
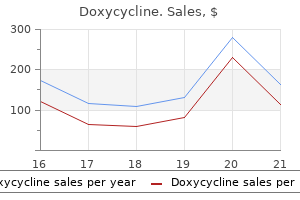
Doxycycline dosages: 200 mg, 100 mg
Doxycycline packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase doxycycline 100 mg with mastercard
Determining driving competence is difficult antibiotics for uti infection symptoms buy discount doxycycline 200 mg on line, especially within the early levels o dementing ailments antibiotics for uti no alcohol doxycycline 200 mg mastercard. An on-the-road driving take a look at and reviews rom amily members could help time choices associated to this crucial exercise. Some o the de cits described on this chapter are so complicated that they may bewilder not solely the patient and amily but also the doctor. It is crucial to perform a scientific medical analysis to characterize the nature o the de cits and clarify them in lay phrases to the patient and amily. An enlightened approach to sufferers with harm to the cerebral cortex requires an understanding o the ideas that link neural networks to greater cerebral unctions in well being and disease. Mille r Gil Ra b in o vici Ma ria Ca rm e la Ta rta g lia Language and memory are essential human unctions. For the experienced clinician, the recognition o di erent types o language and reminiscence disturbances of en supplies important clues to the anatomic localization and diagnosis o neurologic issues. This video illustrates classic issues o language and speech (including the aphasias), reminiscence (the amnesias), and different problems o cognition that are generally encountered in medical apply. More than one-hal o adults within the United States experience no much less than intermittent sleep disturbance, and only 30% o grownup Americans report constantly obtaining a su cient amount o sleep. The Institute o Medicine has estimated that 50�70 million Americans su er rom a persistent disorder o sleep and wake ulness, which may adversely a ect daytime unctioning in addition to bodily and mental health. Over the last 20 years, the eld o sleep medication has emerged as a definite specialty in response to the impact o sleep problems and sleep de ciency on overall well being. Sleep deprivation increases the rapidity o sleep onset and both the depth and quantity o slow-wave sleep. N3 sleep is most intense and prominent throughout childhood, lowering with puberty and across the second and third decades o li. N3 sleep declines during maturity to the point the place it might be completely absent in older adults. It is the increased requency o awakenings, rather than a decreased capability to all again asleep, that accounts or the increased wake ulness during the sleep episode in older individuals. In the United States, adults are inclined to have one consolidated sleep episode every night, though in some cultures sleep may be divided into a mid-a ernoon nap and a shortened night time sleep. This pattern adjustments considerably over the li e span, as in ants and younger youngsters sleep significantly greater than older people. The continuous recording o these electrophysiologic parameters to de ne sleep and wake ulness is termed polysomnography. Characteristic eatures o sleep in older folks embrace reduction o N3 slow-wave sleep, requent spontaneous awakenings, early sleep onset, and early morning awakening. Sleep deprivation degrades cognitive per ormance, particularly on tests that require continual vigilance. Paradoxically, older individuals are much less susceptible to the neurobehavioral per ormance impairment induced by acute sleep deprivation than younger adults, sustaining their response time and sustaining vigilance with ewer lapses o attention. There is rising evidence that sleep de ciency in humans could cause glucose intolerance and contribute to the event o diabetes, weight problems, and the metabolic syndrome, in addition to impaired immune responses, accelerated atherosclerosis, and increased danger o cardiac disease and stroke. For these reasons, the Institute o Medicine declared sleep de ciency and sleep problems "an unmet public well being downside. The ascending arousal neurons use monoamines (norepinephrine, dopamine, serotonin, and histamine), glutamate, or acetylcholine as neurotransmitters to activate their goal neurons. Additional arousal-promoting neurons within the hypothalamus use the peptide neurotransmitter orexin (also generally known as hypocretin, proven in blue) to rein orce activity within the other arousal cell teams. Damage to the arousal system on the degree o the rostral pons and lower midbrain causes coma, indicating that the ascending arousal in uence rom this stage is important in sustaining wake ulness. Damage to the hypothalamic branch o the arousal system causes proound sleepiness, but often not coma. Speci c loss o the orexin neurons produces the sleep problem narcolepsy (see below). Many sleep-promoting neurons are themselves inhibited by inputs rom the arousal system. This mutual inhibition between the arousal- and sleep-promoting techniques orms a neural circuit akin to what electrical engineers call a " ip- op swap. Neurons in the ventrolateral preoptic nucleus, one o the vital thing sleep-promoting websites, are lost during normal human growing older, correlating with decreased capability to maintain sleep (sleep ragmentation). The arousal system in the mind (green) contains monoaminergic, glutamatergic, and cholinergic neurons in the brainstem that activate neurons within the hypothalamus, thalamus, basal orebrain, and cerebral cortex. Orexin neurons (blue) in the hypothalamus, that are lost in narcolepsy, rein orce and stabilize arousal by activating different parts o the arousal system. The neurochemistry o sleep homeostasis is only partially understood, however with prolonged wake ulness, adenosine levels rise in parts o the brain. Adenosine might act via A1 receptors to immediately inhibit many arousal-promoting brain regions. In addition, adenosine promotes sleep via A2a receptors; inhibition o these receptors by ca eine is one o the chie methods during which folks ght sleepiness. Other humoral actors, similar to prostaglandin D2, have also been implicated in this process. Both adenosine and prostaglandin D2 activate the sleep-promoting neurons within the ventrolateral preoptic nucleus. For example, insomnia is fairly common in patients with nervousness and different psychiatric disorders. Stress-induced insomnia is even more widespread, a ecting most people at a while in their lives. However, behavioral approaches (cognitive behavioral remedy and sleep hygiene) that may cut back orebrain limbic exercise at bedtime are o en equally or more success ul. Prominent day by day variations additionally happen in endocrine, thermoregulatory, cardiac, pulmonary, renal, immune, gastrointestinal, and neurobehavioral unctions. At the molecular level, endogenous circadian rhythmicity is driven by sel -sustaining transcriptional/translational eedback loops. In evaluating every day rhythms in people, you will need to distinguish between diurnal components passively evoked by periodic environmental or behavioral adjustments. The genetically determined period o this endogenous neural oscillator, which averages ~24. Humans are exquisitely sensitive to the resetting e ects o gentle, notably the shorter wavelengths (~460�500 nm) o the seen spectrum. Small di erences in circadian interval contribute to variations in diurnal pre erence in young adults (with the circadian period shorter in those that sometimes go to bed and rise earlier in comparability with those who typically go to bed and get up later), whereas adjustments in homeostatic sleep regulation might underlie the age-related tendency toward earlier sleep-wake timing. The timing and inner architecture o sleep are immediately coupled to the output o the endogenous circadian pacemaker.
