
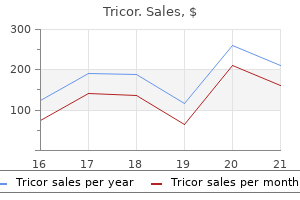
Tricor dosages: 160 mg
Tricor packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Tricor 160 mg cheap without prescription
It could occur in a wide spectrum of hematologic cholesterol medication names buy discount tricor 160 mg line, neoplastic cholesterol uptake by cells tricor 160 mg buy generic, infectious, inflammatory, vascular, and systemic disorders. Demographic and Clinical Features Splenomegaly can happen at any age from a variety of situations. The normal grownup spleen is mostly not palpable because of its position under the rib cage. As the spleen enlarges, it usually retains its normal shape, protrudes inferiorly below the costal margin, and becomes palpable on physical examination. Patients could come to scientific consideration with indicators and symptoms referable to the underlying disorder inflicting splenomegaly, with left-upper-quadrant fullness, or with a palpable left belly mass. However, patients could experience pain with splenic infarction, infection, or inflammation. Patients with splenomegaly may come to clinical consideration with indicators and symptoms of hypersplenism, which may trigger anemia, leukopenia, and/or thrombocytopenia. Pathology Congestive splenomegaly is certainly one of the most typical causes of splenic enlargement. It is attributable to venous congestion from portal hypertension, splenic vein thrombosis, or right-sided coronary heart failure. At gross pathologic examination, the spleen may be moderately or markedly enlarged, weighing from 500 to 5000 g. Elevated venous pressures causes collagen deposition in the sinusoids and gradual blood flow through the sinusoids allows time for macrophages to destroy blood cells, which can end in hypersplenism. Inflammatory disorders of the spleen generally cause mild enlargement of the spleen and acute congestion of the purple pulp. Neutrophils and plasma cells are normally current all through the pink and white pulp. Depending on the inflammatory or infectious agent, microabscesses or large abscesses and white pulp may be present. A measurement of 12 cm is considered the higher restrict for regular for an adult with an roughly 150-g spleen. Evaluation of the patency of the splenic vein and artery with shade and spectral Doppler may be made. One of the most regularly encountered causes of splenomegaly is portal hypertension. In addition to splenomegaly, different findings of portal hypertension related to the spleen could also be present on cross-sectional 595 596 Gastrointestinal Imaging bodies are foci of decreased signal intensity on T1- and T2-weighted images. Differential Diagnosis Congestive splenomegaly: Cirrhosis, portal or splenic vein thrombosis or occlusion, congestive heart failure. Hematologic disorders: Leukemias, lymphomas, multiple myeloma, myeloproliferative problems, hemolytic anemias, extramedullary hematopoiesis. Immunologic problems: Systemic lupus erthyematosus, rheumatoid arthritis, amyloid. Infections: Disseminated hematogenous infections, mononucleosis, tuberculosis, cytomegalovirus, malaria, histoplasmosis, typhoid, brucellosis, leishmaniasis, echinococcosis. Supine abdominal radiograph shows an enlarged spleen (*) as a delicate tissue density extending from the left upper quadrant to the left midabdomen. It displaces the stool-filled transverse colon inferiorly and the abdomen (arrowhead) to the best. Focal hemosiderin deposition in the spleen is usually observed in sufferers with portal hypertension. They are the result of perivascular hemorrhage and comprise fibrous tissue and iron and calcium deposition. Splenic index or splenic quantity measurements present extra accurate evaluation of splenic size in contrast with a single measurement of size. Vascular patency and presence of masses ought to be assessed when splenic enlargement is encountered on imaging studies. Abscesses and Infections Definition the spleen may be involved in hematogeneously disseminated bacterial and fungal infections, tuberculosis, and pneumocystis. These infections cause diffuse splenomegaly, multiple splenic nodules or cystic lesions, or solitary cystic lesions. Patients may also present with belly pain and tenderness and could also be discovered to have splenomegaly on bodily examination. Fungal microabscesses from Candida, Aspergillus, and Cryptococcus may occur in immunocompromised sufferers. Pyogenic abscesses of the spleen may occur within the setting of sepsis because of septic emboli in sufferers with endocarditis, spread from contiguous infection, or as a complication of infarction or trauma. In addition to generalized sepsis, pyogenic splenic abscesses may develop in immunocompromised sufferers. Splenic infarcts and pancreatic pseudocysts involving the spleen might become secondarily contaminated. Patients with splenic hydatid illness may be asymptomatic or complain of abdominal 598 ache, left-upper-quadrant ache, or belly fullness. Pathology the analysis of splenic infections requires the identification or culture of the offending organism. In widespread fungal disorders corresponding to disseminated candidiasis, blood tradition typically supplies the analysis when there are typical imaging options. Occasionally it may be essential to obtain the prognosis clinically via tissue sampling. Histologically, Candida is a 4- to 6-m budding yeast admixed with pseudohyphae that stain constructive with periodic acidSchiff and silver stains. Echinococcal cysts are most often recognized serologically when there are imaging options to counsel the presence of a hydatid cyst. The larval forms of the echinococcal tapeworm, which have a characteristic histologic type with scolices and hooklets, are found throughout the cysts. Imaging Features Calcified splenic granulomas from prior an infection with tuberculosis or histoplasmosis in immunocompetent persons are among the many most typical imaging findings of splenic an infection. Other findings of prior tuberculosis or histoplasmosis-such as calcified pulmonary granulomas, lymph nodes, and liver granulomas-are typically present in the identical patient. On ultrasound, these are punctate echogenic foci which will produce posterior acoustic shadowing. In lively tuberculosis infection, the splenic manifestations embody splenomegaly and microabscesses. Lymphadenopathy within the splenic hilum, peripancreatic region, and retroperitoneum can be regularly present in disseminated M. Fungal microabscesses are hardly ever larger than 2 cm in size and are normally quite a few. In these cases, refined lesions may be seen as hyperintense nodules on T2-weighted and diffusion weighted sequences.
Bovine Testicle extract (Orchic Extract). Tricor.
- How does Orchic Extract work?
- Are there safety concerns?
- Dosing considerations for Orchic Extract.
- What is Orchic Extract?
