
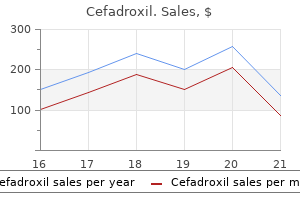
Cefadroxil dosages: 250 mg
Cefadroxil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Order 250 mg cefadroxil visa
The second pharyngeal arch provides origin to the m uscles of facial expression antibiotics yom kippur generic 250 mg cefadroxil with visa, the posterior stomach of the digastric bacteria 6 facts buy cefadroxil 250 mg mastercard, the st ylohyoid m uscle, and the stapedius. The fourth and sixth pharyngeal arches give rise to the cricothyroid m uscle, levator levi palatini, constrictor pharyngis, and the intrinsic m uscles of the larynx. The nerve provide to the m uscles can additionally be explained in term s of their em bryologic origins (see D). The hum an em bryo has 4 pharyngeal arches separated by intervening pharyngeal cleft s. Like different tissues of the pharyngeal arches, they m igrate with further developm ent to form numerous skeletal and ligam entous elem ents within the grownup (see C). Overview Pharyngeal arch artery Pharyngeal arch nerve Cartilaginous elem ent Pharyngeal pouch Pharyngeal cleft Tym panic cavit y Endoderm External auditory canal First pharyngeal arch Second pharyngeal arch Third pharyngeal arch Fourth pharyngeal arch Palatine tonsil Parathyroid glands, superior pair Parathyroid glands, inferior pair Ultim obranchial body Eustachian tube Foram en cecum Thyroid gland Thym us Mesenchym e Laryngotracheal Ectoderm groove E Internal construction of the pharyng eal arches (after Sadler) Anterior view (plane of section shown in B). The pharyngeal arches are covered externally by ectoderm and internally by endoderm. Each pharyngeal arch contains an arch artery, an arch nerve, and a cartilaginous elem ent, all of that are surrounded by m esoderm al and m uscular tissue. The exterior furrows are known as the pharyngeal cleft s, and the inner furrows are known as the pharyngeal pouches. The endoderm al lining of the pharingeal pouches develops into endocrine glands of the neck, a course of which m ay involve signi cant m igration of cells from their website of origin. F Mig ratory movements of the pharyng eal arch tissues (after Sadler) Anterior view. During em bryonic developm ent, the epithelium from which the thyroid gland is type ed m igrates from it s website of origin on the basal m idline of the tongue to the extent of the rst tracheal cartilage, the place the thyroid gland is located in postnatal life. As the thyroid tissue buds o from the tongue base, it leaves a vestigial melancholy on the dorsum of the tongue, the foram en cecum. The parathyroid glands are derived from the fourth pharyngeal arch (superior pair) or third pharyngeal arch (inferior pair), which also gives origin to the thym us. The ultim obranchial body, whose cells m igrate into the thyroid gland to form the calcitonin-producing C cells or parafollicular cells, is derived from the fth, vestigial, pharyngeal arch. The lat ter arch is the final to develop and is normally considered a part of the fourth pharyngeal arch. The external auditory canal is derived from the rst pharyngeal cleft, the t ym panic cavit y and eustachian tube from the rst pharyngeal pouch, and the palatine tonsil from the second pharyngeal pouch. Median cysts and stulas within the neck (a, b) are rem nant s of the thyroglossal duct. Lateral cysts and stulas in the neck are anom alous rem nant s of the ductal parts of the cervical sinus, which type s as a outcome of tissue m igration throughout em bryonic developm ent. If epithelium -lined rem nant s persist, neck cyst s (right) or stulas (left) m ay appear in postnatal life (c). A full stula opens into the pharynx and onto the floor of the pores and skin, whereas an incomplete (blind) stula is open at one end solely. The exterior ori ce of a lateral cervical stula is t ypically located on the anterior border of the sternocleidom astoid m uscle. This view was chosen as an introduction to the skull as a outcome of it displays the greatest num ber of cranial bones (indicated by di erent colours in B). The particular person bones and their salient features in addition to the cranial sutures and apertures are described within the items that comply with. The chapter as an entire is meant to fam iliarize the reader with the nam es of the cranial bones before proceeding to ner anatom ical details and the relationships of the bones to one another. Bones, Liga ments, a nd Joints Temporal bone, squam ous part Frontal bone Parietal bone Sphenoid bone, higher wing Ethm oid bone Lacrim al bone Nasal bone Zygom atic bone Maxilla Occipital bone Mandible Temporal bone, petrous part Temporal bone, t ympanic part B Lateral view of the cranial bones Left lateral view. The bones are proven in di erent colors to dem onstrate m ore clearly their extent s and boundaries. C Bones of the neurocranium (g ray) and viscerocranium (orange) Left lateral view. E Bones of the neurocranium and viscerocranium Neurocranium (gray) Viscerocranium (orange) � Front al bone � Sphenoid bone (excluding the pterygoid process) � Temporal bone (squam ous part, petrous part) � Pariet al bone � Occipit al bone � Ethm oid bone (cribriform plate) � Auditory ossicles � Nasal bone � Lacrim al bone � Ethmoid bone (excluding the cribriform plate) � Sphenoid bone (pterygoid process) � Maxilla � Zygom atic bone � Tem poral bone (t ym panic part, st yloid process) � Mandible � Vom er � Inferior nasal turbinate � Palat ine bone � Hyoid bone (see p. The bones of the cranium both develop directly from m esenchym al connective tissue (intram em branous ossi cation, gray) or kind indirectly by the ossi cation of a cartilaginous m odel (enchondral ossi cation, blue). Elem ents derived from intram em branous and endochondral ossi cation (desm ocranium and chondrocranium respectively) m ay fuse together to form a single bone. This explains why congenital defect s of intram em branous ossi cation a ect each the skull and clavicle (cleidocranial dysostosis). F Bones of the desmocranium and chondrocranium Desmocranium (gray) Chondrocranium (blue) � � � � � � � � Nasal bone Lacrimal bone Maxilla Mandible Zygom atic bone Frontal bone Parietal bone Occipital bone (upper part of the squam a) � Temporal bone (squam ous part, t ympanic part) � Palatine bone � Vomer � Ethmoid bone � Sphenoid bone (excluding the medial plate of the pterygoid process) � Tem poral bone (petrous and m astoid part s, st yloid process) � Occipital bone (excluding the higher part of the squam a) � Inferior nasal turbinate � Hyoid bone (see p. The bony