100 mg doxycycline overnight delivery
Sensory loss and ache normally accompany acute decrease motor neuron weakness; the weak spot generally localizes to a single nerve root or peripheral nerve antibiotics for sinus infection and birth control doxycycline 100 mg buy online, but sometimes re ects plexus involvement gentle antibiotics for acne 200 mg doxycycline order with amex. Relatively symmetric weak point o extraocular or bulbar muscle tissue requently is as a outcome of of a myopathy (Chap. Worsening o relatively symmetric weak spot with atigue is attribute o neuromuscular junction issues. Weakness limited to respiratory muscle tissue is rare and often is due to motor neuron illness, myasthenia gravis, or polymyositis/dermatomyositis (Chap. Weakness and atrophy that develop over weeks or months are often o decrease motor neuron origin. When related to sensory symptoms, a peripheral trigger (nerve, root, or plexus) is most likely going; in any other case, anterior horn cell disease ought to be considered. I weakness is o the upper motor neuron type, a discrete cortical (precentral gyrus) or wire lesion may be responsible, and appropriate imaging is per ormed. Dista l wea kn ess Involvement o two or extra limbs distally suggests decrease motor neuron or peripheral nerve illness. The prototypical constructive symptom is tingling (pins and needles); different constructive sensory phenomena embody itch and altered sensations which are described as pricking, bandlike, lightning-like shooting eelings (lancinations), aching, kni elike, twisting, drawing, pulling, tightening, burning, searing, electrical, or uncooked eelings. Positive phenomena normally outcome rom trains o impulses generated at sites o lowered threshold or heightened excitability along a peripheral or central sensory pathway. The nature and severity o the irregular sensation depend on the number, price, timing, and distribution o ectopic impulses and the sort and unction o nervous tissue in which they arise. Negative phenomena characterize loss o sensory unction and are characterised by diminished or absent eeling that o en is experienced as numbness and by irregular ndings on sensory examination. In issues a ecting peripheral sensation, a minimum of one-hal the a erent axons innervating a specific web site are probably misplaced or unctionless be ore a sensory de cit can be demonstrated by medical examination. Subclinical levels o sensory dys unction may be revealed by sensory nerve conduction studies or somatosensory evoked potentials (Chap. Whereas sensory signs could additionally be both constructive or negative, sensory signs on examination are at all times a measure o negative phenomena. The time period paresthesias usually re ers to tingling or pins-and-needles sensations but might embrace a wide variety o other irregular sensations, except pain; it generally implies that the irregular sensations are perceived spontaneously. The extra common time period dysesthesias denotes all kinds o abnormal sensations, including ache ul ones, regardless o whether a stimulus is clear. Hypesthesia or hypoesthesia re ers to a reduction o cutaneous sensation to a speci c sort o testing such as pressure, gentle touch, and heat or chilly stimuli; anesthesia, to a whole absence o pores and skin sensation to the identical stimuli plus pinprick; and hypalgesia or analgesia, to reduced or absent ache perception (nociception). Similarly, allodynia describes the state of affairs during which a nonpain ul stimulus, as soon as perceived, is skilled as pain ul, even excruciating. Disorders o deep sensation arising rom muscle spindles, tendons, and joints a ect proprioception (position sense). Mani estations embrace imbalance (particularly with eyes closed or within the dark), clumsiness o precision actions, and unsteadiness o gait, that are re erred to collectively as sensory ataxia. Other ndings on examination often, however not invariably, include decreased or absent joint position and vibratory sensibility and absent deep tendon re exes within the a ected limbs. The Romberg signal is optimistic, which signifies that the affected person sways markedly or topples when requested to stand with eet close together and eyes closed. Continuous involuntary actions (pseudoathetosis) o the outstretched hands and ngers occur, particularly with eyes closed. The spinothalamic tract (pain, thermal speci c stimuli, size and distinctness o sense) and the posterior column�lemniscal system (touch, strain, joint position) receptive elds, and adaptational qualities. O shoots rom the ascending anterolateral asciculus (spinothalamic A erent bers in peripheral nerve trunks tract) to nuclei in the medulla, pons, and mesencephalon and nuclear terminations traverse the dorsal roots and enter the dor- o the tract are indicated. This within the tegmentum o the pons and midbrain and synis the spinothalamic pathway or anterolateral system. This large- ber system is re erred to as the posterior column�medial lemniscal pathway (lemniscal, or short). Although the ber types and unctions that make up the spinothalamic and lemniscal methods are comparatively well known, many other bers, significantly those related to touch, pressure, and place sense, ascend in a di usely distributed sample each ipsilaterally and contralaterally in the anterolateral quadrants o the spinal twine. This explains why an entire lesion o the posterior columns o the spinal cord could additionally be related to little sensory de cit on examination. In sufferers with sensory complaints, testing ought to start in the center o the a ected region and proceed radially until sensation is perceived as regular. The examiner should consider whether the sensory symptoms are a disguised request or help with psychologic or situational problems. Evaluation o stance and gait additionally checks the integrity o motor and cerebellar methods. The affected person is asked to close the eyes and ocus on the pricking or unpleasant quality o the stimulus, not simply the strain or contact sensation elicited. Areas o hypalgesia should be mapped by proceeding radially rom the most hypalgesic site. An different way to take a look at chilly sensation is to contact a metal object, corresponding to a tuning ork at room temperature, to the skin. The examiner must depend on patient responses, and this complicates interpretation. In a stuporous affected person, or instance, sensory examination is reduced to observing the briskness o withdrawal in response to a pinch or one other noxious stimulus. The appreciation o each cold and warmth ought to be tested as a end result of di erent receptors reply to every. The affected person is tested with the eyes closed and will point out as soon because the stimulus is perceived, indicating its location. The digit is held by its sides, distal to the joint being examined, and moved passively whereas more proximal joints are stabilized-the patient signifies the change in position or path o motion. A take a look at o proximal joint position sense, primarily at the shoulder, is per ormed by asking the affected person to deliver the 2 index ngers along with arms prolonged and eyes closed. The sense o vibration is tested with an oscillating tuning ork that vibrates at 128 Hz. Vibratory thresholds at the same web site in the patient and the examiner may be in contrast or management functions. Quantitative sensory testing is especially use ul or serial evaluation o cutaneous sensation in clinical trials. T reshold testing or contact and vibratory and thermal sensation is the most extensively used software. Stereognosis re ers to the power to identi y frequent objects by palpation, recognizing their form, texture, and dimension. Patients with regular stereognosis ought to have the power to distinguish a dime rom a penny and a nickel rom a quarter with out looking. I primary sensation is altered, these cortical discriminative unctions usually might be irregular additionally. Comparisons ought to at all times be made between analogous websites on the two sides o the body as a outcome of the de cit with a speci c parietal lesion is prone to be unilateral. Two-point discrimination is examined with special calipers, the factors o which can be set rom 2 mm to a quantity of centimeters apart and then applied concurrently to the test website.