- Maintaining healthy testicle function in men and other uses.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96975
Best tricor 160 mg
This will increase the pressure on the decrease esophagus and reduces acid reflux cholesterol medication controversy tricor 160 mg generic on-line, permitting the esophagus to heal xanthomas cholesterol treatment buy tricor 160 mg fast delivery. Also, during the procedure a coexistent hiatal hernia is pulled down and sutured so that it remains throughout the abdomen. There should be clean, tapered narrowing of the distal esophagus because it extends via the wrap for 2 to three cm. The wrap ought to be positioned beneath the diaphragm with a constant and circumferential relationship to the esophagus. Postsurgical Complications In the early postoperative interval, edema could cause a good wrap, with subsequent dysphagia and obstruction. The distal esophagus is narrowed because it extends although the wrap (arrow) with out obstruction or leak. Some patients might have persistent narrowing of the distal esophagus, inflicting dysphagia or "gas bloat" syndrome with abdominal fullness and lack of ability to belch. Recurrent hernia could occur with an intact fundoplication wrap and should or might not embrace the wrap. With intrathoracic migration of the wrap, the fundoplication migrates above the esophageal hiatus. These complications usually have a tendency to happen with preexisting esophageal shortening. A shortened esophagus may pull the wrap above the diaphragm or the wrap may slip distally as the esophagus retracts into the chest. An esophageal lengthening procedure on the time of preliminary surgery could help to forestall these complications. Disruption of the fundoplication wrap could additionally be complete or partial and might trigger recurrent hiatal hernia and reflux. The clean and symmetric appearance of a fundoplication wrap ought to assist to differentiate it from a fundal neoplasm. Common Variants and Mimics It may be difficult to distinguish a slipped fundoplication from the traditional look following esophageal lengthening or Collis gastroplasty. With a Collis gastroplasty, gastric folds may be seen extending above the wrap into the neoesophagus created from the gastric cardia. Knowledge of the surgical procedures performed can help make the right analysis. Management/Clinical Issues Patients presenting with dysphagia, nonspecific chest or belly ache, vomiting, or symptoms of obstruction following fundoplication are often evaluated radiologically. The decrease esophageal sphincter is strengthened with a fundal wrap and a hiatal hernia is repaired. Knowledge of the particular surgical process carried out could assist within the acceptable diagnosis of postoperative complication. Note the mild luminal narrowing the place the abdomen extends via the diaphragm (arrow). Surgical strategy to gastroesophageal reflux disease: what the radiologist have to know. Intrathoracic migration of the wrap after laparoscopic 114 Gastrointestinal Imaging Nissen fundoplication: radiologic analysis. Pathology Partial gastric resection with removal of the pylorus and denervation of the abdomen can alter gastric emptying, intestinal motility, and absorption and can cause metabolic abnormalities. Dumping syndrome has been reported in up to 50% of sufferers and causes vasomotor and cardiovascular signs, together with weakness, dizziness, sweating, colic, nausea, and diarrhea. Gastric stasis without mechanical obstruction may happen in as a lot as 25% of sufferers and might cause postprandial bloating, vomiting, ache, and weight loss. These signs are as a outcome of ineffective gastric emptying, impaired motility, and/or alkaline reflux gastritis. Diminished peristalsis and decreased gastric acid permit retention of fibrous materials and the formation of a conglomerate. Afferent loop syndrome may cause epigastric pain, postprandial fullness, nausea, vomiting, and, not often, obstructive jaundice; it can be due to any process causing obstruction, together with gastrojejunal stomal stenosis, recurrent tumor near the anastomosis, adhesions, inner hernia, or volvulus. Alternatively, afferent loop syndrome may be because of preferential circulate into the afferent limb (retrograde flow). There is an increased danger of gastric stump (remnant) carcinoma following partial gastrectomy for benign issues. This most often occurs more than 5 years postoperatively; after 15 to 20 years, the chance increases three to six times. This may be associated to bile reflux with persistent gastritis and a gradual progression from regular mucosa to metaplasia to dysplasia and most cancers. Also, after partial gastrectomy for localized neoplasm, patients may develop recurrent tumor. Billroth/Gastrojejunostomy Definition Gastrojejunostomy is a surgical process that creates a communication between a portion of the abdomen and the jejunum, usually related to resection of the distal abdomen. Demographic and Clinical Features Gastrojejunostomy is a surgical process that could be performed for malignancy, benign lots, and inflammatory conditions including peptic ulcer illness and obesity. With the Roux-en-Y gastric bypass process for morbid weight problems, the remainder of the abdomen is left in place and the gastric pouch is anastomosed to a jejunal limb (see Chapter 18A). With advances in medical therapy for peptic ulcer illness, surgical remedy is much less common; however, surgery could additionally be indicated for perforation, hemorrhage, obstruction, and intractable or nonhealing ulcers. Surgical Procedures Billroth procedures involve resection of the distal abdomen with anastomosis to a different bowel phase. This process goals to restore continuity between the abdomen and duodenum without a substantial gastric resection. With a Roux-en-Y configuration the jejunum is split just distal to the ligament of Treitz and brought up to the stomach. The duodenojejunal (afferent) limb is anastomosed to more downstream jejunum, diverting bile and pancreatic secretions away from the gastric remnant. With a loop-type gastrojejunostomy the abdomen is anastomosed to the facet of the proximal jejunum. The proximal or afferent loop contains pancreaticobiliary secretions and drains towards the stomach. As in all postoperative sufferers, preliminary attention is directed to the surgical anatomy. Rarely, contrast could reflux into the duodenum, demonstrating leak from an overseen duodenum. A collection in the antrectomy bed or close to the overseen duodenum may elevate concern for a breakdown in the suture line and consequent leak. A bezoar seems as a discrete mottled mass of meals particles in the gastric remnant. A small ulcer crater with thickened, edematous radiating folds may be seen along the enteric aspect of the anastomosis. There can additionally be extravasation of distinction materials tracking medial to the anastomosis (arrowheads), according to an anastomotic leak.
160 mg tricor purchase visa
Primar y Peritoneal Malignancies 657 Key Points Diffuse peritoneal malignant mesothelioma produces sheet-like thickening of the peritoneum and encases bowel percentage of cholesterol in eggs tricor 160 mg buy amex. Localized peritoneal malignant mesothelioma produces a focal mass that will invade adjoining organs cholesterol medication calculator tricor 160 mg buy low cost. Ancillary findings supporting the prognosis of peritoneal malignant mesothelioma include the dearth of proof of a primary malignancy, lymphadenopathy, and metastasis elsewhere. Clinical symptoms embody belly distention, ache, fullness, increasing belly girth, nausea, and/or vomiting. Pathology Primary peritoneal serous carcinoma is indistinguishable from metastatic serous ovarian carcinoma on gross, histopathologic, and immunohistochemical examination. Histopathologically the tumors are composed of irregular interconnecting clusters of malignant cells arranged in a stable, cribiform, or cystic structure. The following criteria have been established to make the diagnosis of main peritoneal carcinoma: (1) each ovaries are regular, (2) the involvement of extraovarian websites should be higher than the involvement on the surface of both ovary, or (3) the ovarian involvement have to be nonexistent, confined to ovarian surface epithelium with out stromal invasion, or involving the cortical stroma with tumor dimension lower than 5 by 5 mm. Primary Peritoneal Serous Carcinoma Definition Primary peritoneal serous carcinoma arises from the peritoneum. It is a novel clinicopathologic entity that differs from malignant ovarian surface epithelial stromal tumors even though it has related histopathologic options. Demographic and Clinical Features Primary peritoneal serous carcinoma nearly all the time happens in women (mean age 56 to 62 years). The peritoneal recesses of the higher stomach, notably the subphrenic areas, should be fastidiously evaluated for the presence of illness because this is the most important website of lymphatic clearance of the peritoneum. Differential Diagnosis Peritoneal carcinomatosis, metastatic ovarian carcinoma, and malignant mesothelioma: Primary peritoneal serous carcinoma must be instructed in the differential prognosis when the findings of ascites and carcinomatosis are recognized in a female affected person with no proof of a visceral major or ovarian mass. Classification the nomenclature surrounding main peritoneal serous carcinoma is confusing. There are a quantity of synonyms for this tumor: serous surface papillary carcinoma, primary peritoneal carcinoma, extraovarian pelvic serous carcinoma, primary serous papillary carcinoma, and psammomacarcinoma. Management/Clinical Issues the therapy and prognosis for major peritoneal serous carcinoma is identical to that for serous ovarian carcinoma. Demographic and Clinical Features Desmoplastic small round cell tumor is a very rare malignancy that mostly happens younger men (mean age 19 years). A number of abdominal symptoms deliver patients to clinical attention: crampy belly ache, abdominal distention, constipation, weight loss, diarrhea, hematemesis, jaundice, and hematuria. Pathology Desmoplastic small round cell tumor may be a solitary, multifocal, or confluent grey to white firm nodule or mass that arises from the peritoneal surface. Imaging Features Although desmoplastic small round cell tumor spreads diffusely all through the peritoneal surfaces and the primary imaging discovering is most commonly diffuse peritoneal thickening, nodules, and masses, a solitary peritoneal mass will be the only finding present at initial presentation. Imaging after the administration of intravenous gadolinium reveals heterogeneous enhancement. Patients may present with or develop issues such as bowel or ureteral obstruction. The latter is especially widespread in patients that have dominant intraperitoneal pelvic lots. Serous surface papillary carcinoma of the peritoneum: clinical, radiologic, and pathologic findings in eleven sufferers. There is a small quantity of ascites and left hydronephrosis from tumor obstructing the left ureter. Differential