
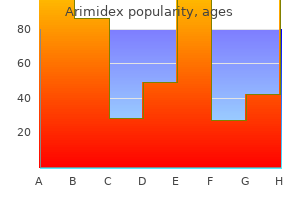
Arimidex dosages: 1 mg
Arimidex packs: 30 pills, 60 pills, 90 pills
Buy arimidex 1 mg low cost
Because there have been no indicators or signs of glucocorticoid or androgen extra menstruation 10 year old arimidex 1 mg order otc, Conn suspected menopause urinary incontinence effective arimidex 1 mg, based mostly on his previous research, that M. In his presidential address, Conn acknowledged: "It is believed that these studies delineate a new medical syndrome which is designated temporarily as main aldosteronism. In 1995, Gittler and Fajans described the surgical scene: "To the immense delight of Conn and those in the operating room, the surgeon, Dr. William Baum, encountered a right 13-g adrenal tumor which was eliminated whereas leaving the contralateral gland intact. Conn had achieved irrefutable proof of the validity of his investigative conclusions and established for the primary time the relationship among adrenal aldosterone-producing tumors, hypertension, and hypokalemia. A new period had arrived within the study of hypertension and adrenal mineralocorticoids. Conn stated148: "I even have prepared no comprehensive evaluate of my private philosophy of medical investigation. Instead, I plan to make a scientific report again to you about a clinical syndrome, the investigation of which has been most enjoyable to me since I initiated it in April of this yr. He instructed that these responses have been the end result of increased adrenocortical function with elaboration of salt-retaining steroids. Patients with marked hypokalemia could have muscle weakness and cramping, headaches, palpitations, polydipsia, polyuria, nocturia, or a mix of these. The polyuria and nocturia are a result of hypokalemia-induced renal concentrating defect, and the presentation is frequently mistaken for prostatism in males. The diploma of hypertension is often reasonable to extreme and may be resistant to the standard pharmacologic therapies. Hypokalemia is frequently absent, so all patients with hypertension are candidates for this dysfunction. In different sufferers, the hypokalemia becomes evident only with the addition of a potassium-wasting diuretic. Deep-seated renal cysts are present in up to 60% of sufferers with chronic hypokalemia. This scientific clue is very useful in the initial assessment for potential primary aldosteronism. Several research have shown that sufferers with major aldosteronism are at greater threat than different patients with hypertension for target-organ harm of the guts and kidney. Diagnosis the diagnostic strategy to major aldosteronism can be considered in three phases: case-detection tests, confirmatory exams, and subtype evaluation tests. Case-DetectionTests Spontaneous hypokalemia is rare in sufferers with uncomplicated hypertension; when current, it strongly suggests associated mineralocorticoid excess. However, a quantity of studies have proven that the majority sufferers with major aldosteronism have baseline serum levels of potassium in the regular range. Patients with hypertension and hypokalemia (regardless of presumed cause), treatmentresistant hypertension (poor control on three antihyper- tensive drugs), severe hypertension (160 mm Hg systolic or 100 mm Hg diastolic), hypertension and an incidental adrenal mass, or onset of hypertension at a younger age ought to undergo screening for primary aldosteronism. This check could additionally be carried out whereas the affected person is taking antihypertensive medicines (with some exceptions, mentioned later) and without posture stimulation. It may be troublesome to interpret data obtained from sufferers treated with a mineralocorticoid receptor antagonist (spironolactone and eplerenone). In this distinctive circumstance, the analysis for main aldosteronism can proceed regardless of remedy with mineralocorticoid receptor antagonists. However, in most patients already receiving spironolactone, remedy should be discontinued for a minimal of 6 weeks. In patients with out major aldosteronism, many of the variation occurs inside the normal range. However, the outline of the reference normal and the attribution of analysis at the finish of the research were incomplete, and there was a scarcity of standardization in regards to the origin of the research cohort, ongoing antihypertensive drugs, use of high-salt versus low-salt food regimen, and circumstances throughout blood sampling. The authors concluded that none of the studies offered any legitimate estimates of take a look at traits (sensitivity, specificity, and likelihood ratio at varied cutoff levels). However, few studies have compared the completely different strategies of testing for main aldosteronism, and these studies lack confirmatory testing. After hypertension and hypokalemia have been managed, patients ought to receive a highsodium diet (supplemented with sodium chloride tablets if needed) for three days, with a goal sodium intake of 5000 mg (equivalent to 218 mEq of sodium or 12. On the third day of the high-sodium diet, a 24-hour urine specimen is collected for measurement of aldosterone, sodium, and creatinine. To doc sufficient sodium repletion, the 24-hour urinary sodium excretion should exceed 200 mEq. Urinary aldosterone excretion of greater than 12 �g/24 hours in this setting is in maintaining with autonomous aldosterone secretion. The intravenous saline infusion take a look at has also been used broadly for the prognosis of major aldosteronism. Historically the saline infusion take a look at has been performed in the supine position and the false-negative fee has been extreme; preliminary knowledge recommend that if the saline infusion test is carried out in the seated position the accuracy is improved. In the fludrocortisone suppression test, fludrocortisone acetate is administered for four days (0. In these circumstances, additional testing is required to decide the supply of excess aldosterone secretion. Also, apparent adrenal microadenomas may very well represent areas of hyperplasia, and unilateral adrenalectomy would be inappropriate. For patients who wish to pursue a surgical treatment for their hypertension, adrenal venous sampling is frequently a key diagnostic step (see text for details). The sensitivity and specificity of a cortisolcorrected plasma aldosterone focus lateralization ratio greater than 4. The confirmatory test for major aldosteronism was also constructive, with the 24-hour urinary excretion of aldosterone measured at 53 �g on a high-sodium diet (urinary sodium, 196 mEq/24 hours). A, Adrenal computed tomography reveals a 12-mm, low-density mass (arrow, proper panel) in the medial limb of the left adrenal and two low-density, 10-mm nodules (arrows, left panel) inside the best adrenal gland. B, Adrenal venous sampling lateralized aldosterone secretion to the best, and two cortical adenomas (1. Hypokalemia was cured and blood pressure was normal with out the assist of antihypertensive medications. Safeguards ought to be in place to prevent mislabeling of the blood tubes within the radiology suite and to stop sample mixup in the laboratory. The venous pattern from the left facet usually is obtained from the frequent phrenic vein instantly adjoining to the entrance of the adrenal vein. In the absence of glucocorticoid therapy, this mutation leads to overproduction of aldosterone and the hybrid steroids 18-hydroxycortisol and 18-oxycortisol, which could be measured within the urine to make the analysis. Knowing the cause for the primary aldosteronism helps to decide the appropriate therapy. In addition to the kidney and colon, mineralocorticoid receptors are present within the coronary heart, brain, and blood vessels.
Syndromes
- Vasa previa
- High blood pressure
- Testis
- Changes in alertness and consciousness
- Female: 12.1 to 15.1 gm/dL
- Make sure your vision is good. Have your eyes checked once or twice a year by an eye doctor.