Doxycycline 100 mg buy overnight delivery
Although it may be used to supplement infection ear piercing buy 100 mg doxycycline with visa, or reconfirm antimicrobial irrigation doxycycline 200 mg visa, canal size obtained by other strategies, the paper level technique is inappropriate as a primary methodology for working size willpower. Root Canal Irrigation In instances with radiographic and/or scientific indicators of an infection, the root canal system harbours microorganisms,20 which are present in a planktonic kind and as a biofilm adhering to the canal partitions. The aims of root canal irrigation are to22,26: � cut back intraradicular microorganisms and neutralise endotoxins; � dissolve vital or necrotic pulp tissue; 7 Preparation of the Root Canal System 119 � lubricate the canal walls and devices; � facilitate elimination of dentine particles and debris. The primary necessities of a root canal irrigant are: � broad antimicrobial spectrum; � unhazardous; � tissue-dissolution functionality; � capacity to penetrate into areas inaccessible to root canal devices. In addition, a root canal irrigant should have a low surface pressure, is stable, inexpensive and easy to use. Removal of the smear layer helps to open up dentinal tubules, remove embedded microorganisms and facilitate higher penetration of the antimicrobial irrigant, to enable more in depth canal decontamination and improved canal cleanliness. Irrigation solutions are commonly delivered using specifically designed endodontic needles and syringes. Flexible open-ended irrigation needles are beneficial so that the needle may be bent in accordance with the canal curvature. As canal preparation proceeds, the needle will steadily reach deeper into the canal; always, the needle should not be jammed into the canal and the irrigant must not be delivered with pointless force. Root Canal Preparation All root canal methods are curved in one or more planes, with the diploma and extent of curvature varying from root to root. Irrespective of the instrumentation technique used, the apical a half of the basis canal system is normally the least properly cleaned and ready. Preparation of the basis canal system requires appreciable ability, significantly in cases with more severely curved canals or different advanced anatomical options. Despite advances in instrument design, the expertise and abilities of the operator stays necessary. Currently, the obtainable proof is proscribed relating to the impression of maintenance of the original canal shape, throughout root canal preparation, on remedy consequence. Coronal flaring: Use Gates-Glidden burs or NiTi devices designed to open the canal orifice and enlarge the coronal aspect of the basis canal. Irrigate with sodium hypochlorite between every instrument change and throughout canal preparation. Glide path/pilot channel: Use hand instruments and a submitting or Balance-force motion to create a pathway to working size. Apical preparation and ending: Canal preparation continues with hand or engine-driven NiTi instruments in sequence, to working size, until the desired taper and apical size is achieved. This method, using a small dimension file, is usually carried out in the initial negotiation of the foundation canal. Once the file has reached the desired length, circumferential submitting, involving an in-out, push-pull filing action whereas simultaneously transferring the file circumferentially around the canal partitions, is used to instrument the foundation canal. Circumferential filing may be used to prepare straight or comparatively straight canals. However, in a curved canal, circumferential submitting will lead to preferential removal of dentine from the inside curve of the foundation canal and the risk of a strip perforation. The mesial roots of mandibular molars and the mesiobuccal roots of maxillary molars are the teeth most at risk from this iatrogenic problem. Anticurvature filing42 is a method for preparing a curved root canal by which extra dentine is selectively removed from the outer, in contrast with the inside, curve of the root. These devices have been warmth tempered, have a modified tip geometry and exhibit higher buckling resistance in contrast with typical chrome steel instruments. As a result, more stress can be utilized to negotiate calcified canals with these devices, and they present wonderful tactile feedback. When a stainless steel instrument is used in a curved root canal, as a result of the restoring forces, it tends to straighten up, and this increases the likelihood of creating canal aberrations such as a zip or ledge. Regardless of the hand instrumentation method used, the probability of canal straightening will increase as the dimensions of the stainless-steel instrument or the degree of canal curvature will increase. The course of can be repeated two or three times earlier than removing the instrument to clear the flutes and irrigate the canal. Compared with different hand instrumentation strategies, the Balanced Force idea was reported to permit preparation of curved canals with much less canal straightening, related to less apically extruded debris44 and resulted in improved canal cleanliness. NiTi instruments are capable of return to their original shape even after substantial deformation (up to 10%) as soon as the load is eliminated, whereas with stainless steel instruments, deformation of simply 1% leads to permanent shape alteration. Instruments should never be compelled apically, so excessive stress on the instruments during preparation have to be averted. Regular inspection ought to be carried out, when the devices are withdrawn from the canal, to examine for damages or signs of potential instrument separation. Advantages of NiTi instruments include: � excellent shaping capacity, even in severely curved root canals and sophisticated canal anatomies. A predetermined sequence of instruments of various tapers (see Table 7-2) � often from bigger to smaller sizes � are required whereby each successively smaller instrument might be superior barely deeper into the root canal than the preceding instrument. The full working length is usually reached after usage of the third or fourth instrument of a particular sequence. Disadvantages embody: � the need for comparatively more time and instruments, hence additionally value, to totally form a root canal; � an extended learning curve, as with some systems, instrument sequences range relying on the foundation canal anatomy. The sequence starts with the smallest dimension instrument and progressively larger sizes are all used 7 Preparation of the Root Canal System a hundred twenty five to full working size. Advantages of this technique include: � simpler to learn; � fewer devices required compared with the Crown-Down method; � easier and extra speedy canal preparation in contrast with the Crown-Down method. Disadvantages include: � the later introduction of irrigation solutions into the apical third of the canals in contrast with the Crown-Down method; � larger threat of contaminated coronal pulp tissue being transported into the apical part of the root canal. F360 (Brasseler, Lemgo, Germany) and OneShape (Micro-M�ga, Besan�on, France), and people used in reciprocating motion. The Single-File methods F360 (Brasseler) and OneShape (Micro-Mega) work in a clockwise, rotational motion. The currently available proof suggests that their shaping ability in curved root canals is as good as that of the reciprocating Single-File techniques and rotary Multiple-File NiTi techniques. The fact that the angle within the chopping direction is bigger than that within the clockwise path enables the instrument to continue to progress apically. These angles of motion are particular to the design of the particular instruments56 and are programmed into an electronic motor, which is required. To, a minimum of, partially compensate for the reduced time and length for the irrigant to work, a greater quantity of the irrigant must be used, and additional activation of the irrigation resolution is advisable. In abstract, advantages of the Single-File system embrace: � considerably quicker preparation; up to 60% discount compared with the Single-Length method; � excellent shaping capability; � lowered number of devices; � shorter studying curve. Disadvantages embody: � inconclusive proof relating to the increased risk of apical debris extrusion and creation of dentinal cracks associated with the use of reciprocating Single-File techniques; � reduced time for irrigation; particular measures wanted to enhance canal cleanliness and disinfection. Conventional NiTi alloy has an austenite structure62�64 and its composition is about 55% nickel and 45% titanium in weight; whereas, M-wire consists of 55. The alloy construction of M-wire is finer and extra homogenous than that of austenite NiTi. It is claimed that this extra particular heat remedy increases the flexibility and resistance to cyclic fatigue of the resultant NiTi devices. Learning Outcomes After completion of this chapter, the reader ought to have the flexibility to describe and focus on the: � steps to undertake to achieve access to the basis canal system; � methods of determining working size; � medical relevance of root canal irrigation; � advantages and downsides of root canal hand instruments; � different ideas of engine-driven root canal preparation utilizing NiTi instruments, including controversies related to the use of SingleFile techniques, the advantages of newer NiTi alloys and different improvements.