m argins of the anterior nasal aperture m ark the start of the respiratory tract within the skull. The nasal cavit y, like the orbit s, contains a sensory organ (the olfactory m ucosa). The anterior view of the skull also displays the three clinically essential openings through which sensory nerves move to supply the face: the supraorbital foram en, infraorbital foram en, and m ental foram en (see p. Bones, Liga ments, a nd Joints Frontal bone Parietal bone Sphenoid bone, higher wing Nasal bone Ethm oid bone, m iddle nasal concha Inferior nasal concha Temporal bone Sphenoid bone, greater wing Zygom atic bone Maxilla Frontal sinus Ethm oid cells Sphenoid sinus Maxillary sinus Nasal cavit y Mandible B Cranial bones, anterior view Frontonasal pillar Horizontal zygom atic pillar C Paranasal sinuses: pneumatization lightens the bone Anterior view. These cavities, known as the paranasal sinuses, com m unicate with the nasal cavit y and, prefer it, are lined by ciliated respiratory epithelium. In am m ations of the paranasal sinuses (sinusitis) and associated complaint s are very com m on. These pillars develop along the principal lines of force in response to local m echanical stresses. In visual time period s, the fram e-like development of the facial skeleton m ay be likened to that of a fram e house: the paranasal sinuses characterize the room s whereas the pillars (placed alongside m ajor lines of force) symbolize the supporting colum ns. The m axilla is separated from the higher facial skeleton, disrupting the integrit y of the m axillary sinus (low transverse fracture). The m ain fracture line passes by way of the orbit s, and the fracture m ay moreover involve the ethm oid bones, frontal sinuses, sphenoid sinuses, and zygomatic bones. The cranial sutures are a particular t ype of syndesm osis (= ligam entous at tachm ents that ossify with age, see F). The outer floor of the occipital bone is contoured by m uscular origins and insertions: the inferior, superior, and suprem e nuchal lines. The exterior occipital protuberance serves as an anatom ical reference point: It is palpable at the back of the top. Sagit tal suture: scaphocephaly (long, slender skull) Coronal suture: oxycephaly (pointed skull) Frontal suture: trigonocephaly (triangular skull) Asym m etrical suture closure, often involving the coronal suture: plagiocephaly (asym m etrical skull). When the mind becom es dilated as a result of cerebrospinal uid accum ulation before the cranial sutures ossify (hydrocephalus, "water on the brain"), the neurocranium will broaden while the facial skeleton rem ains unchanged. The at cranial bones m ust develop as the brain expands, and so the sutures wager ween them m ust rem ain open for som e tim e (see F). They close at di erent tim es (the sphenoid fontanelle in in regards to the sixth m onth of life, the m astoid fontanelle within the 18th month, the anterior fontanelle within the thirty sixth m onth).
Purchase cefadroxil 250 mg overnight delivery
At the apical finish of the standard incision antibiotics for acne doxycycline 250 mg cefadroxil order fast delivery, the rectus portion of the quadriceps tendon is isolated and divided obliquely at an angle of 45� antibiotic guideline malaysia generic 250 mg cefadroxil, extending superiorly and laterally. The capsulotomy is straightforward to repair and permits a normal postoperative physiotherapy program. This technique may be modified by starting the snip more distally with the benefit of an improved exposure, however at the value of increased tension on the restore. This strategy maintains the musculotendinous bridge of vastus medialis and of vastus lateralis facilitating a standard rehabilitation program. It can also be very helpful when bone cement must be accessed a great distance down the tibial shaft. Mobilizing the extensor mechanism by tibial tubercle osteotomy offers superior visualization than turn down methods,30 and has the potential for lengthening and realignment of the extensor mechanism. The osteotomy, however, is technically extra demanding and has been associated with elevated morbidity when compared to proximal mobilization of the extensor mechanism. There have been a number of stories of tibial fractures occurring after tibial tubercle osteotomy. This could be achieved by protected weight-bearing within the cooperative patient, or by bypassing the osteotomy with a press-fit stem. When a brief stem is used on the tibial element, the tibial tubercle osteotomy causes focus of stress within the anterior tibial cortex and will increase the chance of fracture. Moreover, too quick an osteotomy fragment often may be associated with fracture of the tubercle fragment itself. An extra modification of this technique includes preserving a small bone shell immediately above the tibial tubercle to stabilize the fragment in opposition to proximal migration (Chandler H, personal communication; Wiedel J, personal communication). To perform the osteotomy, the incision is extended distally from the medial facet of the tibial shaft a further 10 cm. The osteotomy is carried out with an oscillating saw from the medial to lateral path. The bone block must be 8�10 cm in size, 2 cm wide and approximately 1 cm thick. The osteotomy is incomplete on the lateral side, maintaining the periosteum and muscular attachments to stabilize the osteotomy from proximal migration. The osteotomy is hinged open laterally, and the lateral attachments of the quadriceps enlargement are left connected to the lateral tibial flare. Whiteside reattached the fragment utilizing two or three cerclage wires passed around the tibial tubercle and across the tibial part inside the canal. The wires are angled down 45� to the shaft of the tibia to keep the distal attachment of the osteotomy. Following insertion of a press-fit stern, the wires are tightened on to the shaft, and the remaining joint is closed in a routine manner. During active knee extension, tensile forces are lower in the patellar tendon than in the quadriceps tendon, theoretically giving the tubercle osteotomy an advantage over the quadriplasty. Femoral Peel Mobilization of the extensor mechanism is normally enough to afford adequate publicity of the elements throughout a revision arthroplasty. However, in circumstances where the publicity stays tight and notably in stiff knees with a hard and fast flexion deformity, launch of the capsular attachments to the distal femur may be indicated. The publicity of the joint is accomplished by stripping the