
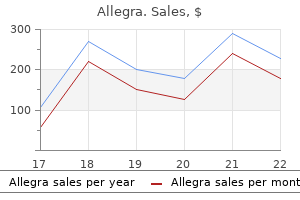
Allegra dosages: 180 mg, 120 mg
Allegra packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Allegra 180 mg cheap amex
Note the characteristic soft tissue shadow (open arrow) protruding by way of the ground into the superior portion of the maxillary sinus food allergy symptoms 1 year old allegra 180 mg discount without prescription. The fracture happens in the thinnest allergy hair loss generic allegra 180 mg without prescription, weakest portion of the orbit, which is the orbital flooring simply above the maxillary sinus. Note the displacement of the inferior rectus muscle (solid arrow) in this affected person, who had restricted upward gaze. Interruption of the orbital rim (white arrow), lateral maxillary fracture (black arrow), and nondisplaced zygomatic arch fracture (arrowheads) are demonstrated. Submentovertex projection demonstrates two fractures on the best with melancholy of the zygomatic arch. Herniation of orbital fats and extraocular muscular tissues into the fractured orbital ground produces a attribute gentle tissue shadow protruding via the ground into the superior portion of the maxillary sinus. Opacification of the sinus caused by hemorrhage and mucosal edema is an oblique signal of orbital ground fracture. Zygomatic arch fractures are best demonstrated on underexposed images taken in the basal (submentovertex) projection ("jug-handle" view). It is so named as a outcome of it displays separation of the zygoma from its three principal attachments. The mandible is a prominent, uncovered phase of the facial skeleton and is thus a typical web site for each intentional and unintentional trauma. The angle of the mandible is the most common web site of fracture, although fractures can contain any portion of the body and the condylar and coronoid processes. Because the mandible capabilities basically as a bony ring, bilateral fractures are frequent. Treatment for nasal bone fractures varies depending on the quantity of bony displacement. More severe facial fractures require surgical reconstruction, probably utilizing inside or external fixation gadgets to prevent disfigurement. Panoramic examination in edentulous (without teeth) patient reveals fractures of the left angle and the right body of the mandible. The radiographic evaluation of cerebrovascular illness is determined by the signs and the most probably prognosis. Stroke Syndrome Stroke denotes the sudden and dramatic growth of a focal neurologic deficit, which can differ from dense hemiplegia (paralysis on one facet of the body) and coma to only a trivial neurologic disorder. A stroke, also referred to as an acute mind infarction, mostly includes the circulation of the interior carotid arteries and is seen with symptoms that include acute hemiparesis (weakness of one aspect of the body) and dysarthria (difficulty speaking). The purpose of radiographic evaluation within the patient with acute stroke is not to verify the analysis of a stroke but to exclude different processes that may simulate the scientific findings. Pathologic processes inflicting cerebrovascular disease include abnormalities of the vessel wall, occlusion by thrombus or emboli, rupture of blood vessels with subsequent hemorrhage, and decreased cerebral blood move brought on by lowered blood strain or narrowed lumen caliber. Low-attenuation area (arrows) reveals sharply outlined borders and some midline shift. The grey matter and white matter in the distribution of the left center cerebral artery reveal low density. Occlusion or stenosis of an artery or vein could be demonstrated along with the associated hemorrhage as a outcome of ischemic infarction. There is just a small window of two or three hours after the onset of a stroke during which fibrinolytic agents are effective in decreasing the risk of permanent neurologic deficits. Low-attenuation area exhibits sharply outlined borders (arrows) and a few dilation of the adjacent ventricle. All sufferers with stroke are began on bed relaxation with decreased exterior stimuli to decrease cerebral oxygen calls for. Patients with thrombotic strokes obtain anticoagulants and possibly thrombolytic agents. There is extreme narrowing (arrow) of the origin of the inner carotid artery (I) by densely echogenic arteriosclerotic plaque (asterisks). They could result from emboli originating from the floor of an arteriosclerotic, ulcerated plaque (embolic stroke), which causes momentary occlusion of cerebral vessels, or from stenosis of an extracerebral artery, which results in a discount in important blood perfusion. This method combines high-resolution ultrasound imaging and Doppler ultrasound with spectral analysis into a "duplex" unit that avoids lots of the issues associated with each of those modalities used alone. High-resolution, real-time ultrasound strategies provide hemodynamic information about blood flow velocity. With use of ultrasound strategies, it could be unimaginable to differentiate a complete occlusion of the interior carotid artery from a tiny residual lumen. This is an important medical distinction as a outcome of the patient with even a small remaining lumen can undergo a profitable carotid endarterectomy (surgical removal of atherosclerotic plaque). The reconstitution signal (flow gap) confirms a stenosis higher than 60%, indicating advanced disease requiring surgical intervention. The anteroposterior perspective of the neck demonstrates vessels from the subclavian arteries to the origin of the basilar artery, and the bifurcation of the common carotid arteries. Common carotid arteriogram reveals an ulcerated lesion (arrowhead) at the origin of the interior carotid artery, with severe stenosis of the interior carotid (open arrow) and exterior carotid (black arrow) arteries. Common carotid arteriogram shows the bulbous origin of the interior carotid artery (solid arrow) and a quantity of branches of the exterior carotid artery (open arrows). Accurate analysis and appropriate remedy (antiplatelet remedy, anticoagulation therapy, or carotid endarterectomy) are essential to prevent permanent deficits. Intraparenchymal Hemorrhage Aside from head trauma, the principal reason for intraparenchymal hemorrhage (hemorrhagic stroke) is hypertensive vascular disease. Hypertensive hemorrhages end in oval or circular collections that displace the surrounding brain and can have vital mass impact. A widespread complication is rupture of the hemorrhage into the ventricular system or subarachnoid area. The low-density area (arrowheads) adjacent to the hematoma represents associated ischemia and edema. Hematoma has entered the ventricular system, and a prominent cerebrospinal fluid�blood level may be seen in the dependent lateral ventricle (arrow). Such extension of blood into the ventricular system is an especially poor prognostic sign. Mass effect due to the hematoma has compressed the third ventricle and the foramen of Monro and has resulted in obstructive enlargement of the lateral ventricles. They embrace the sylvian fissure (middle cerebral artery) and the midline subfrontal space (anterior communicating artery). Hematomas produce ventricular compression and, when massive, considerable midline shift and brain herniation. Contrast enhancement usually develops across the periphery of a hematoma after 7 to 10 days. Once the methemoglobin is totally converted to paramagnetic hemosiderin, the hematoma demonstrates very low sign intensity on T2-weighted sequences.
180 mg allegra purchase with mastercard
Lamotrigine allergy forecast tacoma wa allegra 120 mg discount on line, tiagabine allergy symptoms to pollen allegra 180 mg low price, and topiramate are capable of interacting with a number of other anticonvulsants. Many drugs are able to decreasing seizure threshold and should p the effectiveness of anticonvulsants, together with tricyclic antidepressants and phenothiazines. Toxicity and Overdose: Monitor serum drug levels routinely all through anticonvulsant therapy, particularly when adding or discontinuing other brokers. Potential Nursing Diagnoses Implementation Administer anticonvulsants across the clock. Patient/Family Teaching Instruct patient to take medicine daily, exactly as directed. Do not resume driving till doctor gives clearance based on control of seizures. Other uses include: Treatment of tension (doxepin, duloxetine, fluoxetine, paroxetine, sertraline, venlafaxine); Enuresis (imipramine); Chronic ache syndromes (amitriptyline, doxepin, duloxetine, imipramine, nortriptyline); Smoking cessation (bupropion); Bulimia (fluoxetine); Obsessive-compulsive disorder (fluoxetine, fluvoxamine, paroxetine, sertraline); Social anxiousness dysfunction (paroxetine, sertraline, venlafaxine). General Action and Information Antidepressant activity is most likely because of stopping the reuptake of dopamine, norepinephrine, and serotonin by presynaptic neurons, resulting in accumulation of these neurotransmitters. Most tricyclic brokers possess important anticholinergic and sedative properties, which explains many of their unwanted side effects (amitriptyline, amoxapine, doxepin, imipramine, nortriptyline). Elderly males with prostatic enlargement could also be more prone to urinary retention. Anticholinergic unwanted effects of tricyclic antidepressants (dry eyes, dry mouth, blurred vision, and constipation) might require dosage modification or drug discontinuation. Additive anticholinergic effects with other medication possessing anticholinergic properties. Risk of adverse reactions could additionally be q by almotriptan, frovatriptan, rizatriptan, naratriptan, sumatriptan, or zolmitriptan. Symptoms embody chest ache, extreme headache, nuchal rigidity, nausea and vomiting, photosensitivity, and enlarged pupils. Health care skilled must be contacted immediately if symptoms of hypertensive disaster develop. Frequent rinses, good oral hygiene, and sugarless candy or gum might diminish dry mouth. Advise patient to notify health care professional of medicine regimen and any natural different therapies earlier than therapy or surgical procedure. Emphasize the importance of participation in psychotherapy and follow-up exams to consider progress. It may also be used in sort 2 diabetes mellitus when food regimen and/or oral medicines fail to adequately control blood sugar. The selection of insulin preparation (rapid-acting, intermediate-acting, long-acting) is decided by the degree of control desired, daily blood glucose fluctuations, and history of previous reactions. It also promotes the conversion of amino acids to proteins in muscle, stimulates triglyceride formation, and inhibits the release of free fatty acids. Miglitol delays digestion of ingested carbohydrates, thus decreasing blood glucose, especially after meals. Oral hypoglycemic agents- Hypersensitivity (cross-sensitivity with different sulfonylureas and sulfonamides may exist). Avoid use in sufferers with severe kidney, liver, thyroid, and different endocrine dysfunction. Precautions Insulin- Infection, stress, or changes in food regimen may alter requirements. Use with sulfonylureas with warning in patients with a historical past of heart problems. Interactions Insulin-Additive hypoglycemic results with oral hypoglycemic agents. Oral hypoglycemic agents-Ingestion of alcohol might result in disulfiram-like reaction with some brokers. Assess serum electrolytes, ketones, glucose, and, if indicated, blood pH, lactate, pyruvate, and metformin ranges. Lab Test Considerations: Serum glucose and glycosylated hemoglobin ought to be monitored periodically all through remedy to consider effectiveness of remedy. Potential Nursing Diagnoses Imbalanced diet: greater than physique requirements (Indications). Withhold oral hypoglycemic agents and reinstitute after decision of acute episode. Patients switching from every day insulin dose might require gradual conversion to oral hypoglycemics. Check sort, species, source, dose, and expiration date with another licensed nurse. If hypoglycemia happens, advise affected person to take a glass of orange juice or 2� 3 tsp of sugar, honey, or corn syrup dissolved in water (glucose, not table sugar, if taking miglitol), and notify health care skilled. Advise affected person to carry sugar or a type of glucose and identification describing treatment regimen always. Counsel feminine patients to use a form of contraception apart from oral contraceptives and to notify well being care professional promptly if being pregnant is deliberate or suspected. Insulin: Instruct affected person on proper approach for administration; embrace type of insulin, equipment (syringe and cartridge pens), storage, and syringe disposal. Sulfonylureas: Advise affected person that concurrent use of alcohol might cause a disulfiram-like reaction (abdominal cramps, nausea, flushing, headache, and hypoglycemia). Control of blood glucose levels with out the appearance of hypoglycemic or hyperglycemic episodes. General Action and Information Diphenoxylate/atropine, difenoxin/atropine, and loperamide gradual intestinal motility and propulsion. Bismuth subsalicylate can be used as part of the administration of ulcer illness because of Helicobacter pylori. Polycarbophil acts as an antidiarrheal by taking up water inside the bowel lumen to create a fashioned stool. Precautions Use cautiously in patients with severe liver disease or inflammatory bowel disease. Safety in pregnancy and lactation not established (diphenoxylate/atropine and loperamide). Instruct patient to notify well being care skilled if diarrhea persists; or if fever, belly pain, or palpitations happen. Dimenhydrinate, scopolamine, and meclizine are used nearly exclusively to forestall motion illness. General Action and Information Phenothiazines act on the chemoreceptor set off zone to inhibit nausea and vomiting. Dimenhydrinate, scopolamine, and meclizine act as antiemetics primarily by diminishing movement illness. Aprepitant acts as a selective antagonist at substance P/neurokinin 1 receptors within the mind. Precautions Use phenothiazines cautiously in youngsters who could have viral illnesses.