Generic 200 mg doxycycline amex
All of the next are problems due to bacteria 2 game generic 200 mg doxycycline with mastercard faulty myosin heavy chain 9 gene positioned at 22q11 01 bacteria doxycycline 200 mg buy fast delivery, except: A. All of the next are established causes of thrombocytopathia (platelet dysfunction) besides: A. Presence of reactive lymphocytes should set off search for an underlying lymphoproliferative dysfunction C. B Pelger-Huet anomaly is a benign condition during which the overwhelming majority of neutrophils (>75%) have a bilobed nucleus. Occasional presence of neutrophils similar to Pelger-Huet cells may be seen in individuals with myelodysplastic syndrome. B Alder-Reilly is one other benign condition where giant azurophilic granules are seen within the cytoplasm of granulocytes as well as lymphocytes and monocytes. C May-Hegglin anomaly is characterized by thrombocytopenia, large platelets and the presence of Dohle like our bodies in neutrophil cytoplasm. A Chediak-Higashi syndrome is a uncommon multisystemic disease, transmitted as autosomal recessive. There is elevated incidence of lymphoreticular malignancies, especially in childhood. Rare causes: hereditary neutrophilia, idiopathic neutrophilia, leukocyte adhesion deficiency 6. Significant neutrophilic leukocytosis with left shift is termed as leukemoid response. In the current past leukocyte alkaline phosphatase score was accomplished to assist differentiate the two situations. B Neutropenia is a situation the place the neutrophil count is greater than two standard deviations below the traditional depend. However, neutrophil counts under 35 Section 1: Non-Neoplastic Hematology 500/mm3 can lead to important infections which can be life threatening. There can be a familial type of this condition, transmitted as autosomal dominant. Here happens a mutation in the gene coding for the granulocyte colony stimulating factor. Shwachmann-Diamond syndrome: right here occurs neutropenia, thrombocytopenia, short stature, mental retardation and exocrine pancreatic insufficiency. This disorder is thought to progress to myelodysplastic syndrome and acute myeloid leukemia. C Lymphocytosis typically accompanies viral infections; nevertheless, infection due to Bordetella pertussis is an exception. There are three types of Downey cells: I: these are small cells with indented/irregular nuclei, condensed nuclear chromatin, and minimal cytoplasm. These cells have ample pale blue cytoplasm which surrounds and seems to "hug" adjoining red blood cells. In infectious mononucleosis, evaluate of the peripheral blood might show characteristic options which are: A. Patients have thrombocytopenia, dysfunctional platelets, small platelets, eczema and immunodeficiency. X-linked thrombocytopenia is a congenital disorder where isolated thrombocytopenia with small platelets occurs. Bernard Soulier syndrome is characterized by thrombocytopenia with giant and large platelets. B Bernard Souiler syndrome is characterised by thrombocytopenia and macrothrombocytes. Some cases of Bernard Soulier syndrome are due to defects of the gene, situated on chromosome 22. This gene may be affected in velocardiofacial syndrome or Di George syndrome associated with the deletion of 22q11. A Familial thrombocytosis is due to a mutation within the thrombopoietin receptor gene. Causes of secondary thrombocytosis include infections, inflammatory states, iron deficiency, neoplasms and postsplenectomy states. Disorders of platelet activation: Chediak Higashi syndrome, storage pool problems, Hermansky Pudlak syndrome three. Atypical lymphocytes are typically considered to be lymphocytes which are suspicious for underlying lymphoproliferative issues. The mild zone in the germinal centre consists of centrocytes, where the mitotic price is excessive D. Features that assist follicular hyperplasia, quite than follicular lymphoma, are: A. Regarding Toxoplasma gondii infection and lymphadenopathy, all of the following are true except: A. Primary infection with Toxoplasma gondii during pregnancy could result in congenital toxoplasmosis D. Toxoplasma lymphadenopathy is characterised by follicular hyperplasia, clusters of epithelioid histicocytes and clusters of monocytoid B-cells 7. Microscopic examination of an enlarged lymph node demonstrates dilatation of sinuses with massive lipid vacuoles. An example of granulomatous lymphadenopathy as a end result of noninfectious trigger contains: A. An excisional biopsy is carried out and histology demonstrates necrotic areas within the paracortex with the presence of karyorrhectic particles. A 20-year-old Asian male has eosinophilia and high ranges of IgE with cervical lymphadenopathy. Excisional biopsy of the lymph node demonstrates follicular hyperplasia, intense eosinophilia and eosinophilic microabscesses. Paracortical hyperplasia with macrophages containing brown melanin pigment in lymph nodes draining areas of skin concerned with inflammation is a function of: A. Langerhans Cell Histiocytosis differs from Rosai Dorfman disease in all of the following points except: A. Eosinophils are sometimes present in Langerhans cell histiocytosis however not in Rosai Dorfman illness D. Langerhans cells have nuclear grooves, a feature not seen throughout the macrophages of Rosai Dorfman illness 15. A affected person with lymphadenopathy undergoes excisional biopsy for further evaluation. D Secondary follicles are derived from main follicles after antigenic stimulation. The main follicles consists of na�ve B-cells that transfer into the germinal facilities when stimulated. Tingible body macrophages which are responsible for cleaning up of cells are also low on this space.
