
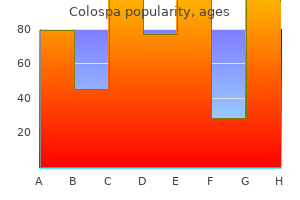
Colospa dosages: 135 mg
Colospa packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Colospa 135 mg discount free shipping
Because of the effect of gravity spasms while eating generic 135 mg colospa free shipping, blood move is slower when a person stands quietly muscle relaxant for tmj colospa 135 mg generic without a prescription. During train, blood obtained by the deep veins from the superficial veins is propelled by muscular contraction to the femoral and then the exterior iliac veins. The deep veins are more variable and anastomose much more regularly than the arteries they accompany. Lymphatic Drainage of Lower Limb the decrease limb has superficial and deep lymphatic vessels. The lymphatic vessels accompanying the good saphenous vein finish in the vertical group of superficial inguinal lymph nodes. Most lymph from these nodes passes on to the external iliac lymph nodes, positioned alongside the external iliac vein. Some lymph also passes to the deep inguinal lymph nodes, situated beneath the deep fascia on the medial facet of the femoral vein. Deep lymphatic vessels from the leg accompany deep veins and also enter the popliteal lymph nodes. Most lymph from these nodes ascends through deep lymphatic vessels to the deep inguinal lymph nodes. These nerves, except for some proximal unisegmental nerves arising from the T12 or L1 spinal nerves, are branches of the lumbar and sacral plexuses. The areas of skin supplied by the individual spinal nerves, together with these contributing to the plexuses, are known as dermatomes. The dermatomal or segmental sample of distribution of sensory nerve fibers persists despite the merging of spinal nerves in plexus formation during growth. The dermatome sample of the lower limb based on Foerster (1933) is preferred by many due to its correlation with medical findings. The dermatome sample of the decrease limb based on Keegan and Garrett (1948) is most popular by others for its aesthetic uniformity and apparent correlation with growth. Although depicted as distinct zones, adjacent dermatomes overlap significantly, besides along the axial line. Motor Innervation of Lower Limb Somatic motor (general somatic efferent) fibers touring in the same blended peripheral nerves that convey sensory fibers to the cutaneous nerves transmit impulses to the muscle tissue of the decrease limb. The unilateral embryological muscle mass receiving innervation from a single spinal twine segment or spinal nerve includes a myotome. Lower limb muscle tissue usually obtain motor fibers from several spinal twine segments or nerves. Myotomes are the segmental innervation of muscle groups and actions of lower limb. The stage of spinal cord harm or nerve impingement may be decided by the strength and ability to perform particular actions. Trauma to muscle tissue and/or vessels in the compartments from burns, sustained intense use of muscles, or blunt trauma may produce hemorrhage, edema, and irritation of the muscles. Because the septa and deep fascia of the leg forming the boundaries of the leg compartments are robust, the increased quantity consequent to any of those processes will increase intracompartmental strain. The strain might reach ranges excessive enough to compress structures considerably in the compartment(s) involved. The small vessels of muscles and nerves (vasa nervorum) are notably susceptible to compression. Structures distal to the compressed space may turn out to be ischemic and permanently injured. Increased pressure in a confined anatomical house adversely affects the circulation and threatens the perform and viability of tissue inside or distally, constituting compartment syndromes. Loss of distal leg pulses is an obvious sign of arterial compression, as is reducing of the temperature of tissues distal to the compression. A fasciotomy (incision of overlying fascia or a septum) may be performed to relieve the strain within the compartment(s) concerned. In a healthy vein, the valves allow blood to move toward the heart (B) while preserving blood from flowing away from the center (C). Valves in varicose veins (D) are incompetent because of dilation or rotation and now not perform correctly. A giant thrombus that breaks free from a lower limb vein may travel to a lung, forming a pulmonary thromboembolism (obstruction of a pulmonary artery). Because there are so many different leg veins, removal of the great saphenous vein not often produces a major drawback within the lower limb or critically affects circulation, supplied the deep veins are intact. In truth, removing of this vein could facilitate the superficial to deep drainage pattern to reap the benefits of the musculovenous pump. This procedure, called a saphenous cutdown, is used to insert a cannula for 1602 prolonged administration of blood, plasma expanders, electrolytes, or drugs. The saphenous nerve accompanies the nice saphenous vein anterior to the medial malleolus. Should this nerve be minimize throughout a saphenous cutdown or caught by a ligature throughout closure of a surgical wound, the affected person may complain of ache or numbness along the medial border of the foot. Abrasions and minor sepsis, attributable to pathogenic microorganisms or their toxins within the blood or other tissues, could produce average enlargement of the superficial inguinal lymph nodes (lymphadenopathy) in in any other case wholesome people. When inguinal lymph nodes are enlarged, their whole field of drainage-the trunk inferior to the umbilicus, including the perineum, in addition to the complete decrease limb-should be examined to determine the trigger of their enlargement. In female sufferers, the relatively remote risk of metastasis of cancer from the uterus also wants to be thought of because some lymphatic drainage from the uterine fundus may flow alongside lymphatics accompanying the round ligament of the uterus by way of the inguinal canal to reach the superficial inguinal lymph nodes. Regional Nerve Blocks of Lower Limbs Interruption of the conduction of impulses in peripheral nerves (nerve block) may be achieved by making perineural injections of anesthetics near the nerves whose conductivity is to be blocked. Paresthesia (tingling, burning, tickling) radiates to the knee and over the medial side of the leg if the saphenous nerve (terminal branch of femoral) is affected. Pain sensation is examined by using a pointy object and asking the affected person if ache is felt. Veins: the veins of the lower limb embrace both superficial (in the subcutaneous tissue) and deep (internal to the deep fascia) veins. Lymphatic vessels: Most lymph from the lower limb drains by way of 1604 lymphatics that follow the superficial veins. Lymph drainage from the decrease limb then passes deep to the exterior and common iliac nodes of the trunk. Cutaneous nerves: the cutaneous innervation of the decrease limb displays each the original segmental innervation of the pores and skin via separate spinal nerves in its dermatomal sample and the outcome of plexus formation in the distribution of multisegmental peripheral nerves. Typically, the actions of lower limb muscular tissues are described as if the muscle had been appearing in isolation, which not often occurs. It is essential to be acquainted with decrease limb actions and concentric and eccentric contractions of muscle tissue, as described within the Introduction, and to have a fundamental understanding of the processes of standing and strolling. The mechanical arrangement of the joints and muscular tissues are such that a minimum of muscular exercise is required to hold from falling. In the 1605 stand-easy place, the hip and knee joints are prolonged and are of their most stable positions (maximal contact of articular surfaces for weight switch, with supporting ligaments taut). The relationship of the road of gravity to the transverse rotational axes of the pelvis and lower limb in the relaxed standing (stand-easy) position is demonstrated.
Ficus carica (Fig). Colospa.
- Dosing considerations for Fig.
- How does Fig work?
- Constipation, diabetes, and other conditions.
- Are there safety concerns?
- Are there any interactions with medications?