- Malnutrition
Arimidex 1 mg purchase without a prescription
Up to that point womens health quotes arimidex 1 mg order on-line, all embryonic cells are morphologi cally similar breast cancer 3 cm tumor arimidex 1 mg order amex, really totipotential, and able to beginning a brand new individual or any lineage. The formation of a 16cell morula marks the beginning of the method of differentia tion, with cells being allocated to the inside or outside of the embryo. At the following stage, the blastocyst, three lineages are outlined: trophectoderm, which is the precursor of the placenta; epiblast, which supplies rise to the somatic cells of the embryo; and primitive endoderm, which ultimately varieties the yolk sac. After the embryo implants, a bunch of cells inside the epiblast form the precursors of the primor dial germ cells, the primary cells of the long run ovary to be outlined. Entry into meiosis marks the developmental stage at which any progenitor cells which are able to differentiating to oocytes disappear. The meiotically arrested oocytes finally become surrounded by pregranulosa cells and kind particular person primordial fol licles, the resting pool of oocytes that have the potential to be recruited into the growing follicle pool during the postpubertal stage to be fertilized and to contribute to the following technology. These phenomena have been primarily observed in mice and are thought to be applicable to people. The triggers that initiate primordial germ cell migration and the chemoat tractants required for directional movement toward the genital ridge are beginning to be uncovered. A critical set off could additionally be expression of a key receptor on the primor dial germ cell and expression of the secreted chemoattrac tants from the genital ridge. From the third week on, germ cells of epiblast origin situated on the base of the yolk sac cross the dorsal mesentery of the hindgut and migrate to the gonadal ridges. By the identical token, germ cells play an indispensable role in the induc tion of gonadal improvement. On arrival on the genital ridge by the fifth week of gesta tion, the premeiotic germ cells are referred to as oogonia. This protuberance is created by proliferation of floor (coelo mic) germinal epithelium, by development of the underlying mesenchyme, and by oogonial multiplication. The highest number of oocytes is discovered in the ovaries of a human fetus at midgestation. After start, the progressive decline within the variety of ovarian follicles containing oocytes continues till full depletion at menopause. From this point on, the oogonial endowment is topic to three simultaneous processes: mitosis, meiosis, and oogonial atresia. Stated differently, the onset of oogo nial meiosis and oogonial atresia is superimposed on oogo nial mitosis. At this time, two thirds of the total germ cells are intrameiotic main oocytes; the remaining third can still be seen as oogo nial. The midgestational peak and the postpeak decline are accounted for in part by the progressively lowering fee of oogonial mitosis, a course of destined to finish totally by concerning the seventh month of intrauterine life. During this period, regulation of the ovarian developmental course of is complex and proba bly involves a various group of genes. From midgestation onward, relentless and irreversible attrition progressively diminishes the germ cell endow ment of the gonad. [newline]For essentially the most part, this is completed by way of follicular atresia somewhat than oogonial atresia, begins at about month 6 of gestation, and continues all through life. In distinction, oogonial atresia is destined to finish at 7 months of intrauterine life as follicular atresia sets in. Fol licular atresia has a profound effect on germ cell endow ment, as a end result of only one to 2 � 106 germ cells are present at delivery. Consequently, newborn women enter life still far from realizing their reproductive potential however having misplaced as much as 80% of their germ cell endowment. The germ cell mass decreases further to roughly 300,000 by the onset of puberty. Of these follicles, only four hundred to 500 (<1% of the total) are recruited for ovulation in the center of a reproductive life span. Between weeks eight and thirteen of fetal life, a variety of the oogonia depart from the mitotic cycle to enter the prophase of the first meiotic division. This change marks the conversion of these cells to major oocytes properly earlier than actual follicle formation. Once fashioned, the primary oocyte persists in prophase of the primary meiotic division till the time of ovulation, when meiosis is resumed and the first polar physique is fashioned and extruded. This speculation is predicated on the statement that denuded (granulosafree) oocytes are able to spontaneously finishing meiotic maturation in vitro. At ovulation, the secondary oocyte and the surrounding granulosa cells (cumulus oophorus) are extruded and enter the fallopian tube. If sperm penetra tion happens, the secondary oocyte undergoes a second meiotic division, after which the second polar physique is eliminated. Number of germ cells (millions) Granulosa Cell Layer In the developing ovaries of a human feminine fetus, oo cytes initially exist as germ cell clusters before an ovarian follicle is shaped. During the second half of in utero life, these germ cell clusters break down, and the surviving oocytes turn into individually surrounded with squamous pregranulosa cells to give rise to primordial follicles. The transition from primordial to main follicle is marked histologically by a morphologic change in granulosa cells from squamous to cuboidal. By the secondary stage, there are a minimum of two layers of cuboidal granulosa cells and an extra layer of somatic cells, the theca, which types outdoors the basement membrane of the follicle. A basement lamina separates the oocyte and granulosa cells from the encircling stromal cells. The avascular nature of the granulosa cell compartment necessitates contact between neighboring cells. The granu losa cells are interconnected by in depth intercellular gap junctions, which outcome of their coupling to yield an expanded, built-in, and useful syncytium. Connexin 37 and other connexins have been demonstrated in hole junctions in follicles. During meiosis, the chromosomes that have been inherited from the parents of the person and saved in gonads are processed to put together their genetic material for transmission to the offspring. Meiosis occurs completely in germ cells and serves two important purposes: generation of germ cells genetically distinct from the somatic cells and era of a mature egg (or sperm) with a reduction in the variety of chromosomes from 46 to 23. Genetic recombination via crossover of genes between homologous chromosomes and random assortment of (grand-) maternal and (grand-) paternal chromosomes into daughter cells during the first meiotic division are liable for the primary operate of meiosis, upkeep of genetic variety. The second function is offered by a reduction within the number of chromosomes so that each daughter cell, or ovum, receives randomly one chromosome from each of the 23 pairs. During fertilization, the fusion of ovum and sperm, every of which contributes 23 chromosomes, produces a genetically novel individual with 46 chromosomes. The chromosome marked as white within the oogonium (upper left corner) originates from the daddy of the female fetus, whereas the blue chromosome comes from the mother of the fetus. The random change of genes (alleles) between homologous chromosomes (crossover) takes place before the meiotic arrest within the prophase I stage earlier than start. Moreover, the granulosa cells lengthen cytoplasmic processes that penetrate the zona pellucida to type gap junctions with the plasma membrane of the oocyte. Several gene products regulate the transition from pri mordial to major follicle, which is marked by a change within the morphologic look of granulosa cells from squamous to cuboidal, followed by a rise in granu losa cell layers in the secondary follicle. Cumulus oophorus granulosa cells Fully grown oocyte Theca externa Theca Cell Layer After the follicle achieves two layers of granulosa cells, another morphologically distinct layer of somatic cells, the theca, differentiates from ovarian stroma.