Allegra 180 mg order visa
Note the white spaces throughout the blood vessel as a outcome of allergy shots pregnancy order allegra 180 mg free shipping fat that was dissolved away throughout slide processing allergy symptoms ragweed allegra 180 mg discount. This could be seen with skeletal fractures, crush injury to fatty tissue, burns, and even liposuction. This stage may be rapidly fatal if the embolized fats quantity is giant enough and is dispersed into blood vessels shortly, even before it passes through to affect the brain. Diffusely there are perivascular "ring" hemorrhages with intravascular empty areas that compress the adjacent cells and tissues similar to the intravascular fats globules dissolved during processing. Fat embolism syndrome normally presents between 1 and 3 days after trauma with shortness of breath, neurological changes, and petechial rash. Both on H&E and Luxol quick blue, pale areas correspond to areas of demyelination, usually in a perivascular distribution with lymphocytes and macrophages. In the pons this is to be contrasted with the midline demyelination found in central pontine myelinolysis. There are usually no signs within the first 24 hours following overdose, leading to large liver necrosis between three and 5 days. The spectrum leading up to this will likely embrace delicate lymphocytic infiltrates of the portal tracts and partial sparing of periportal hepatocytes. Glycolic acid is liable for the metabolic acidosis in ethylene glycol poisoning. The elevated oxalic acid excretion results in the formation of calcium oxalate crystals within the renal tubules and the foamy appearance of the tubules. Activated charcoal is an absorbent powder used for gastrointestinal decontamination following a poisonous ingestion. Note the gastric mucosal tablet fragments that are demonstrated in numerous degrees of polarization. Frequent causes embrace alcohol abuse, gallstones, metabolic problems, infections, and endoscopic retrograde cholangiopancreatography. Wernicke� Korsakoff encephalopathy occurs in alcoholics with thymine (vitamin B1) deficiency. Grossly these malformations might appear as red spongy plenty or may be too small to establish easily. Symptoms embody these related to sympathetic hyperactivity including fluctuations in blood stress, coronary heart price, weight reduction, and anxiousness. The highly vascular nature will lead to a point of pink to brown discoloration. Note the histopathology sections with marked congestion, fibrosis, and Gamna�Gandy our bodies from iron pigments with calcium salts. The sinusoidal areas are diffusely congested and crammed with sickle-shaped red blood cells. Isolated sickled pink blood cells might happen in sufferers with out sickle cell anemia. Hemoglobin crystallization leading to malformed sickle-shaped pink blood cells could also be perpetuated by hypoxia acidosis and dehydration from actions similar to vigorous exercise. Sickled cells create blood move obstruction, additional sickling, and further hypoxia with hemolysis. This is associated with severe pain and probably tissue infarction that may lead to demise. Even people with sickle cell trait, under severe conditions, have been known to go into disaster and die. In low-androgen states in a postpubertal male such as persistent ethanol abuse and anabolic steroid use, the seminiferous tubules present hyalinization with atrophy of the germ cells leaving only Sertoli and Leydig cells. The infected glial cells are can seem bizarre and pleomorphic with glassy nuclear inclusions. In a thermal burn, the epidermis and dermis are contracted with hypereosinophilia and nuclear streaming. Strongyloides is an intestinal parasite that may cause pulmonary infections, principally in immunocompromised hosts. Strongyloidiasis can current with acute respiratory insufficiency/failure or pulmonary embolism. A crescent is the outcome of marked basement membrane injury and characterized by epithelial cells, macrophages, fibrin, and particles within Bowman house. The degree and quantity of glomerular crescents typically correspond to the degree of renal damage. The etiology can be vasculitis (immune), collagen vascular disease, or antiglomerular basement membrane illness. The immature trophozoite (ring) varieties are seen throughout the mature purple blood cells on this smear. In the lung, the basophilic calcification appears within the alveolar walls and is optimistic with Von Kossa staining. In uncommon cases, metastatic calcification may find yourself in vital pulmonary edema, respiratory compromise, and death. After roughly 16 hours monocytes first seem consisting of lymphocytes and macrophages. While the inflammatory response is going on, granulation tissue begins to type at about 24�72 hours and continues for up to 7 days or more. Note the free connective tissue with early blood vessel formation, plump fibroblasts, and early collagen deposition. It generally takes weeks for full healing with scar formation and wound contraction to occur. When found in lungs and organs of nondecomposed bodies retrieved from fresh water, they assist drowning as a reason for death and may be useful in figuring out the location of demise as properly. A shot record with correct angles, scales, and tools will provide a formulation that will cowl all of the photographic proof wanted for the investigation. Without a minimal shot record of images, the viewers not current at the scene could misread proof. This chapter will provide a easy system that breaks down scene and autopsy photography into three easy sections: overalls, midrange, and closeups. These three sections will cover all the pictures abilities wanted to correctly document forensic evidence and create a quick, consistent workflow. Legal and Regulatory Considerations the American legal system often uses photographic and digital photographs obtained throughout a forensic dying investigation as evidence. The legal requirements for inclusion of images embrace: � the picture has to be related to the problem before the court docket (Federal Rules of Evidence 401). In addition, there are a plethora of tips regarding the usage of digital images in forensics. Most pictures obtained in the course of a forensic demise investigation fall beneath Category 1.