- What is Fig?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96454
Buy discount colospa 135 mg on line
The medial floor of the lateral malleolus articulates with the lateral surface of the talus muscle relaxant modiek proven colospa 135 mg. The malleoli grip the talus tightly as it rocks within the mortise during movements of the joint muscle relaxer ketorolac colospa 135 mg generic line. In A, the foot has been inverted (by placing a wedge under the foot) to demonstrate the articular surfaces and make the lateral ligaments taut. The ankle joint is comparatively unstable throughout plantarflexion as a result of the trochlea is narrower posteriorly and, subsequently, lies relatively loosely within the mortise. It is during plantarflexion that most accidents of the ankle occur (usually as a end result of sudden, unexpected-and due to this fact inadequately resisted- inversion of the foot). Its fibrous layer is hooked up superiorly to the borders of the articular surfaces of the tibia and the malleoli and inferiorly to the talus. The synovial cavity often extends superiorly between the tibia and the fibula as far as the interosseous tibiofibular ligament. The relationships of the flexor tendons to the medial malleolus and sustentaculum tali are shown as they descend the posterolateral aspect of the ankle region and enter the foot. Except for the part tethering the flexor hallucis longus tendon, the flexor retinaculum has been removed. The 4 elements of the medial (deltoid) ligament of the ankle are demonstrated in this dissection. Anterior talofibular ligament, a flat, weak band that extends anteromedially from the lateral malleolus to the neck of the talus. Posterior talofibular ligament, a thick, pretty sturdy band that runs horizontally medially and barely posteriorly from the malleolar fossa to the lateral tubercle of the talus. Calcaneofibular ligament, a round twine that passes postero-inferiorly from the tip of the lateral malleolus to the lateral floor of the calcaneus. The medial ligament followers out from the malleolus, attaching distally to the talus, calcaneus, and navicular through four adjoining and steady parts: the tibionavicular half, the tibiocalcaneal part, and the anterior and posterior tibiotalar parts. The medial ligament stabilizes the ankle joint during eversion and prevents subluxation (partial dislocation) of the joint. Because the narrow finish of the trochlea of the talus lies loosely between the malleoli when the foot is plantarflexed, some "wobble" (small amounts of abduction, adduction, inversion, and eversion) is possible on this unstable place. Dorsiflexion of the ankle is produced by the muscles within the anterior compartment of the leg (see Table 7. Dorsiflexion is usually limited by the passive resistance of the triceps surae to stretching and by tension in the medial and lateral ligaments. Plantarflexion of the ankle is produced by the muscular tissues within the posterior compartment of the leg (see Table 7. In toe dancing by ballet dancers, for example, the dorsum of the foot is in line with the anterior floor of the leg. The important intertarsal joints are the subtalar (talocalcaneal) joint and the transverse tarsal joint (calcaneocuboid and talonavicular joints). Inversion is augmented by flexion of the toes (especially the great and 2nd toes), and eversion by their extension (especially of the lateral toes). All bones of the foot proximal to the metatarsophalangeal joints are united by dorsal and plantar ligaments. The bones of the metatarsophalangeal and interphalangeal joints are united by lateral and medial collateral ligaments. The subtalar joint happens where the talus rests on and articulates with the calcaneus. The interosseous talocalcaneal ligament lies inside the tarsal sinus, which separates the subtalar and talocalcaneonavicular joints, and is particularly robust. Orthopedic surgeons use the time period subtalar joint for the compound practical joint consisting of the 1830 anatomical subtalar joint plus the talocalcaneal part of the talocalcaneonavicular joint. The two separate components of the clinical subtalar joint straddle the talocalcaneal interosseous ligament. Structurally, the anatomical definition is logical as a outcome of the anatomical subtalar joint is a discrete joint, having its own joint capsule and articular cavity. Transection across the transverse tarsal joint is a standard methodology for surgical amputation of the foot. Sequential stages of a deep dissection of the solely real of the best foot exhibiting the attachments of the ligaments and the tendons of the lengthy evertor and invertor muscular tissues. The lengthy plantar ligament is essential in sustaining the longitudinal arch of the foot. It extends from the anterior side of the inferior floor of the calcaneus to the inferior surface of the cuboid. Because the foot consists of numerous bones related by ligaments, it has appreciable flexibility that enables it to deform with every floor contact, thereby absorbing much of the shock. Furthermore, the tarsal and metatarsal bones are arranged in longitudinal and transverse arches passively supported and actively restrained by versatile tendons that add to the weight-bearing capabilities and resiliency of the foot. Thus, much smaller forces of longer duration are transmitted by way of the skeletal system. The arches distribute weight over the pedal platform (foot), appearing not only as shock absorbers but additionally as springboards for propelling it during walking, 1833 working, and leaping. Between these weight-bearing factors are the comparatively elastic arches of the foot, which turn out to be slightly flattened by body weight during standing. Body weight is divided approximately equally between the hindfoot (calcaneus) 1834 and the forefoot (heads of the metatarsals). The forefoot has 5 factors of contact with the ground: a big medial one that features the two sesamoid bones associated with the top of the first metatarsal and the heads of the lateral four metatarsals. The 1st metatarsal supports the main share of the load, with the lateral forefoot providing steadiness. Functionally, each elements act as a unit with the transverse arch of the foot, spreading the weight in all instructions. The medial longitudinal arch consists of the calcaneus, talus, navicular, three cuneiforms, and three metatarsals. The tibialis anterior and posterior, via their tendinous attachments, assist support the medial longitudinal arch. The medial longitudinal arch is larger than the lateral longitudinal arch, which may contact the bottom when standing erect. The transverse arch is demonstrated on the stage of the cuneiforms, receiving stirruplike assist from a serious invertor (tibialis posterior) and evertor (fibularis longus). The elements of the medial (dark gray) and lateral (light gray) longitudinal arches are indicated. The medial arch is primarily weight bearing, whereas the lateral arch supplies balance. The active (red lines) and passive (gray) supports of the longitudinal arches are represented.
Colospa 135 mg buy on-line
The nerve traverses a lot of the length of the posterior compartment of the thigh deep to the fascia lata; solely its terminal branches enter the subcutaneous tissue as cutaneous nerves spasms while sleeping 135 mg colospa purchase free shipping. The popliteal artery passes inferolaterally by way of the fossa and ends at the inferior border of the popliteus by dividing into the anterior and posterior tibial arteries infantile spasms 4 year old colospa 135 mg buy line. The deepest (most anterior) construction in the fossa, the popliteal artery, runs in close proximity to the joint capsule of the knee because it spans the intercondylar fossa. The many arteries making up the peri-articular anastomosis around the knee provide an necessary collateral circulation for bypassing the popliteal artery when the knee joint has been maintained too lengthy in a totally flexed position or when the vessels are narrowed or occluded. Five genicular branches of the popliteal artery supply the capsule and 1702 ligaments of the knee joint. They participate in the formation of the peri-articular genicular anastomosis, a community of vessels surrounding the knee that provides collateral circulation able to sustaining blood provide to the leg throughout full knee flexion, which can kink the popliteal artery. Other contributors to this necessary genicular anastomosis are the descending genicular artery, a branch of the femoral artery, superomedially. Muscular branches of the popliteal artery provide the hamstring, gastrocnemius, soleus, and plantaris muscle tissue. The superior muscular branches of the popliteal artery have clinically necessary anastomoses with the terminal a part of the profunda femoris and gluteal arteries. Throughout its course, the vein lies close to the popliteal artery, lying superficial to it in the identical fibrous sheath. The popliteal vein is initially posteromedial to the artery and lateral to the tibial nerve. More superiorly, the popliteal vein lies posterior to the artery, between this vessel and the overlying tibial nerve. Superiorly, the popliteal vein, which has a quantity of valves, becomes the femoral vein as it traverses the adductor hiatus. The small saphenous vein passes from the posterior side of the lateral malleolus to the popliteal fossa, where it pierces the deep popliteal fascia and enters the popliteal vein. The superficial popliteal lymph nodes are normally small and lie in the subcutaneous tissue. The deep popliteal lymph nodes encompass the vessels and obtain lymph from the joint capsule of the knee and the lymphatic vessels that accompany the deep veins of the leg. The lymphatic vessels from the popliteal lymph nodes comply with the femoral vessels to the deep inguinal lymph nodes. The anterior (dorsiflexor or extensor) compartment incorporates 4 muscle tissue (the fibularis tertius lies inferior to the extent of this section). The posterior (plantarflexor or flexor) compartment, containing seven muscular tissues, is subdivided by an intracompartmental transverse intermuscular septum into a superficial group of three (two of that are generally tendinous/aponeurotic at this level) and a deep group of 4. The popliteus (part of the deep group) lies superior to the extent of this part. The anterior compartment of the leg, or dorsiflexor (extensor) compartment, is situated anterior to the interosseous membrane, between the lateral surface of the shaft of the tibia and the medial surface of the shaft of the fibula. The anterior compartment is bounded anteriorly by the deep fascia of the leg and skin. The deep fascia overlying the anterior compartment is dense superiorly, providing a part of the proximal attachment of the muscle immediately deep to it. With unyielding constructions on three sides (the two bones and the interosseous membrane) and a dense fascia on the remaining aspect, the comparatively small anterior compartment is very confined and subsequently most susceptible to compartment syndromes (see the medical box "Containment and Spread of Compartmental Infections in the Leg"). These dissections demonstrate the continuation of the anterior and lateral leg muscular tissues into the foot. The thinner parts of the deep fascia of the leg have been removed, leaving the thicker portions that make up the extensor and fibular retinacula, which