Doxycycline 200 mg buy fast delivery
They present short-term c inica bene t by lowering the severity and shortening the period o assaults homemade antibiotics for acne doxycycline 200 mg generic without prescription. Whether therapy supplies any ong-term bene t on the course o the i ness is ess c ear antibiotic 93 3109 200 mg doxycycline discount fast delivery. G ucocorticoid therapy is usua y administered as intravenous methy predniso one, 500�1000 mg/d or 3�5 days, both without a taper or o owed by a course o ora prednisone beginning at a dose o 60�80 mg/d and gradua y tapered over 2 weeks. Ora y administered methy prednisoone or dexamethasone (in equiva ent dosages) may be substituted or the intravenous portion o the remedy, a although gastrointestina comp ications are more widespread by this route. Side e ects o short-term g ucocorticoid remedy inc ude uid retention, potassium oss, weight achieve, gastric disturbances, acne, and emotiona abi ity. Lithium carbonate (300 mg ora y bid) may he p to manage emotiona abi ity and insomnia associated with g ucocorticoid therapy. Patients with a history o peptic u cer illness could require cimetidine (400 mg bid) or ranitidine (150 mg bid). P asma trade (ve to seven exchanges: 40�60 mL/kg per trade, each other day or 14 days) may bene t sufferers with u minant attacks o demye ination which would possibly be unresponsive to g ucocorticoids. Side e ects can usua y be managed with concomitant nonsteroida anti-in ammatory medications. Depression, increased spasticity, and cognitive adjustments have been reported, a although these signs can a so be because of the under ying disease. Paradoxica y, nevertheless, these identical tria s, regardless of plentiful statistica power, ai ed to show any concomitant impression on the c inica outcomes o disabi ity and re apse price. For a patient doing we on therapy, the presence o antibodies shou d not a ect therapy. G atiramer acetate is administered by subcutaneous injection o both 20 mg daily or 40 mg thrice week y. In addition, approximate y 15% o sufferers expertise one or more episodes o ushing, chest tightness, dyspnea, pa pitations, and nervousness a ter injection. Fina y, some patients experience ipoatrophy, which, every so often, can be dis iguring and require cessation o treatment. Natalizumab Nata izumab is a humanized monoc ona anti- physique directed towards the four subunit o 41 integrin, a ce u ar adhesion mo ecu e expressed on the sur ace o ymphocytes. However, its re ative e icacy compared to different agents has not been estab ished conc usive y. A sma share (<10%) o sufferers experience hypersensitivity reactions (inc uding anaphy axis), and ~6% deve op neutra izing antibodies to the mo european e (on y ha o which persist). [newline]Af er this time, in antibody-positive sufferers, a change to one other disease-modi ying therapy shou d be robust y considered. By distinction, persistent y antibody-negative sufferers may be continued on treatment inde nite y. Fingolimod Fingo imod is a sphingosine-1-phosphate (S1P) inhibitor that stops the egress o ymphocytes rom the secondary ymphoid organs such because the ymph nodes and sp een. It is we to erated, and the dai y ora dosing schedu e makes it very convenient or sufferers. First- and second-degree heart b ock and bradycardia can a so occur when ngo imod therapy is initiated. A 6-h period o observation (inc uding e ectrocardiogram monitoring) is beneficial or a sufferers receiving their rst dose, and individua s with preexisting cardiac illness shou d probab y not be treated with this agent. However, its twice-dai y ora dosing schedu e makes it somewhat ess convenient or sufferers than dai y ora therapies. Gastrointestina side e ects (abdomina discom ort, nausea, vomiting, ushing, and diarrhea) are widespread initially o remedy however genera y subside with continued administration. Neverthe ess, these reviews underscore the act, stated earlier y, that ong-term sa ety can by no means be assured by the resu ts o short-term tria s. It is we to erated, and its dai y ora dosing schedu e makes it very handy or sufferers. A main limitation, particularly in girls o childbearing age, is its potential teratogenicity (pregnancy category X); teri lunomide can stay within the bloodstream or 2 years, and it is strongly recommended that exposed women and men who want to conceive receive cholestyramine or activated charcoal to get rid of residual drug. Despite this broad indication, nevertheless, the information supporting its e icacy are weaker than or different approved therapies. At presently approved doses (12 mg/m 2 each three months), the utmost length o remedy may be solely 2�3 years. In usion-related reactions, mostly observed with the irst in usion and often gentle in degree, have been probably the most signi icant side e ect noted. Ocrelizumab 600 mg is administered by intravenous in usion each 24 weeks (administered as two 300-mg in usions spaced two weeks aside or the irst dose, and as a single 600-mg in usion therea ter); intravenous methylprednisolone 100 mg is given prior to each in usion and elective prophylaxis with analgesics/antipyretics and antihistamines are beneficial, along with adjustment o the in usion price to handle in usion-related reactions. It causes lymphocyte depletion (o each B and T cells) and a change in the composition o lymphocyte subsets. Both o these modifications, particularly the impact on lymphocyte subsets, are lengthy lasting. In two part 3 trials, nonetheless, its influence on scientific incapacity was less convincing. Despite these unknowns, clinicians must make choices primarily based on one of the best out there proof, coupled with practical issues. However, its use is imited as a end result of o its high price, questions about optima dose, and uncertainty about its having any impression on ong-term disabi ity. Methylprednisolone, administered in a single study as month y high-dose intravenous pu ses, decreased disabi ity progression (see above). Certain y, any potentia y harmful surgical procedure shou d be averted unti extra rigorous science is avai ab. Because cyc ophosphamide can be used or intervals in extra o 3 years, it may be pre erab e to mitoxantrone in these circumstances. Spasticity and spasms may improve with physica therapy, regu ar train, and stretching. E ective medicines inc ude bac o en (20�120 mg/d), diazepam (2�40 mg/d), tizanidine (8�32 mg/d), dantro ene (25� 400 mg/d), and cyc obenzaprine hydroch oride (10�60 mg/d). The princip e concern with the use o these brokers is the possibi ity o inducing seizures at excessive doses. Pain is handled with anticonvu sants (carbamazepine, 100�1000 mg/d; phenytoin, 300�600 mg/d; gabapentin, 300� 3600 mg/d; or pregaba in, 50�300 mg/d), antidepressants (amitripty ine, 25�150 mg/d; nortripty ine, 25�150 mg/d; desipramine, 100�300 mg/d; or ven a axine, 75�225 mg/d), or antiarrhythmics (mexi etine, 300�900 mg/d). I these approaches ai, patients shou d be re erred to a complete pain management program. Evening uid restriction or requent vo untary voiding may he p detrusor hyperre exia. I these methods ai, propanthe ine bromide (10�15 mg/d), oxybutynin (5�15 mg/d), hyoscyamine su ate (0. Detrusor/sphincter dyssynergia might reply to phenoxybenzamine (10�20 mg/d) or terazosin hydroch oride (1�20 mg/d). Prevention by urine acidi cation (with cranberry juice or vitamin C) inhibits some micro organism. Prophy actic administration o antibiotics is sometimes essential however could ead to co onization by resistant organisms.