180 mg allegra trusted
Premedicating with antipyretics allergy symptoms versus sinus infection order allegra 120 mg with mastercard, corticosteroids allergy symptoms urination allegra 180 mg fast delivery, antihistamines, meperidine, and antiemetics might decrease these reactions. Monitor vital indicators every 15 min throughout check dose and each 30 min for 2� four hr after administration. May be diluted in 250 mL of D5W if being administered through a central venous catheter. To acquire check dose, withdraw 1 mg (10 mL) from 500 mL infusion and additional dilute with D5W to a complete quantity of 20 mL. Intermittent Infusion: Diluent: Reconstitute and dilute 50-mg vial as per the directions above. Y-Site Compatibility: aldesleukin, aminocaproic acid, argatroban, carmustine, dactinomycin, diltiazem, etoposide, hydromorphone, ifosfamide, lorazepam, nesiritide, octreotide, oxaliplatin, tacrolimus, teniposide, thiotepa, zidovudine, zoledronic acid. Y-Site Incompatibility: acyclovir, alemtuzumab, alfentanil, allopurinol, amifostine, amikacin, ampi- amphotericin B 157 cillin, ampicillin/sulbactam, anidulafungin, atropine, azithromycin, aztreonam, benztropine, bivalirudin, bleomycin, bumetanide, butorphanol, calcium chloride, calcium gluconate, cangrelor, carboplatin, caspofungin, cefepime, cefotetan, ceftaroline, chloramphenicol, chlorpromazine, cisplatin, clindamycin, cyanocobalamin, cyclophosphamide, cytarabine, dacarbazine, dantrolene, daptomycin, daunorubicin, dexamethasone, dexmedetomidine, dexrazoxane, diazepam, digoxin, diphenhydramine, dobutamine, docetaxel, dolasetron, dopamine, doxorubicin, doxorubicin liposome, doxycycline, ephedrine, epinephrine, epirubicin, epoetin alfa, eptifibatide, ertapenem, erythromycin, esmolol, etoposide phosphate, famotidine, fenoldopam, filgrastim, fluconazole, fludarabine, fluorouracil, foscarnet, fosphenytoin, ganciclovir, gemcitabine, gentamicin, glycopyrrolate, granisetron, haloperidol, hetastarch, hydralazine, hydrocortisone, hydroxyzine, idarubicin, irinotecan, isoproterenol, ketorolac, labetalol, leucovorin, levofloxacin, lidocaine, linezolid, melphalan, meperidine, mechlorethamine, meropenem, mesna, methotrexate, methylprednisolone, metoclopramide, metoprolol, metronidazole, midazolam, milrinone, mitomycin, mitoxantrone, morphine, mycophenolate, nafcillin, nalbuphine, nicardipine, nitroprusside, norepinephrine, ondansetron, oxacillin, paclitaxel, palonosetron, pamidronate, pancuronium, pantoprazole, papaverine, pemetrexed, penicillin G, pentamidine, pentazocine, phenylephrine, phenytoin, piperacillin/tazobactam, potassium acetate, potassium chloride, prochlorperazine, promethazine, propofol, propranolol, protamine, pyridoxine, quinupristin/dalfopristin, rituximab, rocuronium, sodium acetate, sodium bicarbonate, succinylcholine, telavancin, thiamine, tigecycline, tirofiban, tobramycin, topotecan, trastuzumab, trimethoprim/sulfamethoxazole, vancomycin, vasopressin, vecuronium, verapamil, vinblastine, vincristine, vinorelbine, voriconazole. If administering by way of an current line, flush line with D5W earlier than infusion or use a separate line. Y-Site Compatibility: acyclovir, allopurinol, aminocaproic acid, aminophylline, amiodarone, anidulafungin, argatroban, azithromycin, aztreonam, bumetanide, buprenorphine, busulfan, butorphanol, carboplatin, carmustine, cefazolin, cefepime, cefotaxime, cefotetan, cefoxitin, ceftazidime, ceftriaxone, cefuroxime, chloramphenicol, chlorpromazine, cisatracurium, clindamycin, cyclophosphamide, cyclosporine, cytatabine, dactimomycin, dexamethasone, digoxin, diphenhydramine, docetaxel, doxorubicin liposome, enalaprilat, ephedrine, epinephrine, eptifibatide, ertapenem, etoposide, famotidine, fentanyl, fludarabine, fluorouracil, fosphenytoin, furosemide, ganciclovir, granisetron, heparin, hydrocortisone, hydromorphone, ifosfamide, insulin, ketorolac, lidocaine, linezolid, lorazepam, mannitol, melphalan, meperidine, methotrexate, methylprednisolone, metoclopramide, mitomycin, nafcillin, nesiritide, nitroglycerin, nitroprusside, octreotide, oxaliplatin, paclitaxel, pamidronate, pantoprazole, pemetrexed, pentazocine, pentobarbital, phenobarbital, piperacillin/tazobactam, procainamide, ranitidine, succinylcholine, sufentanil, tacrolimus, telavancin, teniposide, theophylline, thiopental, thiotepa, verapamil, vinblastine, vincristine, zidovudine, zoledronic acid. Replace needle from syringe full of amphotericin B lipid advanced with 5-micron filter needle. Solution Incompatibility: Do not dilute or admix with saline solutions, other medications, or options containing a bacteriostatic agent. Immediately shake vial vigorously for a minimum of 30 seconds till all particulate matter is completely dispersed. Attach the 5-micron filter to the syringe and inject syringe contents into an applicable volume of D5W. Concentration: Final focus of infusion should be 1� 2 mg/mL; a lower concentration (0. Infusion time could also be shortened to 1 hr if patient tolerates infusion without any adverse reactions. May be administered via an in-line filter with pore diameter of no much less than 1 micron. Y-Site Compatibility: acyclovir, amifostine, aminocaproic acid, aminophylline, anidulafungin, argatroban, atropine, azithromycin, bivalirudin, bumetanide, buprenorphine, busulfan, butorphanol, carboplatin, carmustine, cefazolin, cefoxitin, ceftriaxone, cefuroxime, clindamycin, cyclophosphamide, cytarabine, dactinomycin, daptomycin, dexamethasone, dexmedetomidine, diphenhydramine, doxorubicin liposomal, enalaprilat, ephedrine, epinephrine, eptifibatide, ertapenem, esmolol, etoposide, famotidine, fenoldopam, fentanyl, fludarabine, fluorouracil, foscarnet, fosphenytoin, furosemide, granisetron, haloperidol, heparin, hydrocortisone, hydromorphone, ifosfamide, isoproterenol, ketorolac, lidocaine, linezolid, mesna, methotrexate, methylprednisolone, metoprolol, milrinone, mitomycin, nesiritide, nitroglycerin, nitroprusside, octreotide, oxaliplatin, oxytocin, palonosetron, pamidronate, pancuronium, pantoprazole, pemetrexed, pentobarbital, phenobarbital, phenylephrine, piperacillin/tazobactam, potassium acetate, potassium chloride, procainamide, ranitidine, sufentanil, tacrolimus, theophylline, thiopental, thiotepa, tigecycline, trimethoprim/sulfamethoxazole, vasopressin, vincristine, voriconazole, zidovudine, zoledronic acid. Unlabeled Use: Prevention of an infection in sure high-risk patients undergoing cesarean part. Spectrum: Active against: Streptococci, nonpenicillinase-producing staphylococci, Listeria, Pneumococci, Enterococci, Haemophilus influenzae, Escherichia coli, Enterobacter, Klebsiella, Proteus mirabilis, Neisseria meningitidis, N. Action ampicillin 159 Pharmacokinetics Absorption: Moderately absorbed from the duodenum (30� 50%). Distribution: Diffuses readily into physique tissues and Bacterial Meningitis Caused by H. Powder for injection: 125 mg/vial, 250 mg/vial, 500 mg/vial, 1 g/vial, 2 g/vial, 10 g/vial. Obtain a historical past before initiating remedy to determine earlier use and reactions to penicillins or cephalosporins. Assess skin for "ampicillin rash," a nonallergic, boring purple, macular or maculopapular, mildly pruritic rash. Reconstituted oral suspensions retain efficiency for 7 days at room temperature and 14 days if refrigerated. Y-Site Compatibility: acyclovir, alemtuzumab, alprostadil, amifostine, anidulafungin, argatroban, bivalirudin, bleomycin, carboplatin, carmustine, cisplatin, cyclophosphamide, cytarabine, dactinomycin, daptomycin, dexmedetomidine, docetaxel, doxacurium, doxapram, doxorubicin liposome, eptifibatide, etoposide, etoposide phosphate, filgrastim, fludarabine, fluorouracil, foscarnet, gemcitabine, granisetron, hetastarch, ifosfamide, irinotecan, levofloxacin, linezolid, mechlorethamine, melphalan, methotrexate, metronidazole, milrinone, octreotide, oxaliplatin, paclitaxel, palonosetron, pamidronate, pancuronium, pantoprazole, pemetrexed, perphenazine, potassium acetate, propofol, remifentanil, rituximab, rocuronium, sodium acetate, teniposide, thiotepa, tigecycline, tirofiban, trastuzumab, vecuronium, vincristine, vitamin B complex with C, voriconazole, zoledronic acid. Y-Site Incompatibility: If aminoglycosides and penicillins have to be administered concurrently, administer in separate websites a minimum of 1 hr apart, aminophylline, amphotericin B ldl cholesterol, amphotericin B colloidal, amphotericin B lipid advanced, amphotericin B liposome, buprenorphine, caspofungin, chlorpromazine, dantrolene, diazepam, diazoxide, diphenhydramine, dobutamine, dopamine, doxorubicin hydrochloride, doxycycline, epirubicin, fenoldopam, fluconazole, ganciclovir, haloperidol, hydroxyzine, idarubicin, ketamine, lorazepam, midazolam, mitoxantrone, mycophenolate, nafcillin, nesiritide, nicardipine, nitroprusside, ondansetron, papaverine, penicillin G potassium, pentamidine, pentazocine, pentobarbital, phenobarbital, phenytoin, prochlorperazine, promethazine, protamine, quinupristin/dalfopristin, sargramostim, sodium