retain the tendons as they cross the ankle. At the ankle, the vessels and the deep fibular nerve lie halfway between the malleoli and between the tendons of the long dorsiflexors of the toes. Synovial sheaths surround the tendons as they cross beneath the retinacula of the ankle. The superior extensor retinaculum is a strong, broad band of deep fascia, passing from the fibula to the tibia, proximal to the malleoli. The inferior extensor retinaculum, a Y-shaped band of deep fascia, attaches laterally to the anterosuperior floor of the calcaneus. It varieties a strong loop across the tendons of the fibularis tertius and the extensor digitorum longus muscular tissues. These muscle tissue pass and insert anterior to the transversely oriented axis of the ankle (talocrural) joint and, subsequently, are dorsiflexors of the ankle joint, elevating the forefoot and miserable the heel. The long extensors also pass alongside and attach to the dorsal side of the digits and are thus extensors (elevators) of the toes. The latter is important to a easy gait and is necessary to deceleration (braking) relative to working and strolling downhill. During standing, the dorsiflexors reflexively pull the leg (and thus the center of gravity) anteriorly on the mounted foot when the body starts to lean (the heart of gravity begins to shift too far) posteriorly. In so doing, its tendon is positioned farthest from the axis of the ankle joint, giving it essentially the most mechanical advantage and making it the strongest dorsiflexor. This dissection reveals the muscles of the anterolateral leg and dorsum of the foot. The widespread fibular nerve, coursing subcutaneously throughout the lateral aspect of the head and neck of the fibula, is essentially the most generally injured peripheral nerve. In this deeper dissection of the anterior compartment, the muscles and inferior extensor retinaculum are retracted to show the arteries and nerves. The central band inserts into the bottom of the middle phalanx, and the lateral slips converge to insert into the base of the distal phalanx. It might play a special proprioceptive position in sensing sudden inversion after which contracting reflexively to defend the anterior tibiofibular ligament, essentially the most generally sprained ligament of the physique. It is probably certainly one of the two terminal branches of the widespread fibular nerve, arising between the fibularis longus muscle and the neck of the fibula. The deep fibular nerve then exits the compartment, persevering with across the ankle joint to supply intrinsic muscular tissues (extensors digitorum and hallucis brevis), and a small space of the pores and skin of the foot. The smaller terminal branch of the popliteal artery, the anterior tibial artery, begins on the inferior border of the popliteus muscle. At the ankle joint, midway between the malleoli, the anterior tibial artery modifications names, changing into the dorsalis pedis artery (dorsal artery of the foot). The popliteal artery begins on the site of the adductor hiatus (where it may be compressed) after which lies successively on the distal finish of the femur, joint capsule of the knee joint, and popliteus muscle (not visible) before dividing into the anterior and posterior tibial arteries on the inferior angle of the popliteus fossa. Sniderman, Associate Professor of Medical Imaging, University of Toronto, Toronto, Ontario, Canada. These muscles have their fleshy bellies within the lateral compartment but are tendinous as they exit the compartment throughout the frequent synovial sheath deep to the superior fibular retinaculum. Developmentally, the fibularis muscle tissue are postaxial muscle tissue, receiving innervation from the posterior divisions of the spinal nerves, which contribute to the sciatic nerve.
Discount 135 mg colospa fast delivery
The ganglion is flattened and crescent formed (hence its unofficial name muscle relaxant safe in pregnancy 135 mg colospa generic with visa, semilunar ganglion) and is housed inside a dural recess (trigeminal cave) lateral to the cavernous sinus muscle relaxant valium colospa 135 mg cheap visa. Cutaneous (sensory) zones are innervated by the three divisions of the trigeminal nerve. Each cranial nerve division provides skin and mucous membranes and sends a branch to the dura of the anterior and middle cranial fossae. This open-book view exhibits the innervation of the lateral wall and septum of the nasal cavity and palate. It serves buildings derived from the paraxial mesoderm of the embryonic frontonasal process. Each abducent nerve then pierces the dura mater to run the longest intradural course within the cranial cavity of all of the cranial nerves-that is, its point of entry into the dura mater overlaying the clivus is the most distant from its exit from the cranium via the superior orbital fissure. It also carries proprioceptive fibers from the muscle tissue it innervates, though the muscular tissues of facial features embody relatively few muscle spindles (mechanoreceptors for muscle stretch), so proprioceptive sensory fibers are fewer than in different motor nerves (Haines, 2013). The central processes of those involved with taste finish in the nuclei of the solitary tract within the medulla. The bigger major root (facial nerve proper) innervates the muscles of facial expression, and the smaller intermediate nerve (L. After traversing the inner acoustic meatus, the nerve proceeds a short distance anteriorly inside the temporal bone and then turns abruptly posteriorly to course alongside the medial wall of the tympanic cavity. Somatic (Branchial) Motor 2397 As the nerve of the embryonic 2nd pharyngeal arch, the facial nerve provides striated muscles derived from its mesoderm, mainly the muscles of facial expression and auricular muscular tissues. It also provides the posterior bellies of the digastric, stylohyoid, and stapedius muscular tissues. Parasympathetic fibers synapse in these ganglia, whereas sympathetic and sensory fibers pass through them. Somatic (General) Sensory Some fibers from the geniculate ganglion accompany the auricular department of the vagus nerve to supply small areas of pores and skin on both elements of the auricle, within the region of the concha and on the opening of the exterior acoustic meatus. Special Sensory (Taste) Peripheral fibers of sensory neurons of the geniculate ganglion are carried by the chorda tympani. The inside surface of the cranial base reveals the placement of the bony labyrinth of the interior ear inside the temporal bone. The vestibular nerve is composed of the central processes of bipolar neurons in the vestibular ganglion. The peripheral processes of the neurons 2400 prolong to the maculae of the utricle and saccule (sensitive to linear acceleration and the pull of gravity relative to the place of the head) and to the cristae of the ampullae of the semicircular ducts (sensitive to rotational acceleration). The cochlear nerve is composed of the central processes of bipolar neurons in the spiral ganglion; the peripheral processes of the neurons extend to the spiral organ for the sense of listening to. Motor-somatic (branchial) motor and visceral (parasympathetic) motor for derivatives of the 3rd pharyngeal arch. It additionally carries sensory fibers from the carotid body and carotid sinus, conveying information about blood strain and gasoline ranges in addition to somatic (general) sensation from the inner ear, pharynx, and fauces and taste from the 2402 posterior tongue. They are instantly posterior to the internal carotid artery as they emerge from it. Somatic (Branchial) Motor Motor fibers cross to one muscle, the stylopharyngeus, derived from the 3rd pharyngeal arch. The plexus supplies sensory innervation for the mucosa of the tympanic cavity, antrum of mastoid air cells, and the posterolateral portion of the pharyngotympanic tube. The pharyngeal, tonsillar, and lingual nerves to the mucosa of the oropharynx and isthmus of the fauces (L. In addition to basic sensation (touch, ache, temperature), tactile (actual or threatened) stimuli determined to be uncommon or disagreeable here might evoke the gag reflex and even vomiting. The vagus offers the afferent (sensory) limb of the cough reflex stimulated by overseas irritants, stopping aspiration and an infection. Taste and somatic (general) sensation from the basis of the tongue and style buds on the epiglottis. Somatic (branchial) motor to the taste bud, pharynx, intrinsic laryngeal muscles (phonation), and a nominal extrinsic tongue muscle, the palatoglossus, which is actually a palatine muscle based mostly on its derivation and innervation. Nuclei: Sensory-sensory nucleus of the trigeminal nerve (somatic sensory) and nuclei of the solitary tract (taste and visceral sensory). The recurrent laryngeal nerves ascend to the larynx, the left from a extra inferior (thoracic) level. In the stomach, the anterior and posterior vagal trunks reveal additional asymmetry as they supply the terminal esophagus, abdomen, and intestinal tract as far distally as the left colic flexure. Enlarged view of decrease esophageal plexus transitioning to anterior and posterior vagal trunks. Anterior and posterior vagal trunks kind as continuations of the esophageal plexus surrounding the esophagus, which can be joined by branches of the sympathetic trunks. The trunks cross with the esophagus by way of the diaphragm into the abdomen, the place the vagal trunks break up into branches that innervate the stomach and intestinal tract as far as the left colic flexure. They enter the superior mediastinum posterior to the sternoclavicular joints and brachiocephalic veins. Branches of the cervical plexus conveying sensory fibers from spinal nerves C2�C4 be part of the spinal accent nerve within the posterior cervical area, providing these muscular tissues with ache and proprioceptive fibers. Some fibers continue past the origin of the superior root to reach the thyrohyoid muscle. Terminal lingual branches supply the styloglossus, hyoglossus, genioglossus, and intrinsic muscles of the tongue. Injury to the cranial nerves is a frequent complication of a fracture in the base of the skull. Further, cranial nerve accidents also generally happen with traumatic harm to the brain, which could find yourself in delayed analysis and intervention (Russo et al. In such circumstances, the onset of symptoms usually occurs gradually, and the effects rely upon the extent of the stress exerted. Consequently, elderly people typically have decreased acuity of the sensation of scent, ensuing from progressive reduction in the number of olfactory 2416 receptor neurons within the olfactory epithelium. The chief grievance of most people with anosmia is the loss or alteration of taste; nonetheless, medical studies reveal that in all but a few individuals, the dysfunction is in the olfactory system (Simpson, 2013). Transitory olfactory impairment occurs as a outcome of viral or allergic rhinitis- irritation of the nasal mucous membrane. To take a look at the sense of smell, the person is blindfolded and requested to determine widespread odors, such as freshly ground espresso placed near the exterior nares (nostrils). If the loss of smell is unilateral, the particular person may not be aware of it with out medical testing. Injury to the nasal mucosa, olfactory nerve fibers, olfactory bulbs, or olfactory tracts may also impair scent.