posterior capsule from the back of the femur. Release of the medial and lateral heads of the gastrocnemius may be necessary. The knee is destabilized in flexion permitting the tibia to be externally rotated and angled into valgus. The patella is dislocated in its valgus position with out additional mobilization of the extensor mechanism. Medial Epicondylar Osteotomy this is additionally indicated in very tight or ankylosed knees. With the knee flexed to 90� and positioned in a determine of 4 place, a 1 inch osteotome is used to elevate a 1 cm thick wafer of bone, together with the medial epicondyle and adductor tubercle, from the distal femur in a distal to proximal course. The adductor magnus, the epicondyle and the attached collateral ligament are raised as a continuous flap. The wafer of bone is hinged from the femur exposing the posteromedial joint capsule. Fibers of the posterior indirect ligament and posteromedial joint capsule may have to be launched from the posterior margin 3378 TexTbooK of orThopedics and Trauma three. Technical issues of complete knee arthroplasty after proximal tibial osteotomy. Midline or parapatellar Incision for knee arthroplasty: a comparative examine of wound viability. The relationship of lateral releases to patellar viability in whole knee arthroplasty. Postoperative patellar issues with or without lateral launch during whole knee arthroplasty. Stress fracture of the patella following duopatellar total knee arthroplasty with patellar resurfacing. It is then possible to evert the patella and open the knee by external rotation and hinging into valgus. The femoral epicondylar osteotomy is inherently secure as the adductor tendon inserting into the bone fragment creates proximal stability, and the collateral ligaments provide distal stability. It is possible to perform this strategy laterally as properly by elevating the lateral femoral epicondyle. This could also be necessary in circumstances of allograft reconstruction of the distal femur allowing full skeletonization for publicity and removal of the parts. The lateral epicondyle will reposition much because the medial epicondyle throughout closure of the capsule and could be reattached with staples or screws. Quadriceps Myocutaneous Flap this approach which has been described for tumor resection,37,forty one can be utilized for unusually advanced revision knee arthroplasties the place a circumferential exposure of the distal femur is critical. The extensor mechanism is accessed using a U-shaped myocutaneous flap based mostly on the quadriceps muscle. Surgeons performing difficult revision cases ought to have a sound knowledge of the native anatomy, and must be familiar with a broad range of approaches. If not, consideration must be given to an extensile or devoted revision strategy. Osteotomies and soft-tissue incisions ought to be adequate and avoid uncontrolled bone and soft-tissue disruption. The acceptable surgical publicity ought to be determined by cautious preoperative planning primarily based on a data of the earlier exposures used, an evaluation of the kind of implant to be eliminated, and on the extent of bone deficiencies to be reconstructed. Joint line restoration and flexion extension steadiness with revision complete knee arthroplasty. The use of a modified V-Y quadricepsplasty throughout total knee replacement to achieve exposure and enhance flexion within the ankylosed knee. The technical challenges embrace upkeep of joint line and alignment of the limb, ligament steadiness in addition to the ways of dealing with the loss of bone inventory. Type 2 defect: Damaged metaphyseal bone-Loss of cancellous bone that requires substitution with cement, bone graft or augments to restore joint level.
Diseases
- Diethylstilbestrol antenatal infection
- Growth delay, constitutional
- TNF receptor associated periodic syndrome (TRAPS)
- Phosphoribosylpyrophosphate synthetase deficiency
- Talipes equinovarus
- Yellow nail syndrome
Purchase cefadroxil 250 mg fast delivery
However antibiotic resistant uti in dogs cefadroxil 250 mg order with visa, latest studies recommend that in as a lot as inhaled antibiotics for sinus infections cefadroxil 250 mg discount overnight delivery 30% of the cases the extra chromosome 21 could also be of paternal origin. The attribute mongoloid facies with epicanthic folds and mental retardation give these kids a putting resemblance immaterial of the race or area they belong to . Autosomal Recessive Inheritance Autosomal recessive issues form the only largest category of Mendelian problems. In general, ailments ensuing from mutations involving enzyme proteins are inherited as autosomal recessive traits. The characteristics are as follows: � the affected people are homozygotes whereas their dad and mom are heterozygotes, i. The pedigree chart exhibits a horizontal sample with involvement of siblings of either intercourse. Pycnodysostosis the condition is characterized by brief stature, delayed closure of cranial sutures, dysplasia of skull bones, flattened obtuse mandibular angle, dental caries, partial or whole aplasia of terminal phalanges, elevated bone density and proclivity for fractures of bones. Thus, the male is hemizygous for X-linked mutant genes resulting in the expression of those disorders in them. Duchenne Type Progressive Pseudohypertrophic Muscular Dystrophy It accounts for 65% of all dystrophies. While the precise muscle mass is reduced, pseudohypertrophy of some muscle tissue (calf muscles) occurs as a outcome of infiltration of mature fat cells between degenerative muscle fibers. In addition to the frequent X-linked recessive transmission, it might be transmitted as autosomal recessive trait. In an autosomal dominant model, carriers of the G allele (35% of subjects) had more fast development and 12�19% less grip power. Myositis Ossificans Progressiva (Fibrodysplasia Ossificans Progressiva) It is characterised by progressive ossification within muscle tissue and certain particular skeletal abnormalities. It is a rare disabling illness in which group after group of muscles, tendons and joints ligaments are affected changing the sufferer right into a veritable statue. This is followed by metaplasia of collagenoblasts into osteoblast and chondroblast which ultimately transform into mature bone. It progresses along X-linked Dominant Inheritance It is similar to autosomal dominant inheritance besides that all the daughter, however not one of the sons of affected male will exhibit the illness. This