 patients were enrolled. At now, 60 sufferers have been enrolled, fifty seven of which treated at the maximum tolerated dose of romidepsin.
Red Jujube Date (Jujube). Bactroban.
- What is Jujube?
- How does Jujube work?
- Dosing considerations for Jujube.
- Are there safety concerns?
- Liver disease, muscular conditions, ulcers, dry skin, wounds, diarrhea, fatigue, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96108
Generic bactroban 5 gm fast delivery
This is the so-called glandar lamella acne location generic bactroban 5 gm amex, which is an actively proliferating layer many cells thick at its proximal margin acne glycolic acid order 5 gm bactroban amex. Within every week, proliferation of the lamella rolls the preputial folds progressively over the base of the glans to kind a preputial groove between the corona and the nascent prepuce. Proliferation of the Glandar Lamella In the proximal a part of the preputial groove, epithelial cells of the glandar lamella (stippled) grow to type a shelf between the preputial fold and the glans. As the preputial folds are pushed distally, the epithelial tissue of the lamella remains most lively on the proximal end, the bottom of the groove. The ground of the ectodermal intrusion makes contact with the top of the urethral plate that varieties the roof of the advancing urethra and the intervening double wall breaks down. This locations the brand new ectodermal lumen in continuity with the proximal, endodermal portion of the urethra. The mesenchyme lying between the epithelium of the preputial fold and the glandar lamella becomes active in conjunction with the lamellar epithelium and is incorporated between the margins of the glandar lamella because the preputial fold and the ventral margin of the glandar lamella are carried onto the glans with it. Thus, the preputial fold is transported distally by energetic growth of the mesenchyme between the folds in addition to by the fast proliferation of the ectoderm of the glandar lamella. The course of continues till the preputial fold covers all the glans aside from the ventral portion, which is blocked by the late closure of the urethral groove. Covering of the Glans By the time the fetus reaches 12 weeks of age, the distal urethra has formed and the flattened preputial fold not only covers the complete glans however, because of continued mesenchymal proliferation, extends beyond it. Separation of Prepuce and Glans the single epithelial layer between the prepuce and the glans forms epithelial pearls that start its degeneration into two layers. The separation begins distally, forming the glandopreputial area and it continues to the time of birth. Development of the Corpora the corpus spongiosum is shaped from the mesenchyme carried ventrally with the urethral folds and remaining after their fusion. The unorganized mesenchyme of the paired our bodies of the corpora cavernosa at first is supplied by capillaries. Dorsal vessels develop from the capillaries to turn into recognized because the dorsal arteries and deep dorsal vein by the thirteenth week. Two weeks later, the peripheral cells differentiate into the tunica albuginea, and people centrally distributed become organized into trabeculae. The grownup construction of the penis is fashioned within the new child interval, with the aggregation of smooth muscle and elastic tissue around the cavernous areas. Female Genital Differentiation Differentiation of Female External Genitalia Other than an increase within the distance between the anus and the genital constructions, probably the most certain sign of male differentiation in the genitalia is the appearance of an extended urethral groove on the caudal slope of the male genital tubercle. The finish of the indifferent stage at about 9 weeks additionally may be indicated by the formation of the perineal raphe via fusion of the urethral folds on the junction of the penis and scrotum and by the caudal migration of the genital swellings to kind the scrotum. Female sex could additionally be even more positively determined at about 10 weeks when the caudal curvature of the clitoris is clear and no perineal raphe has developed. Compared with those in the male, the homologous genital buildings within the feminine endure relatively little change after the indifferent stage. In the detached stage, the noncurved phallus has a recess at the website of the future