Discount colospa 135 mg visa
During 2102 chewing spasms side of head 135 mg colospa, the tongue (centrally) muscle relaxant patch colospa 135 mg purchase on-line, buccinator (laterally), and orbicularis oris (anteriorly) work together to retain the bolus of meals between the occlusive surfaces of the molar enamel. The oral cavity proper is the house between the upper and the lower dental arches or arcades (maxillary and mandibular alveolar arches and the enamel they bear). Posteriorly, the oral cavity communicates with the oropharynx (oral a part of the pharynx). When the mouth is closed and at rest, the oral cavity is totally occupied by the tongue. The lips function as the valves of the oral fissure, containing the sphincter (orbicularis oris) that controls entry and exit from the mouth and upper alimentary and respiratory tracts. The lips are used for grasping meals, sucking liquids, maintaining food out of the oral vestibule, forming speech, and osculation (kissing). Lymph from the higher lip and lateral components of the lower lip drains to the submandibular nodes. The labial frenula (frena) are free-edged folds of mucous membrane in the midline, extending from the vestibular gingiva to the mucosa of the higher and lower lips. Other smaller frenula typically appear laterally within the premolar vestibular regions. As the alveolar mucosa approaches the necks of the enamel, it modifications in texture and shade to become the gingiva proper. The pulse of those arteries may be palpated by grasping the higher or lower lip lightly between the primary two digits. The higher lip is supplied by superior 2105 labial branches of the facial and infra-orbital arteries. The decrease lip is equipped by inferior labial branches of the facial and psychological arteries. The prominence of the cheek happens on the junction of the zygomatic and buccal areas. Lay individuals think about the zygomatic and parotid areas additionally to be a half of the cheek. These buccal fat-pads are proportionately a lot bigger in infants, presumably to reinforce the cheeks and maintain them from collapsing during sucking. The cheeks are supplied by buccal branches of the maxillary artery and innervated by buccal branches of the mandibular nerve. The gingiva correct adjoining to the tongue is the superior and inferior lingual gingivae, and that adjoining to the lips and cheeks is the maxillary and mandibular labial or buccal gingiva, respectively. The alveolar mucosa (unattached gingiva) is generally shiny purple and nonkeratinizing. Teeth the chief features of teeth are as follows: Incise (cut), reduce, and blend meals materials with saliva throughout mastication (chewing). Help sustain themselves in the tooth sockets by helping the development and safety of the tissues that support them. The tooth are set in the tooth sockets and are utilized in mastication and in aiding in articulation. A tooth is recognized and described as deciduous (primary) or permanent (secondary), the sort of tooth, and its proximity to the midline or front of the mouth. The alveolar strategy of the maxilla and alveolar a part of the mandible are carved to reveal the roots of the teeth and tooth buds. Pharoah, Associate Professor of Dental Radiology, Faculty of Dentistry, University of Toronto, Toronto, Ontario, Canada. As used in medical (dental) follow, the mesial floor of a tooth is directed towards the median airplane of the facial part of the skull. The root is fixed in the tooth socket by the periodontium (connective tissue surrounding the roots). The root canal (pulp canal) transmits the nerves and vessels to and from the pulp cavity by way of the apical foramen. In dwelling people, the pulp cavity is a hollow area throughout the crown and neck of the tooth containing connective tissue, blood vessels, and nerves. The cavity narrows right down to the basis canal in a single-rooted tooth or to one canal per root of a multirooted tooth. Bite-wing radiograph of maxillary premolar and molar tooth demonstrating features proven and described partly A. The bone of the socket has a thin cortex separated from the adjoining labial and lingual cortices by a variable amount of trabeculated bone. Therefore, the labial surface generally is broken to extract incisors and the lingual surface is broken to extract molars. The roots of the teeth are connected to the bone of the alveolus by a springy suspension forming a special sort of fibrous joint called a dento-alveolar syndesmosis or gomphosis. The periodontium (periodontal membrane) consists of collagenous fibers that extend between the cement of the root and the periosteum of the alveolus. It is abundantly supplied with tactile, pressoreceptive nerve endings, lymph capillaries, and glomerular blood vessels that act as hydraulic cushioning to curb axial masticatory stress. Pressoreceptive nerve endings are capable of receiving modifications in pressure as stimuli. The alveolar veins have the same names and distribution 2113 accompany the arteries. It separates the oral cavity from the nasal cavities and the nasopharynx, the part of the pharynx superior to the taste bud. The superior (nasal) floor of the palate is roofed with respiratory mucosa, and the inferior (oral) surface is covered with oral mucosa, densely packed with glands. The palate consists of two regions: the exhausting palate anteriorly and the taste bud posteriorly. The soft palate acts 2114 as a valve, elevating to seal the pharyngeal isthmus connecting the nasal cavity and nasopharynx with the oral cavity and oropharynx. The incisive fossa is a despair in the midline of the bony palate posterior to the central incisor teeth into which the incisive canals open. The palatine aponeurosis is fashioned by the merging of the flattened tendons of the proper and left tensor veli palatini muscles. Before they become flattened, each tendon makes use of the pterygoid hamulus as a trochlea or pulley, redirecting its line of pull approximately 2116 90�. The greater palatine vessels and nerve emerge from this foramen and run anteriorly on the palate. The lesser palatine foramina posterior to the larger palatine foramen pierce the pyramidal strategy of the palatine bone. The taste bud has no bony skeleton; nevertheless, its anterior aponeurotic half is strengthened by the palatine aponeurosis, which attaches to the posterior edge of the onerous palate. The aponeurosis is thick anteriorly and skinny posteriorly, the place it blends with a posterior muscular part of the taste bud. Postero-inferiorly, the taste bud has a curved free margin from which hangs a conical course of, the uvula.
