
Atorlip-10 dosages: 10 mg
Atorlip-10 packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

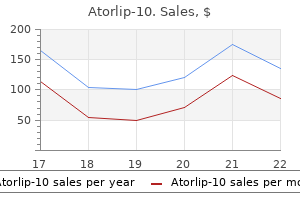
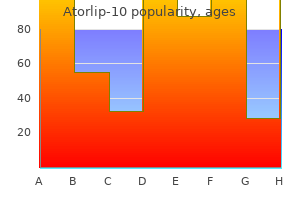
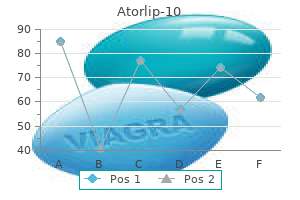
Atorlip-10 10 mg line
Progression of myopia and excessive myopia within the Early Treatment for Retinopathy of Prematurity Study cholesterol jones and his band atorlip-10 10 mg purchase mastercard. Visual field extent at 6 years of age in children who had high-risk prethreshold retinopathy of prematurity cholesterol medication dangers generic atorlip-10 10 mg fast delivery. Grating visual acuity results in the Early Treatment for Retinopathy of Prematurity Study. Outcome of eyes growing retinal detachment during the Early Treatment for Retinopathy of Prematurity Study. Retinopathy of prematurity in infants weighing less than 500 grams at birth enrolled in the Early Treatment for Retinopathy of Prematurity Study. Prevalence and course of strabismus through age 6 years in participants of the Early Treatment for Retinopathy of Prematurity randomized trial. Correlation of recognition visible acuity with posterior retinal structure in superior retinopathy of prematurity. Refractive outcomes following bevacizumab monotherapy compared with standard laser therapy: A randomized medical trial. The influence of macular edema on visible function in intermediate, posterior, and panuveitis. Associations among visual acuity and vision- and health-related high quality of life amongst patients in the Multicenter Uveitis Steroid Treatment Trial. Fluorescein angiography versus optical coherence tomography for diagnosis of uveitic macular edema. Cost-effectiveness of fluocinolone acetonide implant versus systemic therapy for noninfectious intermediate, posterior, and panuveitis. Benefits of systemic anti-inflammatory therapy versus fluocinolone acetonide intraocular implant for intermediate uveitis, posterior uveitis, and panuveitis. Quality of life and dangers related to systemic anti-inflammatory remedy versus fluocinolone acetonide intraocular implant for intermediate uveitis, posterior uveitis, or panuveitis: Fifty-four-month results of the Multicenter Uveitis Steroid TreatmentTrial and Follow-up Study. The Multicenter Uveitis Steroid Treatment Trial: Rationale, design, and baseline characteristics. Validation of a photographic vitreous haze grading method for medical trials in uveitis. Identifying a clinically significant threshold for change in uveitic macular edema evaluated by optical coherence tomography. Evaluation of an intravitreal fluocinolone acetonide implant versus standard systemic therapy in noninfectious posterior uveitis. Dexamethasone intravitreal implant for noninfectious intermediate or posterior uveitis. Use of the fluocinolone acetonide intravitreal implant for the treatment of noninfectious posterior uveitis. Mortality in sufferers with the acquired immunodeficiency syndrome handled with both foscarnet or ganciclovir for cytomegalovirus retinitis. Morbidity and toxic results associated with ganciclovir or foscarnet remedy in a randomized cytomegalovirus retinitis trial. Clinical vs photographic evaluation of treatment of cytomegalovirus retinitis: Foscarnet�Ganciclovir Cytomegalovirus Retinitis Trial report eight. Assessment of cytomegalovirus retinitis: medical evaluation vs centralized grading of fundus images. Rhegmatogenous retinal detachment in patients with cytomegalovirus retinitis: the Foscarnet�Ganciclovir Cytomegalovirus Retinitis trial. Quality of life after I-125 brachytherapy versus enucleation for choroidal melanoma: 5-year outcomes from the Collaborative Ocular Melanoma Study. Risk elements for development of cytomegalovirus retinitis in patients with acquired immunodeficiency syndrome. Photographic measures of cytomegalovirus retinitis as surrogates for visible outcomes in handled sufferers. Reliability, validity, and responsiveness of basic and disease-specific quality of life measures in a clinical trial for cytomegalovirus retinitis. The ganciclovir implant plus oral ganciclovir versus parenteral cidofovir for the treatment of cytomegalovirus retinitis in sufferers with acquired immunodeficiency syndrome: the Ganciclovir Cidofovir Cytomegalovirus Retinitis Trial. Visual loss in sufferers with cytomegalovirus retinitis and acquired immunodeficiency syndrome earlier than widespread availability of extremely energetic antiretroviral remedy. Complications of ganciclovir implant surgery in sufferers with cytomegalovirus retinitis. Course of cytomegalovirus retinitis within the era of highly lively antiretroviral remedy. The relationship between visual field size and electroretinogram amplitude in retinitis pigmentosa. Further analysis of docosahexaenoic acid in sufferers with retinitis pigmentosa receiving vitamin A treatment: subgroup analyses. Clinical trial of lutein in sufferers with retinitis pigmentosa receiving vitamin A. Methods, statistical features, and baseline outcomes of a standardized, multicentered ophthalmological surgical trial: the Silicone Study. Vitrectomy with silicone oil or with perfluoropropane gasoline in eyes with extreme proliferative vitreoretinopathy. Relaxing retinotomy with silicone oil or long-acting gasoline in eyes with severe proliferative vitreoretinopathy. Vitrectomy with silicone oil or long-acting fuel in eyes with severe proliferative vitreoretinopathy: outcomes of extra and long-term follow-up. Internal limiting membrane peeling versus no peeling for idiopathic full-thickness macular hole: A pragmatic randomized managed trial. Baseline traits, pure historical past, and danger elements to development in eyes with stage 2 macular holes. Prospective randomized trial of vitrectomy or statement for stage 2 macular holes. Vitrectomy for the treatment of full-thickness stage 3 or 4 macular holes: results of a multicenter randomized clinical trial. A randomized managed trial of alleviated positioning after small macular gap surgery. Two-year outcomes of a randomized clinical trial evaluating natural historical past, vitrectomy, and vitrectomy plus autologous serum: Moorfields Macular Hole Study Group report no. Comparison of face-down and seated position after idiopathic macular gap surgery: A randomized clinical trial. Improvement in patient-reported visible perform after ocriplasmin for vitreomacular adhesion. A multicenter randomized managed scientific trial comparing pneumatic retinopexy with scleral buckling. Dexamethasone posterior segment drug delivery system in the treatment of macular edema ensuing from uveitis or Irvine�Gass syndrome. Intravitreal bevacizumab for prevention of early postvitrectomy hemorrhage in diabetic sufferers.