bicarbonate, tranexamic acid, trimethoprim/sulfamethoxazole, verapamil, vinorelbine. Patient/Family Teaching Instruct patient to take medicine around the clock and to end the drug fully as directed, even if feeling better. Caution patient to notify well being care skilled if fever and diarrhea happen, particularly if stool incorporates ampicillin/sulbactam 161 blood, pus, or mucus. Patients with a historical past of rheumatic heart illness or valve replacement need to be taught the importance of using antimicrobial prophylaxis before invasive medical or dental procedures. Advise patients taking oral contraceptives to use an alternate or additional nonhormonal technique of contraception whereas taking ampicillin and until subsequent menstrual interval. Metabolism and Excretion: Ampicillin is variably metabolized by the liver (12� 50%). Binds to bacterial cell wall, leading to cell death; spectrum is broader than that of penicillin. Addition of sulbactam will increase resistance to beta-lactamases, enzymes produced by micro organism that will inactivate ampicillin. Spectrum: Active in opposition to: Streptococci, Pneumococci, Enterococci, Haemophilus influenzae, Escherichia coli, Proteus mirabilis, Neisseria meningitidis, N. Use should be reserved for infections caused by beta-lactamase� producing strains. Interactions Drug-Drug: Probenecidprenal excretion andq Route/Dosage Dosage primarily based on ampicillin part. Obtain a historical past before initiating therapy to determine earlier use of, and reactions to , penicillins or cephalosporins. Discontinue the drug and notify the physician or different health care professional instantly if these happen. May cause transientpestradiol, complete conjugated estriol, estriol-glucuronide, or conjugated estrone in pregnant ladies. Stability of answer varies from 2� eight hr at room temperature or 3� 72 hr if refrigerated, depending on concentration and diluent. Concentration: Final focus of infusion should be 3� forty five mg of ampicillin/sulbactam per mL. Y-Site Compatibility: alemtuzumab, amifostine, aminocaproic acid, anidulafungin, argatroban, azithromycin, bivalirudin, bleomycin, cangrelor, carboplatin, carmustine, cisplatin, cyclophosphamide, cytarabine, dactinomycin, daptomycin, dexmedetomidine, dexrazoxane, docetaxel, doxorubicin liposomal, eptifibatide, etoposide, etoposide phosphate, fenoldopam, filgrastim, fludarabine, fluorouracil, foscarnet, fosphenytoin, granisetron, hydromorphone, ifosfamide, irinotecan, leucovorin, levofloxacin, linezolid, mesna, methotrexate, metronidazole, milrinone, mitomycin, octreotide, oxaliplatin, paclitaxel, palonosetron, pamidronate, pancuronium, pantoprazole, pemetrexed, potassium acetate, remifentanil, rituximab, rocuronium, sodium acetate, televancin, teniposide, thiotepa, tigecycline, tirofiban, trastuzumab, vecuronium, vinblastine, vincristine, voriconazole, zoledronic acid. Y-Site Incompatibility: acyclovir, amiodarone, amphotericin B colloidal, amphotericin B lipid complex, amphotericin B liposome, azathioprine, caspofungin, chlorpromazine, ciprofloxacin, dacarbazine, dantrolene, daunorubicin, diazepam, diazoxide, dobutamine, dolasetron, doxorubicin, doxycycline, epirubicin, ganciclovir, haloperidol, hydralazine, hydrocortisone sodium succinate, hydroxyzine, idarubicin, lansoprazole, lorazepam, mechlorethamine, methylprednisolone sodium succinate, midazolam, mitoxantrone, mycophenolate, nesiritide, nicardipine, ondansetron, papaverine, pentamidine, pentazocine, phenytoin, prochlorperazine, promethazine, protamine, quinupristin/dalfopristin, sargramostim, topotecan, tranexamic acid, trimethoprim/sulfamethoxazole, verapamil, vinorelbine. If aminoglycosides and penicillins should be given concurrently, administer in separate sites at least 1 hr apart. Rep: Advise sufferers taking oral contraceptives to use an alternative or further nonhormonal technique of anastrozole 163 contraception whereas taking ampicillin/sulbactam and until subsequent menstrual interval. Length of time for full decision is decided by the organism and web site of infection. Availability (generic available) Indications Adjuvant therapy of postmenopausal hormone receptor-positive early breast most cancers. Initial therapy in ladies with postmenopausal hormone receptor-positive or hormone receptor unknown, domestically advanced, or metastatic breast cancer. Advanced postmenopausal breast most cancers in ladies with disease development regardless of tamoxifen remedy. Advise affected person to read the Patient Information leaflet earlier than starting and with each Rx refill; adjustments could happen. Inform affected person of potential for opposed reactions, and advise affected person to notify well being care professional immediately if allergic reactions (swelling of the face, lips, tongue, and/or throat, issue in swallowing and/or breathing), liver issues (general feeling of not being nicely, yellowing of skin or whites of eyes, ache on the proper side of abdomen), skin reactions (lesions, ulcers, or blisters), or chest pain occurs.
Allegra 120 mg overnight delivery
Distribution: Widely distributed all through extracellular fluid; cross the placenta; small amounts enter breast milk allergy treatment while nursing cheap allegra 120 mg online. Postdistribution peak happens 30 min after the end of a 30min infusion and 15 min after the end of a 1-hr infusion allergy questions generic allegra 120 mg without prescription. Subsequent doses/intervals based mostly on blood stage monitoring and renal perform assessment. Possible respiratory paralysis after inhalation anesthetics or neuromuscular blocking brokers. Inhaln (Adults and Children 6 yr): Nebulizer solution- 300 mg twice every day for 28 days, then off for 28 days, then repeat cycle; powder for inhalation- Inhale contents of four 28-mg capsules twice daily for 28 days, then off for 28 days, then repeat cycle. Premixed injection: forty mg/50 mL, 60 mg/50 mL, 60 mg/100 mL, 70 mg/50 mL, eighty mg/50 mL, eighty mg/100 mL, 90 mg/100 mL, 100 mg/50 mL, one hundred mg/100 mL, one hundred twenty mg/100 mL. In mixture with: different topical antibiotics or anti-inflammatory agents for pores and skin, ear, and eye infections. Evaluate eighth cranial nerve operate by audiometry before and throughout remedy. Eighth cranial nerve dysfunction is associated with persistently elevated peak aminoglycoside ranges. Monitor consumption and output and day by day weight to assess hydration status and renal operate. Assess for indicators of superinfection (fever, higher respiratory infection, vaginal itching or discharge, increasing malaise, diarrhea). May causepserum calcium, magnesium, potassium, and sodium concentrations (streptomycin and tobramycin). Nebulizer so- Potential Nursing Diagnoses Risk for an infection (Indications) Disturbed sensory perception (auditory) (Side Effects) Canadian drug name. Preoperative Bowel Prep: Neomycin is normally used along side erythromycin, a low-residue food regimen, and a cathartic or enema. Y-Site Compatibility: acyclovir, aldesleukin, alemtuzumab, alfentanil, amifostine, aminophylline, amiodarone, anidulafungin, argatroban, ascorbic acid, atropine, aztreonam, benztropine, bivalirudin, bleomycin, bumetanide, buprenorphine, butorphanol, calcium chloride, calcium gluconate, cangrelor, carboplatin, carmustine, caspofungin, chloramphenicol, chlorpromazine, cisatracurium, cisplatin, clindamycin, cyanocobalamin, cyclophosphamide, cyclosporine, cytarabine, dactinomycin, daptomycin, dexamethasone, dexmedetomidine, dexrazoxane, digoxin, diltiazem, diphenhydramine, dobutamine, docetaxel, dolasetron, dopamine, doripenem, doxorubicin hydrochloride, doxycycline, enalaprilat, ephedrine, epinephrine, epirubicin, epoetin alfa, eptifibatide, ertapenem, erythromycin, esmolol, etoposide, etoposide phosphate, famotidine, fentanyl, filgrastim, fluconazole, fludarabine, fluorouracil, foscarnet, fosphenytoin, furosemide, gemcitabine, gentamicin, glycopyrrolate, granisetron, hydrocortisone, hydromorphone, idarubicin, ifosfamide, imipenem/cilastatin, irinotecan, isoproterenol, ketamine, ketorolac, labetalol, leucovorin, levofloxacin, lidocaine, linezolid, lorazepam, magnesium sulfate, mannitol, mechlorethamine, melphalan, meperidine, mesna, methotrexate, methylprednisolone, metoclopramide, metoprolol, metronidazole, midazolam, milrinone, mitoxantrone, morphine, multivitamins, mycophenolate, nalbuphine, naloxone, nicardipine, nitroglycerin, nitroprusside, norepinephrine, octreotide, ondansetron, oxaliplatin, oxytocin, paclitaxel, palonosetron, pamidronate, pancuronium, papaverine, pemetrexed, pentazocine, perphenazine, phenobarbital, phenylephrine, phytonadione, posaconazole, potassium acetate, po- tassium chloride, procainamide, prochlorperazine, promethazine, propranolol, protamine, pyridoxime, quinupristin/dalfopristin, ranitidine, remifentanil, rituximab, rocuronium, sargramostim, sodium acetate, sodium