Arimidex 1 mg amex
The prevalence of this disorder varies based on womens health diet arimidex 1 mg generic overnight delivery ethnic background breast cancer nike shoes arimidex 1 mg discount fast delivery, and the prevalence reported by totally different investigators has various extensively. The attribute presentation consists of anovulatory uterine bleeding and progressive hirsutism of pubertal onset. Patients of northern European ancestry have a low frequency of this dysfunction, whereas Ashkenazi Jews, Hispanics, and patients of central European ancestry have a a lot larger preva lence. Although most ladies with nonclassic adrenal hyperplasia are anovulatory, some girls with this dysfunction present with regular intervals and hirsutism of pubertal onset or with only unexplained infertility. Values between 2 and eight ng/mL are thought of increased but not diagnostic of nonclassic adrenal hyperplasia. A screening baseline degree of 17hydroxyprogesterone must be obtained for sufferers with premature pubarche, those with androgen extra of early pubertal onset, ladies with progressive hirsutism or virilization, and patients with robust household histories of extreme androgen extra. Salient medical options are of paramount importance to guide laboratory testing. The most necessary options are the onset and severity of the signs and the rapidity with which they progress. Rapidly progressing severe androgen excess implies an androgensecreting tumor till proved otherwise. The chance of a tumor is additional underscored in a postmenopausal lady or in a reproductiveage woman with a latest history of cyclic, predictable periods. The most useful preliminary check to evaluate androgen extra is the serum stage of total testosterone (Table 173). Ultrasonography of the ovaries also may help to identify an ovarian tumor or polycystic ovaries. Rare causes of androgen extra embrace an adrenal tumor, Cushing syndrome, and glucocorticoid resistance. A screening take a look at for Cushing syndrome and glucocorticoid resistance may be performed to discover rare adrenal causes of androgen excess (see Chapter 15). These ladies have highnormal or elevated tes tosterone ranges and no other laboratory abnormalities. TreatmentofHirsutism Therapy for androgen extra should be directed toward its particular cause and suppression of abnormal androgen secre tion. However, bilateral oophorectomy may turn out to be essential to management androgen extra arising from hyperthecosis (see later discussion). When treating andro gen excess associated with nonclassic adrenal hyperplasia, an antiandrogen. Although a glucocorti coid could additionally be thought of, the doses of glucocorticoids needed to suppress the adrenal can usually cause symptoms and indicators of glucocorticoid excess throughout longterm deal with ment. Thus, a mix oral contraceptive plus spi ronolactone is favored to deal with androgen excess if the patient responds to this therapy with decreased hirsut ism. Several courses of medications are reviewed in detail under for the remedy of androgen extra and hirsutism. Oral contra ceptives may additional enhance the outcomes of antiandrogen therapy in patients with idiopathic hirsutism or nonclassic adrenal hyperplasia. The mostly used androgen blocker for the remedy of hirsutism in the United States is spi ronolactone, an aldosterone antagonist structurally related to progestins. Treatment with spironolactone for 6 months reduces FerrimanGallwey scores of hirsutism by a mean of 38. Apart from inhibiting steroidogenesis and performing as an androgen antagonist, spironolactone has a big impact in inhib iting 5reductase activity. Although doses of 100 mg/ day normally are efficient for the remedy of hirsutism, higher doses (200 to 300 mg/day) could also be preferable in extremely hirsute or markedly obese girls. This strategy may be useful to decrease unwanted effects corresponding to gastritis, dry pores and skin, and anovulation. Monitoring for electrolytes and blood strain is imperative within the first 2 weeks at every dose stage. Adjustments in dose should be made solely after 3 to 6 months, as with other antiandrogens, to account for the sluggish modifications within the hair cycle. Some girls with regular cycles complain of menstrual irregularity with spironolactone; this is remedied by a downward dose adjustment or the addition of an oral con traceptive. Effec tive contraception should at all times be offered in women taking spironolactone. Cyproterone acetate is a 17hydroxy progesterone acetate spinoff with strong progestagenic properties. There can additionally be some proof that cyprot erone acetate and ethinyl estradiol in combination can inhibit 5reductase exercise in pores and skin. The drug usually is administered every day in doses of 50 to 100 mg on days 5 through 15 of the treat ment cycle. This regimen is needed for menstrual control and is usually referred to as the reverse sequential regimen. Cyproterone acetate in doses of fifty to 100 mg/day, com bined with ethinyl estradiol at 30 to 35 �g/day, is as effec tive as the combination of spironolactone (100 mg/day) and an oral contraceptive in the treatment of hirsutism. This regimen is primarily fitted to people with a milder form of hyperandrogenism. Finasteride inhibits 5reductase exercise and has been used primarily for the treatment of prostatic hyperplasia. Because hirsutism outcomes from the combined effects of sort 1 and sort 2, this agent is just partially efficient. Although prolonged expertise with finasteride is lacking, one of the potential benefits of this agent is its benign facet impact profile. The medi cations described in the previous paragraphs could also be effec tive when administered as particular person therapies. An oral contra ceptive containing 30 to 35 �g of ethinyl estradiol com bined with spironolactone (100 mg/day) is the preliminary treatment of choice. Even in women with idiopathic hir sutism, the addition of an oral contraceptive to the anti androgen spironolactone can improve efficacy and stop abnormal bleeding. For women with only minor com plaints of hirsutism, the utilization of an oral contraceptive alone may be an acceptable first approach. Scoring methods and evaluation of anagen hair shafts are difficult; taking photographs is the best and most objective device. Pictures of the face and chosen midline body areas before and during therapy are particularly useful for the encouragement of the affected person and compliance with the remedy. Plucking, waxing, and shaving are ineffective for hair removal and trigger irritation, folliculitis, and ingrown hairs. Then, depending on the wishes and medical responses of patients, therapy can be stopped and the patient reevaluated. Patients with clitoromegaly may be referred to a urologist for clito ral reduction surgery after the supply of virilization has been successfully eliminated. The precise mechanism liable for the therapeutic impact of elimination or destruction of part of the ovarian tissue is still not nicely understood. Subsequent scientific, morphologic, hormonal, and metabolic research uncovered multiple underlying pathologies, and the term polycystic ovary syndrome was launched to mirror the heterogeneity of this dysfunction. C, Histologic section of a polycystic ovary with a number of subcapsular follicular cysts and stromal hypertrophy at low energy (left).
Generic arimidex 1 mg with amex
The traditional features of a pituitary microadenoma are a hypodense lesion after contrast enhancement menopause 30s quality arimidex 1 mg, which may be related to deviation of the pituitary stalk womens health 092012 effective arimidex 1 mg, and a convex higher floor of the pituitary gland. Adrenal carcinomas are normally giant and are sometimes associated with metastatic spread at presentation. The mostly used agent is 131I-labeled 6-iodomethyl-19norcholesterol,278 a marker of adrenocortical cholesterol uptake. In patients with adrenal adenomas, the isotope is taken up by the adenoma however not by the contralateral suppressed adrenal gland. Glucocorticoid alternative regimens vary, however many facilities use low doses (15-20 mg) of hydrocortisone, and withdrawal regimens differ. One sensible approach is to measure the morning plasma cortisol having omitted the dose of hydrocortisone within the morning at 3-month intervals. A hypodense lesion is seen in the best aspect of the gland (arrow), with deviation of the pituitary stalk away from the lesion. After a biochemical diagnosis of Cushing disease, this patient was cured by transsphenoidal hypophysectomy. In distinction to smaller tumors, large macroadenomas are invariably invasive and recur after surgery. D, Cushing syndrome attributable to surgically confirmed primary pigmented nodular adrenal disease in a 21-year-old patient. Notice the a quantity of small nodules with comparatively atrophic internodular adrenocortical tissue involving the medial limb of the proper adrenal gland (arrow). In the interim, all sufferers should carry a steroid alert card and enhance their dose of alternative therapy within the event of an intercurrent sickness. Adrenal carcinomas have had a very poor prognosis, and most sufferers have died inside 2 years of analysis. Radiotherapy to the tumor mattress and to some metastases, corresponding to those in the backbone, may be of restricted worth. An irregular right adrenal mass is proven in A, and a large liver metastasis is seen in B. A, Plain chest radiograph demonstrates a suspicious lesion behind the left coronary heart border (arrow). B and C, Axial and sagittal computed tomographic pictures demonstrate a bronchial carcinoid tumor (arrow) abutting the diaphragm. D, Three-dimensional reconstruction illustrates adherence of the tumor to the diaphragm (arrow), which was confirmed at surgical procedure. The 10-year survival fee for sufferers with T1 N0 M0 disease is about 80% but is considerably impaired with elevated tumor mass, optimistic lymph nodes, and distant metastases, reaching lower than 20% for patients with T1-4 N0-1 M1. The major risk was the next growth of Nelson syndrome (postadrenalectomy hyperpigmentation with a regionally aggressive pituitary tumor). Several years later, the patient introduced with Nelson syndrome and a right third cranial nerve palsy (B and C) related to cavernous sinus infiltration from a domestically invasive corticotropinoma (D). Hypophysectomy and radiotherapy were performed with reversal of the third cranial nerve palsy (E). The surgical consequence for transsphenoidal hypophysectomy varies from middle to heart and with surgical expertise. In optimal facilities, remission