10 mg atorlip-10 effective
Retinal cavernous hemangioma: fifty-two years of scientific follow-up with clinicopathologic correlation cholesterol levels in beef atorlip-10 10 mg best. Macular cavernous hemangioma related to peripheral vascular anomalies and nonperfusion cholesterol med chart 10 mg atorlip-10 purchase with amex. Cavernous haemangioma of the retina and optic disc: a report of three circumstances and a review of the literature. Epiretinal membrane demonstrated by optical coherence tomography in a affected person with retinal cavernous hemangioma. Cavernous hemangioma of the retina: a four-generation pedigree with neurocutaneous manifestations and an example of bilateral retinal involvement. Vitrectomy for persistent vitreous hemorrhage from a cavernous hemangioma of the optic disk. Although this can be related to a cavernous hemangioma of the midbrain, Yen and Wu38 have reported a patient with agenesis of the internal carotid artery related to retinal cavernous hemangioma and bilateral oculomotor palsies. One daughter had a retinal cavernous hemangioma, one other daughter had seizures and cutaneous lesions, six relatives had seizures, and 14 different relatives had cutaneous vascular lesions. Cavernous hemangioma of the retina and agenesis of inner carotid artery with bilateral oculomotor palsies. Cerebral cavernomas in a family with multiple cutaneous and uterine leiomyomas related to a model new mutation in the fumarate hydratase gene. Cavernous hemangioma of the retina, cutaneous angiomas, and intracranial vascular lesion by computed tomography and nuclear magnetic resonance imaging. A case of bilateral cavernous hemangioma related to intracerebral hemangioma. Cavernous angiomas of the brain: account of fourteen personal cases and review of the literature. Mutations in 2 distinct genetic pathways lead to cerebral cavernous malformations in mice. Those affected had been from 7 to eighty four years old (mean 36 years old, normal deviation � 15 years), and 151/335 (45%) have been male. Neovascularization of the iris, neovascular glaucoma, and phthisis bulbi can occur in eyes with massive or a quantity of tumors. Five small retinal hemangioblastomas at varied stages of early development are seen in temporal retina posterior to the equator. The largest two lesions (arrowheads) remain sessile (flat) and present easily visible early afferent and efferent vessels. Two nodular hemangioblastomas manifest well-developed afferent and efferent vessels, with none related exudation. Retinal hemangioblastomas of varied sizes, dilated and tortuous afferent and efferent vessels, hard exudates, and foci of epiretinal fibrosis are seen on this severely affected eye. Visual acuity is decreased in the setting of extreme onerous exudates involving the macula. These tumors typically exhibit minimal growth over years, but typically evolve exudation finally. Very small lesions, as talked about earlier, could also be exhausting to distinguish from other focal microvascular abnormalities when different situations are being considered. The lesion that the majority closely resembles bigger tumors, and could additionally be tough to differentiate in some circumstances, is a vasoproliferative tumor of the ocular fundus. For identifying small tumors or evaluating atypical lesions or options, ancillary testing can be helpful. Vision loss is usually brought on by exudation affecting the macula, glial proliferation or posterior hyaloid contraction related to the tumor with resultant retinal striae and thickening, or in advanced instances, traction and/or exudative retinal detachment. Cellophane maculopathy within the setting of thickened posterior hyaloid and/or early epiretinal membrane formation is seen temporally. Expanding cerebellar hemangioblastomas could trigger intracranial hypertension, papilledema, and eventual optic atrophy if not handled in a well timed fashion. Central nervous system hemangioblastomas hardly ever happen in the optic nerve, optic chiasm, or optic tract. Older ultrastructural and immunohistochemical studies instructed that these cells might symbolize lipidized fibrous astrocytes or glial cells. Small tumors with features suggesting inactivity or partial regression can sometimes be observed, however in such circumstances, shut surveillance is imperative, and the threshold for offering ablative remedy for any sign of development or exercise ought to be low. Small tumors may be destroyed fairly readily, earlier than vision loss has occurred and with minimal dangers of therapy; in distinction, larger lesions can be rather more difficult to ablate, and injury induced by remedy frequently results in a variable and occasionally significant acute exudative response that can cause retinal detachment and threaten imaginative and prescient. Identification of any ocular lesions requires prompt intervention and close subsequent surveillance, with follow-up tailored to the circumstances. Treated tumors are adopted carefully after any attempted ablation, to assess for expected regression or any signal of regrowth or recurrent exudation. Various teams have published suggestions for age of initial screening and frequency of follow-up testing for cardinal disease features (Table 134. The feasibility and efficacy of remedy depend on a number of elements, such as tumor size, tumor location, degree of exudation, presence of retinal detachment, associated epiretinal fibrosis or hemorrhage, associated chorioretinal scarring (as from previous ablative treatment), position relative to location of any scleral buckling supplies in previously operated eyes, the number and traits of different viable tumors inside the eye, associated retinal vascular changes or vascular proliferation, and response to earlier treatment. Hemangioblastoma of the Retina and Von Hippel�Lindau Disease 2433 typical for panretinal photocoagulation or laser retinopexy, and energy adequate to create whitening within the area of the burn. Some have advocated laser photocoagulation of the retina across the tumor, but we often confine burns to an space sufficient to blanch the whole tumor surface. The look of scant intraretinal or preretinal hemorrhage on the tumor floor instantly following laser photocoagulation is common, however vitreous hemorrhage is rare and normally solely seen with treatment of bigger lesions (see below). Retreatment is typically essential, especially for bigger tumors (see below), and the technique for retreatment is the same. Success presumably depends on whether or not sufficiently intense photocoagulation can be applied all through the thickness of the tumor. The treatment technique is much like the one described above for small lesions, but frequently involves applying long-duration burns (often more than zero. Sessile tumors are extra simply handled than very nodular ones, and any associated exudation, epiretinal fibrosis, or preexisting hemorrhage can significantly hamper ability to apply adequate therapy. Appearance of scant intraretinal or preretinal hemorrhage on the tumor is widespread with therapy, as for smaller lesions, and vitreous hemorrhage is unusual. Reasonable success rates have been reported with use of laser endophotocoagulation at vitrectomy in instances in which ablative remedy is utilized adjunctive to vitreoretinal surgery. However, transscleral cryotherapy is regularly efficient for destruction of those tumors, even within the setting of related exudation, hemorrhage, or fibrosis. Treatment may be utilized transconjunctivally in the office setting for anterior tumors, or utilized transsclerally in the surgical suite after conjunctival incision to enable for acceptable probe placement for postequatorial tumors. In either case, we usually use a double freeze�thaw technique as advocated by Singh and colleagues. Whether following laser photocoagulation or cryotherapy, complete disappearance of a treated tumor this size is rare, and evaluation of whether or not enough destruction has been achieved could be challenging. Encouraging signs include a decrease in tumor size, lower in redness or vascularity, decision of any subretinal fluid and onerous exudates, normalization of the caliber and decrease in the tortuosity of any feeding and draining vessels, and an underlying chorioretinal scar. Thermal laser photocoagulation and photodynamic therapy are virtually all the time ineffective for giant tumors.