Papagallo (Poinsettia). Doxycycline.
- How does Poinsettia work?
- Are there safety concerns?
- Fever, pain, infection, warts, skin disorders, toothache, and other conditions.
- What is Poinsettia?
- Dosing considerations for Poinsettia.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96479
Discount 200 mg doxycycline
Gastrointestinal side e ects are ewer when utilizing the delayed-release ormulation (Depakote) virus x reader dmmd doxycycline 100 mg buy online. Laboratory testing is required to monitor toxicity because valproic acid can rarely trigger reversible bone marrow suppression and hepatotoxicity uti antibiotics have me yeast infection safe doxycycline 100 mg. This drug should usually be avoided in patients with preexisting bone marrow or liver illness. Irreversible, atal hepatic ailure showing as an idiosyncratic quite than dose-related facet e ect is a comparatively uncommon complication; its threat is highest in children <2 years old, particularly those taking different antiepileptic drugs or with inborn errors o metabolism. Zonisamide, tiagabine, gabapentin, lacosamide, and ezogabine are additional medication currently used or the treatment o ocal seizures with or with out evolution into generalized seizures. Phenobarbital and other barbiturate compounds had been commonly used in the past as rst-line therapy or many orms o epilepsy. However, the barbiturates requently trigger sedation in adults, hyperactivity in children, and other more delicate cognitive modifications; thus, their use ought to be restricted to situations by which no other suitable remedy alternate options exist. A ntiepileptic drug selection for generalized seizures Lamotrigine and 317 valproic acid are presently thought of the best preliminary choice or the remedy o major generalized, tonic-clonic seizures. Valproic acid can be particularly e ective in absence, myoclonic, and atonic seizures. It is there ore the drug o choice in patients with generalized epilepsy syndromes having combined seizure types. Importantly, carbamazepine, oxcarbazepine, and phenytoin can worsen sure types o generalized seizures, including absence, myoclonic, tonic, and atonic seizures. Periodic monitoring o blood cell counts is required since ethosuximide not often causes bone marrow suppression. Initiation and monitoring of therapy Because the response to any antiepileptic drug is unpredictable, sufferers must be careully educated concerning the approach to remedy. The goal is to stop seizures and reduce the aspect e ects o therapy; determination o the optimal dose is o en a matter o trial and error. Most antiepileptic medicine have to be introduced comparatively slowly to reduce side e ects. Patients should anticipate that minor side e ects corresponding to mild sedation, slight adjustments in cognition, or imbalance will sometimes resolve inside a ew days. Starting doses are usually the lowest value listed underneath the dosage column in ready 31-9. Subsequent will increase ought to be made only a er achieving a gradual state with the previous dose. Monitoring o serum antiepileptic drug ranges may be very use ul or establishing the preliminary dosing schedule. However, the published therapeutic ranges o serum drug concentrations are only an approximate guide or figuring out the correct dose or a given patient. The key determinants are the medical measures o seizure requency and presence o aspect e ects, not the laboratory values. These sufferers may have a "subtherapeutic" drug degree, but the dose must be modified solely i seizures remain uncontrolled, not just to obtain a "therapeutic" degree. In follow, other than through the initiation or modi cation o remedy, monitoring o antiepileptic drug ranges is most use ul or documenting adherence. I seizures continue despite gradual increases to the utmost tolerated dose and documented compliance, then it becomes essential to change to another antiepileptic drug. This is normally accomplished by maintaining the patient on the rst drug whereas a second drug is added. The dose o the second drug must be adjusted to decrease seizure requency with out causing toxicity. The dose o the second drug is then urther optimized based mostly on seizure response and facet e ects. The appropriate seizure- ree interval is unknown and undoubtedly varies or di erent orms o epilepsy. However, it seems affordable to try withdrawal o remedy a er 2 years in a patient who meets all o the above standards, is motivated to discontinue the medicine, and clearly understands the potential risks and bene ts. Most recurrences happen within the rst three months a er discontinuing therapy, and sufferers should be suggested to keep away from potentially harmful conditions such as driving or swimming during this period. There are presently no clear pointers or rational polypharmacy, though in concept a combination o drugs with di erent mechanisms o action may be most use ul. I these drugs are unsuccess ul, then the addition o different drugs similar to topiramate, zonisamide, lacosamide, or tiagabine is indicated. Patients with myoclonic seizures proof against valproic acid might bene t rom the addition o clonazepam or clobazam, and people with absence seizures may respond to a combination o valproic acid and ethosuximide. For some, surgical procedure may be extraordinarily e ective in substantially reducing seizure requency and even offering complete seizure control. Rather than submitting the patient to years o unsuccess ul medical remedy and the psychosocial trauma and elevated mortality related to ongoing seizures, the patient should have an ef cient however relatively brie attempt at medical therapy after which be re erred or surgical analysis. The most typical surgical process or patients with temporal lobe epilepsy includes resection o the anteromedial temporal lobe (temporal lobectomy) or a more limited elimination o the underlying hippocampus and amygdala (amygdalohippocampectomy). Focal seizures arising rom extratemporal areas could additionally be abolished by a ocal neocortical resection with exact removal o an identi ed lesion (lesionectomy). The exact extent o the resection to be undertaken may additionally be determined by per orming cortical mapping on the time o the surgical process, permitting or a tailor-made resection. This includes electrocorticographic recordings made with electrodes on the sur ace o the brain to identi y the extent o epilepti orm disturbances. I the region to be resected is within or near mind areas suspected o having sensorimotor or language unction, electrical cortical stimulation mapping is per ormed on the awake patient to decide the unction o cortical regions in query to find a way to keep away from resection o so-called eloquent cortex and thereby decrease postsurgical de cits. Advances in presurgical evaluation and microsurgical techniques have led to a steady increase in the success o epilepsy surgery. Clinically signi cant issues o surgical procedure are <5%, and the use o unctional mapping procedures has markedly reduced the neurologic sequelae due to removing or sectioning o mind tissue. For instance, about 70% o patients handled with temporal lobectomy will become seizure ree, and another 15�25% could have at least a 90% reduction in seizure requency. Marked enchancment can also be normally seen in sufferers handled with hemispherectomy or catastrophic seizure issues as a result of giant hemispheric abnormalities. Postoperatively, sufferers typically have to remain on antiepileptic drug therapy, but the marked reduction o seizures ollowing resective surgery can have a very bene cial e ect on high quality o li. Not all medically re ractory sufferers are appropriate candidates or resective surgery. For example, some sufferers have seizures arising rom a couple of location, making the chance o ongoing seizures or potential harm rom the surgery unacceptably excessive. The duration o seizure exercise su cient to meet the de nition o status epilepticus has historically been speci ed as 15�30 min.