consciousness ought to immediate early genetic consultation and testing and the establishment of assiduous precautions to forestall iatrogenic hurt. Microdactyly of great toes with or without hallux valgus and generally of thumbs is almost diagnostic, and forms part of the syndrome. The monophalangeic nice toe is attribute of patients with myositis ossificans progressiva. Other abnormalities include brief first metacarpal bones, microdactyly, malformation of the little finger, reduction defects of all limbs and abnormalities of the cervical vertebrae. Minor traumas similar to neglected intramuscular injection usually prove to be precipitating the episode. Characteristically muscles concerned are these of the hand and again, then the shoulder muscles and hips. The muscles of the face, larynges, tongues and diaphragm are characteristically spared. Low-frequency radiotherapy and immune modulators, which are in vogue for most cancers chemotherapy, are also probably being modified for scientific use. One vista which holds great promise for the remedy of this dismal situation is the usage of gamma interferon but the purposes are but evolving. The hallmark or pathognomonic characteristic of this uncommon and disabling genetic condition is characterised by congenital malformation of the great toes and by progressive heterotopic ossification in particular anatomic patterns. Most sufferers with fibrodysplasia ossificans progressiva are misdiagnosed early in life before the looks of heterotopic ossification and undergo diagnostic procedures that may cause lifelong incapacity. Recently, the genetic cause of fibrodysplasia ossificans progressiva was identified, and definitive genetic testing for fibrodysplasia ossificans progressiva is now out there before the appearance of heterotopic ossification. The person is tall with exceptionally long extremities especially of the forearm and the thighs with lengthy fingers and toes (arachnodactyly). Dislocation of the lens, cystic medionecrosis of the aorta resulting in dilation or rupture and joint laxity are different notable features. Clinical observations have shown qualitative and quantitative differences in certain disorders relying whether or not the transmission is maternal or paternal. Through the mechanism of genomic imprinting one of the parental genes is marked to scale back its expression in the offspring, and each allele is completely different in expression relying on its parental derivation. In sure areas of the genome, genes from the mother are imprinted and in other space genes from the father are imprinted. If a gene is maternally imprinted, it will be turned off in expression when inherited from the maternal side, however will express itself if inherited from the father. Inheritance of both members of a chromosome pair from only one mother or father is called uniparental disomy and could end in an irregular phenotype. Ninety p.c of these seen at start right spontaneously or with early postural intervention. Intrinsically derived deformations are a results of major neuromuscular illness or malformations. Breech presentation is associated with a 10-fold increased incidence of deformities. Extrinsic factors like small uterine cavity, being pregnant in one horn of a unicornuate uterus, presence of multiple fetus or abnormal web site of placental implantation also cause deformities. Clinical displays are as follows: � A affected person who has previously delivered an infant with lethal dwarfism or bone dysplasia and needs antenatal assessment at the subsequent conception. Nomograms can be found for fetal biparietal diameter and size of all long bones. Special nomograms with percentiles for gestational age have been constructed to relate relative lengths of lengthy bones to each other or different body components to long bones. An approach to structural defects includes an evaluation of the character of the defect, clues to the time of onset, mechanisms of damage and potential etiology. There can be a single primary defect in growth or a multiple malformation syndrome with secondary defects arising out of the developmental penalties of the first defect. The actual size of long bones and mineralization is determined in the early second trimester. Fractures, bowing and shortening (rhizomelic, mesomelic, acromelic) have to be ruled out. An precise analysis ought to be entertained solely after full clinical assessment and an entire set of radiographs. Most instances comply with Mendelian inheritance which may be obvious from the family pedigree pattern. A special effort must be made to get pictures, radiographic evidences and necropsy details on all dysplasias, more so for stillbirths. Thoracic circumference is the same as (anteroposterior diameter + transverse diameter) � 1. Ribs and vertebrae are evaluated in the second trimester by a longitudinal scan done for the axial skeleton. The different modalities of prenatal diagnosis are as follows: Autosomal Dominant Conditions the chance to offspring of affected members is half regardless of whether the illness is totally developed or preclinical.
Discount cefadroxil 250 mg visa
In addition infection jaw bone symptoms cheap 250 mg cefadroxil otc, the features in elbow vary of movement with this therapy are less than those reported with different forms of conservative treatment/ bracing antibiotic shelf life generic cefadroxil 250 mg on line. Morning 15 min scorching tub, eight am�12 pm flexion, 12 pm�6 pm extension, 6 pm�12 am flexion, evening 15 min icing, 12 am�6 pm extension, 1 hour rest in between splint adjustments. At four weeks of splinting 80� correction is fascinating, night time splints to proceed till 6 months, full correction realized at the end of 1 12 months. Nonoperative management of stiffness ought to be thought-about for up to 6 months (after contracture sets in)20�22 evidence has been discovered that even extended contractures profit from splinting. Week 1-alternate flexion or extension splint each 2�3 days to be adopted with 2nd week onwards week of maximum extension or flexion after cryotherapy stretch under supervision till 6�8 weeks. In arthroscopic contracture series: After first 48�72 hours of volar extension splint, steady cryotherapy for the primary two weeks with minimal dressing inside cryocuff with or without sling permitting energetic assisted range of movement during early postoperative period using gravity assisted flexion/extension and pronation/supination, serving to with unaffected arm. During third and