Diseases
- Protein R deficiency
- Braddock Jones Superneau syndrome
- Lupus anticoagulant, familial
- Contact dermatitis
- Telecanthus with associated abnormalities
- Chromosome 1, monosomy 1p31 p22
- Giant axonal neuropathy
Order 10 mg atorlip-10 mastercard
When the anterior chamber hemorrhage has been cleared to adequately visualize the pars plana infusion cannula complete list of cholesterol lowering foods 10 mg atorlip-10 buy fast delivery, the blunt infusion needle may be eliminated and changed with a fiberoptic probe cholesterol synthesis flow chart purchase atorlip-10 10 mg overnight delivery. Surgery for Ocular Trauma: Principles and Techniques of Treatment 2099 aims of the procedure. In most cases the lens is eliminated via the pars plana utilizing both the vitrectomy probe or an ultrasonic fragmenting system. After the anterior segment is cleared, the vitrectomy may be carried out, continuing from anterior to posterior. The peripheral retina is then fastidiously inspected for retinal tears and detachment. Cryopexy should be averted because of concern about the elevated inflammatory response and launch of profibrotic cytokines. Placement of a posterior radial scleral buckle is beneficial in circumstances with persistent traction adjoining to a posterior retinal tear. Subretinal fluid normally is drained transvitreally during a fluid�gas change either by way of a posterior retinal break or via a posterior retinotomy created in an area freed from traction, ideally superonasal to the optic nerve. In some circumstances, extrusion can be utilized to flatten the retina by drainage of posterior subretinal fluid through a peripheral retinal break. Long-acting gases, similar to sulfur hexafluoride or perfluoropropane, or silicone oil may be injected to present a longer-lasting inner tamponade. However, when the incarceration is extra posterior, scleral buckling is more difficult and retinotomy may be necessary. In the latter situation, they carried out retinotomies circumscribing the retinal incarceration website. With these methods, they achieved anatomic success in eleven of 15 eyes (73%), but solely six eyes regained visual acuity of 5/200 or higher. Eyes with traumatic retinal detachment related to retinal incarceration appear to carry a poor prognosis even when managed aggressively. Intraocular bleeding is a frequent intraoperative hazard of vitrectomy for penetrating accidents and, if huge and uncontrolled, can preclude successful vitrectomy. Control of bleeding by infusion of a thrombin answer at a focus of a hundred U/mL has been reported. When the cornea becomes cloudy because of epithelial edema, the epithelium may be carefully removed with a surgical blade. In circumstances during which the cornea is grossly edematous, markedly distorted by a stellate laceration with multiple sutures, or broken with tissue loss requiring a patch graft, vitreoretinal surgery can be performed with a brief keratoprosthesis or with endoscopic visualization. The first short-term keratoprosthesis, the Landers�Foulks system, is a transparent cylindrical polymethylmethacrylate lens that fits into a trephinated corneal bed and permits glorious visualization of the vitreous and retina with out an additional contact lens. Our choice is the Eckardt momentary keratoprosthesis,119 which is made of clear silicone rubber and has regular magnification and a short optical cylinder, permitting visualization for anterior vitreoretinal dissections, in addition to posterior phase pathology. In a collection of eleven traumatized eyes surgically rehabilitated with the aid of an Eckardt keratoprosthesis, five (45%) obtained a visible acuity of 20/400 or higher. However, functional outcomes are often disappointing, typically due to graft failure and hypotony from ciliary physique dysfunction. Disadvantages of endoscopy embrace the need for specialized tools, necessary extra surgery for corneal transplantation, and a steep studying curve. No potential controlled research has evaluated the efficacy of vitrectomy in penetrating ocular damage. The frequency of obtaining useful visible acuity of 5/200 or better ranged from 52% to 78%. In a more recent retrospective series of 36 eyes treated with immediate vitrectomy and silicone oil endotamponade for coexisting penetrating harm and retinal detachment, ambulatory imaginative and prescient was achieved postoperatively in 64%. Patients were more than likely to attain ambulatory imaginative and prescient if they offered preoperatively with ambulatory vision and without macular detachment. However, the preliminary diagnosis of posttraumatic endophthalmitis can be tough because the appreciable postoperative irritation and pain that commonly happen in these eyes can obscure infectious endophthalmitis. Delay in diagnosis, compounded by the virulent micro organism involved in these cases, makes the prognosis for recovery particularly grim. In one retrospective investigation, threat factors for endophthalmitis after penetrating ocular trauma were subjected to univariate and multivariate evaluation. Only lens rupture was independently significant for the development of endophthalmitis, carrying a relative threat of infection of 15. In a more modern comparative cohort examine, patients creating posttraumatic endophthalmitis had been ascertained prospectively and compared with historical controls of sufferers with open-globe harm. Delay in primary repair, ruptured lens capsule, and dirty wound have been each independently related to the development of posttraumatic endophthalmitis. Three more modern sequence have reported decrease charges of endophthalmitis, and the authors attributed this discount in part to the systematic use of antibiotics. Cultures of the aqueous and vitreous are obtained, any retained overseas body is eliminated, and antibiotic therapy is run. Cultures should embrace blood agar, chocolate agar, thioglycolate broth incubated at 37�C for micro organism, and Sabouraud agar incubated at 25�C for fungi. Gram stains also wants to be obtained and should provide useful information for antibiotic selection. We advocate antibiotic delivery through systemic, subconjunctival, intraocular, and topical routes. We favor a third- or fourthgeneration fluoroquinolone (levofloxacin 500�750 mg or moxifloxacin four hundred mg daily for 7 days) because of its broad coverage of common pathogens and its glorious vitreous penetration following intravenous or oral administration. Intraocular antibiotics in cases of suspected endophthalmitis ought to goal a broad vary of gram-positive and gramnegative organisms, and intraocular toxicity must be negligible. Vancomycin is lively against gram-positive bacteria, is bactericidal, not often promotes resistance, and is nicely tolerated by the eye in efficacious dosages (1. Prophylactic intraocular injection of antibiotics to stop endophthalmitis in sufferers with penetrating injury is controversial. In a prospective study of eyes with penetrating harm, sufferers had been randomized to receive both intraocular injection of antibiotics (40 �g of gentamicin sulfate and forty five �g of clindamycin sulfate) or balanced saline answer. The price of endophthalmitis within 2 weeks was significantly decrease within the group treated with antibiotics (2. Diagnosis of cataract at presentation can be difficult, as fibrin within the anterior chamber virtually instantly after the harm can simultaneously obscure visualization of the lens and provides the looks of a cataract. In such settings, we not often carry out a lensectomy on the time of restore of the corneal laceration. In some instances, nevertheless, a lease can be recognized in the anterior lens capsule accompanying an opacified lens. It is on this situation that cataract extraction at the time of major repair of the laceration may be thought of to reduce the possibility of postoperative inflammation and infection. After deciding to carry out a major lensectomy, the surgeon ought to first restore the laceration using the methods and rules described earlier in this chapter. One should then determine whether or not the cataract extraction could be performed through a limbal incision or via the pars plana.
Atorlip-10 10 mg order on line
Numerous sea fans have been apparent cholesterol lowering foods livestrong 10 mg atorlip-10 buy otc, and a glucose tolerance check and hemoglobin and serum protein electrophoresis research have been adverse reduce cholesterol by food 10 mg atorlip-10 cheap mastercard. Levielle and Morse48 described a affected person with continual myelogenous leukemia who had a comparatively low (33. In general, the blood viscosity begins to improve remarkably only with white blood cell counts of >50 �109/L. The affected person developed bilateral rubeosis, and after aggressive laser and vitrectomy, her vision declined to 20/200 bilaterally as a end result of macular ischemia. The accelerated course of diabetic retinopathy correlated most carefully with the anemia accompanying her leukemia and its treatment. They described progression of the neovascularization brought on by the additive effects of radiation retinopathy and chemotherapy, leading to macular traction detachment. The authors postulated that poisonous results of chemotherapy when mixed with radiation therapy might result in a extra severe form of ischemic retinal vasculopathy than would be encountered with acute lymphocytic leukemia alone. Although generally related to severe leukocytosis, white-centered hemorrhages could also be present regardless of the degree of leukocytosis. We have prospectively correlated the ocular findings with hematologic values on presentation in our series of one hundred twenty cases examined within a few days of analysis. In addition, there was also a statistical distinction between hematocrits (a mean of 20. We consider that the platelet depend plays a much stronger position in determining the presence or absence of intraretinal hemorrhage. The presence of specific retinal manifestations of leukemic retinopathy and the following danger of developing an intracranial hemorrhage was reported by Jackson et al. No elevated threat of intracranial hemorrhage existed with the presence of non-macular intraretinal hemorrhages, white-centered hemorrhages, or cotton-wool spots. Therefore, patients with macular hemorrhages might require close monitoring for the potential improvement of intracranial hemorrhages, and these patients may need platelet transfusions if such an intracranial hemorrhage happens. Patients with cotton-wool spots were eight times extra more likely to die within the follow-up interval than sufferers without this discovering, possibly due to extreme bone marrow dysfunction. The prognostic significance of leukemic retinopathy in childhood leukemia was evaluated in sixty three sufferers by Ohkoshi and Tsiaras. These two research recommend that sufferers with scientific leukemic retinopathy might have more aggressive systemic disease which may lead to a worse prognosis. Opportunistic Infections Opportunistic infections are frequent in immunosuppressed patients. Rather, systemic chemotherapy is run in an try to control the underlying systemic drawback. Varying doses have been