Diagnosis Peritoneal carcinomatosis and lymphomatosis: Uncommon conditions in young males. The discovering of single or a quantity of dominant plenty inside a diffuse course of is extra attribute of desmoplastic small spherical cell tumor than of carcinomatosis or lymphomatosis. Prognosis and Management Patients with desmoplastic small round cell tumor have a universally poor prognosis. Key Points Desmoplastic small round cell tumor is a rare malignancy of the Ewing tumor family that happens predominantly in adolescent and younger adult males. Up to 50% of the patients have distant metastases on the time of medical presentation. Desmo-plastic small spherical cell tumor of the abdomen: radiologic-histopathologic correlation. Peritoneal Carcinomatosis Definition Peritoneal carcinomatosis is metastatic spread of carcinoma to the peritoneal cavity. It may happen by direct seeding from gastrointestinal or ovarian main malignancies, secondary seeding from iatrogenic spread of tumor, direct invasion, hematogenous dissemination, or lymphatic spread. When peritoneal carcinomatosis is the initial manifestation of malignancy, immunohistochemical staining assists in figuring out the primary lesion. Imaging Features Ascites may be the dominant clinical and imaging manifestation of peritoneal carcinomatosis. On imaging, loculation of ascitic fluid is amongst the most useful options to suggest a malignant etiology. Thickening, nodularity, and enhancement of the peritoneum with intravenous distinction can be suggestive of a malignant process. Sonographically the fluid may be anechoic or could contain hypoechoic particulate matter from proteinaceous exudate. Demographic and Clinical Features Initially patients with peritoneal carcinomatosis may be asymptomatic. Progressive involvement of the peritoneum will trigger them to complain of stomach enlargement from ascites in addition to of nausea, vomiting, and belly ache. A fibrotic response could occur and the omental fats may be changed with tumor and fibrosis producing omental caking. The pattern of peritoneal carcinomatosis varies from multifocal discrete nodules in clinically occult disease to infiltrative lots in symptomatic sufferers. Infiltration of the small bowel mesentery with carcinomatosis may produce characteristic pleated or stellate patterns that happen as the soft tissue tumor replaces normal mesenteric fats. Tumor may infiltrate the perivascular spaces, causing the vessels throughout the mesentery to seem denser than the adjoining regular mesenteric fat. Obstruction of the small bowel is the commonest complication of peritoneal carcinomatosis and could also be secondary to diffusely infiltrating tumor or focal tumor plenty. Because the normal peritoneum enhances to an identical degree because the liver, irregular enhancement must be suspected when the peritoneum is enhancing greater than the liver or has related thickening, nodularity, or mass. Differential Diagnosis Malignant mesothelioma: Most frequent main neoplastic lesion to diffusely involve the peritoneum. Evidence of asbestosis exposure corresponding to pleural plaques helps to recommend the diagnosis over carcinomatosis. Lymphomatosis: Peritoneal lymphomatosis secondary to a preexisting lymphoma mimics peritoneal carcinomatosis and malignant mesothelioma. Extensive adenopathy in lymph node chains sometimes concerned with lymphoma, similar to those in the retrocrural region and small bowel mesentery, could counsel lymphomatosis over carcinomatosis. Tuberculous peritonitis: May have a similar appearance to malignant mesothelioma and peritoneal carcinomatosis however can also present evidence of ileocecal tuberculosis or low-attenuation lymph nodes within the small bowel mesentery, peripancreatic region, or retroperitoneum.
Discount 160 mg tricor mastercard
Levine Definition Esophageal accidents could also be categorised as mucosal lacerations cholesterol test meaning discount 160 mg tricor otc, intramural dissections or hematomas cholesterol test validity 160 mg tricor quality, and full-thickness perforations. The latter perforations occur both as confined leaks or as free leaks into the mediastinum. Other patients might develop fistulas to the airway (trachea or bronchi), pleura, or, hardly ever, aorta. Demographic and Clinical Features Mucosal laceration of the esophagus, also recognized as a Mallory-Weiss tear, sometimes occurs in alcoholics who expertise severe retching and vomiting after an alcoholic binge. Affected people typically current with huge hematemesis, however the bleeding is self-limited. Esophageal hematomas/intramural dissections are attributable to a mucosal laceration within the distal esophagus. If the tear is partially or fully occluded, continued hemorrhage might result in a progressive submucosal accumulation of blood, producing an intramural hematoma. Endoscopy is the most common cause of full-thickness esophageal perforation, accounting for up to 75% of cases. Patients with thoracic esophageal perforation could present with the traditional triad of vomiting, extreme substernal chest pain, and subcutaneous emphysema of the chest wall and neck. These patients typically develop fever and leukocytosis and will turn out to be acutely ill from mediastinitis and sepsis. Esophageal-airway fistulas often outcome from direct invasion of the tracheobronchial tree by advanced esophageal carcinoma. Such fistulas have been reported in 5% to 10% of all patients with esophageal cancer, often occurring after therapy with radiation therapy. Other causes of esophageal-airway fistulas embrace esophageal instrumentation, trauma, international our bodies, and surgical procedure. Affected people typically current with violent episodes of coughing and choking throughout deglutition. Esophagopleural fistulas are usually attributable to surgery, esophageal instrumentation, radiation, or advanced esophageal carcinomas invading the pleural house. Affected people typically have nonspecific clinical findings corresponding to chest ache, fever, dysphagia, dyspnea, or foul-smelling regurgitations. Patients with aortoesophageal fistulas may current with a "sentinel" episode of arterial hematemesis followed by a variable latent period earlier than experiencing huge hematemesis, exsanguination, and death. These perforations sometimes happen as 1- to 4-cm vertically oriented linear tears on the left lateral wall of the distal esophagus close to the gastroesophageal junction. Imaging Features Most Mallory-Weiss tears (mucosal lacerations) are recognized by endoscopy. Esophageal hematomas normally seem on esophagography as solitary ovoid submucosal masses in the esophagus. Cervical esophageal perforation may appear on neck or chest radiographs as subcutaneous emphysema, retropharyngeal air, and pneumomediastinum. Single-contrast esophagogram exhibits a linear assortment of barium (arrows) abutting the distal esophagus because of a discrete mucosal laceration precipitated by recurrent retching after binge drinking in an alcoholic affected person. Single-contrast esophagogram exhibits focal extravasation of a water-soluble distinction agent right into a small, sealed-off leak (black arrow) within the upper esophagus as a result of tried endoscopic dilatation of a high esophageal stricture. Contrast agent can additionally be seen to fill a easy intramural assortment (white arrows) paralleling the esophageal wall distal to the perforation due to an intramural dissection, producing a double-barrelled esophagus. Both the contained leak and intramural dissection healed on conservative management. In contrast, thoracic esophageal perforation may be related to pneumomediastinum, mediastinal widening, and a pleural effusion or hydropneumothorax. Esophagography is usually performed on sufferers with suspected esophageal perforation. Some patients might have free leaks into the neck or mediastinum, whereas others could have small sealed-off leaks. Although barium is essentially the most sensitive contrast agent for detecting small leaks, it can potentially cause a granulomatous reaction in the mediastinum. However, water-soluble contrast agents are much less radiopaque than barium and can miss a considerable proportion of esophageal perforations. If, subsequently, the initial research with a water-soluble contrast agent exhibits no proof of perforation, it is strongly recommended that the examination be repeated with high-density barium to detect refined leaks. In contrast, when an esophagopleural fistula is suspected, the presence and placement of the fistula can be confirmed by a water-soluble distinction research. Aortoesophageal fistulas are extremely rare but are associated with a excessive mortality fee. Such fistulas could additionally be brought on by a ruptured aortic aneurysm, aortic dissection, contaminated aortic graft, swallowed international physique, or esophageal carcinoma. Patients with aortoesophageal fistulas may current with an initial episode of arterial hematemesis followed by a variable latent interval earlier than experiencing hematemesis, exsanguination, and demise. Finally, when an aortoesophageal fistula is suspected, oral research with water-soluble contrast are unlikely to show the fistula due to excessive aortic pressures. Contrast aortography can also be unsuccessful due to occlusion of the fistulous tract by thrombus. Therefore these fistulas are extremely tough to show on radiographic examinations. Single-contrast esophagogram exhibits focal extravasation of water-soluble distinction agent into a small, irregular, contained assortment (arrow) on the web site of perforation. This sealed-off leak healed on conservative treatment with no need for surgical repair. This affected person had small-cell carcinoma of the lung with a mediastinal mass compressing the midesophagus (small black arrows). There is also focal ulceration (large black arrow) with barium filling an esophagobronchial fistula (white arrow) as a result of invasion of the esophagus by this mass. However, a diverticulum will have a smoother contour and rounder configuration, and distinction materials is more prone to empty from a diverticulum than from a confined perforation into the esophageal lumen. Single-contrast esophagogram exhibits focal extravasation of water-soluble contrast from the left lateral wall of the midesophagus (white arrow), with contrast dispersing within the adjoining mediastinum (black arrows). Management/Clinical Issues In sufferers with Mallory-Weiss tears and intramural hematomas, the lesions normally heal spontaneously; with conservative medical management, bleeding is subsequently Esophageal Per foration 43 self-limited. With full-thickness esophageal perforation, the treatment and prognosis depend on the location of the damage. If untreated, perforations of the thoracic esophagus are related to a mortality fee of practically 100 percent because of a fulminant mediastinitis that happens in these patients. Free perforation from the thoracic esophagus therefore necessitates early surgical intervention with surgical closure of the perforation and mediastinal drainage.