fourth weeks 2 hours of cryotherapy periods 4 times per day with energetic range of motion, gravity eliminated adopted by anti gravity movements, active and passive selfassisted workout routines with 1�2 lbs. Elbow Rehabilitation in Children Avoid surgery if attainable as results are unpredictable and rehabilitation is extraordinarily troublesome hence one ought to delay surgery until physis closure. Manipulation beneath Anesthesia It is a useful adjunct in rehabilitation of posttraumatic elbow stiffness, especially in the setting of delayed recovery of functional arc of motion following any elbow surgical procedure for instance, arthroscopic contracture launch. Also, it helps to improve the forearm rotation and prevent pronation-supination contracture formation following radial head fixation. In retrospective review of forceful joint manipulation in 230 head injured adults with heterotopic ossification, Garland et al. Early "easy" launch of posttraumatic elbow contracture related to heterotopic ossification. Resection of elbow ossification and continuous passive motion in post-comatose patients. The prevention of heterotopic ossification in high-risk patients by low-dose radiotherapy after complete hip arthroplasty. Current Therapy in the Management of Heterotopic Ossification of Elbow: A Review with Case Studies (New York). Restoring range of movement via stress rest and static progressive stretch in posttraumatic elbow contractures. Turnbuckle orthotic correction of elbow flexion contractures after acute injuries. Reverse dynamic slings: Results of use in the therapy of posttraumatic flexion contractures of the elbow. The mons pubis, the perineum, and the labia share an ectodermal origin and have a keratinized, stratified, squamous epithelial structure with hair follicles, sebaceous glands, and sweat glands, much like these of other skin websites. The diploma of thickness of the vulvar skin epidermal keratinization progressively decreases from the outer half, the labia majora, to the inner part, the labia minora. The vulvar vestibule, conversely, is nonkeratinized and derived from the endodermal fold. The posterior ends of the labia and the connecting skin between them type the posterior labial commissure. The labia majora are lined with a various amount of hair and include sebaceous, sweat eccrine, and apocrine glands. Anteriorly, the labia minora are cut up into two elements: one part passes over the clitoris to kind the prepuce, whereas the opposite joins with the contralateral one underneath the clitoris and varieties the frenulum. They are fairly small in childhood, develop throughout puberty, after which turn out to be atrophic after menopause. The physique consists of two corpora cavernosa coated by their ischiocavernous muscle tissue. The glans is a small mass of erectile tissue that caps the physique of the clitoris and is hidden by the prepuce. The mucosa of the distal third of the urethra is lined by stratified squamous epithelium, whereas the proximal two-thirds are lined by stratified transitional epithelium. It may be very prominent in newborn children, because of maternal estrogens, and it regresses throughout childhood earlier than the normal pubertal changes. Sexual intercourse and childbirth trigger the disappearance of its bigger part, leaving only remnants. Lymph drains from the vulva into the medial group of superficial inguinal nodes on each the ipsilateral and contralateral sides. The sensory nerve system involves the genitofemoral nerve (L1 and L2) and the cutaneous branch of the ilioinguinal nerve (L1) for the anterior vulva, the pudendal nerve for the posterior a half of the vulva, and the clitoris and the perineal branch of the posterior cutaneous nerve of the thigh for a small area of the posterior vulva. A skin biopsy is seldom required in persistent types to exclude different unusual situations, such as Hailey�Hailey disease. Differential analysis: Candidiasis, bacterial infections, eczema (contact, atopic, and seborrheic dermatitis), Hailey�Hailey illness, inverse psoriasis, erythrasma, dermatophytosis, acrodermatitis entheropathica, Darier illness, and extramammary Paget disease. Therapy: Treatment with a topical barrier and lenitive nongreasy lotions and trauma avoidance is often effective. Prevention and remedy of intertrigo in giant skin folds of adults: A systematic review. Symptoms are highly variable and will range from minimal discomfort to intense itching and/or burning. If pruritic, excoriations and lichenification because of scratching and rubbing may be noticed. Definition: Psoriasis is a chronic and/or relapsing erythemato-squamous inflammatory skin dysfunction. Local components (mechanical or chemical irritation from tight garments, sexual activity, aggressive hygiene products, bacterial overgrowth, and so forth. Epidemiology: the genitocrural area is type of at all times affected in inverse psoriasis, although only a minority of sufferers show an unique genital involvement. Clinical course: It runs a continual and relapsing course, inflicting significant psychological results. In case of bacterial or yeast superinfection, fissuration, oozing, and crusting may occur. Diagnosis: It may be advised by the presence of psoriatic lesions at different sites, typical nail findings or joint complaints, but traditionally requires histological affirmation. Differential diagnosis: Candidiasis, bacterial an infection, dermatophytosis, erythrasma, eczema (contact, atopic, and seborrheic dermatitis), Hailey�Hailey illness, lichen simplex chronicus, and Darier disease. Therapy: In case of exclusive genital involvement, topical corticosteroids, together or not with vitamin D analogs (calcipotriol), or calcineurin inhibitors (pimecrolimus ointment or tacrolimus cream) could also be helpful. Systemic treatment is indicated when vulvar involvement happens as part of a extreme generalized psoriasis. Prevention of local traumas and accurate genital hygiene must be recommended so as to prevent bacterial and/or fungal secondary infections associated to the disease itself or favored by the long-term use of topical steroids or immunomodulators. Vulvar psoriasis in adults and youngsters: A medical audit of 194 circumstances and evaluate of the literature. Evaluation of the vascular sample in psoriatic plaques in youngsters utilizing videodermatoscopy: an open comparative research. The main complaint is burning, but some sufferers are asymptomatic or have gentle pruritus; eroded lesions are quite painful.