used,1 and consultation with an skilled radiation oncologist is crucial. The sufferers had peripheral white blood cell counts of 129, 379, and 1 043 �109/L, respectively. In addition, the authors cite a number of different circumstances by which the process has been used successfully. In addition, malignant lymphomas are divided into primary intraocular lymphoma and secondary intraocular lymphoma. Primary intraocular lymphoma includes major central nervous system lymphoma, whereas secondary intraocular lymphoma entails a metastasis from a major visceral lymphoma. The incidence of neoplastic intraocular involvement in patients with lymphomas is probably much less than that in patients with various leukemias. They are predominantly of B-cell lymphocytic origin, though some could additionally be derived from T cells. In the past decade there was a gradual improve within the frequency of reviews of major intraocular lymphomas. Retinal hemorrhages and cotton-wool spots associated to anemia or thrombocytopenia are common in patients with non-Hodgkin lymphoma, but direct retinal involvement in sufferers with systemic lymphoma is extraordinarily rare. The patient was treated with 3000 cGy of exterior beam radiation, and a partial response occurred. The authors believed that the more than likely cause was lymphomatous infiltration, though no pathologic examination was carried out. Lymphoma cells are sometimes 2�4 occasions the size of normal lymphocytes and display high nuclear/cytoplasmic ratios, prominent nucleoli, nuclear pleomorphism, and coarse chromatin patterns. Neuroimaging has been shown to have a low sensitivity for differentiating intraocular lymphoma from uveitis or melanoma. The paraneoplastic syndrome of bilateral diffuse uveal melanocytic proliferation has been reported in the single case of a patient with non-Hodgkin systemic lymphoma. The disease is characterised by painless swelling of the lymph nodes, and Reed�Sternberg cells are seen on histopathologic examination. Patients with "numerous white deposits within the retinal periphery," chorioretinitis, Roth spots, and perivascular retinitis have been reported. A vitrectomy specimen demonstrated solely acute and chronic inflammatory cells, and no tumor cells have been seen. Toxoplasmic uveitis and chorioretinitis,133 Nocardia infection,134 and just about all viral infections of the herpes household have been beforehand reported. In the past few years, ophthalmologists have employed the utilization of intravitreal injection of chemotherapeutic agents as an alternative choice to exterior beam radiation of the attention. Reports have demonstrated profitable use of intravitreal methotrexate and rituximab. There are three levels of the illness: (1) a chronic section of premycotic/eczematous skin lesions; (2) a section characterised by infiltrative plaque lesions; and (3) a last section of frank cutaneous tumor. Most affected people develop the disease in the fifth decade of life, and a lot of die of unrelated causes before widespread involvement. Mycosis fungoides entails the attention in up to one-third of individuals and tends to contain the external eye and adnexa rather more generally than the intraocular constructions. The disc swelling was in all probability related to papilledema as a result of lethargy, confusion, and focal neurologic indicators had been noticed. On histopathologic examination, atypical cells and lymphocytes, in addition to polymorphonuclear cells, were seen within the vitreous. Similar atypical cells infiltrated the retina, and a perivascular lymphocytic infiltrate was noted. Rossi reported on a patient with bilateral papilledema, venous stasis, retinal edema, and retinal hemorrhages. A 16-year-old lady who died of visceral mycosis fungoides had no mild perception in either eye or bilateral disc swelling. The largest sequence of sufferers with mycosis fungoides reported within the ophthalmic literature is that of Stenson and Ramsay. Note disc hyperfluorescence, perivascular staining, and foci of hyperfluorescence on the stage of the retinal pigment epithelium. Burkitt lymphoma is the most common childhood tumor in Africa, but it occurs solely not often in the United States.
Atorlip-10 10 mg buy generic online
Rates of local management metastasis and general survival in patients with posterior uveal melanomas handled with ruthenium-106 plaques cholesterol test in pharmacy atorlip-10 10 mg discount line. Results following episcleral ruthenium plaque radiotherapy for posterior uveal melanoma cholesterol in eggs bodybuilding buy atorlip-10 10 mg amex. Survival of patients and metastatic and native recurrent tumor growth in malignant melanoma of the uvea after ruthenium plaque radiotherapy. Tumor regression after brachytherapy for choroidal melanoma: reduction of thickness and cross-sectional space by shape and regression pattern. Post-irradiation regression of choroidal melanomas as a risk issue for demise from metastatic. Relationship between fee of posterior uveal melanoma flattening following plaque radiotherapy and gene expression profile class of tumor cells. Plaque radiotherapy for juxtapapillary choroidal melanoma: visible acuity and survival end result. Metastatic risk for distinct patterns of post-irradiation native recurrence of posterior uveal melanoma. Malignant melanomas of the human uvea: 25-year follow-up of cases in Denmark, 1943�1952. Uveal melanoma in Finland: an epidemiological, medical, histological, and prognostic examine. Uveal melanoma: therapeutic consequences of doubling instances and irradiation results; a evaluation. Helium ions versus iodine125 brachytherapy within the administration of uveal melanoma: a potential, randomized, dynamically balanced trial. Anterior phase problems after helium ion radiation therapy for uveal melanoma: radiation cataract. Radiation related problems after ruthenium plaque radiotherapy of uveal melanoma. Vision following helium ion radiotherapy of uveal melanoma: a northern California Oncology group study. Visual operate following enucleation or episcleral plaque radiotherapy for posterior uveal melanoma. The dimension and form of malignant melanomas of the choroid and ciliary body in relation to prognosis and histologic traits: a statistical study of 210 tumors. The position of orbital exenteration in choroidal melanoma with extrascleral extension. Identification of chromosomes 3, 6, and eight aberrations in uveal melanoma by microsatellite analysis compared to comparative genomic hybridization. Abnormalities of chromosomes three and eight in posterior uveal melanoma correlate with prognosis. Cytogenetic findings in six posterior uveal melanomas: involvement of chromosomes three, 6, and 8. Correlation of cytogenetic abnormalities with the result of sufferers with uveal melanoma. Monosomy three in uveal melanoma: correlation with medical and histologic predictors of survival. Gene expression profiling in uveal melanoma reveals two molecular lessons and predicts metastatic death. Fluorescent in situ hybridization of for monosomy three by way of 30-gauge fine needle aspiration biopsy of choroidal melanoma in vivo. Small choroidal melanoma with chromosome three monosomy on fantastic needle aspiration biopsy. Variable results for uveal melanoma-specific gene expression profile prognostic take a look at in choroidal metastasis. Age, survival predictors, and metastatic death in sufferers with choroidal melanoma: tentative proof of a therapeutic impact on survival. Genotypic profiling of 452 choroidal melanomas with multiplex ligation-dependent probe amplification. American Joint Committee on Cancer Classification of Uveal Melanoma (Anatomic Stage) predicts prognosis in 7,731 patients: the 2013 Zimmerman Lecture. The prognostic impact of American Joint Committee on Cancer staging and genetic standing in sufferers with choroidal and ciliary physique melanoma. Microvascular loops and networks as prognostic indicators in choroidal and ciliary body melanomas. Comparison of the prognostic worth of fibrovascular loops, mean of the ten largest nucleoli, cell kind, and tumor size. Microcirculation and tumor-infiltrating macrophages in choroidal and ciliary body melanoma and corresponding metastases. Genetic Testing in Clinical Trials Diagnosis and Treatment of Current Uveal Melanoma Patients Conclusion which uveal melanocytes elude their antiproliferative and proapoptotic harnesses to form a melanoma, and in up to half of patients, metastasize hematogenously to the liver and different organs. It is equally essential that sufferers not in danger for metastasis are spared from unnecessary therapy with systemic chemotherapy with their attendant risks and side-effects. Here, we offer an overview of how our current understanding of the molecular genetics of choroidal melanoma has supplied insight into the pathogenesis of this devastating ocular most cancers, and how it could influence the analysis, remedy, and survival of these sufferers. Iris melanomas are relatively benign; nonetheless, ciliary body and choroidal melanomas still present important diagnostic and therapeutic challenges. Metastases mostly goal the liver, and the detection of hepatic metastatic lesions predicts a dismal outcome, with a median survival of only some months. Mutations in genes encoding for heterotrimeric G-protein subunits have been reported in a big selection of cancers. Gain of chromosome 6p happens mainly in nonmetastasizing tumors and carries a greater prognosis. Conversely, lack of one copy of chromosome three (monosomy 3) happens most regularly in metastasizing tumors and predicts a poor consequence. This observation has prompted efforts to use this unique molecular distinction to predict which sufferers are at greater risk for later developing metastases. However, this technique requires highly educated cytogeneticists, and the accuracy of the outcomes is restricted by sampling error attributable to evaluation of just a few tumor cells, and to the shortcoming to detect small genetic modifications. The prognostic accuracy of those methods in contrast with standard karyotyping is unclear. This know-how not solely permits comparison of gene profiles in regular and pathologic tissues or cells, but additionally among totally different levels of disease development, and has confirmed to be notably helpful in finding out most cancers. At this stage, the melanoma chooses considered one of two mutually unique paths, acquire of chromosome 6p or loss of chromosome 3, resulting in the development of less aggressive (lower metastatic rate) or extra aggressive (higher metastatic rate) tumors, respectively. The further loss of 8p in the more aggressive tumors further increases the chance for metastasis. A subset of gene markers can then be recognized and used as a "prognosis classifier" that can assist predict the later look ("poor prognosis") or absence ("good prognosis") of clinical metastasis. The two lessons have further been subdivided into four prognostically significant subclasses (1A, 1B, 2A and 2B), based on gene-expression profiling. The subclass 1B signature corresponds carefully to gain of chromosome 6p, and the subclass 2B signature corresponds carefully to loss of chromosome 8p.