coronal sulcus. By 8 weeks, the phallus appears to recede because the genital (labioscrotal) swellings encompass it and as greater growth of cavernous tissue in contrast with that of urethral tissue produces downward curvature. The caudal ends of the genital swellings which are to turn out to be the labia majora fuse to form the posterior commissure, and the urethral folds elongate to become the labia minora. The urethral groove prevents fusion of the urethral folds with the glandar lamella, leaving the prepuce covering only the dorsum of the clitoris. The phallic tubercle develops at a slower fee in the feminine than in the male and develops into a clitoris at term. The clitoris bends downward, in distinction to the perpendicular stance of the male phallus. It accommodates corpora cavernosa, but the corpus spongiosum stays vestigial except for the divided posterior portion, which stays as erectile tissue on both side of the vagina. The posterior ends of the urethral folds fuse, and the remaining portion develops into the labia minora. Epispadias results from failure of the mesodermal swellings to fuse in the midline in time, leaving a portion of the cloacal membrane exposed ventral to the genital tubercle. Rarely, the penile urethra and even the posterior urethra could additionally be absent so that the opening lies at the neck of the bladder. Superior duplication of the urethra could additionally be due to late fusion of the margins of an epispadiac urethral groove. Briefly, in contrast with epispadias, vesical exstrophy is the result of greater displacement and persistence of an abnormally large cloacal membrane that stops ingrowth of mesenchyme. Duplication of the clitoris is the rule within the feminine with vesical exstrophy, and failure of fusion of the m�llerian ducts is usually seen with more severe forms of cloacal exstrophy. The penis is markedly bifid in cloacal exstrophy, although in milder instances of the anomaly, the findings are a short penis resulting from separation of the pubic rami and dorsal chordee secondary to a short urethra or urethral plate. Hypospadias is a form of incomplete male differentiation that leaves the meatus mendacity proximal to its regular terminal position secondary to failure of the urethral groove to kind or from its failure to close fully. In hypospadias, the urethra derived from the urethral plate has not been closed by the urethral folds far sufficient distally to reach this ingrowth. At left, the tip of the forcep is near the urethral meatus, which lies proximal to its normal place, indicated by the blind pit in the glans. At right, urethral meatotomy has been carried out, a catheter has been inserted into the urethra, and the repair is about to start. Failure of fusion of the urethral folds in the formation of the glandar urethra and the associated growth of the preputial fold and glandopreputial lamella inhibit preputial growth on the ventrum, leaving a hooded prepuce. The perineal raphe, although it normally begins in the central level of the perineum where urethral closure begins, extends only to the proximal margin of the urethral orifice. At operation, chordee often seems as a sheet of disorganized fibrous tissue extending from the meatus distally along the shaft but may be represented only as ventral mucous membrane adherent to the incomplete urethral groove. The extra severe the diploma of hypospadias, the larger the enlargement of the prostatic utricle. Possible causes of hypospadias embrace a lapse in testosterone manufacturing throughout fetal life, insufficient conversion of testosterone to dihydrotestosterone by 5-alpha reductase in the native tissues or deficient local androgen receptors. A familial incidence has been reported by Bauer and associates who found that the risk of a second son being born with hypospadias is 26%. Other congenital anomalies are often found in boys with hypospadias: abnormalities associated with the higher urinary tract which would possibly be discovered on intravenous urography, undescended testes, and, rarely, orthopedic and cardiac defects. Alternatively, even though the corpus spongiosum types normally, the ventral side of the corpora cavernosa could fail to develop on the similar price because the dorsal aspect. Phimosis might be the outcomes of continued distal progress of the preputial lamella and delay in breakdown of the glandar lamella.