Discount cefadroxil 250 mg mastercard
The specific muscle tissue which are essential are as follows: � Flexors of the fingers and thumb to hold handgrips firmly � Dorsiflexors of wrist to stabilize the wrist in practical place � Extensors of the elbow to stabilize elbow in slight flexion � Flexors of the shoulder to transfer the walking help ahead � Depressor of the shoulder girdle to assist the physique weight antibiotic kinds cefadroxil 250 mg generic amex. The distance between bars and the peak of the bars can be adjusted in order that the elbows are in 30� of flexion antibiotic resistance can we ever win cefadroxil 250 mg discount otc. Holding the cane in the reverse hand widens the bottom of support and reduces the stress on the concerned decrease limb by shifting the center of gravity toward the contralateral arm. The top of the cane must be so adjusted that the very best level is at the level of the greater trochanter. Gait Patterns Point Gaits � Four-point gait (sequence): Right crutch, left foot, left crutch, proper foot. This is slow and difficult to be taught but is very steady and is usually utilized by ataxic patients. This stable gait pattern can also be utilized by ataxic patients and considerably reduces weight bearing. Crutches Crutches give better stability than canes as it has two-point contact with the physique. Axillary Crutches Axillary crutches provide better trunk support and might transmit as a lot as 80% of body weight. The patient is measured from heel to anterior axillary fold and 5 cm is added to accommodate shoes. In an upright place, distance from anterior axillary fold to some extent 15 cm laterals to little toe. Wheelchair the goals for wheelchair prescription are as follows: � Maximization of environment friendly impartial mobility � Prevention/Minimization of deformity or damage � Maximization of impartial functioning � Projection of wholesome, engaging, body picture � Minimization of short-term and long-term gear value. Walkers Parallel walker: this might be described as miniature portable parallel bars. Manual Wheelchair Components � Frameandaxle � Wheelsandtyres: Solid tyres work better on smooth surfaces. Pneumatic, treaded tyres work higher on uneven terrains � Hand rims, wheel locks, grade aids � Casters: Front casters are used. Small exhausting casters turn properly, whereas massive pneumatic casters are better on uneven terrains. Back peak should be low enough to avoid pushing the scapulae and shoulders forward. It should be excessive sufficient so that the foot is supported sufficiently to preserve circulation within the decrease extremity however not so high in order to shift the load the leg backward to ischial tuberosity. Selection of seat and cushion must take following factors in account: � Stability of support for upper extremity function � Pressure distribution � Maintenance of posture to stop deformity � Seatwidth:1" wider than the width of widest part of buttocks (A). These are gained through the biomechanical effects of: � Trunk help � Motion management � Spinal realignment � A partial switch of weight to trunk in case of cervical spine when affected person is upright. Though custom molded and halo kind produce no movement in cervical spine at an individual vertebral level the orthotic gadget must not be fitted so tightly that the strain exerted by the orthotic gadget exceeds a capillary stress of 20�30 mm of Hg. The affected person will attempt to change the posture in the orthosis to present consolation. If the orthosis is merely too tight, the affected person will either loosen it or reject it altogether. Collars the basic collar is a device that wraps round a neck and is adjustable circumferentially. It might have provision for peak adjustment, be single or a quantity of layered, and is of variable firmness. Materials used include resilient polyethylene foams, sponge rubber and felt in addition to inflexible polyethylene sheeting. Cervicothoracic Orthosis the assorted degree of neck fixation offered by a cervical orthosis is as proven in Table 1. This device is definitely applied with affected person supine in the case of spinal wire injury and requires little or no affected person movement by the orthotist in its utility and becoming. Postappliances Four postcollar: It consists of chin and occipital piece related by four uprights to sternal and thoracic plate. Flexible Spinal Orthosis Sacroiliac belt It encircles the pelvis between iliac crest and trochanters. Sacroiliac Corset It is a fabric garment that encompasses the pelvis and is adjustable in circumference by means of facet, front, again laces or hooks. Anteriorly the inferior border is simply above degree of pubic symphysis and posteriorly it extends to the apex of gluteal bulge. It extends anteriorly from just under the xiphoid processes to above the pubic symphysis. Modifications include posterior rigid or semirigid stays, posterior pads, extra-abdominal reinforcements, and so forth. Functions Anterior and lateral trunk containment elevates the intracavitary pressure, reducing the loadings on the vertebras and disk. Depending on the quantity, placements and rigidity of vertical stays, three level strain is utilized that tends to restrict the spinal motion. An interscapular band stabilizes the uprights and serves as attachment for axillary straps. Function A three point pressure system restricts forward flexion within the thoracolumbar space and encourages hyperextension posture. Functions It applies two-three pressure systems-one restricts trunk extension, will increase intracavitary strain and decreases lordosis, and second acts to prohibit trunk flexion. The thoracic band extends anteriorly and superiorly and subclavicular pads are offered. Two oblique lateral uprights are attached pivotably to the lateral uprights and rigidity to the pelvic band. It offers single three level drive system that limits extension however encourages flexion. The design is sort of efficient in sustaining trunk alignment and aside from bony prominences, contact is essentially total. Orthoses for Spinal Deformity the objectives of remedy of grownup idiopathic scoliosis: � Control curvature, enhance steadiness and cosmetic appearance at the similar time preventing the curvature from rising and requiring surgical stabilization. Table three: Pads used for various curves Major curve High thoracic Thoracic Thoracolumbar Lumbar Pad Trapezius Thoracic Oval and lumbar Lumbar Milwaukee brace Description It consists of molded pelvic part with three uprights, one anterior and two posterior, connected to a neck ring, the pelvic section and neck ring curving posteriorly. Custom molding of pelvic part is finished which is both made from leather-based or thermoplastic material. Biomechanics It works on a three or 4 point pressure system which is definitely a passive system. The pads exert their drive through ribs in thoracic and thoracolumbar space, with the lumbar pad appearing immediately over the lumbar spine via paravertebral muscular tissues. This tends to shift the vector of its corrective force extra laterally minimizing the anterior pressure. Improvement could be obtained in affected person with progress potential with mild to average curvature of 20�40�. Patient should put on the orthosis full time, 23 hours a day till the tip of adolescent growth spurt.
Syndromes
- Liver disease
- Bronchoscopy with washings, biopsy, and bronchoalveolar lavage
- Poor vision in one eye
- Do you have abdominal distention?
- Sinusitis
- Blood test to check vitamin A levels
- Lumbar puncture (spinal tap) with careful testing of walking before and after the spinal tap
- 100% alcohol = 200-proof
- Hammer toe
- What is the pattern of the cough? Did it begin suddenly? Has it been increasing recently? Is the cough worse at night? When you first wake up?