Atorlip-10 10 mg line
Shields and Shields average cholesterol test buy atorlip-10 10 mg on line,24 who list astrocytic hamartoma within the differential analysis of retinoblastoma lowering cholesterol best foods atorlip-10 10 mg order on line, affirm the rarity of a mistaken prognosis in their very own series. Of the 136 sufferers sent to their clinic with the prognosis of possible retinoblastoma, only one patient had an astrocytic hamartoma. Other issues that can mimic astrocytic hamartoma embrace myelinated nerve fibers and inflammatory lesions. However, optic disc drusen lie within the disc, whereas astrocytic hamartomas protrude above it54 and obscure both the optic nerve and retinal blood vessels. Gliomas of the optic disc could initially appear with disc swelling or obscuration of the disc by a whitish, protuberant mass. These lesions may be simply confused with astrocytic hamartomas, especially within the case of a noncalcified hamartoma. Although more generally described in neurofibromatosis, Shields and Shields24 notice that optic disc glioma can also seem in patients with tuberous sclerosis. Other neoplastic lesions of the optic disc must be considered within the differential prognosis, including capillary and cavernous hemangioma. They are inclined to current with extra hypomelanotic pores and skin macules and learning disabilities with more frequent neurologic and ophthalmologic signs, renal cysts, and ungual fibromas. Selerose tubereuse des circonvolutions cerebrales: idiotie et epilepsie hemiplegique. Spontaneous regression of retinal astrocytic hamartoma in a affected person with tuberous sclerosis. Fluorescein angiography: an aid within the differential analysis of intraocular tumors. Atypical retinitis proliferans, retinal telangiectasis, and vitreous hemorrhage in a patient with tuberous sclerosis. Astrocytic hamartoma in tuberous sclerosis mimicking necrotizing retinochoroiditis. Vitreous seeding by retinal astrocytic hamartoma in a patient with tuberous sclerosis. Spontaneous regression of parafoveal exudates and serous retinal detachment in a patient with tuberous sclerosis and retinal astrocytoma. Learning incapacity and epilepsy in an epidemiological sample of individuals with tuberous sclerosis complicated. Tuberous sclerosis: particular reference to the microscopic alterations within the cutaneous hamartomas. Renal angiomyolipoma related to tuberous sclerosis: evaluate of the literature. Linkage investigation of three putative tuberous sclerosis determining loci on chromosome 9q, 11q, and 12q. Identification and characterization of the tuberous sclerosis gene on chromosome sixteen. Shields Introduction Definition of Hamartia, Hamartoma, Chorista, Choristoma Neurofibromatosis (Von Recklinghausen Syndrome) Encephalofacial Hemangiomatosis (Sturge�Weber Syndrome) Racemose Hemangiomatosis (Wyburn-Mason Syndrome) Retinal Cavernous Hemangiomatosis Organoid Nevus Syndrome Phacomatosis Pigmentovascularis Oculodermal Melanocytosis Other Phakomatoses Combined Systemic Hamartomatoses Conclusion been categorized with these traditional oculoneurocutaneous syndromes. Examples of hamartomas embody the retinal hemangioblastoma (capillary hemangioma) that happens from already current vascular tissue within the retina in von Hippel�Lindau syndrome, or the cutaneous peripheral nerve tumors that happen from the already present neural tissue throughout the pores and skin in sufferers with neurofibromatosis. Most phakomatoses display an autosomal dominant mode of inheritance, usually with incomplete penetrance. They are normally stationary or slowly progressive lesions that generally lack the capacity for limitless proliferation found with cancers. Renal cell carcinoma occurs with greater frequency in sufferers with von Hippel�Lindau disease. Patients with the phakomatoses might solely manifest a few of the medical options of a specific syndrome and that is referred to as a "forme fruste. Variable medical manifestations of these syndromes are acknowledged, and complete care of the affected person often entails coordination of a quantity of specialists, together with neurologists, dermatologists, ophthalmologists, and oncologists. The term "phakoma" was first utilized by Van der Hoeve in 1932 to point out a mother spot, or birthmark, a attribute finding in plenty of of those entities. Later, encephalofacial hemangiomatosis (Sturge�Weber syndrome), racemose angiomatosis (Wyburn-Mason syndrome), and cavernous hemangioma of the retina with cutaneous and central nervous system involvement had been included with these situations. More recently, different entities such as organoid nevus syndrome, oculodermal melanocytosis, and phacomatosis pigmentovascularis have 2446 Phakomatoses 2447 be seen in sufferers with tuberous sclerosis advanced or encephalofacial hemangiomatosis. In other chapters in the book, the conditions of tuberous sclerosis complex (Bourneville syndrome) and retinocerebellar hemangiomatosis (von Hippel�Lindau syndrome) have been described. These phakomatoses embody neurofibromatosis (von Recklinghausen syndrome), encephalofacial hemangiomatosis (Sturge�Weber syndrome), retinal racemose hemangiomatosis (Wyburn-Mason syndrome), retinal cavernous hemangiomatosis, organoid nevus syndrome (Solomon syndrome), phacomatosis pigmentovascularis (Cesioflammea type), and oculodermal melanocytosis (nevus of Ota). Because this e-book covers primarily diseases of the ocular fundus, most emphasis is placed on retinal and choroidal manifestations. Caf�-au-lait 6caf�-au-laitspotslargerthan 5mmdiameterinprepubertal children(<10years) or 6caf�-au-laitspotslargerthan 15mmindiameterin postpubertalindividuals(adults) Crowesign 2typicalneurofibroma or 1plexiformneurofibroma 2lesions Sphenoiddysplasia or Longboneabnormalities(cortex thinningorpseudoarthrosis) Parent,siblingoroffspring 136 2. About one-half of the cases happen initially as spontaneous mutations with a negative household history. Type 1 is recognized as peripheral neurofibromatosis or von Recklinghausen syndrome, whereas sort 2 known as central or bilateral acoustic neurofibromatosis. Type 1 neurofibromatosis is characterized by peripheral and cutaneous manifestations and is related to an abnormality on chromosome 17. The diagnostic analysis and multidisciplinary administration of neurofibromatosis 1 and neurofibromatosis 2. This extremely penetrant phenotype has a broad variety of manifestations and may range within households. Ophthalmologic Features Neurofibromatosis has probably the most diversified ocular findings among the phakomatoses. Nodular neurofibroma seems as a solitary or multifocal painless, smooth-surfaced, and well-defined mass, often the dimensions of a pea, and without shade change. Plexiform neurofibroma presents as a diffuse thickening of the eyelid that may produce the typical S-shaped curvature to the eyelid, a discovering highly characteristic of neurofibromatosis. Patients with neurofibromatosis have an elevated incidence of congenital glaucoma, which can be secondary to a number of mechanisms. Multiple iris hamartomas, known as Lisch nodules, are the commonest uveal abnormality of neurofibromatosis kind 1. Histopathologically, iris Lisch nodules are hamartomas composed of aggregates of melanocytes on the anterior border layer of the iris. The choroidal findings in patients with neurofibromatosis type 1 embrace unifocal or multifocal choroidal nevus, diffuse plexiform neurofibroma, neurilemoma, and melanoma. Multiple bilateral, choroidal nevi are highly suggestive of neurofibromatosis kind 1. They could be best seen with nearinfrared reflectance imaging or multispectral imaging with lengthy wavelength. Choroidal neurilemoma (schwannoma) is a rare discovering and manifests as a circumscribed, amelanotic elevated tumor. There appears to be the next incidence of uveal melanoma in sufferers with neurofibromatosis.