Purchase 5 gm bactroban visa
They have related coats and the smooth muscle in each has a helical arrangement as within the ureter skin carecom 5 gm bactroban discount amex, though the musculature of the ureter is thicker acne 60 year old woman bactroban 5 gm generic with amex. From a lobe, the accumulating ducts in a pyramid empty right into a calyx by way of a papilla. A minor calyx drains a single, compound or conjoined papilla; a major calyx drains two or more minor calyces. With the fusion, the medial margins of the calyceal cups lose their individual identification, leading to a compound papilla that empties right into a compound calyceal cup. The term calyx is utilized to the mix of three elements: (1) a cup-shaped receptacle, (2) a connecting neck, and (3) a funneled tube that opens into the renal pelvis. Strictly, calyx means cup, so the word is acceptable for that cup-shaped portion into which the papilla protrudes. Because calyx is also the word used for the whole advanced through such usage as minor calyx and main calyx, confusion arises when trying to check with the subdivisions of the complicated. Despite the disadvantages of adding one other time period, for readability the word calyceal cup replaces the strict which means of calyx on this textual content. In a minor calyx, the neck provides the transition from the taper of the cup to the expanse of the renal pelvis. In a significant calyx, the neck is the connection of the cup to the broader lumen of the following segment, the calyceal infundibulum. The infundibulum intervenes between the necks (and cups) of two or more papillae before connecting to the pelvis. The term is appropriate because the construction resembles and capabilities as a funnel, collecting from the necks and emptying at the infundibulopelvic junction. Thus, by definition, a minor calyx has one neck and one cup; a major calyx has no much less than two necks and two or more cups joined to the pelvis by an infundibulum. A main calyx drains two or extra calyceal cups and accompanying calyceal necks by way of a calyceal infundibulum into the renal pelvis. The pelvis can be thought-about a dilated portion of the ureter, with the calyces as its branches. The pelvis divides primarily into two or three major calyces, outlined as these with an infundibulum and two or extra necks and cups. Secondary division of the main calyces results in seven or eight nonbranching minor calyces. In the everyday kidney, these are arranged in two longitudinal rows, with the calyceal necks of those within the posterior row being extra attenuated than the stubbier anterior ones. The ends of the kidneys are drained by upper and lower pole calyces which would possibly be regularly compound or conjoined. Two kinds of pelves are recognized: the frequent one has a funnel form that continues to be open to receive urine previous to ureteral peristalsis; the other has a extra rounded form with an apparently closed outlet, the field pelvis. From a surgical viewpoint, the pelvis is considered intrarenal or extrarenal depending on its relation with the hilum, and intermediate variations are potential. An intrarenal pelvis could additionally be considered as the results of later division of the ureteric bud, leading to shorter calyces than within the extrarenal kind. E Major calyx Infundibulum Minor calyx Such a pelvis makes surgical access to and manipulation inside the inside of the kidney more difficult. The capacity of the pelvis is about 6 ml; volumes higher than 15 ml may be considered irregular. The major calyces could develop from a single pelvis (true pelvis of Br�del), from a transitional form, or from a divided pelvis with a zone of cortical substance between the second and third, and the fourth and fifth full calyces. The divided pelvis, the intense of which is the bifid pelvis shown in the figure, has a smaller higher pole major calyx and a bigger lower pole main calyx, leaving the midportion of the kidney without branches. In the divided kidney, the arrangement of the minor calyces seldom follows the usual anteroposterior sample, thus posing issues for calyceal puncture and requiring indirect radiographs. The kidneys are slightly rotated on a vertical axis in three planes: coronal, transverse, and sagittal. Measurement from the Frontal Plane of the Kidney From the frontal aircraft of the kidney, the angles are 46� anteriorly for the axis of the anterior calyces and 30� posteriorly for that of the posterior calyces. Transverse Projection the pelvis and hilum have a extra anterior position than the outer convex border by an angle of 30�. Sagittal Projection the lengthy axis of the kidney is angled posteriorly by about 10�. Radiologic Orientation for Endourology, Right Kidney In transverse section, the body is shown positioned within the indirect place preparatory to puncture of a posterior calyx. It is critical to know the angles that the calyces take relative to the coronal airplane of the body previous to percutaneous puncture. The use of lateral and indirect radiographic views along with an anteroposterior view allows psychological construction in three dimensions. Computed tomographic reconstruction of pyelograms produces a three-dimensional image that could be helpful. Radiologic Orientation for Endourology, Left Kidney Orientation from the Coronal Plane of the Body the angle of the axis of the anterior calyceal angle is 3� anterior to the coronal aircraft of the physique. Therefore, most parts of an anterior calyx are visualized on a urogram of a supine subject, whereas the posterior calyces appear end-on. The angle of the axis of the posterior calyx is 60 levels posteriorly from the coronal plane. Orientation from the Frontal Plane of the Kidney From the frontal aircraft of the kidney, the anterior calyces have an angle of 33� anteriorly; the posterior calyces have a similar angle of 30�, but posteriorly. The fornix marks the site where the wall of a calyceal cup joins the renal parenchyma; it seems as a rim around the base of the papilla. The fornix is marked at the margin of the papilla by a change from the thick, whitish epithelial wall of the calyx to the darker and extra clear overlaying of the papilla. Microscopically, the transitional epithelium of the calyx adjustments abruptly to a single layer of low cuboidal epithelium where the calyx joins the papilla on the fornix. Beneath the fornix, an extensive vascular bed drains into the interlobar arteries and veins and into lymph collectors. In addition, the fornical rim acts as a hinge for mobility of the wall of the cup because the fornix is in a position to spherical out throughout ureteral obstruction, making the calyceal cup seem extra spherical on pyelography. In the higher half is the tip of a papilla, with cross sections of amassing ducts. Studies using injection of India ink have shown that the pathway developing during acute obstruction passes from the fornix to the perirenal area through the renal sinus. The papilla is surmounted by the cribriform plate, on which the collecting ducts of Bellini open. Structure of the Pelvic and Calyceal Wall the conducting structures are contained in the renal sinus, which extends from the fornix at the papillary rim to the hilum. Areolar tissue surrounding the pelvis and the vessels, and the nerves and the lymphatics in the hilum is steady with perirenal fats.