Cheap cefadroxil 250 mg with amex
It is used in prosthetic and orthotic joints antimicrobial wash cefadroxil 250 mg buy generic online, metallic bands antibiotic amoxicillin generic cefadroxil 250 mg with visa, rivets, cuffs, cables, springs, bearings, and hydraulic and pneumatic components. Joints, Joint Mechanism and Structures � Motion in a single designated airplane � About one axis: Uniaxial � About multiple axes: Polycentric � Motion in two designated planes � About two axes: Dual axis � Motion in three planes � About finite axes: Multiaxial � About infinite variety of axes: Flexible � No motion in any aircraft: Rigid � Alignment units Aluminum this is lighter than metal. It is helpful in higher extremity, pediatric and different applications the place weight is a major concern. These are of two sorts: the one replaces delicate tissues of the limb and provides form; the other supplies skin. Secondly, there are formed fairings used without underlying soft tissue element; made of glass fiber or nylon fiber impregnated with plastic prefabricated to completely different shapes and sizes. Plastics these are any artificial materials that may be molded, extruded, laminated or hardened into any type. Plastics are lightweight and prosTheTics and orThoTics: an inTroducTion offer quite a lot of flexibility. They may be formed into complex anatomic shapes and are inert and impervious to body fluids thereby maintaining good hygiene levels. Plastics may be strengthened with fibers corresponding to glass or carbon to kind plastic composites that have higher load bearing capability and skill to retailer and release power. Flexible foams: Flexible foams of various densities and thicknesses are used for various functions within the subject of prosthetics and orthotics corresponding to: � Padding or lining of appliances (making the home equipment washable) � Making soft sockets/inserts for prosthetic use � Molded insoles for the partially sensate/insensate/deformed foot � External beauty cowl for endoskeletal prostheses. Thermoplastics these supplies become delicate and malleable when heated and become hard when cooled. Materials that become workable at temperatures less than 70� centigrade are referred to as "low temperature thermoplastics" and with care they are often fashioned instantly on body phase. These are also called as reminiscence plastics, since they are often fashioned and deformed umpteen number of times. The materials that turn out to be malleable above 80�C are referred to as "excessive temperature thermoplastics" these must be shaped over. They are used for making posterior shoe inserts, spinal, jackets and prosthetic sockets depending on the thickness of the sheet used. Elastomers Generic name: Polyurethane thermoset these are noncellular but resilient thermoplastics which are ready stretch and deform at room temperature. They are sometimes termed viscoelastic supplies as they exhibit each elastic and plastic properties. Composite Materials these are shaped from mixture of plastic with a number of additives so that the resultant composite material has particular properties not possessed by plastic alone. Many of the orthoses launch and retailer vitality benefit from this property of carbon fiber strengthened plastic components. The mannequin may be laminated with layers of cotton/nylon stockinette interspersed with layers of fiber glass or carbon fiber for imparting strength in medium of either polyester or epoxy resin to form a laminate. The laminate could be sanded, ground down, drilled and riveted and could be pigmented. They are used for making prosthetic sockets and components requiring extensive load bearing capabilities. Properties of wood are lightweight, sturdy, cheap, simply formed and constant in texture. They are laminated from the exterior to impart energy, resistance to water and enhance cosmesis of the prosthesis. Foamed Thermoplastics these are formed by forcing nitrogen or another fuel throughout heating. These are open cell or closed cell supplies, depending on the cells shaped by the fuel bubbles are linked or remain separated from each other. Generic name Polyethylene foam Ethylene vinyl acetate plus polyethylene foam Polyurethane foam Leather Leather of various varieties have various uses within the prosthetic and orthotic business as mentioned under: � Orthopedic footwear (buffalo hide and cow hide) � Thigh lacers for standard prostheses � Lining/padding material for P and O home equipment � Fixation straps � Molded insoles. Orthotic application Foot orthoses, shoe inserts, accommodative foot put on, padding on inflexible orthoses Shoe inserts or inlays Shoe inserts/inlays, vibration gloves and grips Fabric Natural wool, cotton, silk, lycra, and so forth. In prostheses these are used for waist belts, straps, harnesses, socks that maintain pores and skin dry, cushioning of limb, taking over space to enhance becoming of prosthesis on limb segments. In orthoses these are used for fastening or for less rigid supports like corsets, belts, stockings. They could be broadly divided into two categories: (1) rigid foams and (2) flexible foams. They are additionally used for making pressure garments whereby compressive forces are employed to obtain volumetric reduction of the section in query. Rubber Elastic properties and excessive coefficient of friction make these helpful for padding in prosthetic and orthotic gadgets for seals in hydraulic and pneumatic mechanisms, for heels, bumpers in prosthetic toes and special footwear. Fabrication Option Components which are mass-produced and stocked by prosthetist are prone to be of: 1. Standardized, interchangeable off the shelf components ought to make replacement and repair of units easier and faster. Important Characteristics of Prosthetic and Orthotic Materials Strength the maximum external load, which a part can stand up to. Central Fabrication vs Local Fabrication Central fabrication allows complicated and expensive technology with out the necessity for each faculty to buy, use and keep costly, excessive expertise trendy gear. Stiffness Stress strain ratio, the amount of bending power and stiffness each depend on kind of material, thickness and form of fabric. Cylindrical and semicircular shapes and parts with ridges, flanges or corrugations are inherently stronger and stiffer than flat and skinny sections. Areas of concern are interfaces of two supplies that have considerably completely different properties and areas that are stretched or notched. Disadvantages of Central Fabrication � There is a communication drawback with technicians. Fabrication � Fast, modular � Readily and broadly obtainable Economics � Affordable � Cost-effective prosTheTics and orThoTics: an inTroducTion Reactions and Adjustment Associated with Amputation and Use of Prosthesis Physical Factors � Loss of motor perform � Loss of sensory suggestions � False joint between skeletal system and prosthesis resulting in feeling of insecurity. Pressure drawback like atrophy of subcutaneous tissue, muscle, osteoporosis, physique spurs, allergic reactions to socket material, cysts, infections, and decreased blood move and neuromata could occur � Central body temperature regulation drawback might occur, due to lost physique phase. Perspiration over rest of the body increases � Increase in fatigue due to elevated vitality consumption � Normally the features carried at subcortical degree automatically now require cortical consideration by the amputee. Such an attention limits concurrent activities � Discomfort is related to the prosthetic device � Phantom sensation. Vocational/Economic Factors these are more in laborers than skilled, managerial or govt duties. The acceptance of upper extremity prosthesis is usually low as compared to decrease extremity prosthesis. The longer the patient is without a prosthesis, the more he/she learn operate single handed, utilizing residual limb for object stabilization as wanted. Flow chart 1 Terminal devices Body Powered Components It makes use of body movements managed with harness straps and cables to function the terminal device. Terminal Devices the terminal device is considered most essential element of upper extremity prosthesis because it supplies substitute of probably the most required operate, i. Passive mitt is soft, flexible, mitten-shaped system with skintoned rubberized material for infants to initially develop bilateral activities. Passive hand is mild weight, hand-shaped system with bendable or spring-loaded finger for static grasper.