Buy 135 mg colospa fast delivery
Another method muscle relaxant pills over the counter colospa 135 mg buy overnight delivery, 1238 lithotripsy infantile spasms 6 months old cheap 135 mg colospa mastercard, focuses a shockwave by way of the physique that breaks the calculus into small fragments that pass with the urine. The central renal sinus is occupied by the renal calices and renal pelvis, segmental arteries, and renal veins which might be embedded in perinephric fat. Ureters: the abdominal parts of the ureters descend on the anterior surface of the psoas muscular tissues from the apex of the renal pelvis to the pelvic brim. Suprarenal glands: the suprarenal glands are located superomedially to the kidneys but are attached primarily to the diaphragmatic crura by the encircling renal fascia. They lie anterior to the renal veins, with the right renal artery being longer than the left, and the left renal vein being longer than the best. Suprarenal arteries arise from three sources: superior suprarenal arteries from the inferior phrenic arteries, center suprarenal arteries from the stomach aorta, and inferior suprarenal arteries from the renal arteries. Lymphatics from the suprarenal glands, kidneys, and higher ureters follow the venous drainage to the best or left lumbar (caval or aortic) lymph nodes. Visceral afferent fibers (accompanying the sympathetic fibers) conduct pain sensation from the ureters to spinal twine segments T11�L2, with sensation referred to the corresponding dermatomes overlying the loin and groin. These fibers traverse both the paravertebral (sympathetic trunks) and prevertebral (celiac) ganglia without synapsing. The periarterial extensions of those plexuses deliver postsynaptic sympathetic fibers and 1240 the continuations of parasympathetic fibers to the stomach viscera, the place intrinsic parasympathetic ganglia occur. Origin and distribution of presynaptic and postsynaptic sympathetic and parasympathetic fibers, and the ganglia 1241 involved in supplying belly viscera are proven. The fibers supplying the intrinsic plexuses of belly viscera are demonstrated. The nerve plexuses are mixed, shared with the parasympathetic nervous system and visceral afferent fibers. The abdominopelvic splanchnic nerves convey presynaptic sympathetic fibers to the abdominopelvic cavity. The fibers cross successively through the anterior roots, anterior rami, and white communicating branches of thoracic and upper lumbar spinal nerves to attain the sympathetic trunks. They pass via the paravertebral ganglia of the trunks without synapsing to enter the abdominopelvic splanchnic nerves, which convey them to the prevertebral ganglia of the abdominal cavity. The abdominopelvic splanchnic nerves embrace the: Lower thoracic splanchnic nerves (greater, lesser, and least): from the thoracic a part of the sympathetic trunks. The decrease thoracic splanchnic nerves are the main supply of presynaptic sympathetic fibers serving abdominal viscera. The higher splanchnic nerve (from the sympathetic trunk at T5 through T9 or T10 vertebral levels), lesser splanchnic nerve (from T10 and T11 levels), and least splanchnic nerve (from the T12 level) are the particular abdominopelvic splanchnic nerves that come up from the thoracic a half of the sympathetic trunks. They pierce the corresponding crus of the diaphragm to convey presynaptic sympathetic fibers to the celiac, superior mesenteric, and aorticorenal (prevertebral) sympathetic ganglia, respectively. The lumbar splanchnic nerves come up from the stomach part of the 1243 sympathetic trunks. Medially, the lumbar sympathetic trunks give off three to four lumbar splanchnic nerves, which pass to the intermesenteric, inferior mesenteric, and superior hypogastric plexuses, conveying presynaptic sympathetic fibers to the related prevertebral ganglia of those plexuses. The cell bodies of postsynaptic sympathetic neurons constitute the major prevertebral ganglia that cluster across the roots of the major branches of the belly aorta: the celiac, aorticorenal, superior mesenteric, and inferior mesenteric ganglia. Minor, unnamed prevertebral ganglia occur throughout the intermesenteric and superior hypogastric plexuses. Postsynaptic sympathetic nerve fibers move from the prevertebral ganglia to the belly viscera by means of the peri-arterial plexuses associated with the branches of the belly aorta. Sympathetic innervation within the stomach, as elsewhere, is primarily concerned in producing vasoconstriction. With regard to the gastrointestinal tract, it acts to inhibit (slow down or stop) peristalsis. Abdominal (para-aortic) autonomic plexuses and their extensions, the periarterial plexuses. Intrinsic (enteric) parasympathetic ganglia, components of intrinsic enteric plexuses of the enteric nervous system. The nerve plexuses are combined, shared with the sympathetic nervous system and visceral afferent fibers. The vagus nerves convey presynaptic parasympathetic and visceral afferent fibers (mainly for unconscious sensations related to reflexes) to the abdominal aortic plexuses and the peri-arterial plexuses, which extend alongside the branches of the aorta. The fibers conveyed by the pelvic splanchnic nerves provide the descending and sigmoid components of the colon, rectum, and pelvic organs. Thus, in terms of the gastrointestinal tract, the vagus nerves present parasympathetic innervation of the sleek muscle and glands of the gut so far as the left colic flexure; the pelvic splanchnic nerves present the rest. Parasympathetic innervation in the stomach is primarily involved in promotion of peristalsis (restoring it following inhibition by a sympathetic response) and secretion. The celiac, superior mesenteric, and inferior mesenteric plexuses are interconnected. The prevertebral sympathetic ganglia are scattered among the celiac and mesenteric plexuses. The parasympathetic root of the celiac plexus is a department of the posterior vagal trunk, which accommodates fibers from the best and left vagus nerves. The median root is a branch of the celiac plexus, and the lateral roots come up from the lesser and least splanchnic nerves, typically with a contribution from the primary lumbar ganglion of the sympathetic trunk. The inferior mesenteric plexus surrounds the inferior mesenteric artery and provides offshoots to its branches. It receives a medial root from the intermesenteric plexus and lateral roots from the lumbar ganglia of the sympathetic trunks. An inferior mesenteric ganglion can also seem simply superior to the root of the inferior mesenteric artery. The intermesenteric plexus is part of the aortic plexus of nerves between the superior and the inferior mesenteric arteries. The superior hypogastric plexus is steady with the intermesenteric plexus and the inferior mesenteric plexus and lies anterior to the inferior a part of the stomach aorta and extends inferiorly across its bifurcation (Table 5. Right and left hypogastric nerves be part of the superior hypogastric plexus to the inferior hypogastric plexus. The superior hypogastric plexus provides ureteric and testicular plexuses and a plexus on each common iliac artery. The inferior hypogastric plexuses are blended sympathetic and parasympathetic plexuses fashioned on each side because the hypogastric nerves from the superior hypogastric plexus merge with the pelvic splanchnic nerves. The right and left plexuses are located on the perimeters of the rectum, cervix of the uterus, and urinary bladder. The plexuses receive small branches from the superior sacral sympathetic ganglia and the sacral parasympathetic outflow from S2 by way of S4 sacral spinal nerves (pelvic [parasympathetic] splanchnic nerves). Extensions of the inferior hypogastric plexus ship autonomic fibers alongside the blood vessels, which form visceral plexuses on the partitions of the pelvic viscera. Vasomotion (control of blood flow) at this degree influences water and electrolyte movement. Corresponding plexuses with smaller, sparser ganglia lengthen to the pancreas, gallbladder, and cystic and major biliary ducts. The motor neurons of those plexuses are intrinsic or enteric ganglia that serve nominally as postsynaptic neurons for the parasympathetic system.