Generic bactroban 5 gm on-line
Miller acne problems 5 gm bactroban buy with amex, R: Employment Leadership Position: Corvus Pharmaceuticals; Stock Ownership: Corvus Pharmaceuticals acne hyperpigmentation 5 gm bactroban cheap amex. Th skewing in mice was decided utilizing an ovalbumin vaccine adoptive switch mannequin. Treatment was well tolerated with no dose limiting toxicities and no modifications in lymphocyte counts. We are broadening the characterization of this combination regimen in affected person biopsies from our ongoing trial. Changes in the proportion of M1/M2 macrophages and in the expression of immune checkpoints were studied by circulate cytometry. Purroy1 uted in four teams: selinexor (5mg/kg twice a week), ibrutinib (25mg/kg daily), mixture of both or car. Although tumoral development was blocked by all remedies, the combination of both drugs significantly increased survival in comparability with monotherapies. Treatment with both medication favors an anti-tumoral immune response by shifting polarization towards anti-tumoral M1. Bosch, F: Honoraria: Roche, Celgene, Takeda, Astra-Zeneca, Novartis, AbbVie, Janssen; Research Funding: Roche, Celgene, Takeda, AstraZeneca, Novartis, AbbVie, Janssen. Toretsky, J: Consultant Advisory Role: Oncternal Therapeutics; Stock Ownership: Oncternal Therapeutics. Bertoni Institute of Oncology Research, Universit� della Svizzera Italiana, Bellinzona, Switzerland; 2Institute for Research in Biomedicine, Universit� della Svizzera italiana, Bellinzona, Switzerland; 3Department of Cell Biology, Albert Einstein College of Medicine and Montefiore Medical Center, New York, United States; 4Medical Oncology, Oncology Institute of Southern Switzerland, Bellinzona, Switzerland; 5Oncternal Therapeutics, San Diego, United States; 6Departments of Oncology and Pediatrics, Lombardi Comprehensive Cancer Center, Georgetown University, Washington, D. The greatest benefits had been achieved in the mixture with venetoclax and lenalidomide. We assessed its preclinical activity as single agent in 57 lymphoma cell strains and in combination with selected medication in T cell lymphomas-derived cell traces. Zucca, E: Consultant Advisory Role: Roche, Mei Pharma, Astra Zeneca; Honoraria: Gilead; Research Funding: Roche and Janssen; Other Remuneration: travel grants from Abbvie and Gilead. Stathis, A: Research Funding: Bayer, Roche; Other Remuneration: journey grant from AbbVie. Based on a related, grade 2 nonhematologic antagonistic occasion (fever, chills, vomiting), the 3+3 dose escalation design was triggered at the 0. The terminal section half-life estimated for complete antibody in 3 sufferers ranged 37-47 hours. Shah, N: Consultant Advisory Role: Juno, Kite Pharma, Cellectar; Stock Ownership: Onsec, Geron, Exelixis; Research Funding: Lentigen Technology. Krishnan, A: Employment Leadership Position: City of Hope; Consultant Advisory Role: Celgene, Onyx, Janssen Oncology, Takeda, Kite Pharma, Seattle Genetics, Sutter Medical Group, Teuda; Research Funding: Celgene, Takeda. Shah, N: Employment Leadership Position: University of California, San Francisco; Consultant Advisory Role: Takeda, Celgene, Indapta Therapeutics, TeneoBio, Brystol-Myers Squibb, Sanofi, Seattle Genetics; Stock Ownership: Indapta Therapeutics; Research Funding: Celgene, Bluebird Bio, Janssen. Burke, J: Employment Leadership Position: Rocky Mountain Cancer Center; Consultant Advisory Role: Celgene, Genentech, Gilead, Abbvie, Seattle Genetics, Tempus Labs, Kite, Juno; Research Funding: Janssen. Spira, A: Employment Leadership Position: Virginia Cancer Specialists; Research Funding: Roche, AstraZeneca, Boehringer Ingelheim, Astellas