bicarbonate, streptokinase, succinylcholine, sufentanil, tacrolimus, teniposide, theophylline, thiamine, thiotepa, tigecycline, tirofiban, tobramycin, tolazoline, topotecan, vancomycin, vasopressin, vecuronium, verapamil, vinblastine, vincristine, vinorelbine, voriconazole, warfarin, zidovudine, zoledronic acid. Y-Site Incompatibility: allopurinol, amophotericin B cholesteryl, amphotericin B colloidal, amphotericin B lipid advanced, amphotericin B liposome, azathioprine, dacarbazine, dantrolene, diazepam, diazoxide, folic acid, ganciclovir, ibuprofen lysine, indomethacin, mitomycin, pentamidine, pentobarbital, phenytoin, propofol, trastuzumab, trimethoprim/ sulfamethoxazole. Y-Site Incompatibility: allopurinol, amphotericin B chloesteryl, amphotericin B colloidal, amphotericin B lipid advanced, amphotericin B liposome, azathioprine, cangrelor, cefotetan, dacarbazine, dantrolene, diazepam, diazoxide, folic acid, ganciclovir, idarubicin, indomethacin, methotrexate, pemetrexed, pentamidine, pentobarbital, phenytoin, propofol, trimethoprim/sulfamethoxazole, warfarin. Y-Site Incompatibility: allopurinol, amphotericin B cholesteryl, amphotericin B colloidal, amphotericin B lipid complicated, amphotericin B liposome, azathioprine, cangrelor, cefazolin, cefotetan, ceftriaxone, dacarbazine, dantrolene, dexamethasone, diazepam, diazoxide, folic acid, ganciclovir, hetastarch, indomethacin, oxacillin, pemetrexed, pentamidine, pentobarbital, phenytoin, piperacillin/tazobactam, propofol, sargramostim, trimethoprim/ sulfamethoxazole. Y-Site Compatibility: acyclovir, aldesleukin, alemtuzumab, alfentanil, alprostadil, alteplase, amifostine, aminophylline, amiodarone, anidulafungin, argatroban, ascorbic acid, atropine, aztreonam, benztropine, bivalirudin, bleomycin, bumetanide, buprenorphine, butorphanol, calcium chloride, calcium gluconate, carboplatin, carmustine, caspofungin, chloramphenicol, chlorpromazine, ciprofloxacin, cisatracurium, cisplatin, clindamycin, cyanocobalamin, cyclophosphamide, cyclosporine, cytarabine, dactinomycin, daptomycin, daunorubicin hydrochloride, dexmedetomidine, dexrazoxane, digoxin, diltiazem, dimenhydrinate, diphenhydramine, dobutamine, docetaxel, dolasetron, dopamine, doripenem, doxorubicin hydrochloride, doxorubicin liposome, doxycycline, enalaprilat, ephedrine, epinephrine, epirubicin, epoetin alfa, ertapenem, esmolol, etoposide, etoposide phosphate, famotidine, fenoldopam, fentanyl, filgrastim, fluconazole, fludarabine, fluorouracil, foscarnet, furosemide, gemcitabine, gentamicin, glycopyrrolate, granisetron, hydromorphone, idarubicin, ifosfamide, Patient/Family Teaching Instruct affected person to report signs of hypersensitivity, tinnitus, vertigo, hearing loss, rash, dizziness, or issue urinating. Teach patients with a history of rheumatic coronary heart disease or valve replacement the significance of utilizing antimicrobial prophylaxis before invasive medical or dental procedures. Patient ought to assess skin and inform health care professional if skin irritation develops or infection worsens. Inhaln: Instruct patient to take inhalation twice daily as near 12 hr aside as attainable; not 6 hr apart. Solution is colorless to pale yellow and should darken with age with out effecting quality. Instruct patient on a number of therapies to take others first and use tobramycin last. Tobramycin-induced bronchospasm may be decreased if tobramycin is run after bronchodilators. Instruct affected person to sit or stand upright throughout inhalation and breathe usually via mouthpiece of nebulizer. Advise affected person to disinfect the nebulizer components (except tubing) by boiling them in water for a full 10 minutes every different treatment day. Neuro: ataxia, involuntary movement, paresthesia, peripheral neuropathy, poor coordination, tremor. Premixed infusion (Nexterone): 150 mg/100 mL D5W (does not include polysorbate 80 or benzyl alcohol), 360 mg/200 mL D5W (does not comprise polysorbate 80 or benzyl alcohol). If arrhythmia recurs, a small loading infusion of 150 mg over 10 min should be given; as nicely as, the speed of the maintenance infusion could beq Conversion. Assess pacing and defibrillation threshold in patients with pacemakers and implanted defibrillators at starting and periodically throughout therapy. Assess for indicators of pulmonary toxicity (rales/crackles, decreased breath sounds, pleuritic friction rub, fatigue, dyspnea, cough, wheezing, pleuritic ache, fever, hemoptysis, hypoxia). Monitor chest x-ray every 3� 6 mo during remedy to detect diffuse interstitial modifications or alveolar infiltrates. Hypotension often happens throughout first several hours of therapy and is said to rate of infusion. Ophthalmic exams must be carried out earlier than and regularly during remedy and whenever visual adjustments (photophobia, halos around lights, decreased acuity) occur. Lethargy; weight acquire; edema of the palms, feet, and periorbital region; and funky, pale skin counsel hypothyroidism and will require decrease in dose or discontinuation of therapy and thyroid supplementation. Tachycardia; weight loss; nervousness; sensitivity to warmth; insomnia; and warm, flushed, moist pores and skin recommend hyperthyroidism and should require discontinuation of remedy and remedy with antithyroid agents. Lab Test Considerations: Monitor liver and thyroid capabilities before and each 6 mo during therapy. Thyroid operate abnormalities are common, however clinical thyroid dysfunction is rare. If liver function studies are 3 instances regular or double in sufferers with elevated baseline levels or if hepatomegaly occurs, dose must be decreased. Monitor serum potassium, calcium, and magnesium prior to beginning and periodically during therapy. Hypokalemia, hypocalcemia, and/or hypomagnesemia maypeffectiveness or cause extra arrhythmias; correct levels earlier than starting therapy. Before administering, have second practitioner check unique order, dose calculations, and infusion pump settings. Infusions exceeding 2 hr have to be administered in glass or polyolefin bottles to stop adsorption. Continuous Infusion: Diluent: Dilute 900 mg (18 mL) of amiodarone in 500 mL of D5W. Concentration might vary from 1� 6 mg/mL (concentrations 2 m g/mL have to be administered through central venous catheter). Rate: Infuse at a rate of 1 mg/min for the first 6 hr, then lower infusion fee to 0. Y-Site Compatibility: alemtuzumab, alfentanil, amikacin, amphotericin B lipid complicated, anidulafungin, atracurium, atropine, bleomycin, buprenorphine, busulfan, butorphanol, calcium chloride, cangrelor, carboplatin, carmustine, caspofungin, ceftaroline, chlorpromazine, ciprofloxacin, cisatracurium, cisplatin, clindamycin, cyclophosphamide, dacarbazine, dactinomycin, daptomycin, daunorubicin, dexmedetomidine, dexrazoxane, diltiazem, diphenhydramine, docetaxel, dolasetron, dopamine, doripenem, doxycycline, droperidol, enalaprilat, ephedrine, epinephrine, erythromycin lactobionate, esmolol, etoposide, etoposide phosphate, famotidine, fenoldopam, fluconazole, gemcitabine, gentamicin, glycopyrrolate, granisetron, haloperidol, hydralazine, hydromorphone, idarubicin, ifosfamide, irinotecan, isoproterenol, ketamine, labetalol, lidocaine, linezolid, lorazepam, mannitol, meperidine, mesna, metoclopramide, metoprolol, metronidazole, midazolam, milrinone, mitoxantrone, morphine, moxifloxacin, mycophenolate, nafcillin, nalbuphine, naloxone, nesiritide, nicardipine, nitroglycerin, octreotide, ondansetron, oxaliplatin, palonosetron, pancuronium, pemetrexed, penicillin amitriptyline 145 G potassium, pentamidine, pentazocine, phenylephrine, procainamide, prochlorperazine, promethazine, propranolol, quinupristin/dalfopristin, remifentanil, rifampin, rocuronium, streptozocin, succinylcholine, sufentanil, tacrolimus, teniposide, theophylline, tirofiban, tobramycin, topotecan, vancomycin, vasopressin, vecuronium, vinblastine, vincristine, vinorelbine, voriconazole, zoledronic acid. Y-Site Incompatibility: acyclovir, allopurinol, amifostine, aminocaproic acid, aminophylline, ampicillin, ampicillin/sulbactam, azithromycin, bivalirudin, cefotaxime, cefotetan, ceftazidime, chloramphenicol, cytarabine, dantrolene, dexamethasone, diazepam, digoxin, doxorubicin, ertapenem, fludarabine, fluorouracil, foscarnet, fosphenytoin, ganciclovir, heparin, hydrocortisone, imipenem-cilastatin, ketorolac, leucovorin, levofloxacin, mechlorethamine, melphalan, meropenem, methotrexate, micafungin, mitomycin, paclitaxel, pentobarbital, phenobarbital, phenytoin, piperacillin/tazobactam, potassium acetate, potassium phosphates, ranitidine, sodium acetate, sodium bicarbonate, sodium phosphates, thiopental, thiotepa, tigecycline, trimethoprim/sulfamethoxazole, verapamil. Instruct patient to notify well being care skilled of A medication routine earlier than treatment or surgical procedure. Advise patient to notify health care skilled if indicators and signs of thyroid dysfunction occur. Advise feminine affected person to notify health care skilled if being pregnant is deliberate or suspected and to keep away from breast feeding during therapy.