160 mg tricor generic
The keratinocytes in this layer develop spines often known as dermosomes as they shrink and could additionally be referred to as prickle cells cholesterol exercise generic tricor 160 mg visa. These cells are in abundance in this layer and are tightly packed together cholesterol jak go obnizyc order tricor 160 mg on-line, which offers the skin with its strength, integrity and suppleness. As disintegration occurs, the granules contained in these cells type both a waterproof lipid referred to as lamellar granules and keratohyaline granules. Their main operate is to decelerate water loss across the epidermis and stop entry of Stratum granulosum the pores and skin Chapter 19 microbes. The lipids launched by these cells along with their thickened plasma make them extra resistant to destruction. Along with the keratohyaline granules, which help to type keratin within the higher layers, both contribute to making the skin stronger and tougher. Stratum lucidium Consisting of two or three rows of lifeless, flat, clear keratinocytes, with vague boundaries, the stratum lucidium seems as a skinny band mendacity simply above the stratum granulosum. The cells in the stratum lucidium are intently packed together and forestall fluid loss. It is simply present in areas which would possibly be uncovered to put on and tear, such as the soles of the toes and palms of the hands, as its perform is to supply extra safety. It consists of two subtly distinct strata: the decrease stratum compactum and the outside stratum dysjunctum (Bowser and White, 1985). The stratum compactum contains cells that are fibrous in nature and contains keratin, which protects the pores and skin from abrasions and penetrative harm. The stratum dysjunctum is the interface with the setting, and here the cells can reabsorb water, thus resulting in maceration and injury. The main function of the dermis is to present the epidermis with nutrients and help. It accounts for approximately 150% of the total weight of the human physique and varies in thickness from 1 mm within the eyelids to 5 mm within the again (White and Denyer, 2006). In the newborn, the dermis will contain small collagen bundles and the elastin fibres are immature. At birth the dermis is very skinny, oedematous and is loosely certain to the epidermis. The dermis of a new child is 60% as thick as adult skin and takes 6 months to mature, making the infant pores and skin more susceptible to harm. Phagocytes could additionally be discovered circulating in this region, offering a defence mechanism in opposition to microbes. The higher floor of the dermis has protrusions that are known as the dermal papillae, and these comprise capillary loops. In the palms of the palms and the soles of the feet these papillae are known as dermal ridges, which in flip type epidermal ridges within the epidermis lying above. The operate of these ridges, referred to as frictional ridges, is to allow the gripping capability of the arms and toes. These epidermal ridge patterns could also be use diagnostically to detect abnormal chromosome complements. Other areas of the skin contain organized sensory nerve endings such because the Meissner corpuscles. These are closely packed together at delivery, but within a couple of months of life these turn into extra spread out because the pores and skin grows, significantly on the dorsal surfaces (MacGregor, 2012). The collagen in this layer is continually being damaged down and being synthesized into dermal fibroblasts. It is this collagen that gives the skin its tensile energy, thus offering safety from direct injury. Collagen and elastin are produced more rapidly in youngsters; because of this, granulation tissue forms extra quickly. The skin Chapter 19 Within this layer, elastin fibres are current throughout, and their role is to give the skin its elastic recoil. The dermis modifies itself to produce not only dermal ridges but additionally cleavage traces and flexure strains. Cleavage strains are collagen fibres that separate, are invisible and run longitudinally to the skin. The spaces between the collagen and elastin fibres comprise adipose tissue, hair follicles, sebaceous glands and the sudoriferous glands. The appendages Clinical application Consider the young baby who has a significant loss of pores and skin tissue as a result of burns. The skin appendages embody the nails, sweat glands, sebaceous glands, hair follicles and hair. Essential within the production of any of the pores and skin appendages is the formation of an epithelial bud. The nails are fashioned from ectoderm that covers the dorsal tip of the digit which then thickens to turn out to be the nail subject. Growth is sluggish, and finally the encircling dermis covers the proximal and lateral a half of the nail area by forming nail folds. These cells develop over the nail area, keratinization occurs and a nail plate forms. This degenerates and what stays is referred to as the cuticle or the eponychium. The nail body is deeply recessed into the lateral surrounding epithelium on each side by the lateral nail grooves and the lateral nail depressions. The free edge of the nail extends over the hyponychiumthe distal finish of the nail. The pink colour of the nail is as a result of the underlying blood vessels that lie beneath the nail (Pringle and Penzer, 2002). If these vessels are obscured close to the world of the nail root a pale crescent shape may be observed; this is referred to as the lunula. An infant born after forty two weeks may have keratinized nails, which can also be lengthy and stained green because of the passage of meconium in utero. The lanugo is shed both earlier than and after delivery, with the scalp, eyebrows and eyelashes shed final (England, 1996). Terminal hair is the hair on the top, eyebrows and eyelashes; it stays present throughout the lifespan and is extra deeply pigmented than vellus hair. Each hair consists of columns of lifeless keratinized epidermal cells which may be connected along with extracellular protein. When the hair is growing the cells of the hair root absorbs the vitamins from the physique and these are then incorporated the skin Chapter 19 within the hair thus perhaps analysed for diagnostic functions. Hair is a distinguishing function of personal look, and in the younger particular person may be of prime importance. Loss of hair color can occur in young folks however is usually a half of the aging course of.