charges are 70% to 90% for microadenomas and 50% for macroadenomas. The ideal consequence is a cured patient with intact pituitary operate, however this outcome may not be attainable for a affected person with Cushing disease in whom a pituitary adenoma was not recognized preoperatively or during the operation itself. In centers that lack services for frequent monitoring of cortisol levels, perioperative and postoperative hydrocortisone cowl is suggested; this could be reduced to upkeep replacement doses normally within 3 to 7 days. After selective removing of a microadenoma, the encompassing corticotrophs are normally suppressed. As a outcome, plasma cortisol ranges are less than 30 nmol/L (<1 �g/dL) postoperatively, and ongoing glucocorticoid replacement remedy is required. In the previous, pituitary irradiation was often used in the treatment of Cushing illness. However, due to the enhancements in pituitary surgical procedure, far fewer sufferers are so handled. The administration of recurrent Cushing disease involves a consideration of repeat surgery, gamma knife radiosurgery, and medical therapies. The cortisol extra and related hypokalemic alkalosis and diabetes mellitus can be ameliorated by medical therapy. Treatment of the small cell tumor itself may also, at least initially, produce enchancment. The daily dose should be decided by measurements of plasma or urinary free cortisol. The purpose should be to obtain a imply plasma cortisol focus of about 300 nmol/L (11 �g/dL) through the day or a traditional urinary free cortisol stage. For efficient control of Cushing syndrome, 400 to 1600 mg every day has been required. Doses of up to 5 g/day are required to control glucocorticoid extra, though proof that the drug causes tumor shrinkage or improves long-term survival is missing. This agent also produces mineralocorticoid deficiency, and concomitant glucocorticoid and mineralocorticoid replacement remedy may be required. Side results are frequent and embrace fatigue, pores and skin rashes, neurotoxicity, and gastrointestinal disturbance. However, the multireceptor somatostatin analogue, pasireotide, which demonstrates high-affinity binding to somatostatin receptor subtypes 1, 2, three, and 5, normalizes urinary free cortisol in 17% of patients with Cushing illness, with hyperglycemia being a typical aspect effect. Therefore, these sufferers may current with the features of androgen or mineralocorticoid excess, or both. Prognosis of Cushing Syndrome Studies performed earlier than the introduction of effective therapy revealed that 50% of sufferers with untreated Cushing syndrome died inside 5 years, principally from vascular illness. Skin desquamation, steroid-withdrawal arthropathy, profound lethargy, and temper modifications could occur and might take several weeks or months to resolve. They can often be ameliorated by a transient enhance in glucocorticoid alternative therapy. Features of Cushing syndrome disappear over a period of two to 12 months after treatment. Hypertension and diabetes mellitus improve, but as with other secondary causes, they may not resolve completely. The osteopenia of Cushing syndrome improves quickly during the first 2 years after therapy however resolves extra slowly thereafter. Reproductive and sexual function return to regular inside 6 months, provided that anterior pituitary function was not compromised. In the Western world, autoimmune adrenalitis accounts for greater than 70% of all instances of main hypoadrenalism. Conversely, solely 1% to 2% of sufferers with extra frequent autoimmune diseases corresponding to insulin-dependent diabetes mellitus or thyrotoxicosis have antiadrenal autoantibodies and develop adrenal illness, though the determine is larger in patients with autoimmune hypoparathyroidism (16%). Worldwide, infectious ailments are the commonest cause of primary adrenal insufficiency. These ailments embrace tuberculosis, fungal infections (histoplasmosis, cryptococcosis), and cytomegalovirus an infection.
Arimidex 1 mg cheap free shipping
Karyotype evaluation ought to be performed for boys with suspected Klinefelter syndrome stigmata or conduct menopause weight gain on abdomen 1 mg arimidex order amex. A presumptive diagnosis of constitutional delay in progress and adolescence is made if the historical past and growth chart reveal a historical past of brief stature but a consistent progress fee for skeletal age (and no indicators or signs of hypothalamic lesions) womens health doctors buy arimidex 1 mg without prescription, if the household historical past consists of parents or siblings with delayed puberty, if the bodily examination (including evaluation of the olfactory threshold) is regular, if optic discs and visible fields are regular, and if the bone age is significantly delayed. The fee of growth in these sufferers is often appropriate for bone age; a lower in progress velocity occurs in some regular youngsters simply earlier than the looks of secondary sexual traits and will awaken concerns if such a sample happens in these topics. This approach could assist predict spontaneous pubertal growth, but it nonetheless requires considerable watching and ready. Sometimes, years of remark are essential to detect the appearance of spontaneous and progressive signs of secondary sexual improvement or to document rising concentrations of gonadotropins or gonadal steroids earlier than the prognosis is clear. Treatment of Delayed Puberty and Sexual Infantilism Patients with constitutional delay in progress and adolescence ultimately have spontaneous onset and development through puberty. Often, reassurance and continued statement to ensure that the expected sexual maturation happens are adequate. These people could additionally be unable to participate in the relationship actions their associates are starting; smaller dimension might make them keep away from participation in athletics; immature appearance might result in ridicule, particularly in the locker room; and schoolwork could undergo because of their poor self-image. Some kids really feel such intense peer pressure and low vanity that solely the looks of signs of puberty can reassure them and allow them to take part in sports and social actions with their peers. Poor selfimage in late-maturing boys could carry into adulthood, even after normal puberty ensues. Growth retardation appears more usually responsible for many of the stress somewhat than the delay in pubertal development itself. For psychological reasons, for boys 14 years old or older who present no signs of puberty, a 3- to 6-month course of testosterone enanthate, cypionate, or cyclopropionate (50-mg dose given intramuscularly each four weeks) may be helpful. Because starting with the higher dose of a hundred mg can result in priapism in treatment-na�ve boys, care, decrease dosage, and short-acting preparations are advisable. Decades of experience affirm no impact on grownup peak of low dosages in the quick term. Although regression is possible with discontinuation of testosterone therapy, progression to liver failure can happen. Preliminary experience suggests that in a single day (about eight to 9 hours) or every-other-night use of a 2. An overnight examine of transdermal testosterone (5 mg of Virormone) utilized overnight (8 to 12 hours) for 4-week intervals in boys with delayed puberty and brief stature raised salivary testosterone ranges, stimulated leg development measured by knemometry. Functional hypogonadotropic hypogonadism associated with persistent illness is handled by assuaging the underlying drawback. Treatment with T4 allows normal pubertal growth in hypothyroid patients with delayed puberty. The transition of care from the vary of age normally thought-about to be adolescence, administered by a pediatric practitioner, to adult life, administered by a practitioner experienced in adult endocrinology, presents essential implications for a change within the method in which medical care is introduced. It is advisable to provoke puberty in these sufferers with low-dose gonadal steroids by age 14 in boys and age thirteen in ladies, regardless of the definitive analysis of gonadotropin deficiency. Positive psychological outcomes and attainment of normal stretched penile length have been reported. Prevent the potential short-term and long-term psychological, personality, and social handicaps of delayed puberty. Pregnancy could be achieved with this routine in ladies and spermatogenesis in men with hypogonadotropic hypogonadism. At present, long-term gonadal steroid substitute remedy is the treatment of alternative for hypothalamic or pituitary gonadotropin deficiency till fertility is desired. Hypergonadotropic hypogonadism is treated by replacement of testosterone in boys and estradiol in ladies. For remedy of gonadal dysgenesis, estrogen remedy ought to be initiated when the patient is age 13 (bone age >11 years) to enable secondary sexual growth at an acceptable chronologic age. Klinefelter syndrome is compatible with numerous degrees of spontaneous masculinization at puberty; some sufferers require testosterone substitute. Patients receiving gonadal steroid replacement observe the same remedy regimen whether the analysis is hypogonadotropic hypogonadism or hypergonadotropic hypogonadism (see Table 25-24). Various testosterone preparations can be found with several routes of administration. Alkylated testosterone preparations must be averted due to the chance of peliosis hepatis. Males might receive testosterone enanthate, propionate, or cypionate (50 to a hundred mg each four weeks intramuscularly) initially, although priapism has been reported with the upper beginning dose in a testosterone-na�ve boy; later, the dosage is progressively elevated to 200 to 300 mg each 2 to three weeks. Low-dose alternative therapy is suitable until nicely into the pubertal growth spurt. Testosterone may be administered by cutaneous patch on nonsexual pores and skin to cause secondary sexual improvement in hypogonadal adolescents; patches may be given at night to re-create the diurnal variation of testosterone seen in early puberty. Physiologic values of serum testosterone may be reached with these patches, along with secondary sexual growth. A teenage boy could also be less prone to apply a patch day by day, and biweekly or monthly injections might permit higher compliance; nonetheless, 2. New testosterone gel preparations, usually rubbed onto the forearms or shoulders, are accredited for adults but not for adolescents. Contact with the pores and skin, clothes, or towels used by a affected person treated with androgen gel can cause virilization