Trusted 180 mg allegra
Cefotetan (generic available) Powder for injection: 1 g/vial allergy shots allegra 180 mg on line, 2 g/vial allergy symptoms chest tightness discount 120 mg allegra amex, 10 g/vial. Cefoxitin (generic available) Powder for injection: 1 g/vial, 2 g/vial, 10 g/vial. Persons with a adverse historical past of penicillin sensitivity should have an allergic response. Keep epinephrine, an antihistamine, and resuscitation tools close by in the event of an anaphylactic response. Cefotetan- monitor prothrombin time and assess affected person for bleeding (guaiac stools; check for hematuria, bleeding gums, ecchymosis) day by day in high-risk sufferers; may cause hypoprothrombinemia. May hardly ever trigger leukopenia, neutropenia, agranulocytosis, thrombocytopenia, and eosinophilia. If aminoglycosides are administered concurrently, administer in separate websites if possible, at least 1 hr aside. Y-Site Incompatibility: alemtuzumab, amiodarone, amphotericin B colloidal, amphotericin B liposome, azathioprine, caspofungin, chlorpromazine, dantrolene, daunorubicin hydrochloride, diazepam, diphenhydramine, dobutamine, dolasetron, doxorubicin hydrochloride, doxycycline, epirubicin, erythromycin, esmolol, ganciclovir, gentamicin, haloperidol, hydralazine, hydroxyzine, idarubicin, indomethacin, labetalol, mycophenolate, pantoprazole, papaverine, pemetrexed, pentamidine, pentazocine, pentobarbital, phenobarbital, phenytoin, prochlorperazine, promethazine, protamine, quinupristin/dalfopristin, sodium bicarbonate, tobramycin, trastuzumab, trimethoprim/sulfamethoxazole, vinorelbine. Y-Site Incompatibility: alemtuzumab, azathioprine, caspofungin, chlorpromazine, dantrolene, daunorubicin hydrochloride, diazepam, diphenhydramine, dobutamine, dolasetron, doxorubicin hydrochloride, doxycycline, epirubicin, erythromycin, fenoldopam, filgrastim, ganciclovir, haloperidol, hydralazine, hydroxyzine, idarubicin, insulin, labetalol, levofloxacin, methylprednisolone, mitoxantrone, mycophenolate, papaverine, pemetrexed, pentamidine, pentazocine, pentobarbital, phenobarbital, phenytoin, prochlorperazine, promethazine, protamine, quinupristin/dalfopristin, sodium bicarbonate, trastuzumab, trimethoprim/sulfamethoxazole, vinorelbine. C Cefoxitin Intermittent Infusion: Diluent: Reconstituted solution could also be additional diluted in 50� 100 mL of D5W, D10W, 0. Y-Site Compatibility: acetaminophen, acyclovir, alfentanil, amifostine, aminocaproic acid, aminophylline, amphotericin B lipid advanced, amphotericin B liposome, anidulafungin, argatroban, ascorbic acid, atropine, azithromycin, aztreonam, benztropine, bivalirudin, bleomycin, bumetanide, buprenorphine, butorphanol, calcium chloride, calcium gluconate, cangrelor, carboplatin, carmustine, cefazolin, cefotaxime, cefotetan, ceftazidime, ceftriaxone, cefuroxime, chloramphenicol, cisplatin, clindamycin, cyanocobalamin, cyclophosphamide, cyclosporine, cytarabine, dacarbazine, dactinomycin, daptomycin, dexamethasone, dexmedetomidine, dexrazoxane, digoxin, diltiazem, docetaxel, dopa- Cefuroxime Intermittent Infusion: Diluent: Solution may be additional diluted in 50� a hundred mL of 0. Y-Site Compatibility: acyclovir, alfentanil, allopurinol, amifostine, aminocaproic acid, aminophylline, amphotericin B lipid advanced, amphotericin B liposome, anidulafungin, argatroban, ascorbic acid, atropine, aztreonam, benztropine, bivalirudin, bleomycin, bumetanide, buprenorphine, butorphanol, calcium gluconate, cangrelor, carboplatin, carmus- Canadian drug name. Y-Site Incompatibility: alemtuzumab, azathioprine, calcium chloride, caspofungin, chlorpromazine, dantrolene, daunorubicin hydrochloride, dexamethasone, diazepam, diphenhydramine, dobutamine, doxorubicin hydrochloride, doxycycline, epirubicin, filgrastim, ganciclovir, haloperidol, hydralazine, hydroxyzine, idarubicin, labetalol, magnesium sulfate, midazolam, mitoxantrone, mycophenolate, nicardipine, papaverine, pentamidine, pentazocine, pentobarbital, phenobarbital, phenytoin, prochlorperazine, promethazine, protamine, quinupristin/dalfopristin, sodium bicarbonate, trimethoprim/sulfamethoxazole, vinorelbine. Caution patients that concurrent use of alcohol with cefotetan could cause a disulfiram-like response (abdominal cramps, nausea, vomiting, headache, hypotension, palpitations, dyspnea, tachycardia, sweating, flushing). Alcohol and alcohol-containing drugs should be avoided during and for several days after therapy. Indications Treatment of the following infections brought on by susceptible organisms: Skin and pores and skin construction infections (not cefixime), Urinary and gynecologic infections (not cefdinir, cefditoren, or ceftibuten), Respiratory tract infections (not cefdinir, cefditoren, or ceftibuten). Spectrum: Similar to that of second-generation cephalosporins, but exercise in opposition to staphylococci is less, whereas activity in opposition to gram-negative pathogens is bigger, even for organisms immune to first- and second-generation agents. Notable is increased motion towards: Enterobacter, Haemophilus influenzae, Escherichia coli, Klebsiella pneumoniae, Neisseria gonorrhoeae, Citrobacter, Morganella, Proteus, Providencia, Serratia, Moraxella catarrhalis, Borrelia burgdorferi. Some agents have activity against anaerobes, including Bacteroides fragilis (cefotaxime, ceftriaxone). Ceftibuten is nicely absorbed after oral administration; cefixime 40� 50% absorbed after oral administration (oral suspension); cefdinir 16� 25% absorbed after oral administration. Metabolism and Excretion: Cefdinir, ceftazidime, and cefditoren- 85% excreted in urine. Ceftibuten, ceftriaxone, and cefotaxime- partly metabolized and partly excreted in the urine. Hemat: agranulocytosis, bleeding, eosinophilia, hemolytic anemia, lymphocytosis, neutropenia, thrombocytopenia, thrombocytosis. Perioperative prophylaxis- 1 g 30� 90 min earlier than initial incision (one-time dose). Perioperative prophylaxis- 1 g 30� a hundred and twenty min earlier than initial incision (single dose). Cefotaxime (generic available) Powder for injection: 500 mg/vial, 1 g/vial, 2 g/vial, 10 g/vial, 20 g/vial. Ceftazidime (generic available) Powder for injection: 500 mg/vial, 1 g/vial, 2 g/vial, 6 g/vial. Pedi: Assess newborns for jaundice and hyperbilirubinemia earlier than making choice to use ceftriaxone (should not be utilized in jaundiced or hyperbilirubinemic neonates). Monitor prothrombin time and assess affected person for bleeding (guaiac stools; check for hematuria, bleeding gums, ecchymosis) every day in patients receiving cefditoren, as this agentmay cause hypoprothrombinemia. May hardly ever cause leukopenia, neutropenia, agranulocytosis, thrombocytopenia, eosinophilia, lymphocytosis, and thrombocytosis. C Potential Nursing Diagnoses Ceftriaxone (generic available) Powder for injection: 250 mg/vial, 500 mg/vial, 1 g/ vial, 2 g/vial, 10 g/vial. Risk for infection (Indications, Side Effects) Diarrhea (Adverse Reactions) Deficient data, related to medication routine (Patient/Family Teaching) Canadian drug name. Administer cefpodoxime tablets with meals to enhance absorption (suspension could additionally be administered with out regard to meals. Cefixime oral suspension should be used to treat otitis media (results in greater peak concentrations than tablets). Do not administer cefpodoxime within 2 hr before or after an H2 receptor antagonist. Y-Site Compatibility: acyclovir, alfentanil, alprostadil, amifostine, aminophylline, aminocaproic acid, amphotericin B lipid advanced, anidulafungin, argatroban, ascorbic acid, atropine, aztreonam, benztropine, bivalirudin, bleomycin, bumetanide, bupre- norphine, butorphanol, calcium chloride, calcium gluconate, cangrelor, carboplatin, carmustine, cefotetan, cefoxitin, ceftriaxone, cefuroxime, cisplain, clindamycin, cyanocobalamin, cyclophosphamide, cyclosporine, cytarabine, dactinomycin, daptomycin, dexamethasone, dexmedetomidine, dexrazoxane, digoxin, diltiazem, dimenhydrinate, docetaxel, dopamine, doxorubicin liposomal, doxycycline, enalaprilat, ephedrine, epinephrine, epirubicin, epoetin