Purchase 160 mg tricor amex
Manifestations embody jaundice specific cholesterol lowering foods tricor 160 mg with mastercard, irregular liver serum chemistries cholesterol test cost in mumbai 160 mg tricor otc, fever, belly pain, and graft dysfunction. Chronic rejection happens in 1% to 5% of liver transplant recipients, starts no less than three months after surgery, and is a serious reason for late graft failure and late affected person dying in each adult and pediatric liver transplant recipients. Clinically it manifests as jaundice, pruritus, and in the end loss of liver synthetic perform. Vascular Complications Vascular complications normally happen at anastomotic websites and should have an result on hepatic arteries, portal veins, hepatic veins, or the inferior vena cava. Hepatic artery thrombosis, the most extreme vascular complication, occurs in 4% to 12% of adult and 9% to 42% of pediatric liver transplant recipients, often inside 2 months after liver transplantation. It has excessive fatality (up to 60%) and might cause fulminant hepatic necrosis and Key Points Liver transplantation is the therapy of choice for adult or pediatric sufferers with end-stage liver illness, acute liver failure, or hepatocellular carcinoma. In the United States, deceased-donor liver transplantation is far more frequent than living-donor transplantation. A multidisciplinary selection committee at each transplant heart selects appropriate candidates and locations them on the waitlist. Patients with hepatocellular carcinoma are assigned hepatocellular carcinoma exception points if the tumor stage meets applicable standards. The goal of imaging research is to assess hepatic vascular and biliary anatomy, variants, and patency; diagnose and stage hepatocellular carcinoma; and report related ancillary findings such as the presence and severity of ascites. The new liver allocation system: shifting towards evidence-based transplantation coverage. Imaging within the preoperative analysis of adult liver-transplant candidates: objectives, deserves of varied procedures, and recommendations. Model for finish stage liver illness rating predicts mortality throughout a broad spectrum of liver disease. Further Reading 364 Gastrointestinal Imaging graft failure, liver infarction and abscess formation, and ischemic cholangiopathy (see additional on). Manifestations depend upon the severity of the stenosis and embrace elevated serum liver chemistries, graft dysfunction, and ischemic cholangiopathy (see additional on). They could additionally be intra- or extrahepatic and typically current throughout the first months after transplantation. Portal venous thrombosis or stenosis happens in 1% to 3% of liver transplant recipients. Manifestations embrace abdominal pain, graft dysfunction, portal hypertension, and ascites. Uncommonly, hepatic veins and/or the inferior vena cava become thrombosed or stenosed. Affected patients may present with graft dysfunction, portal hypertension, Budd-Chiari syndrome, and lower extremity edema. Biliary Complications Biliary issues develop in 25% of liver transplant recipients and embrace bile leaks at the T-tube exit site, anastomotic strictures, and ischemic cholangiopathy. The time of onset after surgery is variable and relies upon partially on the character and etiology of the complication. T-tube website bile leaks manifest clinically throughout the first 3 months after transplantation with extrahepatic biloma formation. Ischemic cholangiopathy is normally associated with hepatic artery stenosis or thrombosis and develops inside 1 year after transplantation; manifestations embody biliary necrosis, nonanastomotic strictures, bile leaks, bilomas, peribiliary abscesses, and sepsis. Postoperative Fluid Collections Fluid collections are frequent inside the first few weeks after surgery. Collections normally are intra- or perihepatic; perihepatic collections are usually located on the website of vascular or biliary anastomoses. Collections are most commonly bilomas but may be abscesses, seromas, hematomas, or infarctions. Recurrence of Underlying Disease Reinfection of the liver with hepatitis C virus happens in as much as 90% of liver transplant recipients with a history of chronic hepatitis C infection and might advance to extreme fibrosis or cirrhosis in as little as 5 to 10 years; as a lot as 25% will finally require retransplantation. With hepatitis B vaccination, clinically vital hepatitis B reinfection happens occasionally (10% or less of patients). Hepatocellular Carcinoma the frequency of postliver transplantation hepatocellular carcinoma recurrence ranges from 10% to 60% and is dependent upon the pathology-determined tumor stage and grade on the time of surgical procedure as nicely as the presence of microvascular invasion. Cellular rejection is characterized by peribiliary lymphocytic infiltration, whereas humoral rejection is characterized by vasculitis (endotheliitis). Chronic Rejection Chronic rejection is dominated by vascular adjustments (fibrous intimal thickening), interstitial fibrosis, centrilobular hepatocyte swelling, and centrilobular cholestasis. Vascular Complications Hepatic arterial, portal venous, and caval stenosis or thrombosis is usually brought on by technical issues on the donor-recipient anastomosis (clamp damage, intimal damage because of perfusion catheters, anastomosis vessel redundancy), though hypercoagulability and external compression (hematoma, hepatic regeneration) may contribute to portal venous and caval obstructions. The pathophysiologic penalties of vascular stenosis or thrombosis rely upon their location and severity. In hepatic artery thrombosis and hemodynamically vital hepatic artery stenosis, hepatic arterial circulate is absent or decreased, thereby predisposing to hepatic infarction and, as described further on, ischemic cholangiopathy. Portal vein thrombosis or stenosis may cause presinusoidal portal hypertension and world hepatic hypoperfusion, hepatocellular dietary deficiency, and in the end parenchymal atrophy; uncommonly hepatic infarction may occur. Caval obstruction causes hepatic congestion or decrease extremity edema, relying on its location. Biliary Complications Anastomotic bile duct strictures are normally as a result of continual focal ischemia and finally fibrotic scarring. Ischemic cholangiopathy is often caused by hepatic artery thrombosis or stenosis, often resulting in multifocal biliary stricture formation. These abnormalities might predispose to pyogenic cholangitis and the formation of peribiliary abscesses. Less generally, intrahepatic strictures happen in the absence of hepatic arterial obstruction. Recurrence of Underlying Disease In liver transplant recipients with a historical past of persistent hepatitis C, infection of the model new liver happens immediately and histologic options of viral hepatitis-such as acute and chronic inflammatory cellular infiltrates, fibrosis, and finally cirrhosis-are widespread. Recurrent Hepatocellular Carcinoma Tumor recurrence is normally because of extrahepatic metastasis that was current but undiagnosed prior to liver transplantation; after surgical procedure, the metastasis may grow in its extrahepatic location or locations or may spread hematogenously to the liver and then grow as a hepatic lesion. Less generally, postliver transplantation hepatocellular carcinoma is as a result of of de novo tumor improvement associated to recurrent liver disease. Imaging Features Graft Rejection Acute or Chronic Rejection No imaging modality is sensitive or particular for the diagnosis of rejection. Ultrasound imaging may present an intraluminal filling defect within the hepatic artery or might fail to identify a traditional artery alongside its expected course. Doppler ultrasound exhibits irregular move (resistive move proximal to a stenosis, turbulent circulate at a stenosis, tardus parvus waveform distal to a stenosis) or flow may be absent. Postliver transplantation pseudoaneurysms are related in appearance to those occurring in other settings. Portal vein thrombosis has similar imaging findings as described for acute bland thrombosis; portal vein stenosis appears as focal narrowing of the vein with abnormal velocities on Doppler ultrasound. In hepatic venous or caval thrombosis or stenosis, imaging might present absence of circulate or filling defects throughout the lumen of the affected veins. A persistent monophasic wave pattern at Doppler ultrasound suggests a downstream stenosis. Postoperative Fluid Collections Postoperative collections appear as complex cystic lots without inside vascularity and should represent bilomas, seromas, hematomas, abscesses, or parenchymal necrosis.
Syndromes
- DO NOT close the fishhook wound with tape and apply antibiotic ointment. Doing so can increase the chance of infection.
- Abnormal heart rhythm
- Mental changes
- Do you have more than one?
- Elective abortion is done because a woman chooses (elects) to end the pregnancy.
- Items such as jewelry, watches, credit cards, and hearing aids can be damaged.