Pharma, MedImmune, Novartis, Newlink Genetics, Incyte, Abbvie. Popplewell, L: Employment Leadership Position: City of Hope; Honoraria: AstraZeneca, Cardinal Health. Andreadis, C: Employment Leadership Position: University of California, San Francisco. Kaufman, J: Employment Leadership Position: Winship Cancer Institute of Emory University; Consultant Advisory Role: Pharmacyclics, Janssen, Abbvie, Roche, Takeda; Honoraria: Janssen; Research Funding: Novartis, Merck, Celgene. Niesvizky, R: Employment Leadership Position: Weill Cornell Medical College, New York-Presbyterian Hospital. Martin, T: Employment Leadership Position: University of California, San Francisco; Consultant Advisory Role: TeneoBio; Research Funding: Sanofi, Amgen, Genentech/Roche. DiLea, C: Employment Leadership Position: Aclairo Pharmaceutical Development Group. Matheny, S: Employment Leadership Position: Sutro Biopharma; Stock Ownership: Sutro Biopharma. Leonard, J: Employment Leadership Position: Weill Cornell Medical College, New York-Presbyterian Hospital; Consultant Advisory Role: Celgene, Abbvie, Sutter Medical Group. The clinically most relevant unwanted facet effects are neurological signs and cytokine launch syndrome. Prerequisite for durable remission is therapy at the effective dose of 60 g/m�/day. The principal G3/4 toxicities noticed have been haematological, together with thrombocytopenia, neutropenia, and lymphopenia with incidence rising with growing dose. A normal 3+3 design was used; the primary cohort receiving 40mg/m2 iv tinostamustine over 1 hour. Four ascending cohorts to a maximum dose of 120mg/m2, and shorter infusion occasions have been additionally explored. Casasnovas, R: Consultant Advisory Role: Roche, Takeda, Gilead, AbbVie, Bristol-Myers Squibb, Merck, Karyopharm; Research Funding: Roche, Gilead, and Takeda. Munoz, J: Consultant Advisory Role: Pharmacyclics/Janssen, Bayer, Gilead/Kite, Pfizer, Juno/Celgene, and Bristol-Myers Squib; Other Remuneration: Gilead/Kite, Bayer, Pharmacyclics/Janssen, and AstraZeneca. Corrado, C: Employment Leadership Position: Incyte Corporation; Stock Ownership: Incyte Corporation. DeMarini, D: Employment Leadership Position: Incyte Corporation; Stock Ownership: Incyte Corporation. Zhao, W: Employment Leadership Position: Incyte Corporation; Stock Ownership: Incyte Corporation. Chen, X: Employment Leadership Position: Incyte Corporation; Stock Ownership: Incyte Corporation. Coleman, M: Consultant Advisory Role: Gilead, Bayer, Celgene; Stock Ownership: Kite Pharmaceuticals; Research Funding: Incyte, Gilead, Merck, Bayer, Celgene; Other Remuneration: Gilead, Bayer, Celgene, Pharmacyclics. In a deliberate interim futility evaluation carried out within the first forty sufferers handled in Group A, if thirteen (32. Results: At knowledge cutoff (22 Jun 2018), 60 patients (Group A, n = 55; Group B, n = 5) were treated (median age, seventy one years [range, 36�94]; men, sixty three. Gr 3/4 aspartate aminotransferase and alanine aminotransferase elevations occurred in 5. Acalabrutinib/pembrolizumab discontinuations had been as a end result of progressive illness (62%/56%) and antagonistic occasions (15%/26%). Disclosures: Witzig, T: Honoraria: Sandoz; Immune Design; Research Funding: Acerta; Celgene; Novartis; Spectrum. Lyons, R: Employment Leadership Position: Texas Oncology; Stock Ownership: Texas Oncology; Research Funding: avvie, Celgene, Gilead, GenetechIncye, Rigel, Takeda. Chan, E: Employment Leadership Position: Acerta Pharma, Genentech/Roche; Stock Ownership: Acerta Pharma, Genentech/Roche, Eli Lilly & Company. Patel, P: Employment Leadership Position: Acerta/AstraZeneca; Stock Ownership: Acerta/AstraZeneca.