Syndromes
- Brittle nails
- Have other diseases that affect the blood vessels of the neck and leg
- If you are or could be pregnant
- Rib fractures, lung or blood vessel injury
- Pain or numbness in the feet or hands
- Lack of sensation; you may not feel it if someone touches you there
- Increased appetite
Buy colospa 135 mg amex
The knee joint is important for on a daily basis activities corresponding to standing spasms just below rib cage colospa 135 mg discount otc, strolling muscle relaxant metabolism colospa 135 mg discount with visa, and climbing stairs. It can be a major joint for sports activities that involve operating, jumping, kicking, and altering directions. To carry out these activities, the knee joint have to be cellular; nevertheless, this mobility makes it vulnerable to injuries. Hyperextension and severe pressure directed anteriorly towards the femur with the knee semiflexed. Peripheral meniscal tears can typically be repaired, or they may heal on their very own due to the generous blood provide to this area. The arthroscope and one (or more) further cannula(e) are inserted by way of tiny incisions, generally identified as portals. This approach allows removing of torn menisci, unfastened our bodies in the joint (such as bone chips), and d�bridement (the excision of devitalized articular cartilaginous material) in advanced circumstances of arthritis. Although basic anesthesia is often preferable, knee arthroscopy could be carried out using local or regional anesthesia. During arthroscopy, the articular cavity of the knee should be handled basically as two separate (medial and lateral) femorotibial articulations, owing to the imposition of the synovial fold across the cruciate ligaments. When the knee joint is infected and infected, the quantity of synovial fluid could increase. Joint effusions, the escape of fluid from blood or lymphatic vessels, leads to elevated amounts of fluid within the joint cavity. Because the suprapatellar bursa communicates freely with the synovial cavity of the knee joint, fullness of the thigh within the area of the suprapatellar bursa may indicate increased synovial fluid. Direct aspiration of the knee joint is normally carried out with the patient sitting on a table with the knee flexed. The joint is approached laterally, utilizing three bony points as landmarks for needle insertion: the anterolateral tibial (Gerdy) tubercle, the lateral epicondyle of the femur, and the apex of the patella. In addition to being the route for aspiration of serous and sanguineous (bloody) fluid, this triangular area also lends itself to drug injection for treating pathology of the knee joint. Bursitis in Knee Region Prepatellar bursitis is brought on by extreme and repeated friction between the pores and skin and the patella, for instance, jobs related to kneeling. If the irritation is continual, the bursa becomes distended with fluid and varieties a swelling anterior to the knee. Subcutaneous infrapatellar bursitis is brought on by excessive friction between the skin and the tibial tuberosity; the edema happens over the proximal end of the tibia. Deep infrapatellar bursitis ends in edema between the patellar ligament and the tibia, superior to the tibial tuberosity. The irritation is often caused by overuse and subsequent friction between the patellar tendon and the constructions posterior to it, the infrapatellar fat pad and tibia (Anderson et al. The infection may unfold to the cavity of the knee joint, inflicting localized redness and enlarged popliteal and inguinal lymph nodes. Synovial fluid may also escape from the knee joint (synovial effusion) or a bursa across the knee and acquire in the popliteal fossa. In adults, popliteal cysts may be giant, extending so far as the midcalf, and should intervene with knee movements. The artificial knee joint consists of plastic and metal parts which are cemented to the femoral and tibial bone ends after elimination of the faulty areas. The combination of metal and plastic mimics the smoothness of cartilage on cartilage and produces good ends in "low-demand" people who have a relatively sedentary life. In "high-demand" people who discover themselves energetic in sports activities, the bone�cement junctions could break down, and the synthetic knee parts may loosen; nonetheless, improvements in bioengineering and surgical approach have supplied higher outcomes. A sprained ankle is nearly always 1858 an inversion harm, involving twisting of the weight-bearing plantarflexed foot. The individual steps on an uneven surface and the foot is forcibly inverted or lands on an inverted foot from a vertical jump. Lateral ligament sprains happen in operating and leaping sports, notably basketball (70�80% of gamers have had at least one sprained ankle). Shearing accidents fracture the lateral malleolus at or superior to the ankle joint. Avulsion fractures break the malleolus inferior to the ankle joint; a fraction of bone is pulled off by the hooked up ligament(s). This action pulls on the extremely strong medial ligament, usually tearing off the medial malleolus. The talus then strikes laterally, shearing off the lateral malleolus or, extra commonly, breaking the fibula superior to the tibiofibular syndesmosis. If the tibia is carried anteriorly, the posterior margin of the distal end of the tibia can be sheared off by the talus, producing a "trimalleolar fracture. The space involved is from the medial 1861 malleolus to the calcaneus, and the heel pain outcomes from compression of the tibial nerve by the flexor retinaculum. Such deviation occurs especially in females, and its frequency will increase with age. Often, onerous corns (inflamed areas of thick skin) additionally form over the proximal interphalangeal joints, particularly of the little toe. Hammer Toe Hammer toe is a foot deformity during which the proximal phalanx is completely 1862 and markedly dorsiflexed (hyperextended) on the metatarsophalangeal joint and the center phalanx strongly plantarflexed at the proximal interphalangeal joint. This deformity of a quantity of toes may result from weak point of the lumbrical and interosseous muscular tissues, which flex the metatarsophalangeal joints and lengthen the interphalangeal joints. A callosity or callus, hard thickening of the keratin layer of the pores and skin, typically develops the place the dorsal surface of the toe repeatedly rubs on the shoe. Callosities or corns develop on the dorsal surfaces of the toes due to stress of the shoe. They may also kind on the plantar 1863 surfaces of the metatarsal heads and the toe ideas because they bear additional weight when claw toes are present. Pes Planus (Flat Feet) the flat appearance of the sole of the foot earlier than age three is normal; it results from the thick subcutaneous fats pad in the sole. The more common flexible flat ft result from loose or degenerated intrinsic ligaments (inadequate passive arch support). Flexible flat feet is common in childhood however usually resolves with age as the ligaments grow and mature. The condition occasionally persists into maturity and should or may not be symptomatic. Rigid flat ft with a history that goes back to childhood are more doubtless to outcome from a bone deformity (such as a fusion of adjoining tarsal bones). Acquired flat toes ("fallen arches") are more doubtless to be secondary to dysfunction of the tibialis posterior (dynamic arch support) owing to trauma, degeneration with age, or denervation. In the absence of normal passive or dynamic assist, the plantar calcaneonavicular ligament fails to help the top of the talus. As a outcome, some flattening of the medial part of the longitudinal arch happens, together with lateral deviation of the forefoot. Flat feet are common in older people, particularly if they undertake much unaccustomed standing or gain weight quickly, including stress on the muscular tissues and increasing the pressure on the ligaments supporting the arches. Talipes equinovarus, the widespread sort (2 per 1,000 neonates), involves the subtalar joint; boys are affected twice as often as girls.