- Ranitidine
- Drooping of the eyelids
- Nausea
- Nutcracker esophagus
Tricor 160 mg generic with amex
Risk components for iatrogenic biliary injury are periportal inflammation cholesterol over 400 tricor 160 mg purchase without a prescription, bile duct anatomic variants cholesterol lowering food tips 160 mg tricor discount fast delivery, and surgeon inexperience. Bile duct damage could be recognized during or after surgery and should involve biliary obstruction, bile leak, or hemobilia. Intraperitoneal bile duct leaks might present days to weeks after surgical procedure with imprecise symptoms such as fullness or nausea; they might additionally cause bile peritonitis. Bismuth Classification of Injury the Bismuth classification is often used to categorize bile duct injuries and help in therapeutic planning Table 77-1). Injury fully obliterates the frequent hepatic duct stump but the confluence is unbroken. A right variant segmental duct department is current and injured, with or without primary duct involvement. Secondary signs of bile duct obstruction embody segmental hepatic parenchymal hyperenhancement on the arterial phase within the distribution of the bile duct obstruction or absence of expected pneumobilia if the sphincter of Oddi had been compromised, as with prior sphincterotomy or bile duct reinsertion. Nevertheless "bilomas," that are loculated collections of bile from a bile duct leak, should be instructed when postsurgical fluid collections are seen adjoining to 513 514 Gastrointestinal Imaging just lately manipulated bile ducts or along the reduce fringe of the liver. For these research, if the distinction material is excreted into the ducts, frank leakage of distinction out of the biliary tract and right into a suspected biloma can typically be seen. Alternatively nuclear scintigraphy with a biliary-excreted agent also can provide related affirmation of a bile duct leak. Differential Diagnosis of Biliary Tree Injuries Cholelithiasis: Stones in the biliary tree, obstructing the duct, can exist or develop within the postoperative setting and mimic biliary injury. Intraoperative fluoroscopic cholangiogram shows leakage of contrast from an irregular common hepatic duct (large arrow) right into a subhepatic assortment (small arrow), according to a Bismuth sort 1 leak. Clinical Features Patients might present with belly ache, often within a quantity of days after surgery. Fever and an elevated white blood cell count could additionally be seen in circumstances that are sophisticated by cholangitis or sepsis. Imaging Findings Percutaneous transhepatic cholangiography and endoscopic retrograde cholangiography are useful not solely to diagnose biliary strictures but additionally to enable remedy similar to placement of biliary stents; these procedures can even assess for concurrent leaks. Placement of a bile duct stent might help surgeons to subsequently establish the duct and carry out a repair. With time, the liver drained by an excluded bile duct will turn into atrophic and largely nonfunctional. However, the usage of hepatobiliary brokers might assist to define the extent of obstruction and allow subjective comparison of biliary excretion by the nonobstructed and the obstructed ducts. Differential Diagnosis Hemobilia: An uncommon complication that can lead to a temporary biliary obstruction. Blood merchandise may be seen within the bile ducts, in the gallbladder, or within the small bowel distal to the bile duct insertion. Small calculi may be obscured on maximum-intensity-projection images and could additionally be higher seen on thin-section source photographs. Management/Clinical Issues the main determination for management of an excluded duct is to determine whether the duct could be reconnected to the Management/Clinical Issues Percutaneous stenting and balloon dilatation are variably used for patients with biliary tract leaks and strictures. For minor leaks, stenting for a quantity of weeks or months may permit for the biliary wall to restore itself. More complex or extensive bile duct accidents might require surgical restore and even partial hepatectomy. The length of the intact duct distal to the biliary confluence determines whether or not a choledochojejunostomy or hepaticojejunostomy is needed. When the biliary confluence is severed, both a hepaticojejunostomy and repair of confluence are wanted. Key Points Bile duct harm can embody leak, stricture, or obliteration of a duct. Obstructed or Excluded Bile Ducts Definition Iatrogenic bile duct obstruction or "exclusion" could due to both intentional or accidental surgical ligation of a bile duct, complications arising from bile duct reinsertion into bowel, or ischemia often related to hepatic arterial injury. Eventually the obstructed territory of the liver will turn into increasingly atrophic whereas the the rest of the liver will hypertrophy. Care should be taken concerning the decision to drain an excluded duct percutaneously because this remedy may result in long-term issues corresponding to a persistent bile-duct-to-skin fistula. Demographic and Clinical Features Bile leakage is likely certainly one of the commonest early problems of hepatobiliary surgical procedure, including cholecystectomy. Symptoms of biliary leak may be obscure and embrace right stomach ache, fullness, or, if related to peritonitis or cholangitis, might embrace fever and indicators of sepsis. Postcholecystectomy bile duct leaks might occur when surgical clips are dislodged from the cystic duct stump or when biliary anatomic abnormalities are present, corresponding to an aberrant right duct that drains instantly into the gallbladder or into the cystic duct. Bile leakage after hepatobiliary surgical procedure may happen at websites of bile duct reinsertion into bowel or at a bile duct-toduct anastomosis. Bile duct leakage could occur in the early phases after surgery or may be delayed and related to arterial compromise, because bile duct viability is decided by the arterial blood supply. If rim enhancement around the fluid collection is seen, the enhancement is usually gentle. Bile Duct Leak Definition Leakage of bile from the biliary tract into the peritoneal house may happen after trauma or as a complication of hepatobiliary surgical procedure. This assortment is consistent with a biloma and the gas within it could have been residual, left from the trauma or surgical restore. Findings are ambiguous for whether the collection is sterile or contaminated or whether or not an active bile leak is present. Follow-up imaging, clinical correlation, or fluid aspiration are reasonable administration concerns. Also, an irregular or obstructed anastomosis should prompt a search for adjacent fluid collections that my result from a leak. Clinical findings of bilious fluid from drainage catheters affirm that a leak is present. Intravenously administered hepatobiliary distinction brokers can also help assess for biliary leak. Evaluation of photographs enhanced with hepatobiliary brokers requires preand postcontrast imaging to verify biliary leakage; careful inspection of the lumina of the drains is required, since distinction could at occasions preferentially enter into a drain somewhat than into other fluid collections. Further analysis and attainable intervention by biliary stenting can also be obtained by percutaneous transhepatic cholangiography or by endoscopic retrograde cholangiography. Postoperative seromas: May be indistinguishable from bilomas and should be included in the differential diagnosis. Management/Clinical Issues Tiny biliary leaks may not want aggressive remedy and can be observed clinically. Small leaks may be handled by sphincterotomy and stent placement to divert bile flow briefly. Key Points Bile leaks at the cystic duct stump or alongside the gallbladder fossa ought to be sought after cholecystectomy.
Order 160 mg tricor with mastercard
Three-dimensional construction is stabilized by the character of the R-groups cholesterol chemical structure discount tricor 160 mg without prescription, which permits for hydrophobic interactions cholesterol recommendations order 160 mg tricor with visa, to obtain most van der Waals forces, electrostatic (ionic) interactions, and H-bonds. Formation of disulfide (SaSa covalent bonds between two strategically a) situated cysteine residues stabilizes the folded conformation. Quaternary structure refers to those proteins which consist of a couple of polypeptide chain, generally recognized as subunit (monomer) and their meeting right into a practical molecule (oligomers). Subunits are held collectively by noncovalent interactions that exist between complementary surfaces. Globular proteins, in aqueous medium, have their hydrophilic R-groups of amino acid residues on the surface and the hydrophobic R-groups within the inside. Different functional items of a protein similar to binding websites for substrates, cofactors, and modifiers are known as 10. Proteins might exist in two or more different well-defined, energetically favorable conformations to meet the needs of their organic capabilities. Defects in the synthesis, assembly, storage, and disposal of proteins have pathological consequences. Protein degradation (proteolysis) occurs within the body by completely different processes: proteolysis in the gastrointestinal tract by pancreatic and gastrointestinal enzymes, intracellular lysosomal and autophage-phagosome-lysosomal proteolysis, and cytosolic and nuclear proteolysis by the energy-dependent ubiquitinroteasome complex. The inhibition of this pathway by specific and potent chemical inhibitors has therapeutic purposes. Aberrantly folded proteins, which escape degradation, can provide rise to proteolytic-resistant conformations leading to pathological penalties. Proteins that include a single polypeptide chain are typically thought-about at three ranges of group: major, secondary, and tertiary structure. The main construction is the unique sequence of amino acids that make up a particular polypeptide; primary construction is maintained by covalent bonds. Secondary, tertiary, and quaternary structures are maintained principally by noncovalent bonds; disulfide bridges may also be thought of at the secondary and tertiary levels. Secondary construction arises from repeated hydrogen bonding inside a series, as within the -helix, the -pleated sheet, and -turns N. Tertiary construction describes the threedimensional stereo-chemical relationships of all the amino acid residues in a single protein chain. Folding of a polypeptide is an orderly sequential process by which the polypeptide attains the bottom possible state of power. The folding of the polypeptide into its secondary construction is determined primarily by the first structure. Once the secondary buildings are in place, a tertiary structure is shaped and stabilized by interactions among amino acids that could be removed from each other within the major sequence but which may be close to one another within the three-dimensional structure. Configuration refers to the absolute arrangement of atoms or substituent groups in area around a given atom. Conformation refers to a three-dimensional arrangement of groups of atoms that can be altered without breaking any covalent bonds. Theoretically, subsequently, proteins can assume an infinite number of potential conformations, however beneath