in younger children or ladies. The maintenance dose should be the minimal quantity to maintain secondary sexual characteristics, sustain withdrawal bleeding, and prevent osteoporosis. After breakthrough bleeding occurs, or no later than 6 months after the start of cyclic remedy, a progestagen. Undesirable effects are unusual but may include weight gain, headache, nausea, peripheral edema, and mild hypertension. There is a concern in regards to the increased threat of endometrial and breast carcinoma in sufferers receiving persistent estrogen substitute remedy, including sufferers with Turner syndrome. Patients with hypopituitarism could complain of sparse pubic hair growth or, in girls, whole absence of pubic hair. Adolescent or young grownup girls have been given a low dose (25 mg) of long-acting intramuscular testosterone each 4 weeks to stimulate the growth of pubic hair without virilization. Sexual Precocity Sexual precocity (Table 25-25) is the appearance of any sign of secondary sexual maturation before the lower restrict of the normal age at onset of puberty. These newer limits are controversial, but when the cautions described are heeded, the bounds are acceptable. The manufacturing of extreme estrogens in males results in inappropriate feminization, and the manufacturing of elevated androgen levels in females leads to inappropriate virilization; these circumstances are termed contrasexual precocity or heterosexual precocity. In all types of sexual precocity, elevated gonadal steroid secretion will increase height velocity, somatic development, and the rate of skeletal maturation; because of untimely epiphyseal fusion, sexual precocity can result in the paradox of tall stature in childhood but quick adult height (Table 25-26). Blood pressure matches that of normal subjects of the identical top and gender after correcting for bone age somewhat than chronologic age in accordance with the most recent requirements for blood stress. Others reported a 10-fold increased prevalence of precocious puberty in women compared with boys. However, most kids referred for analysis have the benign variants leading to premature thelarche or untimely adrenarche. In in any other case wholesome girls, those with onset of puberty at 6 to 8 years of age usually characterize one end of the traditional range of age at puberty onset; those with constitutional delay in growth and adolescence fall on the opposite end of the conventional range of variation.
Omega-3 Fatty Acids (Dha (Docosahexaenoic Acid)). Arimidex.
- Depression.
- Preventing an eye disease called AMD (age-related macular degeneration), when DHA is consumed as part of the diet.
- Dosing considerations for Dha (docosahexaenoic Acid).
- Are there any interactions with medications?
- What other names is Dha (docosahexaenoic Acid) known by?
- Type 2 diabetes.
- How does Dha (docosahexaenoic Acid) work?
- Are there safety concerns?
- Reducing the risk of death in people with coronary artery disease, when DHA is consumed as part of the diet.
- Psoriasis.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96835
Purchase arimidex 1 mg without a prescription
Accurate substitute is important; in extra fsh 87 menopause arimidex 1 mg buy otc, glucocorticoids will suppress progress menopause longer periods 1 mg arimidex visa, whereas inadequate substitute will end result initially in accelerated linear progress and finally briefly stature because of untimely epiphyseal closure. C, Genotype-phenotype correlation in 21-hydroxylase deficiency is nicely established. Although variation has been reported for the milder mutations, the general correlation is high concerning expression of the adrenal phenotype. Ideally, the biochemical investigations will indicate the necessity for dose adjustments before bodily modifications, growth, and skeletal maturation indicate insufficient or extreme glucocorticoid treatment. The technique of alternative must be a one-stage complete repair using the most recent methods of vaginoplasty, clitoral, and labial surgical procedure. Overtreatment may end in weight problems and delayed menarche/puberty with sexual infantilism, whereas underreplacement will lead to sexual precocity. The follow-up of such sufferers ought to involve multidisciplinary clinics, initially with transition adolescence clinics to facilitate transfer from pediatric to adult care. Problems in maturity relate to fertility considerations, hirsutism, and menstrual irregularity in women; weight problems, metabolic penalties, and impact of short stature; possible increased cardiovascular threat; sexual dysfunction; and psychological problems. Males might develop enlargement of the testes because of so-called testicular adrenal rest tumors-that is, ectopic adrenal tissue, which may regress after glucocorticoid suppression. These sufferers need adequate endocrine remedy quite than urologic referral with ensuing risk of elimination of testis mistaken for a tumor. Hydrocortisone is recommended for substitute remedy from the new child period to adolescence. The optimum timing for offering the very best dose of hydrocortisone stays an ongoing matter of debate, with no knowledge supporting either circadian substitute (giving the highest dose within the morning) or reversephase therapy (giving the largest dose of hydrocortisone at night). Fludrocortisone is required for patients with salt wasting (although this will likely spontaneously improve with age). Sodium must be supplemented, as milk feeds present only upkeep sodium requirements. Adequate mineralocorticoid alternative usually leads to hydrocortisone dose reduction. Fludrocortisone doses of one hundred �g/m2 per day after the primary 2 years of life are generally enough. This requirement drops additional with adolescence and maturity to a day by day dose of 100 to 200 �g (50 to one hundred �g/m2 per day). Mineralocorticoid substitution is monitored by measurements of plasma renin exercise (low or suppressed ranges indicating overtreatment) and blood pressure. In scientific apply, sufficient supplementation of glucose throughout exercise and illness must be assured, to forestall hypoglycemic episodes. Prenatal dexamethasone remedy is effective to keep away from virilization of the external genitalia in the feminine fetus. One strategy is to advocate use of dexamethasone remedy as quickly as being pregnant is confirmed in high-risk instances and to proceed this therapy until the diagnosis is excluded in the feminine fetus. If the fetus is affected, only these of female intercourse require dexamethasone remedy throughout gestation. The advised dexamethasone dose is 20 to 25 �g/kg in three divided doses per day (total most dose, 1. In this fashion, the variety of unnecessarily handled cases can be reduced to three out of eight. Dexamethasone can result in maternal cushingoid results in pregnancy396 and should in flip have long-term, deleterious effects on the fetus, including metabolic, psychological, and intellectual consequences. In this setting, glucocorticoid suppression in isolation rarely controls hirsutism, and additional antiandrogen therapy is often required. An usually overlooked problem is glucocorticoid overtreatment during the first 2 years of life; overtreatment suppresses the infant growth spurt, which is characterized by the highest postnatal progress velocity. Therefore, the bottom optimum dose of glucocorticoid alternative should be established as early in life as attainable. Increased intima media thickness as a marker of atherosclerosis has been detected. In common, greater glucocorticoid doses are wanted to suppress hyperandrogenism in contrast with the scenario in 21-hydroxylase deficiency, and add-on antihypertensive therapy may be needed in some instances. Antihypertensive remedy should be commenced at an early stage to keep away from excessive glucocorticoid exposure. Corticosterone has weaker glucocorticoid activity than cortisol, however corticosterone excess generally prevents adrenal crises. There is lack of pubertal growth due to hypergonadotropic hypogonadism in each sexes. Because gonadal 17-hydroxylase activity can be absent, sex steroid secretion in addition to adrenal androgen secretion is severely impaired, resulting in hypogonadism. A number of totally different mutations have been described, without evidence of a hot spot. The intra-abdominal testes should be removed, and such patients are normally reared as females. The paradox of fetal virilization however sex hormone deficiency in postnatal life might be mediated by a newly found "backdoor" pathway of androgen synthesis in fetal life that depends on neither androstenedione nor testosterone as an intermediate. A287P is the most typical mutation in Caucasians, whereas R457H is essentially the most frequent founder mutation in the Japanese inhabitants. Loss of mineralocorticoid secretion results in salt wasting, though this is absent in 30% to 40% of cases. As with 21-hydroxylase deficiency, absence of salt wasting could delay the presentation into childhood or puberty, ranging from a extreme saltwasting kind with or with out ambiguous genitalia in affected male neonates to isolated premature pubarche in infants and youngsters of both sexes and a late-onset variant manifesting with hirsutism and menstrual irregularities. However, most sufferers current with hypospadias, and even normal male genitalia could also be discovered. In females, genital growth may be regular, but P450 Oxidoreductase Deficiency: Apparent Combined 17-Hydroxylase and 21-Hydroxylase Deficiencies Patients have been described with biochemical evidence of apparent mixed 17-hydroxylase and 21-hydroxylase deficiencies. Mothers pregnant with an affected baby current with low serum estriol and a characteristic urinary steroid profile, allowing for prenatal biochemical analysis. Impaired 17,20-lyase exercise results in poor androgen synthesis, and affected boys are often born undervirilized. Some moms develop signs of virilization during midpregnancy with an affected child; this commonly resolves quickly after birth, further indicating intrauterine androgen extra. Virilization in females can happen because of 3-hydroxysteroid dehydrogenase sort 1 exercise. Consequently, the lipid accumulation worsens the dysfunction and results in adrenal cell destruction. Salt losing sometimes develops within the neonatal interval or after a couple of weeks of life, but later onset may happen. Treatment with glucocorticoid, mineralocorticoid, and sex steroid substitute is required. This suggests blockade of only the terminal 18-oxidation step, with some residual aldosterone synthase exercise remaining.