alfa, eptifibatide, erythromycin, esmolol, etoposide, etoposide phosphate, famotidine, fenoldopam, fentanyl, fludarabine, fluorouracil, folic acid, foscarnet, fosphenytoin, furosemide, glycopyrrolate, granisetron, heparin, hetastarch, hydrocortisone, hydromorphone, ifosfamide, imipenem/cilastatin, indomethacin, insulin, isoproterenol, ketamine, ketorolac, leucovorin, lidocaine, linezolid, lorazepam, magnesium sulfate, mannitol, mechlorethamine, melphalan, meperidine, mesna, methotrexate, metoclopramide, metoprolol, metronidazole, midazolam, milrinone, morphine, multivitamins, nafcillin, nalbuphine, naloxone, nesiritide, nicardipine, nitroglycerin, nitroprusside, norepinephrine, octreotide, ondansetron, oxacillin, oxaliplatin, oxytocin, paclitaxel, palonosetron, pamidronate, pancuronium, penicillin G, perphenazine, phenylephrine, phytonadione, potassium acetate, potassium chloride, procainamide, propofol, propranolol, pyridoxime, ranitidine, remifentanil, rituximab, rocuronium, sargramostim, sodium acetate, streptokinase, succinylcholine, sufentanil, tacrolimus, teniposide, theophylline, thiamine, thiotepa, tigecycline, tirofiban, vasopressin, verapamil, vinblastine, vinorelbine, voriconazole, zoledronic acid. Y-Site Incompatibility: alemtuzumab, allopurinol, amiodarone, amphotericin B liposome, azathioprine, caspofungin, cefazolin, ceftazidime, chloramphenicol, chlorpromazine, dantrolene, daunorubicin hydrochloride, diazepam, diphenhydramine, dobutamine, dolasetron, doxorubicin hydrochloride, filgrastim, ganciclovir, gemcitabine, haloperidol, hydralazine, hydroxyzine, idarubicin, irinotecan, labetalol, methylprednisolone, mitoxantrone, mycophenolate, pantoprazole, papaverine, pemetrexed, pentamidine, pentazocine, pentobarbital, phenobarbital, phenytoin, prochlorperazine, promethazine, protamine, quinupristin/dalfopristin, sodium bicarbonate, trastuzumab, trimethoprim/sulfamethoxazole, vecuronium. Ceftazidime Intermittent Infusion: Diluent: Reconstituted resolution may be additional diluted in no less than 1 g/10 mL of 0. Y-Site Compatibility: acyclovir, alfentanil, allopurinol, amifostine, aminocaproic acid, aminophylline, amphotericin B lipid complicated, anakinra, anidulafungin, argatroban, atropine, aztreonam, benztropine, bivalirudin, bleomycin, bumetanide, buprenorphine, butorphanol, calcium gluconate, cangrelor, carboplatin, carmustine, cefazolin, cefotetan, cefoxitin, ceftriaxone, cefuroxime, ciprofloxacin, cisplatin, clindamycin, cyanocobalamin, cyclophosphamide, cyclosporine, cytarabine, dacarbazine, dactinomycin, daptomycin, dexamethasone, dexmedetomidine, dexrazoxane, digoxin, diltiazem, dimenhydrinate, docetaxel, dolasetron, dopamine, enalaprilat, ephedrine, epinephrine, epoetin alfa, eptifibatide, esmolol, etoposide, etoposide phosphate, famotidine, fenoldopam, fentanyl, filgrastim, fludarabine, fluorouracil, folic acid, foscarnet, fosphenytoin, furosemide, gemcitabine, glycopyrrolate, granisetron, heparin, hetastarch, hydrocortisone, hydromorphone, ibuprofen, ifosfamide, imipenem/cilastatin, indomethacin, insulin, irinotecan, isoproterenol, ketamine, ketorolac, labetalol, leucovorin calcium, levofloxacin, lidocaine, linezolid, lorazepam, magnesium sulfate, mannitol, mechlorethamine, melphalan, meperidine, mesna, methotrexate, methylprednisolone, metoclopramide, metoprolol, metronidazole, milrinone, mitomycin, morphine, multivitamins, nafcillin, nalbuphine, naloxone, nesiritide, nitroglycerin, norepinephrine, octreotide, oxacillin, oxaliplatin, oxytocin, paclitaxel, palonosetron, pamidronate, pancuronium, pantoprazole, penicillin G, phenobarbital, phenylephrine, phytonadione, potassium acetate, potassium chloride, procainamide, propranolol, pyridoxine, ranitidine, remifentanil, rituximab, rocuronium, sodium acetate, sodium bicarbonate, sodium citrate, streptokinase, succinylcholine, sufentanil, tacrolimus, telavancin, teniposide, thiotepa, tigecycline, tirofiban, trastuzumab, vasopressin, vecuronium, vinblastine, vincristine, vinorelbine, voriconazole, zidovudine, zoledronic acid. Y-Site Incompatibility: acetylcysteine, alemtuzumab, amiodarone, amphotericin B liposome, ascorbic acid, azathioprine, calcium chloride, caspofungin, cefotaxime, chloramphenicol, chlorpromazine, dantrolene, daunorubicin hydrochloride, diazepam, diphenhydramine, doxorubicin hydrochloride, doxorubicin liposome, doxycycline, epirubicin, ganciclovir, haloperidol, hydralazine, hydroxyzine, idarubicin, midazolam, mitoxantrone, mycophentolate, nitroprusside, papaverine, pemetrexed, pentamidine, pentazocine, phenytoin, prochlorperazine, promethazine, protamine, quinupristin/dalfopriatin, thiamine, topotecan, trimethoprim/ sulfamethoxazole, verapamil, warfarin. Y-Site Compatibility: acetaminophen, acyclovir, alfentanil, allopurinol, amifostine, aminocaproic acid, aminophylline, amiodarone, amphotericin B lipid advanced, amphotericin B liposome, anidulafungin, argatroban, atropine, aztreonam, benztropine, bivalirudin, bumetanide, buprenorphine, butorphanol, cangrelor, carboplatin, carmustine, cefazolin, cefotaxime, cefotetan, cefoxitin, ceftazidime, cefuroxime, cisatracurium, cisplatin, cyanocobalamin, cyclophosphamide, cyclosporine, cytarabine, dactinomycin, daptomycin, dexamethasone, dexmedetomidine, digoxin, diltiazem, docetaxel, dopamine, doxorubicin liposome, doxycycline, enalaprilat, ephedrine, epinephrine, epoetin alfa, epitifibatide, erythromycin, esmolol, etoposide, etoposide phosphate, fenoldopam, fentanyl, fludarabine, fluorouracil, folic acid, foscarnet, fosphenytoin, furosemide, gemcitabine, glycopyrrolate, granisetron, heparin, hetastarch, hydrocortisone, hydromorphone, ifosfamide, indomethacin, insulin, isoproterenol, ketorolac, levofloxacin, lidocaine, linezolid, lorazepam, mannitol, mechlorethamine, melphalan, meperidine, methotrexate, methylprednisolone, metoclopramide, metoprolol, metronidazole, midazolam, milrinone, morphine, multivitamins, nafcillin, nalbuphine, naloxone, nesiritide, nicardipine, nitroglycerin, nitroprusside, norepinephrine, octreotide, oxacillin, oxaliplatin, oxytocin, paclitaxel, palonosetron, pamidronate, pantoprazole, pemetrexed, penicillin G, phenobarbital, phenylephrine, phytonadione, potassium acetate, potassium chloride, procainamide, propranolol, pyridoxine, ranitidine, remifentanil, rituxumab, rocuronium, sargramostim, sodium acetate, sodium bicarbonate, streptokinase, succinylcholine, sufentanil, tacrolimus, telavancin, teniposide, theophylline, thiamine, thiotepa, tigecycline, tirofiban, topotecan, trastuzumab, vasopressin, vecuronium, verapamil, vinblastine, vincristine, voriconazole, warfarin, zidovudine, zoledronic acid. Action Acts as a tyrosine kinase inhibitor, inhibiting anaplastic lymphoma kinase as nicely as different kinases, leading to decreased progress of certain malignant cell strains. Pedi: Instruct dad and mom or caregivers to use calibrated measuring system with liquid preparations. Advise patient to report indicators of superinfection (furry overgrowth on the tongue, vaginal itching or discharge, loose or foul-smelling stools) and allergy. Instruct patient to notify health care skilled if rash, fever and diarrhea develop, particularly if stool contains blood, pus, or mucus. Drug-Food: Grapefruit/grapefruit juiceqblood ranges and the risk of toxicity; concurrent ingestion must be averted. If clinically significant bradycardia requiring intervention or lifethreatening bradycardia in patients taking concurrent medication recognized to trigger bradycardia or a drugs known to cause hypotension happens, withhold ceritinib until restoration to asymptomatic bradycardia or a heart price 60 bpm. If concurrent treatment can be adjusted or discontinued, resume ceritinib with a 150 mg dose discount and frequent monitoring. If life-threatening bradycardia occurs in sufferers not taking medicines recognized to cause bradycardia or hypotension, discontinue ceritinib completely. If extreme or insupportable nausea, vomiting, or diarrhea continue despite optimum antiemetic or antidiarrheal remedy, withhold ceritinib until improved; then resume with a one hundred fifty mg dose discount.