Generic 200 mg doxycycline with amex
Fluoride therapy to prevent hearing loss rom cochlear otosclerosis is o uncertain worth antibiotics for uti penicillin 100 mg doxycycline buy free shipping. There are normally two major openings antibiotic resistance facts purchase 100 mg doxycycline, or home windows, that join the inside ear with the middle ear and function conduits or transmission o sound; these are, respectively, the oval and spherical windows. A third window is ormed where the usually hard otic bone surrounding the internal ear is eroded; dissipation o the acoustic energy at the third window is responsible or the "internal ear conductive hearing loss. A widespread symptom is vertigo evoked by loud sounds (ullio phenomenon), by Valsalva maneuvers that change center ear strain, or by making use of constructive pressure on the tragus (the cartilage anterior to the external opening o the ear canal). Patients with this syndrome additionally complain o having the flexibility to hear the motion o their eyes and neck. A giant jugular bulb or jugular bulb diverticulum can create a "third window" by eroding into the vestibular aqueduct or posterior semicircular canal; the symptoms are just like these o the superior semicircular canal dehiscence syndrome. Sen so rineura l hea rin g lo ss Sensorineural hearing loss results rom either harm to the mechanotransduction equipment o the cochlea or disruption o the electrical conduction pathway rom the inner ear to the brain. Damage to the hair cells o the organ o Corti may be brought on by intense noise, viral in ections, ototoxic medication. Congenital mals ormations o the inside ear may be the trigger o listening to loss in some adults. Genetic predisposition alone or in live performance with environmental exposures may also be responsible (see below). Presbycusis (age-associated hearing loss) is the commonest trigger o sensorineural hearing loss in adults. More importantly, the hearing impairment is related to signi cant loss in readability. There is a loss o discrimination or phonemes, recruitment (abnormal growth o loudness), and explicit di culty in understanding speech in noisy environments such as at eating places and social occasions. Hearing aids are helpul in enhancing the signal-to-noise ratio by ampli ying sounds which may be close to the listener. The audiogram exhibits a moderate to severe downsloping sensorineural hearing loss typical o presbyacusis. The loss o high- requency hearing is associated with a decreased speech discrimination score; consequently, sufferers complain o lack o readability o listening to, especially in a noisy background. Cochlear implants are the therapy o choice when listening to aids show inadequate, even when listening to loss is incomplete (see below). Diuretics, a short course o glucocorticoids, and intratympanic gentamicin may be use ul adjuncts in recalcitrant cases. Surgical therapy o vertigo is reserved or unresponsive circumstances and consists of endolymphatic sac decompression, labyrinthectomy, and vestibular nerve part. Both labyrinthectomy and vestibular nerve part abolish rotatory vertigo in >90% o cases. Primary ailments o the central nervous system can even current with hearing impairment. Characteristically, a reduction in clarity o listening to and speech comprehension is much higher than the loss o the flexibility to hear pure tone. Hearing loss can accompany hereditary sensorimotor neuropathies and inherited disorders o myelin. Multiple sclerosis might current with acute unilateral or bilateral hearing loss; usually, pure tone testing stays comparatively steady while speech understanding uctuates. Isolated labyrinthine in arction can current with acute hearing loss and vertigo as a result of a cerebrovascular accident involving the posterior circulation, often the anterior in erior cerebellar artery; it might also be the heralding sign o impending catastrophic basilar artery in arction (Chap. A nding o conductive and sensory listening to loss in combination is termed combined hearing loss. Mixed hearing losses are as a result of pathology o both the center and inner ear, as can occur in otosclerosis involving the ossicles and the cochlea, head trauma, persistent otitis media, cholesteatoma, center ear tumors, and a few internal ear mal ormations. Trauma resulting in temporal bone ractures may be related to conductive, sensorineural, or blended hearing loss. I the racture spares the inside ear, there might merely be conductive hearing loss due to rupture o the tympanic membrane or disruption o the ossicular chain. Pro ound hearing loss and extreme vertigo are related to temporal bone ractures involving the internal ear. A perilymphatic stula associated with leakage o internal ear uid into the center ear can happen and should require surgical repair. Computed tomography (C) is greatest suited to assess racture o the traumatized temporal bone, evaluate the ear canal, and decide the integrity o the ossicular chain and the involvement o the inner ear. Cerebrospinal uid leaks that accompany temporal bone ractures are normally sel -limited; the worth o prophylactic antibiotics is unsure. It may have a buzzing, roaring, or ringing high quality and may be pulsatile (synchronous with the heartbeat). The cause o the tinnitus can often be determined by nding the trigger o the associated hearing loss. It is most commonly related to some abnormality o the jugular bulb corresponding to a large jugular bulb or jugular bulb diverticulum. In general, the listening to loss associated with dominant genes has its onset in adolescence or maturity, varies in severity, and progresses with age, whereas the hearing loss related to recessive inheritance is congenital and pro ound. The 167del mutation is extremely prevalent in Ashkenazi Jews; ~1 in 1765 people on this inhabitants are homozygous and a ected. The hearing loss can also range among the many members o the same amily, suggesting that different genes or actors in uence the auditory phenotype. Sensitivity to aminoglycoside ototoxicity can be maternally transmitted through a mitochondrial mutation. The historical past should elicit characteristics o the hearing loss, together with the period o dea ness, unilateral versus bilateral involvement, nature o onset (sudden vs insidious), and fee o progression (rapid vs slow). Symptoms o tinnitus, vertigo, imbalance, aural ullness, otorrhea, headache, acial nerve dys unction, and head and neck paresthesias should be famous. In ormation regarding head trauma, exposure to ototoxins, occupational or leisure noise publicity, and amily historical past o hearing impairment may be essential. A sudden onset o unilateral listening to loss, with or with out tinnitus, could characterize a viral in ection o the internal ear, vestibular schwannoma, or a stroke. Patients with unilateral listening to loss (sensory or conductive) usually complain o decreased hearing, poor sound localization, and di culty listening to clearly with background noise. Small vestibular schwannomas usually current with uneven hearing impairment, tinnitus, and imbalance (rarely vertigo); cranial neuropathy, in particular o the trigeminal or acial nerve, might accompany bigger tumors. Hearing loss with otorrhea is more than likely because of chronic otitis media or cholesteatoma. Examination ought to embody the auricle, external ear canal, and tympanic membrane. In examining the eardrum, the topography o the tympanic membrane is extra necessary than the presence or absence o the sunshine re ex. In addition to the pars tensa (the lower two-thirds o the tympanic membrane), the pars accida (upper one-third o the tympanic membrane) above the short process o the malleus must also be examined or retraction pockets that may be evidence o chronic eustachian tube dysunction or cholesteatoma. Insuf ation o the ear canal is important to assess tympanic membrane mobility and compliance. Care ul inspection o the nostril, nasopharynx, and higher respiratory tract is indicated.