Bactroban 5 gm generic overnight delivery
It is a matter of debate whether or not such vessels contribute significantly to the obstructive course of skin care with vitamin c bactroban 5 gm buy visa. They are nonetheless relatively giant at start skin care with hyaluronic acid buy bactroban 5 gm amex, solely to regress quickly in the course of the first 3 weeks of life. During the eighth gestational month, the zona glomerulosa seems, adopted by the zona fasciculata at time period; the zona reticularis follows within the subsequent 3 to 6 months, with the cortex completely differentiated by 2 years. Origin of the Adrenal Cortex and Medulla Two separate tissues contribute to the formation of the adrenal glands, providing layers that stay distinct into adult life (Table 12-3). The adrenal cortex comes from mesothelial buds on the upper third of the mesonephros that project into the primitive celom with the gonad. Some cells may not be a part of the aggregation, accounting for accent adrenal cortical tissue about the adrenal gland and kidney, with the spermatic vessels or testis within the male and within the broad ligament and ovary in the feminine. The adrenal medulla is derived from primitive ectodermal cells of the neural crest within the creating sympathetic nervous system. These sympathogonia usually mature into sympathoblasts and in the end into ganglion cells within the sympathetic ganglion. Alternatively, and of importance to the formation of the adrenal medulla, they might migrate and differentiate into chromaffin endocrine cells, the pheochromoblasts, that can mature into chromaffin cells after penetrating the adrenal cortical primordium to form the adrenal medulla (Table 12-4). Distribution of Fetal Chromaffin Bodies In fetal life, the pheochromoblasts type chromaffin our bodies which are distributed along the aorta, offering the main supply of catecholamines. These cells migrate to and invade the adrenal cortical aggregation to kind the adrenal medulla. Some of these chromaffin our bodies regress only partially after start and stay because the paraganglion system distributed inside and adjacent to the prevertebral sympathetic ganglia and within the several sympathetic plexuses and ganglia (celiac, mesenteric, renal and adrenal, and hypogastric) in addition to a plexus on the aortic bifurcation, the organ of Zuckerkandl. This system is a secondary source of catecholamines all through life and should turn into the tissue of origin of pheochromocytomas. Two bigger aggregates of chromaffin tissue associated to the superior hypogastric plexus, the para-aortic bodies, stay on either facet of the aorta in an inverted U-shape looped over the inferior mesenteric artery. These our bodies enlarge throughout early postnatal life, solely to just about disappear at puberty. Adrenal Blood Supply Arteries the supply of blood for the adrenal is probably the most cranial of the segmental mesonephric roots that when provided the urogenital (mesonephric) arterial rete. Especially on the best facet, smaller accent arteries, often a number of, could come from the inferior phrenic or the renal arteries. Veins Resolution of the renal venous plexus on the best leaves a single, short vein running obliquely that connects to the posterior floor of the vena cava. However, the place of the adrenal gland is independent of that of the kidney, because with an ectopic kidney, the adrenal gland is present in its regular position. Agenesis might happen, usually associated with renal agenesis secondary to failure of the complete blastema. Of surgical significance when working on a solitary kidney is the rare possibility that the only adrenal gland lies underneath the renal capsule. Accessory adrenal cortical rests are discovered intra-abdominally and retroperitoneally within abdominal and sexual organs. As famous previously, extramedullary chromaffin tissue is often discovered and should turn into remodeled right into a pheochromocytoma. The subcutaneous layer differentiates into the dermis, superficial fascia, and deep fascia of the body wall. The retroperitoneal layer, as the retroperitoneal connective tissue, strains the physique wall and surrounds the gastrointestinal and urinary organs (Table 12-5). With maturation, three strata