180 mg allegra fast delivery
Gout Gout is a disorder within the metabolism of purine (a component of nucleic acids) during which a rise in the blood level of uric acid leads to allergy shots going on vacation allegra 180 mg buy fast delivery the deposition of uric acid crystals within the joints allergy testing labcorp order allegra 120 mg with visa, cartilage, and kidney. Several inherited enzyme defects could cause overproduction of uric acid (primary gout). In secondary gout, hyperuricemia can be brought on by an overproduction of uric acid, which in flip could additionally be brought on by elevated turnover of nucleic acids. Effusion with tophi deposits on the first, fourth, and fifth metatarsophalangeal joints. Clumps of urate crystals (tophi) type along the margins of the articular cortex and erode the underlying bone, leading to small, sharply marginated, punchedout defects at the joint margins of the small bones of the hand and foot. In superior disease, extreme harmful lesions are related to joint area narrowing and even fibrous ankylosis. Continued deposition of urate crystals within the periarticular tissues causes the event of the attribute giant, lumpy delicate tissue swellings representing gouty tophi. In addition to the first metatarsophalangeal joints, other frequent websites of tophi are the ear, the olecranon bursa, and the insertion of the Achilles tendon. Severe joint effusion and periarticular swelling of the proximal interphalangeal joint of the finger. Nonradiopaque pure uric acid stones could be demonstrated only on excretory urograms, where they appear as filling defects in the pelvicalyceal system or ureter. Stones containing the calcium salts of uric acid can be detected on plain abdominal radiographs, on which they appear radiopaque. Untreated gout may result in decreased renal excretion due to renal injury resulting from crystal deposits in the interstitial tissue. Eventually, this process causes obstruction of the renal tubules and renal failure. Destruction of bone, adopted by a reparative process, ends in weakened, deformed, and thickened bony structures that are inclined to fracture simply. The cystlike lesions have skinny sclerotic margins and attribute overhanging edges. Massive deposition of calcium in a long-standing tophaceous lesion concerning the elbow. The reparative process could begin early and will be the distinguished feature, usually involving multiple bones. Increased trabeculation, which is most prominent at the periphery of the bone, produces a rim of thickened cortex and a picture-frame look. Uniform dense sclerosis of one or more vertebral bodies (ivory vertebrae) could occur. In the lengthy bones, the harmful part nearly invariably begins at one finish of the bone and extends along the shaft for a variable distance before ending in a typical, sharply demarcated, V-shaped configuration (blade of grass appearance). During the reparative course of, the sclerosis appears as elevated irregular cortical thickening and enlargement. The downward thrust of the heavy head on the softened bone of the cranium base may compress the brainstem and trigger numerous cranial nerve deficits. Expansion and distortion of softened vertebral our bodies, sometimes with pathologic fractures, might compress the spinal cord and produce nerve root deficits. The chilly spot represents the preliminary damaging part, whereas the new spot is a results of the reparative course of. Sometimes anti-inflammatory medicine scale back the irritation brought on by cell breakdown. Diffuse sclerosis with cortical thickening includes the best femur and both iliac bones. Note the characteristic thickening and coarsening of the iliopectineal line (arrow) on the involved right aspect. Lead poisoning results from the ingestion of lead-containing materials (especially paint) or from the occupational inhalation of lead fumes. Note the characteristic cortical thickening, destruction of fine trabeculae, and accentuation of secondary trabeculae. In the past decade, the United States has experienced concern about imported toys that include lead. The chronic type of lead poisoning could cause psychological retardation, seizures, behavioral issues, or delayed development. Children are more vulnerable to decrease doses, and the impact on their central nervous system is more severe, inflicting interference within the cognitive thought course of. In youngsters, as a end result of lead and calcium are used interchangeably by bone, high concentrations of lead are deposited in essentially the most quickly rising portions of the skeleton, especially the metaphyses on the distal ends of the femur. The goal is to keep the blood lead degree decrease than 60 g/dL to stop potential encephalopathy. Dense transverse bands of sclerosis (arrowheads) prolong throughout the metaphyses of the distal femurs and the proximal tibias and fibulas. Large quantities of lead-containing materials ingested by a young youngster who had obtained no distinction material. The disease could also be confined to a single bone (monostotic) or the bones of one extremity, which is the most common form when it happens in adults. The other form, by which the disease is broadly distributed throughout the skeleton (polyostotic- among sufferers with this form, 25% have involvement of half the skeleton with greater than 25% involvement of the skull), is present in kids and happens most often in women. Fibrous dysplasia involves primarily the lengthy bones (especially the femur and tibia), ribs, and facial bones. The bone is commonly regionally expanded (suggesting a balloon), and the cortex may be eroded from inside, predisposing to pathologic fractures. Fibrous dysplasia is the commonest explanation for an expansile focal rib lesion, which often has a ground-glass or soap-bubble appearance. Treatment of fibrous dysplasia consists of curettage, repair of fractures, and prevention of deformities. Note the smudgy, groundglass appearance of the medullary cavities with failure of normal modeling. An expansile lesion of the humerus incorporates irregular bands of sclerosis, giving it a multilocular look. Mechanical distortion in regards to the hip leads to uneven weight bearing and accelerated secondary osteoarthritis. It is usually essential to acquire two radiographs in sufferers with ischemic necrosis. The first is taken with normal density, whereas the second is made with an increased kVp to enable for enough penetration of the more opaque sclerotic ischemic bone. Radionuclide bone scanning is more sensitive than plain radiography for detecting adjustments of ischemic necrosis. In the initial stages of infarction, radionuclide exercise is absent within the area of involvement. As the illness progresses, this space of decreased activity could turn into rimmed by a zone of elevated exercise on account of the reparative course of. In addition to ischemic adjustments in the subchondral areas of bone, infarction may contain the shaft of a long bone.
Allegra 180 mg generic fast delivery
Transverse scan of the posterior aspect of the elbow shows the thick-walled allergy symptoms face allegra 120 mg purchase with amex, fluid-containing olecranon bursa allergy testing worcester allegra 120 mg order without a prescription. Bursitis Bursitis refers to an inflammation of the bursae, small fluid-filled sacs situated near the joints that scale back the friction brought on by motion. Repeated bodily exercise generally causes bursitis, but trauma, rheumatoid arthritis, gout, or infection also can cause this inflammation. Plain radiographic photographs might exclude different problems that cause comparable symptoms. The major radiographic manifestation of bursitis is the deposition of calcification in adjoining tendons, which is a typical reason for pain, limitation of movement (frozen joints), and disability about a joint. However, calcification may be detected in asymptomatic persons, and severe clinical symptoms may occur without proof of calcification. The deposits differ significantly in measurement and form, from skinny curvilinear densities to large calcific masses. In the acute early levels of bursitis, ultrasonography demonstrates the bursa filled with synovial fluid and having ill-defined margins. During the acute phase of true tendinitis, the thickened tendon has ill-defined margins. Both bursitis and tendinitis could reveal elevated vascularity on Doppler ultrasound. First-line remedies for bursitis embrace utility of warmth, rest, and immobilization. A more aggressive group of drugs, disease-modifying antirheumatic medicine, are utilized in advanced levels to cut back signs. The antimetabolite methotrexate, a cytotoxic drug, tempers cell division in the synovial joint. For infectious arthritis, antibiotics usually eradicate the infection and cure the arthritis. Frontal projection of the shoulder demonstrates amorphous calcium deposits (arrows) within the supraspinatus tendon. Opacification of the subacromial and subdeltoid bursae signifies irregular communication between them and the glenohumeral joint cavity, thus confirming the prognosis. In recurring or extreme bursitis, corticosteroid injections into the affected bursa may cut back the irritation. Rotator Cuff Tears the rotator cuff of the shoulder is a musculotendinous construction composed of the teres minor, infraspinatus, supraspinatus, and subscapularis muscles. Longitudinal ultrasound scan shows thickening and decreased echogenicity of the higher two-thirds of the tendon (arrows). Treatment for Intra-articular Components Anti-inflammatory medications and immobilization of the joint are the primary line of treatment if the damage will restore itself. When irreparable joint injury has occurred, the orthopedist performs arthroscopic surgical procedure to take away an entire or nonhealing tear or to try suture repair. Bacterial Osteomyelitis Bacterial osteomyelitis is an irritation of the bone (osteitis) and bone marrow (myelitis) brought on by a broad spectrum of infectious (most often gram-positive) organisms that attain bone by hematogenous spread, by extension from an adjoining website of an infection, or by direct introduction of organisms (after trauma or surgery). In infants and kids, the metaphyses of long bones, especially the femur and tibia, are most often affected; staphylococci and streptococci are the commonest organisms. Patients with acute osteomyelitis expertise fever and localized heat, swelling, and tenderness. In adults, acute hematogenous osteomyelitis primarily happens in the vertebrae, causing localized back ache and muscle spasm, and it rarely includes the long bones. Although the incidence and severity of osteomyelitis have decreased since the advent of antibiotics, this illness has now become more prevalent as a complication of intravenous drug abuse (in which case, gram-negative organisms are found). Although sometimes the outcomes of acute trauma, meniscal tears extra incessantly replicate a degenerative course of attributable to the persistent trauma inherent in human knee operate. Radionuclide bone scan (posterior projection) demonstrates increased uptake of radionuclide within the trochanteric portion of the proper femur (arrow). Plain x-ray of the pelvis and hips obtained on the same time confirmed no detectable abnormality. Pus produced by the acute irritation spreads down the medullary cavity and outward to the floor. Once the infectious process has reached the outer margin of the bone, it raises the periosteum from the bone and may spread along the surface for a substantial distance. Because the earliest modifications of osteomyelitis are often not evident on plain radiographic images till roughly 10 days after the onset of signs, radionuclide (technetium-99m) bone scanning is probably the most useful imaging modality for the early analysis of osteomyelitis. On plain radiographs, the earliest evidence of osteomyelitis in an extended bone is a localized, deep delicate tissue swelling adjacent to the metaphysis. The inflammation causes displacement or obliteration of the conventional fats planes adjoining to and between the deep muscle bundles, unlike in pores and skin infections, by which the initial swelling is superficial. The preliminary bony change appears as refined areas of metaphyseal lucency reflecting resorption of necrotic bone. Eventually, a appreciable quantity of new bone surrounds the cortex in a thick, irregular bony sleeve (involucrum). Power Doppler ultrasound demonstrates increased vascularity in the irritation elevating the periosteum. After the acute infection has subsided, a sample of persistent osteomyelitis develops. The cortex may become so dense that the medullary cavity is difficult to demonstrate. Antibiotics to eradicate gram-negative or gram-positive organisms should be given for four to eight weeks to prevent recurrence. Surgery may be required for d�bridement of necrotic tissue or for placement of a drain into an abscess. Bone grafts, usually of bone marrow, are positioned to fill bony defects or to help bones heal. After surgical procedure, the patient should proceed to take antibiotics for roughly 3 weeks. Tuberculous Osteomyelitis Tuberculous osteomyelitis (which is uncommon today) mostly involves the thoracic and lumbar spine. Irregular, poorly marginated bone destruction inside the vertebral physique is commonly associated with a characteristic paravertebral abscess, an accumulation of purulent materials that produces a fusiform delicate tissue mass about the vertebra. The unfold of tuberculous osteomyelitis causes narrowing of the adjoining intervertebral disk and the extension of infection and bone destruction throughout the disk to involve the adjoining vertebral body. Caseous necrosis of the vertebral marrow produces a gradual resorption of bony trabeculae, with bone destruction showing 2 to 5 months after onset of infection. The gallium bone scan might help to define the whole tissue involvement and determine response to therapy in tuberculous osteomyelitis. Tuberculosis can, not often, contain a low-grade chronic infection of the long bones that seems radiographically as a typically damaging lytic process with minimal or no periosteal response. The spectrum of radiographic appearances is extensive, various from localized, well-circumscribed, expansile lesions to diffuse, uniform, honeycomb-like areas of destruction which may be usually related to pathologic fractures. Nonoperative therapies for tuberculous osteomyelitis embrace a regimen of antibiotics, antituberculous drug remedy, and possible bracing.