Black Root. Atorlip-10.
- Are there safety concerns?
- Dosing considerations for Black Root.
- What is Black Root?
- Are there any interactions with medications?
- Constipation, liver and gallbladder problems, causing vomiting, and other conditions.
- How does Black Root work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96774
Atorlip-10 10 mg mastercard
The choroidal neovascularization seems similar to cholesterol in shrimp and crab atorlip-10 10 mg buy discount the choroidal neovascularization that develops in macular degenerative conditions cholesterol levels us vs canada order 10 mg atorlip-10 free shipping. Melanocytes, composing the nevi, share a neural crest origin with the other tumors present in von Recklinghausen disease (neurocristopathies). Clinically, a dysplastic nevus have to be suspected if a melanocytic nevus harbors at least two of the next four features:1,106,107 (1) ill-defined or irregular borders; (2) irregular pigmentation; (3) accentuated skin markings; and (4) large dimension (>5 mm). Histopathologically, dysplastic nevi are divided into two sorts: (1) a gentle sort with aberrant differentiation. They often have a surrounding pigmented or nonpigmented halo or a double halo consisting of pigmented and nonpigmented rings. While small melanocytic lesions categorised as choroidal nevi may show gradual, limited growth, especially in a younger affected person,9 the rapid growth of an indeterminate lesion (large nevus versus small melanoma) is generally the determining think about reclassifying the lesion as a melanoma and considering remedy. In addition to the circumstances discussed within the following paragraphs, materials on the differential diagnoses of choroidal nevi can be discovered within the following chapters: Chapter one hundred forty, Congenital hypertrophy of the retinal pigment epithelium; Chapter 141, Combined hamartoma of the retinal pigment epithelium and retina; Chapter 155, Choroidal metastases; Chapter 157, Circumscribed choroidal hemangioma, and in the sections inspecting choroidal melanomas, see Chapter 148, Enucleation for choroidal melanomas. This is extra reliable than descriptions about shape or size; nevertheless, slight misalignment of the axis of the fundus camera can filter the pigmented edges of melanocytic tumors, resulting in an misguided analysis of development or malignant transformation, with subsequent pointless therapy. Wolff-Korman and colleagues detected a pulsatile blood move on the tumor base of sixty two choroidal melanomas where no Doppler signals have been elicited in a collection of 18 choroidal nevi. Choroidal melanomas might show irregular vascular patterns similar to dilation, tortuosity, vascular loops, and branching;121 delayed maximal fluorescence;122 and marginal late dye leakage. This approach may be capable of additional detecting microvascular patterns predictive of growth. Retinal edema, photoreceptor attenuation, and drusen recommend chronicity, whereas subretinal fluid with out retinal atrophy may suggest a more active lesion. Subretinal fluid is hyperfluorescent with the peripheral rim of fluid being barely more hyperfluorescent. Due to the normal restricted, gradual progress of benign nevi, a particular distinction between a nevus and a small melanoma may be problematic. If growth signifies that the lesion is a melanoma, then the treatment is for a malignancy. The treatment of serous macular detachment secondary to choroidal melanoma and nevi. Epidemiologic investigation of elevated incidence of choroidal melanoma in a single inhabitants of chemical staff. Ophthalmologic oncology: conjunctival malignant melanoma in affiliation with sporadic dysplastic nevus syndrome. Poster introduced at: American Academy of Ophthalmology meeting, October, 2004; New Orleans, Louisiana. Diffuse choroidal melanocytoma simulating melanoma in a child with ocular melanocytosis. Pupillary and visual area analysis in patients with melanocytoma of the optic disc. Orbital malignant melanoma and oculodermal melanocytosis: report of two instances and review of the literature. Ocular melanocytosis: a research to determine the prevalence rate of ocular melanocytosis. Association of ocular and oculodermal melanocytosis with the rate of uveal melanoma metastasis: analysis of 7872 consecutive eyes. Metastasis from uveal melanoma associated with congenital ocular melanocytosis: a matched study. Primary malignant melanoma of the central nervous syndrome: pineal involvement in a patient with nevus of Ota and a number of pigmented pores and skin nevi. Melanosis oculodermica, melanoblastosis leptomeninges y melanoma intracerebral primario. Prevalence and traits of choroidal nevi: the multi-ethnic research of atherosclerosis. Clinical spectrum of choroidal nevi primarily based on age at presentation in 3422 consecutive eyes. The association between host susceptibility components and uveal melanoma: a meta-analysis. Combination of scientific elements predictive of progress of small choroidal melanocytic tumors. Malignant melanoma of the human uvea: current follow-up of circumstances in Denmark, 1943�1952. An ultrastructural examine of melanocytomas (magnocellular nevi) of the optic disc and uvea. Ocular abnormalities related to cutaneous melanoma and vitiligo-like leukoderma. Microcirculation structure of melanocytic nevi and malignant melanoma of the ciliary body and choroid: a comparative histopathologic and ultrastructural examine. The nature of the orange pigment over a choroidal melanoma: histochemical and electron microscopical observations. Disciform lesions overlying melanocytoma simulating development of choroidal melanoma. Choroidal nevus with subretinal pigment epithelial neovascular membrane and a optimistic P-32 take a look at. Bilateral metastatic choroidal melanoma, nevi and cavernous degeneration of the optic nerve head. Histogenesis of malignant melanomas of the uvea: prevalence of nevus-like constructions in experimental choroidal tumors. Bilateral diffuse melanocytic uveal tumors related to systemic malignant neoplasms: a lately acknowledged syndrome. Choroidal (sub-retinal) neovascularization secondary to choroidal nevus and profitable remedy with argon laser photocoagulation: case report and evaluation of the literature. Relationship of congenital ocular melanocytosis and neurofibromatosis to uveal melanomas. False positive magnetic resonance imaging of choroidal nevus simulating a choroidal melanoma. Cytogenetics in hereditary malignant melanoma and dysplastic nevus syndrome: is dysplastic nevus syndrome a chromosome instability dysfunction The dysplastic nevus syndrome: a pedigree with major malignant melanoma of the choroid and pores and skin. Bilateral melanocytic uveal tumors related to systemic nodular malignancy: malignant melanomas or benign paraneoplastic syndrome. Observations of suspected choroidal and ciliary physique melanomas for proof of progress prior to enucleation.