Buy 1 mg arimidex amex
Psychosexual functioning in girls with complete androgen insensitivity syndrome: is androgen alternative remedy preferable to estrogen Height and bone mineral density in androgen insensitivity syndrome with mutations in the androgen receptor gene breast cancer xenograft models order 1 mg arimidex with amex. Gonadal maldevelopment as threat issue for germ cell cancer: towards a medical determination mannequin women's health clinic somerset ky arimidex 1 mg cheap overnight delivery. Evaluation of retained testes in adolescent girls and women with full androgen insensitivity syndrome. Normalization of the vagina by dilator therapy alone in complete androgen insensitivity syndrome and Mayer-Rokitansky-Kuster-Hauser syndrome. Managing the danger of germ cell tumourigenesis in problems of sex development sufferers. Molecular genetics of the persistent m�llerian duct syndrome: a examine of 19 households. Insensitivity to anti m�llerian hormone as a outcome of a mutation within the human antim�llerian hormone receptor. Genome-wide affiliation analyses identify variants in developmental genes associated with hypospadias. Fine mapping evaluation confirms and strengthens linkage of 4 chromosomal areas in familial hypospadias. Long-term observe up of men born with hypospadias: urological and cosmetic outcomes. Acquired undescended testes and fertility potential: is orchidopexy at analysis better than awaiting spontaneous descent Anogenital distance and penile size in infants with hypospadias or cryptorchidism; comparability with normative knowledge. Risk of cryptorchidism amongst sons of horticultural workers and farmers in Denmark. A French collaborative controlled examine of a cohort of 300 consecutive children with out genetic defect. A path forward within the debate over well being impacts of endocrine disrupting chemical compounds. Low dose mixture effects of endocrine disruptors and their implications for regulatory thresholds in chemical danger assessment. Male reproductive disorders, illnesses, and costs of exposure to endocrine-disrupting chemical compounds in the European Union. Congenital adrenal hyperplasia because of 21 hydroxylase deficiency: from birth to adulthood. Incidence and scientific features of congenital adrenal hyperplasia in Great Britain. Congenital adrenal hyperplasia as a result of 21hydroxylase deficiency: a paradigm for prenatal prognosis and remedy. Cognitive functions in children in danger for congenital adrenal hyperplasia handled prenatally with dexamethasone. Long-term outcome of prenatal dexamethasone therapy of 21-hydroxylase deficiency. Cognitive and motor improvement of children with and with out congenital adrenal hyperplasia after early-prenatal dexamethasone. Cognitive end result of offspring from dexamethasone-treated pregnancies in danger for congenital adrenal hyperplasia because of 21-hydroxylase deficiency. Congenital adrenal hyperplasia due to 21-hydroxylase deficiency: an Endocrine Society scientific practice guideline. Implementation of a liquid chromatography tandem mass spectrometry assay for eight adrenal C-21 steroids and pediatric reference information. Improving the communication of healthcare professionals with affected children and adolescents. Timing and nature of reconstructive surgical procedure for disorders of intercourse development-introduction. Sexual function and genital sensitivity following feminizing genitoplasty for congenital adrenal hyperplasia. New management technique of pregnancies at threat of congenital adrenal hyperplasia utilizing fetal intercourse dedication in maternal serum: French cohort of 258 cases (2002-2011). A analysis to not be missed: nonclassic steroid 11-hydroxylase deficiency presenting with untimely adrenarche and hirsutism. Generalized glucocorticoid resistance: clinical features, molecular mechanisms, and implications of a uncommon genetic dysfunction. History of aromatase: saga of an necessary biological mediator and therapeutic target. Genetic and medical spectrum of aromatase deficiency in infancy, childhood and adolescence. Molecular basis of aromatase deficiency in an grownup female with sexual infantilism and polycystic ovaries. Recurrent maternal virilization throughout being pregnant caused by benign androgen-producing ovarian lesions. Clinical aspects of MayerRokitansky-Kuester-Hauser syndrome: recommendations for clinical diagnosis and staging. Typical and atypical related findings in a gaggle of 346 patients with Mayer-Rokitansky-KuesterHauser syndrome. Persistent unexplained congenital clitoromegaly in females born extremely prematurely. Predictors of posttraumatic stress in mother and father of youngsters identified with a disorder of sex improvement. Adult women with 21-hydroxylase deficient congenital adrenal hyperplasia, surgical and psychological features. Timing of surgical procedure for feminizing genitoplasty in patients suffering from congenital adrenal hyperplasia. Relationship between final height and health outcomes in adults with congenital adrenal hyperplasia. Increased cardiovascular and metabolic morbidity in patients with 21-hydroxylase deficiency: a Swedish population-based national cohort study. Suboptimal psychosocial outcomes in sufferers with congenital adrenal hyperplasia; epidemiological research in a nonbiased national cohort in Sweden. A part 2 examine of Chronocort, a modified-release formulation of hydrocortisone, in the treatment of adults with congenital adrenal hyperplasia. Psychosexual improvement in adolescents and adults with problems of intercourse development-results 963 485. Male patients with partial androgen insensitivity syndrome: a longitudinal follow-up of development, reproductive hormones and the event of gynaecomastia. Whether linear growth occurs as a steady process or with periodic bursts of development and arrest1-4 has been hard to characterize definitively. There do appear to be seasonal differences of growth, with slower development in autumn and winter and larger progress in spring and early summer. Deviation from such a traditional pattern of development could be the first manifestation of all kinds of disease processes, together with endocrine and nonendocrine disorders and involving nearly any organ system of the body.