can be distinguished in the retroperitoneal connective tissue. The ectopic adrenal tissue is normally subcapsular and is most often in the upper pole. It could assume a plaque-like type (as on this image) but can also be wedge-shaped or spherical. The small mixture of ectopic adrenal cortical cells shown right here was an incidental discovering in a testis excised for unrelated reasons. Fusion of the Colonic Mesenteries In addition to a masking of main retroperitoneum, the kidneys acquire a secondary coat from the fusion of the colonic (and on the left, duodenal) mesenteries because the bowel rotates into its ultimate position. At first, the dorsal mesentery varieties a barrier between the best and left sides because it runs the length of the peritoneal cavity. The future ascending colon rotates over the bottom of the mesentery, exposing the best side of its mesentery. At the same time, the descending colon with its mesentery merely rises into the left upper quadrant, thus maintaining the original right and left orientation of the surfaces of the original colonic mesentery. As the left mesocolon meets the first peritoneum on that side, its left aspect fuses with it, and the underlying mesothelial layers disappear. It differs from the migration fascia that outcomes from the migration of primitive tissues during growth during which migration produces linear orientation of the connective tissue fibers, which, in turn, are compressed by further development. The lack of circumscription imparts an infiltrative appearance, and the histologic similarity between regular adrenal cortical tissue and clear cell carcinoma can create diagnostic difficulty on intraoperative frozen sections. Beneath this layer is the intermediate stratum embedding the urinary system that differentiates into dorsal and ventral layers in the area of the kidneys. By the seventh month of gestation, the layers of the intermediate stratum are properly developed and form the renal fascia as the ventral layer splits into two layers, an anterior lamina (Toldt) with the perirenal fat and a posterior lamina (Zuckerkandl). These lamina fuse laterally on each side behind the ascending and the descending colon, where they kind a single layer, the so-called lateroconal fascia. The conventions used in this guide for naming the fascial layers are shown in Table 12-7. For instance, fascial layers are particularly numerous concerning the kidney in addition to concerning the pelvic and scrotal organs but are absent concerning the umbilicus. Fascias In the renal area, the fascias of surgical importance are the renal fascia and its extension, the lateroconal fascia, and the fusion-fascia underneath the colon. The renal fascia has an anterior and a posterior lamina, with the kidney and adjacent constructions mendacity between in the perirenal area. Anterior Lamina the anterior lamina of the renal fascia (fascia of Toldt), a layer that includes the hooked up perirenal fats, is fashioned by local thickening of the intermediate stratum. Perirenal fats can be distinguished by its paler color and finer texture in contrast with that of the pararenal fats that lies exterior the renal fascia. The perirenal fats incorporates connective tissue fibers that are particularly concentrated concerning the upper renal pole, and the fat is of larger thickness over the posterior and lateral surfaces of the fascia than over the anterior floor. The anterior lamina also becomes fused with the inside (intestinal) stratum on the sites where the vessels to the digestive tract move by way of from the aorta and vena cava. Posterior Lamina the posterior lamina of the renal fascia (fascia of Zuckerkandl), additionally derived from the intermediate stratum, is thicker than the anterior one. Over the psoas major and quadratus lumborum, the posterior lamina turns into fused with the fascia of the outer stratum, represented by the transversalis fascia. In the midline, the lamina is attached to the ventral surfaces of the vertebral bodies and to the anterior lamina of the renal fascia as the two laminas fuse and mix with the connective tissue across the aorta, vena cava, and the renal artery and vein in addition to the tissue surrounding the autonomic nerves of the superior mesenteric plexus.