Atorlip-10 10 mg cheap visa
Typically cholesterol test walgreens atorlip-10 10 mg discount on line, the recurrent retinal detachment is shallow and positioned inferiorly cholesterol amount in shrimp 10 mg atorlip-10 for sale, where the silicone bubble may not be completely in contact with the retina. Peeling is facilitated through the use of perfluorocarbon, which acts as a "third" hurt, offering posterior stabilization to the membranes being peeled. Once the retina is absolutely reattached under perfluorocarbon, the perimeters of the tears are handled by photocoagulation. Cryotherapy ought to be averted, as it enhances breakdown of the blood�ocular barrier and can improve postoperative irritation. It is also thought to restrict the buildup of proinflammatory cytokines in the vitreous cavity. In all circumstances a scleral buckle was used to provide peripheral assist within the area of drainage. If the macula is threatened or indifferent in a watch with beforehand good vision, then reoperation may be warranted. Often, drainage of subretinal fluid combined with injection of more silicone with extra photocoagulation is the treatment of choice. If visualization is poor, the oil should be removed and the retina reattached, as described above, earlier than the oil is reinjected. Lensectomy may be essential, ideally with the implantation of an intraocular lens, sustaining the posterior capsule. Later capsular opacification is widespread, nevertheless, and one should contemplate primary capsulotomy in selected circumstances. Looking on the nerve to avoid a pulsatile perfusion at the onset of surgery, and periodically during surgery, can keep away from further loss of imaginative and prescient from prolonged retina anoxia. A lens extraction is required in practically all cases to expose the full extent of the vitreous base so that every one condensed vitreous and vitreous traction could be eradicated. Posterior epiretinal membranes overlying healthy retina are identified and removed with choose and forceps. Once the posterior wholesome retina is freed from membranes, perfluorocarbon is used to tamponade this retina out to the sting of atrophic retina. As this is nonfunctional retinal tissue, it has no physiologic operate and may greatest be removed. Larger vessels, even though these are attenuated, must be treated with diathermy as they might bleed. This could result in a 360� retinotomy leaving a fairly central space of viable, healthy retina. Once the vitreous, preretinal membranes, and indifferent atrophic retina have been removed, remaining retinal breaks are recognized and marked with endodiathermy. Under perfluorocarbon the sting between healthy and any remaining atrophic retina, in addition to the free edge that was created earlier, are handled by endophotocoagulation, inserting a quantity of rows of laser alongside the sting of healthy retina. If peripheral support is critical, particularly inferiorly, an encircling band or a whole scleral buckle could be placed. The oil ought to be ideally eliminated in 3�6 months to keep away from long-term problems related to its presence. Removal ought to be thought of provided that the chance of redetachment is believed to be minimal. In addition in these conditions, the surgery ought to be carried out as much as potential with a low intraocular strain, because the circulation via the optic nerve may be occluded at even commonplace infusion pressures. Reducing these molecules can enhance the prognosis and implies a concerted local and systemic effort to decrease intraocular irritation. It is best achieved as a team effort between the vitreoretinal surgeon and the uveitis specialist. A multidisciplinary method is most probably to present the optimum outcome in most settings. While in the past, visible results after surgical procedure were comparatively poor, the advent of better gear, less traumatic surgical approaches, and a greater understanding of the pathophysiologic processes at hand have improved each short-term and long-term outcomes. Both timing and extent of surgery are critical issues, which range relying on the etiology. Larger series obtained by combining results from several completely different centers will assist to outline extra exactly these parameters in years to come. The epidemiology of rhegmatogenous retinal detachment: geographical variation and scientific associations. Vitreous intercellular adhesion molecule 1 in uveitis difficult by retinal detachment. Cytokines, chemokines and soluble adhesion molecules in aqueous humor of children with uveitis. Risk components for growth of rhegmatogenous retinal detachment in patients with cytomegalovirus retinitis. Retinal detachment in cytomegalovirus retinitis: intravenous versus intravitreal remedy. The epidemiology and socioeconomic associations of retinal detachment in Scotland: a two-year prospective population-based examine. Course of cytomegalovirus retinitis within the era of extremely energetic antiretroviral remedy: five-year outcomes. Prevalence, clinical features, and causes of imaginative and prescient loss amongst sufferers with ocular toxocariasis. Retinal pigment epithelial detachment: an unusual presentation of ocular sarcoidosis. Necrotizing retinopathy simulating acute retinal necrosis causing rhegmatogenous retinal detachment in sarcoidosis: a case report. Retinal detachment due to a macular gap in a patient with Beh�et illness treated with vitrectomy and silicone oil tamponade. Differential expression of inwardly rectifying K+ channels and aquaporins 4 and 5 in autoimmune uveitis indicates misbalance in M�ller glial cell-dependent ion and water homeostasis. Evidence of cross-link formation of vitreous collagen throughout experimental ocular 30. Rhegmatogenous retinal detachment difficult by extreme intraocular inflammation, hypotony, and choroidal detachment. Randomized clinical trial of cryotherapy versus laser photocoagulation for retinopexy in typical retinal detachment surgery. Silicone oil within the surgical therapy of endophthalmitis associated with retinal detachment. Laser photocoagulation restore of macula-sparing cytomegalovirus-related retinal detachment. Repair of retinal detachment caused by cytomegalovirus retinitis in sufferers with the acquired immunodeficiency syndrome. A masked prospective evaluation of consequence parameters for cytomegalovirus-related retinal detachment surgical procedure in patients with acquired immune deficiency syndrome. Treatment of retinal detachments in sufferers with the acquired immune deficiency syndrome.
Atorlip-10 10 mg on line
Tasks are common to the surgical method to completely different illness states that share widespread pathoanatomic configurations egg cholesterol chart generic atorlip-10 10 mg without a prescription. The choice course of requires end result information cholesterol in raw shrimp purchase atorlip-10 10 mg without prescription, knowledge of physical ideas, particular person affected person components, and experiential info. This article will begin with an outline of related common pathoanatomy, with particular info left to other chapters on specific illness states. Understanding the mechanics of the instruments used will allow dialogue of the main points of the means to perform each task. The chapter concludes with a instructed algorithm for each common disease state, with particular administration particulars once more left to different authors. In the traditional state, the outer floor of the vitreous is in touch with the retina, pars plana, and ciliary physique in a roughly spherical form with an anterior side abutting the lens. A detailed understanding of the irregular vitreoretinal interface and its derivative geometry is requisite to endeavor vitreoretinal surgical procedure. The task entails visualization of vitreous structures and a systematic seek for membranes based mostly on observed retinal topology. In common, membranes are white and matte-finish, whereas the retina has a reflective surface luster and appears pale yellow. Shear Shear slicing happens when drive is applied alongside two opposing right-angle edges transferring previous each other and forced towards one another. Fatigue Failure Fatigue failure happens when repetitive movement, elongation, and compression weaken tissue structure and cause failure. Ultrasonic cavitation (fragmentation, phacoemulsification) is an example of this mode of slicing. Gravity-fed infusion methods were simplistic and will solely trigger low intraocular strain if the bottle was too low or the infusion fluid was depleted. There are many causes of excessively low intraocular strain throughout vitrectomy, every of which shall be discussed. Peeling Force along the axis of a collagen fiber bundle causes nonelastic collagen fibers to barely stretch and in the end to fail. Damage to attached structures is a perform of the variety of fibers and the power of the attachment and the substrate. Membrane peeling requires drive preferably tangential to the retina, which causes failure of the attachment on the vitreoretinal interface by elongation. For this purpose, membrane peeling could additionally be inappropriate in diabetic traction retinal detachment instances. Sutureless 25G vitrectomy initially utilized straight-in trocar cannula trajectories to produce sclerotomies perpendicular to the sclera. When 23G, sutureless surgical procedure was introduced subsequently, oblique trocar-cannula entry was utilized so as to construct a scleral tunnel to scale back wound leakage. Initially, surgeons used a two-plane method; the initial trocar-cannula insertion segment was roughly 30� relative to the sclera and the second segment trajectory perpendicular to the sclera. More just lately, surgeons using both 23G and 25G systems have switched to oblique entry in order to create an extended scleral tunnel;1�3 unfortunately some surgeons use excessively steep angles (~10�). A single plane, 30� trajectory is better compromise between the benefits of a protracted scleral tunnel and the catastrophe of suprachoroidal infusion. Inspecting the infusion cannula with the operating microscope after insertion and earlier than initiating infusion was standard apply with sutured 20G vitrectomy. It is best practice to insert the infusion port within the cannula with the infusion running to prevent bubbles adopted by immediate inspection of the tip of the infusion cannula. The naked eye and endoilluminator present inadequate magnification to make the willpower that the cannula has penetrated the choroid and nonpigmented pars plana epithelium; microscope visualization is essential. Adhesively fastening the infusion cannula tubing and related stopcock(s) and connectors to the drape is crucial to Principles and Techniques of