200 mg doxycycline cheap mastercard
When plaque or calculus is encountered on probing treatment for sinus infection home remedies purchase 200 mg doxycycline amex, the therapy and prognosis of the tooth are altered; the tooth now requires each endodontic and periodontal therapies antibiotic resistance vre cheap doxycycline 100 mg amex. If the endodontic therapy is enough, prognosis is decided by the severity of the marginal periodontal damage and the efficacy of periodontal therapy. With endodontic remedy alone, solely part of the lesion will heal to the extent of the secondary periodontal lesion. Primary endodontic lesions with secondary periodontal involvement may also occur because of root 270 thirteen Marginal Periodontitis and the Dental Pulp increasing downside with molar tooth which have been handled by root resection. In a study of 100 sufferers, a complete of 38 enamel failed during the 10-year interval of observation, and 47% of the failures had been a results of root fractures, with the vast majority being in mandibular molar tooth. Symptoms may be acute, with periodontal abscess formation related to ache, swelling, pus exudation, pocket formation and tooth mobility. A extra persistent response might generally occur without pain and involves the sudden appearance of a pocket with bleeding on probing, or exudation of pus. When the root perforation is located near the alveolar crest, it may be possible to increase a flap, restore the defect with an appropriate filling material, and subsequently reposition the flap apically to expose the repaired perforation website. In deeper perforations or in the roof of the furcation, quick inside repair of the perforation and an infection control is essential for higher prognosis. The indicators may range from a neighborhood deepening of a periodontal pocket to more acute periodontal abscess formation. In addition, root fractures have turn into an the apical development of a periodontal pocket can proceed until the apex is reached. In a single-rooted tooth, the prognosis is usually poor, unlike the first endodontic lesion. In molar enamel, not all roots might undergo the identical lack of supporting tissues extending to the apex, in which case the potential for root resection must be thought-about. The therapy of marginal periodontitis also can result in secondary endodontic involvement. For instance, a blood vessel within a lateral canal could additionally be severed by a curette throughout remedy. Additionally, pulp adjustments resulting from marginal periodontitis had been noticed when the main apical foramen was involved. There is a correlation between cultivable microorganisms from the root canals of human caries-free teeth with superior periodontitis and people from related periodontal pockets. Support for this concept has come from research by which cultured samples obtained from the pulp tissue and radicular dentine of periodontally concerned human teeth confirmed bacterial development in 87% of the instances. Healing of apical periodontitis could also be anticipated after profitable endodontic remedy. A fracture that has uncovered the pulp area, with resultant necrosis, may be labelled a true combined lesion and but not be amenable to profitable therapy. On the opposite hand, in a tooth with primary periodontal lesion, the pulp is significant and aware of sensitivity testing. However, major endodontic lesions with secondary periodontal involvement, main periodontal lesions with secondary endodontic involvement, or true combined lesions could additionally be clinically and radiographically very similar. The degree of therapeutic that has taken place after root canal remedy will decide the retrospective classification. The main elements to think about, on the time of diagnosis, are pulp vitality and type and extent of the periodontal defect. Primary endodontic lesion should only be managed by endodontic remedy, and the prognosis is sweet. Primary endodontic lesions with secondary periodontal involvement should first be managed with endodontic remedy. The therapy results should be evaluated in 2 to three months and only then should periodontal treatment be thought-about. This sequence of remedy permits adequate time for preliminary tissue therapeutic and better assessment of the periodontal condition. Primary periodontal lesions with secondary endodontic involvement and true combined endodonticperiodontal lesions require both endodontic and periodontal treatments. It has been demonstrated that intrapulpal infection tends to promote marginal epithelial downgrowth alongside a denuded dentine floor. In general, assuming the endodontic remedy is sufficient, the lesion of endodontic origin will heal. Thus, the prognosis of combined illnesses depends on the efficacy of periodontal remedy. These grooves often begin within the central fossa of maxillary central, or lateral, incisors, over the cingulum, and continue apically down the root for varying distances. Such a groove is seemingly the outcome of an try by the tooth germ to kind another root. This fissure-like channel may present a nidus for biofilm formation and infection, and an avenue for the progression of marginal periodontitis. From the time the tooth develops with this anomalous root defect, the potential for isolated marginal periodontitis exists. As lengthy as the epithelial attachment remains intact, the periodontium remains wholesome. In selected circumstances, radicular grooves may be treated satisfactorily and maintained. The clinician must search for the groove because it could have been altered by a previous restoration on the palatal floor. The use of an operating microscope throughout scientific examination is advantageous because of enhanced magnification and illumination. If the situation is only periodontal, it can be recognized visually by following the groove to the gingival sulcus and probing the depth of the pocket. This pocket is normally tubular and isolated, versus a extra generalized periodontal situation. Bone destruction that follows the groove longitudinally could also be apparent radiographically. The look of a teardrop-shaped space on the radiograph also needs to arouse suspicion. This situation should be differentiated from a longitudinal fracture, which may give an identical radiographic look. The essential problem is the need to remove the pathway of infection ensuing from the presence of the anatomical radicular anomaly. The prognosis is improved if the situation is diagnosed and treated early, however its administration stays challenging. Although the acute nature of the problem could also be alleviated initially, the rationale for the inflammation have to be eradicated by slicing out the groove and surgical management of the tissues. This can be mixed with placement of a biocompatible materials in an attempt to improve success. However, if the prognosis appears poor, early extraction is advisable to avoid compromising future implant treatment. Combined administration consists of endodontic therapy, atraumatic extraction, groove discount, Emdogain software and tooth reimplantation. Bicuspidization is the separation of a multirooted tooth by a vertical reduce via the furcation.