Arimidex 1 mg buy otc
A splicing mutation in the cytchrome b5 gene from a patient with congenital methemoglobinemia and pseudohermaphrodism breast cancer lymph nodes discount arimidex 1 mg on line. Genotype-phenotype analysis in congenital adrenal hyperplasia because of women's health clinic upland ca buy arimidex 1 mg cheap P450 oxidoreductase deficiency. Pubertal presentation in seven patients with congenital adrenal hyperplasia because of P450 oxidoreductase deficiency. Familial male pseudohermaphroditism with gynaecomastia because of a testicular 17-ketosteroid reductase defect: I. Molecular genetics and pathophysiology of 17 beta-hydroxysteroid dehydrogenase 3 deficiency. Residual exercise of mutant androgen receptors explains wolffian duct growth within the complete androgen insensitivity syndrome. Phenotypic variability in 17-hydroxysteroid dehydrogenase-3 deficiency and diagnostic pitfalls. Crystal constructions of the multispecific 17beta-hydroxysteroid dehydrogenase kind 5: crucial androgen regulation in human peripheral tissues. Steroid 17 beta-hydroxysteroid dehydrogenase deficiency in man: an inherited form of male pseudohermaphroditism. Male pseudohermaphroditism due to 17 beta-hydroxysteroid dehydrogenase deficiency: gender assignment in early infancy. Steroid 5-reductase deficiency in man: an inherited type of male pseudohermaphroditism. Phenotype and molecular traits in forty five Chinese youngsters with 5-reductase type 2 deficiency from South China. Paternity by intrauterine insemination with sperm from a person with 5-reductase-2 deficiency. Molecular characterization of 5 alphareductase type 2 deficiency and fertility in a Swedish household. The Sambia "turnim-man": sociocultural and medical features of gender formation in male pseudohermaphrodites with 5-alpha-reductase deficiency in Papua, New Guinea. The biochemical and phenotypic characterization of females homozygous for five alpha-reductase 2 deficiency. Diagnosis of 5-reductase 2 deficiency: is measurement of dihydrotestosterone essential Kinetics and effect of percutaneous administration of dihydrotestosterone in youngsters. Immunohistochemical localization of steroid 5 alpha-reductase 2 within the human male fetal reproductive tract and grownup prostate. Isoenzyme sort 1 of 5alphareductase is abundantly transcribed in regular human genital pores and skin fibroblasts and should play an necessary position in masculinisation of 5alpha-reductase kind 2 poor males. Molecular analysis of 5a-reductase deficiency in 4 elite younger athletes by way of hormonal screening for hyperandrogenism. Steroid receptor coactivators: servants and masters for management of methods metabolism. Comparison of bone mineral density and body proportions between ladies with full androgen insensitivity syndrome and women with gonadal dysgenesis. Lack of androgen receptor expression in Sertoli cells accounts for the absence of anti-m�llerian hormone repression throughout early human testis development. A novel mutation within the human androgen receptor suggests a regulatory function for the hinge area in amino-terminal and carboxy-terminal interactions. Correlation between genotype, phenotype and intercourse of rearing in 111 sufferers with partial androgen insensitivity syndrome. Androgen insensitivity syndrome: somatic mosaicism of the androgen receptor in seven households and penalties for intercourse assignment and genetic counselling. Promoter-dependent activity on androgen receptor N-terminal area mutations in androgen insensitivity syndrome. Therefore, frequent and accurate evaluation of growth is of main significance in the care of youngsters. Laboratory and radiologic investigations embrace an analysis for occult systemic disease and exclusion of hormonal abnormalities. Measurement Assessment of growth requires accurate and reproducible determinations of top. Supine length is routinely measured in children younger than 2 years of age, and erect peak is assessed in older youngsters. It could be useful to measure each length and height in kids between 2 and 3 years of age to allow comparisons with prior size measurements and to begin to document top measurement for ongoing comparisons. The inherent inaccuracies concerned in measuring length in infants are sometimes obscured by the fast skeletal development throughout this period. Optimally, the kid ought to be relaxed, the legs should be absolutely prolonged, and the top must be positioned in the Frankfurt airplane, with the road connecting the outer canthus of the eyes and the external auditory meatus perpendicular to the long axis of the trunk. But progress and ultimate top may additionally be affected by external elements, together with the quality and amount of diet, and by psychosocial factors. This process is regulated by multiple hormones and growth components interacting with an array of membrane receptors that activate seemingly redundant intracellular signaling cascades. Height determinations ought to be performed by a educated particular person somewhat than an inexperienced member of the employees. We recommend that lengths and heights be measured in triplicate, that variation ought to be not extra than zero. For determination of top velocity when a quantity of measurements are being made inside a brief period, the identical individual should carry out the determinations to remove interobserver variability. Even when each effort is made to acquire accurate height measurements, a minimal interval of 6 months is critical for meaningful top velocity computation. Nine to 12 months of data are preferable in order that errors of measurement are minimized and the seasonal variation in height velocity is assimilated into the information. There are, nonetheless, two limitations of these charts when applied to the person child. For instance, a brief youngster under the third percentile can be described extra exactly as being approximately four. The youngster must be absolutely erect, with the pinnacle in the Frankfurt plane; the again of the top, thoracic backbone, buttocks, and heels should contact the vertical axis of the stadiometer; and the heels ought to be collectively. Every effort ought to be made to correct discrepancies related to lordosis or scoliosis. Second, cross-sectional data are of greater value throughout infancy and childhood than in adolescence, as a result of differences in the timing of pubertal onset can considerably affect regular growth charges. To tackle this issue, Tanner and Davies10 developed longitudinal growth charts in an effort to assemble the curve shapes with centile widths obtained from a large cross-sectional survey, thus accounting for variability in the timing of puberty. Such charts are of particular value in assessing growth throughout adolescence and puberty and for plotting sequential development data for any particular person child. The knowledge from cross-sectional and longitudinal progress studies have been employed to develop peak velocity standards. It is essential to emphasize that carefully documented peak velocity data are invaluable in assessing a baby with abnormalities of progress.
Arimidex 1 mg cheap online
Venous thrombosis in users of non-oral hormonal contraception: follow-up study breast cancer 8 cm quality arimidex 1 mg, Denmark 2001-10 womens health consultants buy cheap arimidex 1 mg on-line. Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding. Effectiveness of the levonorgestrel-releasing intrauterine system within the therapy of adenomyosis diagnosed and monitored by magnetic resonance imaging. A 3-year follow-up of women with endometriosis and pelvic pain users of the levonorgestrelreleasing intrauterine system. Endometrial security after 5 years of steady combined transdermal estrogen and intrauterine levonorgestrel supply for postmenopausal hormone substitution. Effects of the levonorgestrel-releasing intrauterine system plus estrogen therapy in perimenopausal and postmenopausal girls: systematic evaluation and meta-analysis. Bone density restoration after depot medroxyprogesterone acetate injectable contraception use. Steroidal contraceptives and bone fractures in ladies: evidence from observational research. Bone mineral density loss and recovery during 48 months in first-time users of depot medroxyprogesterone acetate. Change in bone mineral density amongst adolescent girls using and discontinuing depot medroxyprogesterone acetate contraception. The impact of past use of the injectable contraceptive depot medroxyprogesterone acetate on bone mineral density in normal post-menopausal ladies. Use of depot medroxyprogesterone acetate contraception and incidence of bone fracture. The effects of depot medroxyprogesterone acetate and intrauterine gadget use on fracture risk in Danish ladies. Depot medroxyprogesterone acetate and bone mineral density in adolescents-the Black Box Warning: a Position Paper of the Society for Adolescent Medicine. Contraceptive and therapeutic effects of the levonorgestrel intrauterine system: an overview. Return to fertility after removal of a levonorgestrel-releasing intrauterine system and Nova-T. Levonorgestrel-releasing intrauterine system for atypical endometrial hyperplasia. Levonorgestrel-impregnated intrauterine system as treatment for endometrial hyperplasia: a national multicentre randomised trial. Treatment of endometrial hyperplasia with out atypia in peri- and postmenopausal ladies with a levonorgestrel intrauterine gadget. Oral progestogens vs levonorgestrel-releasing intrauterine system for endometrial hyperplasia: a systematic evaluate and metaanalysis. Safety and efficacy of Implanon, a single-rod implantable