Vitreoretinal Surgery 1919 prevent traction on the infusion cannula and the eye. Unrecognized pulling on the tubing by the assistant or surgeon can easily trigger the cannula to partially pull out causing a suprachoroidal infusion. Adhesively fastening the infusion cannula tubing to the drape with eye in the main place with a short tubing loop can result in a suprachoroidal infusion when the attention is rotated to view the periphery creating pressure on the cannula. Scleral despair is one other cause of inadvertent suprachoroidal infusion by inflicting torque on the cannula as the attention is rotated by the depressor. In addition, scleral depression can drive blood clots, dense scar tissue, peripheral vitreous, or silicone oil into the infusion cannula and tubing, successfully plugging it, giving the misunderstanding of infusion system failure. Placing the infusion cannula too close to the lower lid quite than simply inferior to the horizontal meridian is a standard cause of suprachoroidal infusion created when the eye is rotated all the method down to visualize the inferior periphery and the cannula is rotated into the suprachoroidal house. Kinking of the more versatile silicone tubing terminal segment of the infusion cannula may be brought on by the surgeon or assistant accidentally pulling on the tubing. This drawback is exacerbated through the use of excessively low infusion pressure settings (10�25 mmHg) inadequate to straighten out the tubing kink. The writer has all the time used 45 mmHg besides when operating on youngsters or patients with very low systemic blood pressure, sometimes beneath basic anesthesia. Some surgeons have lately advocated utilizing infusion settings of 10�20 mmHg due to a completely unfounded perception that occult ischemia is widespread during vitrectomy. Using infusion settings of 10�20 mmHg causes miosis, bleeding, and corneal astigmatism from contact lens stress on the cornea and instrument forces on the sclerotomies as well as scleral infolding often mistakenly thought to be choroidals. Kinking is commonest when excessively low infusion stress settings are used and the tubing bends on the fluid�air stopcock/valve. If choroidals are current at the inception of surgical procedure, a 6-mm as a substitute of 4-mm cannula can be used and/or infusion initiated with a 25G needle as described above. Ideal tissue chopping is defined as that producing zero displacement of the tissue to be removed and no vitreoretinal traction. It is most secure to use the lowest suction drive sufficient to imbricate tissue or vitreous into the cutter port. In abstract, utilizing the best out there cutting price is normally the best approach for all tasks and all instances except all the vitreous has been removed first. Switching of valves, pumps, digital units, and lasers are ideally controlled by a single built-in system, with capabilities managed by the surgeon rather than the circulating nurse and even scrub tech. So-called heads-up surgical procedure, viewing surgery with a television-based system and flat panel display, considerably reduces resolution and dynamic range and presents no advantage. Ceiling-mounted microscopes are less mechanically stable than floor-mounted microscopes because of longer moment arms and inherent lack of ceiling rigidity. All energy and control sources for surgical tools must be integrated right into a single system for higher effectivity. Illumination, diathermy, and infusion are referred to as world functions and are at all times obtainable. Infusion is best managed by digital, sensor-based, pressurized infusion systems. They must be contoured quite than cylindrical to reduce the drive required to stop dropping and constrain grip at a constant place. They ought to be not than the gap from the fingertips to the purpose of contact with the hand. Shorter handles scale back the torque produced by the weight and scale back friction because the cables, fibers, and tubing used to connect surgical instruments slide on the drape.
Order atorlip-10 10 mg amex
A radial sclerotomy is performed parallel to the rectus muscle in the quadrant with the most suprachoroidal hemorrhage cholesterol ratio levels atorlip-10 10 mg purchase with visa. The infusion stress permits a controlled drainage of the liquefied blood via the sclerotomy cholesterol medication and knee pain purchase atorlip-10 10 mg overnight delivery. After a partial drainage, 23G cannulas are inserted into the eye by way of the pars plana and a limited vitrectomy is carried out followed by removing of the posterior hyaloid. Intraoperative hypotony is probably certainly one of the primary danger factors resulting in choroidal effusion with subsequent rupture of small arteries traversing the suprachoroidal area. In addition, extended hypotony may instantly result in rupture of the brief or long posterior ciliary arteries or vortex veins. The biggest danger for suprachoroidal hemorrhage throughout cataract surgical procedure happens immediately after nucleus removal, when the attention is at biggest danger of extended hypotony. While aspirating the cortex, the posterior capsule was ruptured with subsequent vitreous loss. One week after the original surgery, the affected person was introduced again to the working room for drainage of the suprachoroidal blood. Iris retractors have been positioned to have a greater visualization of the anterior chamber. It was noted that patient still had a big blood clot within the suprachoroidal space. A scleral cutdown was carried out superotemporally, and tissue plasminogen activator (0. An infusion cannula might now be placed through the pars plana into the vitreous cavity and vitrectomy was carried out. Systemic danger components embrace advanced age, hypertension, atherosclerosis, diabetes, and bleeding disorders. Air�fluid change was performed, and laser endophotocoagulation was applied across the break and the lattice degeneration inferiorly. Laser was applied across the bubble to stop its migration in course of the posterior pole. Further, the injection must be accomplished by the surgeon (rather than an assistant), and a protected distance from the floor of the retina should be stored through the injection procedure (one has the tendency to transfer closer to the floor of the retina in the course of the injection). The scleral buckle was then loosened significantly, and the same technique was attempted. We hypothesize that extreme cerclage impact of the encircling scleral buckle promoted posterior slippage which was resolved by loosening the buckle (Video 131. In this case, presumably there was the additional issue of excessive 360� of scleral buckle indentation. A "high" indentation could additionally be undesirable and, due to this fact, greatest avoided to decrease slippage. When the subretinal membrane is in the type of branching bands and the extent of the membrane may be visualized through the retina, the membrane could be eliminated using forceps handed by way of preexisting retinal breaks or small retinotomies. Intravitreal triamcinolone acetonide suspension was used to highlight these membranes. Mature preretinal membranes were peeled with forceps and a pick in a bimanual fashion utilizing chandelier mild for illumination. The elimination of subretinal membranes was tried by way of a small access retinotomy. However, the retinal folds nonetheless remained, indicating the presence of residual subretinal membranes inducing traction and folding of the retina. The small retinotomy was not adequate to visualize and take away all the subretinal membranes. It was determined to carry out an inferior 180� retinotomy to relieve the traction and to visualize and remove all the residual subretinal membranes. Subsequently perfluoron was injected into the eye to flatten the retina, and endolaser photocoagulation was utilized across the edges of the retinotomy. Careful examination of the peripheral retina round sclerotomy websites utilizing scleral despair. Placing the light pipe inside the cannula during its removal (pushing again incarcerated vitreous). During the postoperative period it may possibly solely be detected if the peripheral retina is visualized and a peripheral break or detachment occurs. The administration is to treat the secondary problems that ensue, particularly new breaks, opening of existing breaks, and redetachment. It was decided to proceed with a scleral buckling process, and an encircling scleral buckle with a no. A trochar-cannula with a chandelier mild was inserted into the attention to function mild supply. The fundus was visualized beneath the microscope utilizing the wide-angle viewing system. External drainage was carried out by scleral cutdown: making use of cautery to the scleral edges and choroidal bed, and puncturing the choroid with a 30G needle beneath direct visualization with the microscope. The chandelier gentle was removed, and an illuminated endolaser probe was inserted into the attention through the identical cannula to laser around the break. The cannula was removed, the sclerotomy site was not sutured, and the conjunctiva was closed. A week later the patient returned with a recurrent retinal detachment and a break near the sclerotomy site (for chandelier light) with vitreous strand seen incarcerating into the sclerotomy. Suddenly a foreign body was visualized superior to the optic nerve: a barely seen transparent silicone tip of the flute needle. It probably got caught within the 27G valved trochar and detached from the flute needle. During consecutive instrument change via the trochar, the silicone tip was inadvertently mobilized into the eye and fell on the retina. An try was made to remove the silicone tip by slipping it into the tip of 27 G forceps as a sleeve masking the forceps arm. This maneuver unfortunately widened the diameter of the 27G forceps, and the sleeve obtained stuck within the valved trochar. To overcome this drawback, the silicone tip was regrasped and in a bimanual trend the silicone tube was pulled over one of many arms of the forceps. The silicone tip was pulled upwards to the shaft of the forceps, permitting the forceps to safe the silicone tip and remove it. Core and peripheral vitrectomy was performed with the assistance of triamcinolone acetonide. However, the retinal tack dislodged from the implant and fell into the vitreous cavity. The microelectrode array was then placed again over the macula and was stabilized using a new retinal tack without any further issues. Berrocal Vitreous incarceration might happen on the sclerotomy websites and may trigger traction and peripheral retinal breaks. There has been a decrease within the incidence of this complication due to a lower in size of the sclerotomies and using trocar cannulas.