regular organic conditions, they assume only one or a really small variety of "most steady" conformations. Proteins depend on these secure conformations for his or her particular organic features. A functional protein is claimed to be in its native form, normally essentially the most stable one. The threedimensional conformation of a polypeptide chain is ultimately determined by its amino acid sequence (primary structure). Since the organic operate of a protein is decided by a specific conformation, modifications corresponding to denaturation (protein unfolding) can result in loss of biological exercise. Examples of necessary covalent bonds are peptide (amide) and disulfide bonds between amino acids, and C, C, and C bonds within amino acids. Coordinate covalent bonds contain the unequal sharing of an electron pair by two atoms, with both electrons (originally) coming from the same atom. The electron pair donor is the ligand, or Lewis base, whereas the acceptor is the central atom (because it incessantly can accept more than one pair of electrons), or Lewis acid. These bonds are important in all interactions between transition metals and natural ligands. These bonds are formed between positively charged (-ammonium, -ammonium, guanidinium, and imidazolium) side chains and negatively charged (ionized forms of -carboxyl, -carboxyl, -carboxyl, phosphate, and sulfate) groups. Eclipsed and staggered conformations for ethane are potential by advantage of the unrestricted rotation around the carbonarbon single bond. There is a potential power difference between the 2 forms, the staggered kind being on the minimum and the eclipsed type at the most. Three-Dimensional Structure of Proteins and Disorders of Protein Misfolding Chapter 4 33 Hydrogen bonds contain the sharing of a hydrogen atom between two electronegative atoms which have unbonded electrons. These bonds, although weak in comparison with the bonds mentioned beforehand, are important in waterater interactions, and their existence explains most of the unusual properties of water and ice (Chapter 2). Van der Waals attractive forces are due to a set dipole in a single molecule that induces rapidly oscillating dipoles in one other molecule via distortion of the electron cloud. The constructive finish of a set dipole will pull an electron cloud towards it; the negative end will push it away. The power of those interactions is strongly dependent on distance, varying as 1/r6, the place r is the interatomic separation. The van der Waals forces are notably important within the nonpolar inside structure of proteins, where they supply enticing forces between nonpolar facet chains. Hydrophobic interactions trigger nonpolar facet chains (aromatic rings and hydrocarbon groups) to cling collectively in polar solvents, particularly water. Van der Waals repulsive forces function between atoms at very short distances from each other and outcome from the dipoles induced by the mutual repulsion of electron clouds. These repulsive forces function when atoms not bonded to one another method more intently than the sum of their atomic radii and are the underlying forces in steric hindrance between atoms. The partial double bond character of the NaC bond in the transition state most likely greatest represents what exists in nature. Electrons are shared by the nitrogen and oxygen atoms, and the NaC and CaO bonds are each (roughly) "one-and-one-half" bonds (intermediate between single and double). However, X-ray data suggest that the trans type occurs extra frequently in proteins than does the cis form. It has been further postulated that some proline residues (known as "permissive" Repulsive Forces Electrostatic repulsion occurs between charged groups of the same charge and is the opposite of ionic (attractive) forces. Globular proteins often have combined, and fibrous proteins have predominantly one type of secondary structure. In the right-handed -helix, the helix turns counterclockwise (C-terminal to N-terminal), and, within the left-handed, it turns clockwise. A left-handed -helix is less steady than a right-handed -helix because its carbonyl teams and the R-groups are sterically hindered.
Buy 160 mg tricor mastercard
Primarily a classification system is used based on the system proposed by Sir Alan Parks cholesterol lowering diet plan australia tricor 160 mg visa. The suprasphincteric observe courses exterior the anal sphincter (ischioanal space) via the levator plate and then inferiorly to the intersphincteric area of the anal sphincter and the inner opening cholesterol score of 6.3 order tricor 160 mg with visa. The extrasphincteric monitor courses to the rectum with no (active) connection to the anal sphincter and canal. Extrasphincteric tracks are encountered only in sufferers with prior surgical procedure, where the monitor not includes the anal sphincter but active disease is outdoors the anal sphincter. Abscesses can be current, often intersphincteric abscesses, but abscesses could also be current wherever inside or outdoors the anal sphincter. Today imaging is widely used, and this has led to different classification systems as well, profiting from the imaging findings. Most probably this lack of implementation is said to the considerably cumbersome link to treatment. For management it is very important classify the track based on the 5 kinds of the Parks classification and some others features indicating a more complex track. This definition comes from the concept that sufficient external sphincter should be intact for continence when fistulotomy is being thought-about. In patients with cryptoglandular fistulas, the imaging report ought to clearly state the classification, the situation of the interior opening. Further, the presence and extent of defects, fibrosis and atrophy of the anal sphincter muscular tissues ought to be indicated. As primarily medical treatment will be used, particularly the activity of the perianal fistulous disease must be clearly indicated (fluid, granulation tissue, abscesses) and said in the conclusion of the report. These abscesses are often apparent clinically and predominantly drained without preoperative imaging. In troublesome circumstances, imaging can be used to determine whether the abscess has been sufficiently drained. Management/Clinical Issues Patients with cryptoglandular fistulas are often treated by anal surgery. Pivotal is classification, whether it considerations a simple or complicated track and a low or excessive observe. Here the observe is laid open without any or very limited detrimental impact on anal continence. Higher tracks will be handled with more restricted surgery to protect anal continence. As the interior opening is considered the cause of persistent inflammation, several therapy options can be found to close the internal opening. Closing the opening prevents fecal material from getting into the track, which is considered a major factor for maintaining inflammation. The observe can be closed by mucosal advancement flap or by placing materials, such as glue or a plug, within the opening. Noncutting setons are used to secure drainage; aside from small abscesses, abscesses are treated by surgical drainage. Key Points Cryptoglandular fistula-in-ano occur more usually in male patients (2:1). A (fat-saturated) T1-weighted sequence after intravenous distinction administration differentiates an abscess filled with fluid from granulation tissue. Practice parameters for the therapy of perianal abscess and fistula-in-ano (revised). Mortele Definition Primary adenocarcinoma arising from the rectum is distinguished from other colonic adenocarcinomas by its high incidence, clinical presentation, larger array of diagnostic checks, and out there remedies. Demographic and Clinical Features One third of all colorectal cancers come up in the rectum; of these, approximately 30% happen in the distal 6 cm of the rectum. Because of their location at the distal most colon, rectal adenocarcinomas are extra likely than different colorectal carcinomas to current with small-caliber "pencil" stools, colonic obstruction, bright-red blood per rectum, and a palpable mass at digital rectal examination. Colorectal carcinomas are the third commonest cancer identified among women and men in the United States. However, the incidence is declining and survival bettering in part because of screening packages. Risk elements for rectal adenocarcinoma are much like these for colon cancer and embrace age greater than 50 years, African American or Ashkenazi Jewish ethnicity, history of adenomatous colonic polyps, history of colorectal cancer, inflammatory bowel illness, household history of colorectal cancer or adenomatous polyps, and diets excessive in pink or processed meats. Inherited syndromes- including familial adenomatous polyposis, hereditary nonpolyposis colon cancer (Lynch syndrome), and Turcot or Peutz-Jeghers syndrome-carry a excessive danger of colorectal carcinoma occurring during younger adulthood. Pathology Rectal adenocarcinomas are believed to come up from adenomas that could be polypoid or sessile. Adenomatous polyps are by definition neoplastic and progress over a period of a decade to turn out to be dysplastic and then frankly malignant. Cancers are initially isolated to the polyp; they then progress to invade the layers of the rectal wall. Tumor invasion of the muscularis propria is T2, past the muscularis propria into the perirectal fat is T3, and into peritoneum or adjacent organs is T4. Endorectal ultrasound is outstanding for the analysis of the depth of tumor invasion via individual layers of the rectal wall. Imaging is generally carried out after sodium biphosphonate and sodium-phosphate enema treatment; it includes T2-weighted imaging with out fats saturation. An iron- or barium-containing answer may be injected into the rectum to provide adverse intraluminal distinction, or ultrasound gel could also be injected to present optimistic T2 sign distinction. Tumor typically seems as intermediate signal on a T2 sequence, disrupting the normal trilayered appearance of the rectal wall. The normal wall of the rectum sometimes appears as a barely dark innermost layer representing the mucosa, a brilliant sign submucosal layer, and an intermediate hypointense layer similar to the muscularis propria. No lymph nodes are seen within the mesorectal fats, although small blood vessels are widespread. The mesorectum is bounded by the seminal vesicles and prostate anteriorly in males and uterus and vagina anteriorly in ladies; the sacrum posteriorly; and, skinny hypointense mesorectal fascial planes laterally. However, no extension of tumor past the muscularis into the perirectal fats is seen. Again, although obscuration of the low-T2-signal muscularis is seen in some areas, no tumor extension past the muscularis is seen. T3 tumor is recognized as nodular intermediate tumor sign depth protruding into the perirectal fats. Identification of any visible lymph nodes is essential to the treatment and prognosis of rectal adenocarcinoma. In regular patients, seen nodes within the mesorectum are unusual, even with proctitis. Some knowledge suggest that sufferers might achieve enough management of tumor or treatment with chemoradiation alone without surgical excision. In these cases, the postchemoradiation scan serves as an necessary reference for future follow-up.