contraceptive containing etonogestrel. Safety and efficacy of a single-rod etonogestrel implant (Implanon): results from 11 worldwide clinical trials. Unintended pregnancies with the etonogestrel implant (Implanon): a case series from postmarketing expertise in Australia. The management of unacceptable bleeding patterns in etonogestrel-releasing contraceptive implant users. Lactogenesis after early postpartum use of the contraceptive implant: a randomized managed trial. Effects of the progestagen-only contraceptive implant Implanon on cardiovascular threat elements. Contraceptive failure of etonogestrel implant in sufferers handled with antiretrovirals including efavirenz. Population effect of increased entry to emergency contraceptive tablets: a scientific evaluate. Research priorities for preventing unintended pregnancy: moving beyond emergency contraceptive tablets. Ulipristal acetate for emergency contraception: postmarketing expertise after use by more than 1 million girls. Progesterone receptor modulator for emergency contraception: a randomized managed trial. Interest in intrauterine contraception among seekers of emergency contraception and being pregnant testing. The efficacy of intrauterine gadgets for emergency contraception: a scientific evaluation of 35 years of expertise. Likelihood of conception with a single act of intercourse: providing benchmark rates for evaluation of post-coital contraceptives. Effectiveness of emergency contraceptive drugs between 72 and 120 hours after unprotected sexual intercourse. Ulipristal acetate versus levonorgestrel for emergency contraception: a randomised non-inferiority trial and meta-analysis. Ulipristal acetate prevents ovulation extra effectively than levonorgestrel: evaluation of pooled information from three randomized trials of emergency contraception regimens. Immediate pre-ovulatory administration of 30 mg ulipristal acetate significantly delays follicular rupture. American College of Obstetricians and Gynecologists Committee on Gynecologic Practice, Long-Acting Reversible Contraception Working Group. Use of Norplant contraceptive implants within the immediate postpartum interval: safety and tolerance. Postpartum return of ovarian activity in nonbreastfeeding ladies monitored by urinary assays. The mixed contraceptive vaginal ring (NuvaRing) and lipid metabolism: a comparative research. Effects of Mirena (levonorgestrel-releasing intrauterine system) and Ortho Gynae T380 intrauterine copper device on lipid metabolism-a randomized comparative examine. Effect of etonogestrel implant on serum lipids, liver function checks and hemoglobin levels. Hormonal versus non-hormonal contraceptives in girls with diabetes mellitus sort 1 and 2. Effect of a levonorgestrel intrauterine system on ladies with sort 1 diabetes: a randomized trial. Higher threat of venous thrombosis during early use of oral contraceptives in women with inherited clotting defects. Use of contraceptive strategies by ladies with current venous thrombosis on anticoagulant remedy: a scientific review. Oral progestogenonly contraceptives and cardiovascular threat: results from the Transnational Study on Oral Contraceptives and the Health of Young Women. Assessing the risk of venous thromboembolic events in ladies taking progestin-only contraception: a meta-analysis.
Buy arimidex 1 mg cheap
Short stature with normal progress hormone stimulation testing: lack of proof for partial growth hormone deficiency or insensitivity breast cancer backgrounds arimidex 1 mg cheap amex. Augmentation of growth hormone secretion during puberty: proof for a pulse amplitudemodulated phenomenon womens health fitness arimidex 1 mg order without prescription. Divergent effect of endogenous and exogenous sex steroids on the insulin-like development issue I response to progress hormone in short normal adolescents. The impact of testosterone therapy on spontaneous progress hormone secretion in boys with constitutional delay. Administration of low-dose estrogen quickly and directly stimulates development hormone manufacturing. Final heights of boys with normal development hormone responses to provocative exams following priming. Lower growth hormone and better cortisol are associated with greater visceral adiposity, intramyocellular lipids, and insulin resistance in overweight ladies. Multiple endocrine abnormalities of the growth hormone and insulin-like progress issue axis in prepubertal children with exogenous obesity: effect of short- and long-term weight reduction. Effect of body mass index on peak development hormone response to provocative testing in children with quick stature. Reproducibility of progress hormone testing procedures: a comparison between 24-hour built-in focus and pharmacological stimulation. Variability of progress hormone response to pharmacological and sleep tests carried out twice in brief kids. The advantage of measuring stimulated as in contrast with spontaneous development hormone ranges in the analysis of progress hormone deficiency. Diagnostic limitations of spontaneous progress hormone measurements in normally rising prepubertal youngsters. A prospective, randomized examine of testosterone therapy of constitutional delay of growth and improvement in male adolescents. Treatment of constitutional delay of growth and puberty with oxandrolone in contrast with growth hormone. Oxandrolone in constitutionally delayed development, a longitudinal research as a lot as ultimate top. Oxandrolone therapy of constitutional short stature in boys throughout adolescence: impact on linear development, bone age, pubic hair, and testicular improvement. Double blind placebo controlled trial of low dose oxandrolone within the treatment of boys with constitutional delay of growth and puberty. Long-term consequence of oxandrolone treatment in boys with constitutional delay of growth and puberty. Treatment of constitutional development delay in prepubertal boys with a protracted course of low dose oxandrolone. The impact of androgens on the pulsatile release and the twenty-four-hour mean concentration of development hormone in peripubertal males. The results of oxandrolone on the expansion hormone and gonadal axes in boys with constitutional delay of growth and puberty. Androgen-stimulated pubertal growth: the effects of testosterone and dihydrotestosterone on development hormone and insulin-like growth factor-I in the therapy of short stature and delayed puberty. Estrogen receptor blockade with tamoxifen diminishes growth hormone secretion in boys: proof for a stimulatory position of endogenous estrogens throughout male adolescence. Androgen receptor blockade with flutamide enhances progress hormone secretion in late pubertal males: proof for impartial actions of estrogen and androgen. Transdermal testosterone gel improves sexual operate, temper, muscle energy, and physique composition parameters in hypogonadal men. Sexual precocity in a 2-year-old boy attributable to indirect exposure to testosterone cream. Effect of development hormone therapy on grownup top in peripubertal children with idiopathic quick stature: a randomized, double-blind, placebo-controlled trial. Adult height in kids with quick stature and idiopathic delayed puberty after totally different administration. Treatment with the aromatase inhibitor letrozole throughout adolescence will increase near-final height in boys 1021. Alterations in the pulsatile properties of circulating development hormone concentrations throughout puberty in boys. Improvement of diagnostic standards in progress hormone insensitivity syndrome: options and pitfalls. Pedigree analysis of constitutional delay of growth and maturation: dedication of familial aggregation and inheritance patterns. Comparison of predicted and adult heights briefly boys: effect of androgen remedy. The effect of puberty on progress hormone secretion in boys with short stature and delayed adolescence. Growth hormone response patterns to sex hormone administration in growth retardation. Overnight growth hormone concentrations are normally normal in pubertal kids with idiopathic quick stature-a medical analysis center study. Evidence for partial progress hormone insensitivity among patients with idiopathic quick stature. Reduced concentration of serum development hormone-binding protein in youngsters with idiopathic short stature. Serum progress hormone-binding protein is decreased in prepubertal kids with idiopathic brief stature. Spontaneous growth and response to development hormone remedy in kids with growth hormone deficiency and idiopathic quick stature. Neuropathologic verification of Creutzfeldt-Jakob illness within the exhumed American recipient of human pituitary progress hormone: epidemiologic and pathogenetic implications. The prismatic case of Creutzfeldt-Jakob disease related to pituitary growth hormone remedy. Update of tips for the use of progress hormone in youngsters: the Lawson Wilkins Pediatric Endocrinology Society Drug and Therapeutics Committee. Outcome of a four-year randomized research of every day versus 3 times weekly somatropin treatment in prepubertal naive development hormone-deficient youngsters. Subcutaneous versus intramuscular growth hormone therapy: progress and acute somatomedin response. Final peak consequence of development hormone-deficient sufferers treated since lower than 5 years of age. Current dosing of growth hormone in children with development hormone deficiency: how physiologic Long-term therapy in kids with hypopituitarism: pubertal improvement and final top. Factors figuring out pubertal growth and final top in growth hormone remedy of idiopathic progress hormone deficiency.