135 mg colospa buy with visa
The deep lamina of the distal (palpebral) part of the muscle includes clean muscle fibers spasms 1st trimester buy colospa 135 mg low price, the superior tarsal muscle spasms upper right abdomen order colospa 135 mg with visa, that produce further widening of the palpebral fissure, particularly throughout a sympathetic response. However, they appear to perform repeatedly (in the absence of a sympathetic response) because an interruption of the sympathetic provide produces a constant ptosis-drooping of the upper eyelid. Rotation of the eyeball across the vertical axis strikes the pupil medially (toward the midline, adduction) or laterally (away from the midline, abduction). Rotation around the transverse axis moves the pupil superiorly (elevation) or inferiorly (depression). Absence of these movements ensuing from nerve lesions contributes to double vision. Movements could happen across the three axes simultaneously, requiring three phrases to describe the course of motion from the primarily position. The four recti muscles are named for his or her individual positions relative to the eyeball. Because they mainly run anteriorly to connect to the superior, inferior, medial, and lateral aspects of the eyeball anterior to its equator, the first actions of the 4 recti in producing elevation, despair, adduction, and abduction are comparatively intuitive. Several components make the actions of the obliques and the secondary actions of the superior and inferior recti tougher to understand. Therefore, the inserting tendons of the indirect muscle tissue lie in the same oblique vertical aircraft. In follow the primary action of the superior indirect is depression of the pupil in the adducted place. Although the actions produced by the extra-ocular muscular tissues have been thought of individually, all motions require the action of several muscle tissue in the identical eye, assisting one another as synergists or opposing each other as antagonists. However, these muscle tissue are antagonistic as rotators and so neutralize one another in order that no rotation occurs as they work collectively to elevate the pupil. Similarly, no single muscle can act to depress the pupil instantly from the primary place. To direct the gaze, coordination of each eyes have to be achieved by the paired motion of contralateral yoke muscles (functionally paired contralateral extra-ocular muscles). The cup-like fascial sheath is pierced by the tendons of the extra-ocular muscles and is mirrored onto every of them as a tubular muscle sheath. Therefore, when the gaze is directed superiorly, the superior eyelid is further 2047 elevated out of the road of vision. Triangular expansions from the sheaths of the medial and lateral rectus muscular tissues, referred to as the medial and lateral examine ligaments, are hooked up to the lacrimal and zygomatic bones, respectively. A blending of the verify ligaments with the fascia of the inferior rectus and inferior indirect muscle tissue forms a hammocklike sling, the suspensory ligament of the eyeball. Collectively, the examine ligaments act with the indirect muscle tissue and the retrobulbar fats to resist the posterior pull on the eyeball produced by the rectus muscle tissue. In ailments or starvation that reduce the retrobulbar fat, the eyeball is retracted into the orbit (inophthalmos). The optic nerves begin on the lamina cribrosa of the sclera, the place the unmyelinated nerve fibers pierce the sclera and turn into myelinated, posterior to the optic disc. The intra-orbital extensions of the cranial dura and arachnoid represent the optic nerve sheath, which turns into continuous anteriorly with the fascial sheath of the eyeball and the sclera. The trochlear and abducent nerves cross directly to the one muscle supplied by every nerve. The superior division supplies the superior rectus and levator palpebrae superioris. On the right side, three nerves utilized to the roof of the orbit (trochlear, frontal, and lacrimal) are evident. On the left facet, the levator palpebrae superioris and superior rectus have been minimize and mirrored and the orbital fat eliminated to show the nerves that traverse the intraconal fats. It is positioned between the optic nerve and the lateral rectus toward the posterior limit of the orbit. Postsynaptic sympathetic fibers from the inner carotid plexus via the sympathetic root of the ciliary ganglion. The short ciliary nerves include postsynaptic parasympathetic fibers originating within the ciliary ganglion, afferent fibers from the nasociliary nerve that cross through the ganglion, and postsynaptic sympathetic fibers that additionally cross by way of it. The posterior and anterior ethmoidal nerves, branches of the nasociliary nerve arising within the orbit, exit by way of openings within the medial wall of the orbit to provide the mucous membrane of the sphenoidal and ethmoidal sinuses and the nasal cavities, as nicely as the dura of the anterior cranial fossa. The terminal branches are end arteries (arterioles), which provide the one blood 2050 supply to the interior side of the retina. The artery supplying the inside a half of the retina (central retinal artery) and the choroid, which in turn nourishes the outer nonvascular layer of the retina, are shown. The choroid is arranged so that the supplying vessels and larger choroidal 2052 vessels are externally positioned, and the smallest vessels (the capillary lamina) are most inner, adjoining to the nonvascular layer of the retina. The vorticose vein (one of 4 to five) drains venous blood from the choroid into the posterior ciliary and ophthalmic veins. The scleral venous sinus returns the aqueous humor, secreted into the anterior chamber by the ciliary processes, to the venous circulation. The external side of the retina can be provided by the capillary lamina of the choroid (choriocapillaris). Of the eight or so posterior ciliary arteries (also branches of the ophthalmic artery), six short posterior ciliary arteries directly supply the choroid, which nourishes the outer nonvascular layer of the retina. Two long posterior ciliary arteries, one on each side of the eyeball, cross between the sclera and the choroid to anastomose with the anterior ciliary arteries (continuations of the muscular branches of the ophthalmic artery to the rectus muscles) to supply the ciliary plexus. The vortex, or vorticose veins, from the vascular layer of the eyeball drain into the inferior ophthalmic vein. The scleral venous sinus is a vascular construction encircling the anterior chamber of the eyeball by way of which the aqueous humor is returned to the blood circulation. The superior ophthalmic vein empties into the cavernous sinus, and the inferior ophthalmic vein empties into the pterygoid venous plexus. They communicate with the facial and supra-orbital veins anteriorly and one another posteriorly. Surface Anatomy of Eye and Lacrimal Apparatus For a description of the floor anatomy of the eyelids, see "Surface Anatomy of Face. When irritated, the vessels might enlarge noticeably, and the bulbar conjunctiva might tackle a distinctly pink look when infected ("red" eyes). The normal powerful, opaque sclera typically appears barely blue in infants and kids and commonly has a yellow hue in many older 2054 folks. The anterior transparent a part of the eye is the cornea, which is continuous with the sclera at its margins. The prominence of the cornea additionally makes actions of the eyeball apparent when the eyelids are 2055 closed. The dark circular opening by way of which light enters the eyeball, the pupil, is surrounded by the iris (plural = irides), a circular pigmented diaphragm.
Colospa 135 mg cheap visa
The lateral surface of the lateral condyle has a central projection referred to as the lateral epicondyle spasms when excited 135 mg colospa for sale. The medial floor of the medial condyle has a bigger and more prominent medial epicondyle muscle relaxant before exercise buy 135 mg colospa overnight delivery, superior to which one other elevation, the adductor tubercle, forms in relation to a tendon attachment. The epicondyles present proximal attachment for the medial and lateral collateral ligaments of the knee joint. Bimanual palpation of anterior superior 1553 iliac spine, used to decide place of pelvis (pelvic tilt). The pubic tubercle can be palpated about 2 cm from the pubic symphysis at the anterior extremity of the pubic crest. The skin dimples are helpful landmarks when palpating the world of the sacro-iliac joints in search of edema (swelling) or local tenderness. These dimples additionally point out the termination of the iliac crests from which bone marrow and items of bone for grafts may be obtained. The gluteal fold coincides with the fat pad associated with the inferior border of the gluteus maximus and indicates the separation of the buttocks from the thigh. The prominences of the higher trochanters are normally answerable for the width of the adult pelvis. Because it lies near the pores and skin, the higher trochanter causes discomfort whenever you lie in your facet on a tough surface. In the anatomical place, a line becoming a member of the ideas of the larger trochanters normally passes by way of the pubic tubercles and the center of the femoral heads. The lesser trochanter is indistinctly palpable superior to the lateral end of the gluteal fold. The patellar surface of the femur is where the patella slides during flexion and extension of the leg at the knee joint. The lateral and medial margins of the patellar floor may be palpated when the leg is flexed. The adductor tubercle, a small prominence of bone, may be felt on the superior a half of the medial femoral condyle by pushing your thumb inferiorly alongside the medial side of the thigh till it encounters the tubercle. The thick base (superior border) slopes infero-anteriorly and the lateral and medial borders converge inferiorly to type the pointed apex. The posterior articular floor is easy, covered with a thick layer of articular cartilage, and is divided into narrower medial and wider lateral articular surfaces by a vertical ridge. The ridge and the balanced pull of the vastus muscles keeps the patella centered within the intercondylar groove of the femur because it provides mechanical benefit to the quadriceps femoris in extending the leg at the knee. The shafts of the tibia and fibula are related by a dense interosseous membrane composed of robust oblique fibers descending from the tibia to the fibula. Tibiofibular syndesmoses, together with the dense interosseous membrane, tightly join the tibia and fibula. The interosseous membrane additionally offers extra floor area for muscular attachment. The anterior tibial vessels traverse the opening in the membrane to enter the anterior compartment of the leg. It flares outward at both ends to provide an increased space for articulation and weight switch. The superior (proximal) end widens to form medial and lateral condyles that overhang the shaft medially, laterally, and posteriorly, forming a comparatively flat superior articular surface, or tibial plateau. This plateau consists of two smooth articular surfaces (the medial one slightly concave and the lateral one barely convex) that articulate with the large condyles of the femur. The 1557 articular surfaces are separated by an intercondylar eminence shaped by two intercondylar tubercles (medial and lateral) flanked by relatively rough anterior and posterior intercondylar areas. The intercondylar tubercles and areas provide attachment for the menisci and principal ligaments of the knee, which hold the femur and tibia together, maintaining contact between their articular surfaces. The lateral condyle also bears a fibular articular aspect posterolaterally on its inferior facet for the head of the fibula. Unlike that of the femur, the shaft of the tibia is truly vertical throughout the leg. It is somewhat triangular in cross-section, having three surfaces and borders: medial, lateral/interosseous, and posterior. It and the adjacent medial surface are subcutaneous throughout their lengths and are generally generally identified as the "shin. At the superior end of the anterior border, a broad, rectangular tibial tuberosity offers distal attachment for the patellar ligament, which stretches between the inferior margin of the patella and the tibial tuberosity. The distal finish of the tibia is smaller than the proximal finish, flaring only medially. The medial enlargement extends inferior to the relaxation of the shaft because the medial malleolus. Inferiorly, the sharp border is changed by a groove, the fibular notch, that accommodates and offers fibrous attachment to the distal finish of the fibula. On the posterior surface of the proximal part of the tibial shaft is a tough diagonal ridge, called the soleal line, which runs inferomedially to the medial border. This line is fashioned in relationship to the aponeurotic origin of the soleus muscle approximately one third of the greatest way down the shaft. Immediately distal to 1558 the soleal line is an obliquely directed vascular groove, which leads to a large nutrient foramen for passage of the main artery supplying the proximal finish of the bone and its marrow. From it, the nutrient canal runs inferiorly in the tibia earlier than it opens into the medullary (marrow) cavity. It serves primarily for muscle attachment, providing distal attachment (insertion) for one muscle and proximal attachment (origin) for eight muscles. The fibers of the tibiofibular syndesmosis are organized to resist the ensuing web downward pull on the fibula. The distal finish enlarges and is extended laterally and inferiorly because the lateral malleolus. The lateral malleolus is more distinguished and posterior than the medial malleolus and extends approximately 1 cm extra distally. The head has a pointed apex and articulates with the fibular aspect on the posterolateral, inferior aspect of the lateral tibial condyle. The shaft of the fibula is twisted and marked by the sites of muscular attachments. The tibial condyles may be palpated anteriorly at the sides of the patellar ligament, particularly when the knee is flexed. The head of the fibula is prominent at the level of the superior a part of the tibial tuberosity because the knob-like head is subcutaneous at the posterolateral facet of the knee. The neck of the fibula can be palpated simply distal to the lateral facet of the fibular head.