Tricor 160 mg order on line
Confident delineation of branch anatomy in circumstances the place the ducts are of normal caliber cholesterol levels 160 mg tricor purchase free shipping, as after trauma or in wholesome dwelling potential liver donors known cholesterol lowering foods cheap tricor 160 mg on line, could additionally be difficult. Use of parallel imaging respiratory gated thin-section three-dimensional imaging and possibly the use of hepatobiliary agents can help to improve the visualization of first- and second-order bile duct branch anatomy. Care should be taken to inspect areas of obstruction since obstructions could obscure the bile duct department factors and cause ambiguity as to whether or not a bile duct anatomic variant is present and whether surgery would require multiple bile duct anastomoses. For nondilated nonobstructed bile ducts, T1-weighted thin-section imaging with a hepatobiliary agent can also be obtained to assist increase confidence within the biliary anatomy. Choledochal Cysts Definition A choledochal cyst is congenital dilatation of the extrahepatic bile duct. The dilatation could contain the intrahepatic ducts and cystic duct in some sufferers. Demographic and Clinical Features Choledochal cysts have a prevalence of roughly 1 in one hundred,000 people in western countries and the next prevalence in Asia. Three fourths of choledochal cysts happen in females and most instances are diagnosed earlier than the age of 10. Choledochal cysts could additionally be difficult by intraductal stones, recurrent cholangitis, pancreatitis, biliary strictures, portal hypertension, and pancreatic ductal stones. Choledochal cysts are associated in 90% of instances with an anomalous pancreaticobiliary ductal junction, also referred to as an elongated widespread channel. This is where the distal frequent bile duct and pancreatic duct join to form a typical duct for over 1. This common channel is assumed to predispose patients to develop malignancies such as cholangiocarcinoma or gallbladder most cancers, presumably associated to the reflux of pancreatic fluid into the biliary tract. Without choledochal cyst excision, patients have a cumulative danger of over 10% to develop extrahepatic cholangiocarcinoma by the time they reach 35 years of age. Choledochal cysts could be subclassified primarily based on location and look, but the surgical treatment is mostly the identical: to resect the whole choledochal cyst and separate the bile ducts from the pancreatic ducts in order to keep away from subsequent improvement of biliary most cancers. Choledochal cysts could also be associated with a pathologic "common channel," which refers to the presence of an elongated conjoined duct after the frequent bile duct joins the pancreatic duct and is a danger issue for growing cholangiocarcinoma. Although completely different types of choledochal cysts are acknowledged, the overall surgical remedy for choledochal cysts is identical: to resect the cyst fully and remove connections between the bile and pancreatic ducts. Note the widespread channel between the widespread bile and pancreatic duct illustrated for the type I cyst. The pancreatic duct (arrowhead) joins with the frequent bile duct to type a long widespread channel, which is a known danger issue for the development of cholangiocarcinoma. These photographs also help to show whether or not a protracted widespread channel between the widespread bile duct and the pancreatic duct exists. Frequently particles or stones may be seen best on the thin-section T2-weighted photographs. Cross-sectional imaging is beneficial to evaluate for cholangiocarcinomas that will come up within the choledochal cyst or, if the affected person has had a partial resection, the remnant parts of the cyst. Cholangiocarcinomas could seem as a mass, irregular thickening of the cyst wall, or much less commonly as papillary nodules arising from the cyst wall. Extrahepatic cholangiocarcinomas associated with choledochal cysts or their remnants are likely to happen in younger adults and are usually much larger in size than the sporadic cholangiocarcinomas that usually happen in the elderly population. Endoscopic retrograde cholangiopancreatography or percutaneous transhepatic cholangiography may be helpful to demonstrate the communication of the choledochal cyst and biliary tract. Direct injection of the ampulla of Vater also helps to define communications with the pancreatic duct. Cystic pancreatic neoplasm: Does not talk with the bile ducts and usually has a multilobulated appearance. Distal biliary stricture: Associated with diffuse upstream bile duct dilatation without focal common bile duct dilatation. Management/Clinical Issues Complete surgical resection of the choledochal cyst prevents the development of cholangiocarcinoma in early adulthood. Longitudinal Doppler ultrasound image through the liver hilum shows an anechoic dilatation of the frequent bile duct without apparent intrahepatic duct dilatation. Developmental and Congenital Disorders of the Bile Duct 489 Key Points Focal dilatations of the bile duct with disproportionately little upstream bile duct dilatation suggests a choledochal cyst. A frequent channel between the common bile duct and pancreatic duct must be sought, since this will likely predispose patients to develop cholangiocarcinoma in early maturity. Risk of subsequent biliary malignancy in patients present process cyst excision for congenital choledochal cysts. Role of magnetic resonance cholangiopancreatography in diagnosing choledochal cysts: case series and review. Forty-year expertise with flow-diversion surgical procedure for sufferers with congenital choledochal cysts with pancreaticobiliary maljunction at a single establishment. Yeh Definition Stones within the bile ducts represent a situation called choledocholithiasis, which can end result from the passage of stones from the gallbladder into the frequent duct or can come up primarily within the bile ducts. Biliary stones are normally composed primarily of cholesterol, but bilirubin pigment stones or these composed of other natural material may occur. Demographic and Clinical Features the demographics of choledocholithiasis are similar to those of gallstones (cholelithiasis). At cholecystectomy, stones are seen within the frequent bile duct in as much as 10% of cases when intraoperative cholangiography is carried out. Nevertheless bile duct stones could happen without gallbladder stones, as in instances of recurrent pyogenic cholangitis. Patients with choledocholithiasis could also be asymptomatic or present with intermittent colicky right-upper-quadrant (A) stomach pain, fever, and infrequently jaundice. Intrabiliary stones predispose sufferers to develop cholangitis and cholangiocarcinoma. Perhaps the most common complication of choledocholithiasis is gallstone pancreatitis, which is the main sort of pancreatitis. Gallstone pancreatitis is thought to happen in two ways: a typical bile duct stone compresses the septum between the widespread bile duct and the pancreatic duct and thereby obstructs the pancreatic duct, or a distal biliary stone in the ampulla of Vater blocks the sphincter of Oddi and permits reflux of biliary fluid into the pancreas, thus inflicting pancreatitis. Imaging Findings Stones could also be rounded or geometric in shape and should have a lamellated appearance on cross-sectional imaging. The dimension and appearance of stones in a given affected person are usually related however broad interpatient variation happens. Common bile duct stones (arrowheads) are seen in (A) a patient after liver transplantation and (B) after cholecystectomy. Common duct stones commonly appear as faceted filling defects that stack one upon one other and are sometimes eccentrically located in the bile duct lumen. Bile duct dilatation is regularly not seen regardless of symptomatic intermittent bile duct obstruction. Longitudinal ultrasound picture exhibits a barely dilated common bile duct with a distal stone (arrow) that has posterior shadowing.