135 mg colospa buy with amex
Rupture of Bladder Because of the superior position of the distended bladder muscle relaxant for bruxism order 135 mg colospa with mastercard, it could be ruptured by injuries to the inferior part of the anterior belly wall or by fractures of the pelvis infantile spasms 6 months old buy colospa 135 mg amex. The rupture may outcome within the escape of urine extraperitoneally or 1392 intraperitoneally. Rupture of the superior a half of the bladder frequently tears the peritoneum, leading to extravasation (passage) of urine into the peritoneal cavity. Posterior rupture of the bladder normally leads to passage of urine extraperitoneally into the perineum. Cystoscopy the interior of the bladder and its three orifices could be examined with a cystoscope. Using a high-frequency electrical current, the tumor is removed in small fragments, that are washed from the bladder with water. It can be easily dilated with out damage; consequently, the passage of catheters or cystoscopes is less complicated in females than in males. Infections of the urethra, and particularly of the bladder, are extra widespread in girls because the female urethra is short, extra distensible, and is open to the outside through the vestibule of the vagina. Rectal Examination Many structures associated to the antero-inferior part of the rectum may be palpated through its walls. Enlarged internal iliac lymph nodes, pathological thickening of the ureters, swellings within the ischio-anal fossae [e. Tenderness of an inflamed appendix can also be detected rectally if it descends into the lesser pelvis (pararectal fossa). The internal facet of the rectum can be examined with a proctoscope, and biopsies of lesions could also be taken by way of this instrument. The operator must additionally know that the transverse rectal folds, which give helpful landmarks for the process, could briefly impede passage of those instruments. Urinary bladder: the superior and inferior portions of the urinary bladder are fairly distinct anatomically and functionally. Urethra: the male urethra consists of 4 parts, two of which are the intramural and prostatic elements. It is surrounded by the prostate, the muscular anterior "lobe" that includes the trough-like superior extension of the exterior urethral sphincter anteriorly, and by the glandular lobes posteriorly. It is firmly connected to and indents the anterior vaginal wall centrally and distally. The testes and epididymides (described in Chapter 5, Abdomen) are thought of internal genital 1396 organs on the idea of their developmental position and homology with the inner feminine ovaries. The genital organs are demonstrated: testis, epididymis, ductus deferens, ejaculatory duct, and penis, with the accent glandular structures (seminal gland, prostate, and bulbo-urethral gland). The spermatic cord connects the testis to the stomach cavity, and the testis lies externally in a musculocutaneous pouch, the scrotum. The ductus deferens has relatively thick muscular partitions and a minute lumen, giving it a cord-like firmness. The ductus crosses superior to the ureter near the posterolateral angle of the urinary bladder, working between the ureter and the peritoneum of the ureteric fold to reach the fundus of the bladder. The relationship of the ductus deferens to the ureter within the male is comparable, though of lesser clinical importance, to that of the uterine artery to the ureter within the feminine. Here, the ductus deferens enlarges to kind the ampulla of the ductus deferens before its termination. During improvement, because the testis descends inferiorly and laterally from its unique position (medial to the positioning of the kidneys on the posterior belly wall) to and then through the inguinal canal, the ureter is crossed by testicular vessels in the abdomen and by the ductus deferens within the pelvis. The umbilical ligaments, like the urinary bladder, are embedded in extraperitoneal or subperitoneal fascia (mostly eliminated on this dissection). The ejaculatory ducts are fashioned by the merger of the duct of the seminal gland and the ductus deferens. The 1400 vestigial prostatic utricle, often seen as an invagination in an anterior view, appears on this posterior dissection as an evagination lying between the ejaculatory ducts. Veins from most of the ductus drain into the testicular vein, together with the distal pampiniform plexus. They secrete a thick alkaline fluid with fructose (an energy source for sperms) and a coagulating agent that mixes with the sperms as they move into the ejaculatory ducts and urethra. Pelvic part of ureters, urinary bladder, seminal glands, terminal parts of ductus deferens, and prostate. The left seminal gland and ampulla of the ductus deferens are dissected free and sliced open. The perineal membrane lies between the exterior genitalia and the deep part of the perineum (anterior recess of ischio-anal fossa). It is pierced by the urethra, ducts of the bulbo-urethral glands, dorsal and deep arteries of the penis, cavernous nerves, and the dorsal nerve of the penis. The superior ends of the seminal glands are coated with peritoneum and lie posterior to the ureters, where the peritoneum of the rectovesical pouch separates them from the rectum. The duct of the seminal gland joins the ductus deferens to kind the ejaculatory duct. The glandular part makes up approximately two thirds of the prostate; the opposite third is fibromuscular. The fibrous capsule of the prostate is dense and neurovascular, incorporating the prostatic plexuses of veins and nerves. The anterior floor is separated from the pubic symphysis by retroperitoneal fats in the retropubic space. Lobules and zones of prostate demonstrated by anatomical part and ultrasonographic imaging. The ducts of the glands in the peripheral zone open into the prostatic sinuses, whereas the ducts of the glands in the central (internal) zone open into the 1404 prostatic sinuses and the seminal colliculus. The isthmus of the prostate (commissure of prostate; traditionally, the anterior "lobe") lies anterior to the urethra. It is fibromuscular, the muscle fibers representing a superior continuation of the exterior urethral sphincter muscle to the neck of the bladder, and contains little, if any, glandular tissue. Right and left lobes of the prostate, separated anteriorly by the isthmus and posteriorly by a central, shallow longitudinal furrow, may every be subdivided for descriptive functions into 4 indistinct lobules outlined by their relationship to the urethra and ejaculatory ducts and-although much less obvious -by the association of the ducts and connective tissue: 1. An inferoposterior (lower posterior) lobule that lies posterior to the urethra and inferior to the ejaculatory ducts. This lobule constitutes the facet of the prostate palpable by digital rectal examination. An inferolateral (lower lateral) lobule instantly lateral to the urethra, forming the major part of the best or left lobe. A superomedial lobule, deep to the inferoposterior lobule, surrounding the ipsilateral ejaculatory duct. An anteromedial lobule, deep to the inferolateral lobule, directly lateral to the proximal prostatic urethra. This region tends to undergo hormone-induced hypertrophy in superior age, forming a middle lobule that lies between the urethra and the ejaculatory ducts and is carefully associated to the neck of the bladder. Enlargement of the middle lobule is believed to be no less than partially answerable for the formation of the uvula (L. Prostatic fluid, a thin, milky fluid, offers approximately 20% of the volume of semen (a mixture of secretions produced by the testes, seminal glands, prostate, and bulbo-urethral glands that provides the vehicle by which sperms are transported) and performs a task in activating the sperms.