Cefadroxil 250 mg purchase without prescription
Lysosomal enzymes bacteria resistant to antibiotics purchase cefadroxil 250 mg on line, alkaline phosphatase for analysis of hypophosphatasia bacteria 2013 generic cefadroxil 250 mg with amex, karyotyping in circumstances of a number of arthrogryposis and chromosomal breaks in instances with radial defects are some available exams. With a scientific approach and detailed sonographic evaluation, at least 80% of the lethal skeletal dysplasias24 may be recognized antenatally. X-linked Disorders Recognition of this pedigree sample and detection of female carriers is crucial. Female carriers will transmit the trait to 50% daughters who will again be carriers, and to 50% male progeny who will be affected. Neural Tube Defects Multifactorial Inheritance A basic rule for recurrence risk is 3% (1�4%), zero. Those orthopedic malformations that are the consequence of another major malformation. The recurrence danger is 5% and 10�15% with one and two affected sibs, respectively. Congenital Talipes Equinovarus (Clubfoot) the incidence is 1:1,000 births with a M:F ratio 2:1. Families that have a robust genetic part of clubfoot only make up about 20�25% of all children with clubfoot. These transcription elements activate other genes which are responsible for normal limb development in the first 12�15 weeks of gestation. Further studies are required to determine which genes are activated by these factors. One factor that clinicians have noted for some time is that the calf is smaller in youngsters with unilateral clubfoot, and it seems to go hand-in-hand that kids with these genetic defects are lacking many tissues that should have developed earlier when these transcription factors are performing on the limb bud. They are utilizing a genetic method called exome sequencing, which sequences all 23,000 genes in a single person, to construct a analysis database. The environment alone or the environment interacting with genes may also trigger clubfoot, in accordance with Gurnett. Smoking and diabetes are risk factors for the clubfoot and these environmental components could play extra of a job in genetically vulnerable people. Anesthesia, as a needed adjunct, has to be tailored based on the age, measurement and basic condition of the patient, as nicely as the surgical procedure. Pediatric anesthesia could probably be thought-about a gentler, extra refined form of anesthesia with the risk threshold lowered inversely proportional to the age of the affected person, especially below 2 years of age. The incidence of significant desaturation is significantly larger in youngsters under 2 years, and they suffer three-times the grownup incidence of cardiac arrest. Even slight trauma may cause crucial reductions in airway, extra so in presence of developmental anomalies, inflammatory situations, etc. Significant oral and airway abnormalities do exist which must be screened earlier than induction of anesthesia. Infants (a child beneath 1 year) have a big physique surface area and lack warmth insulating subcutaneous fat. As a result they lose heat quickly in a cool surroundings like the operation theater. The capability to shiver and generate heat by this muscular activity is poor in infants. Their various for warmth era is by non-shivering thermogenesis from brown fat (brown because of high vascularity). A hypothermic baby could not reply to hypoxia by increasing ventilation as seen in a normothermic child. Preoperative Considerations A youngster beneath 2 years has a larger extracellular fluid compartment which varieties the volume of distribution for water soluble medication. The immaturity of kidney and liver capabilities additionally results in longer half-life of drugs. The plasma proteins produced by liver are decrease resulting in coagulopathy, making administration of vitamin K obligatory before any neonatal surgery. The low albumin values result in much less protein binding of drugs leaving greater ranges of free medication within the blood. The colloid osmotic stress is decrease with a tendency to tissue edema with even slight fluid overload. They have mature renal and hepatic features, regular serum proteins, fat and muscle mass. Thus, a normal child really requires barely larger dose per kilogram of drugs than an grownup. Temperature Regulation A knowledge of temperature regulation and its upkeep in infants during anesthesia helps to cut back the morbidity and General pediaTric orThopedics Inhalational Anesthetics Halothane: Halothane remains the mainstay of inhalational anesthesia in pediatrics. It is the drug of selection for inhalational induction due to its nice scent, predictable period of motion, fast recovery, relaxant property and its remarkable security report in kids. There have been occasional incidences of shocked myocardium in the pediatric age group which has made its use unpopular. It is a helpful agent with remarkable analgesia and minimal cardiovascular melancholy. It is now the choice of inhalational anesthetic amongst the pediatric anesthesiologist. Except for its excessive value the drug is remarkably popular for early restoration and discharge time. Sedatives and Hypnotics Vallergan in 3 mg/kg dose and triclofos in 15 mg/kg dose are both good premedicants. Interestingly Fentanyl lollipops can be found within the western nations, sedation turns into easier. Scoline apnea is a uncommon entity and is to be treated symptomatically by intermittent optimistic stress air flow as long as it lasts whereas the patient is stored normothermic. Intravenous Anesthetics these should be dealt with with caution due to their efficiency and the benefit and speed with which overdose could be given. The dosage has to be accurate and amenities for securing the airway saved ready always. Often the author double dilutes the drug making it secure for injection and lowering the incidence of thrombophleblitis. Thiopentone: In a dose of 4 to 6 mg/kg is adequate to induce anesthesia in healthy unpremedicated babies. Even a small overdose is adequate to trigger cardiovascular and respiratory melancholy. Venepuncture could be achieved after the kid has slept, for subsequent anesthesia. This is an efficient alternative to halothane (the extra generally used inhalational agent) in patients with a identified historical past of neonatal jaundice.

Generic 250 mg cefadroxil visa
This rod can be simply eliminated at the end of the procedure infection jokes discount cefadroxil 250 mg without a prescription, b-A K-wire is inserted via the medial malleolus into the distal fragment antibiotics for acne cysts cefadroxil 250 mg line. Then up the proximal fragment just wanting growth plate, corticotomy; (E) Lengthening at the corticotomy website 3080 textbook of orthopediCs and trauma Contact area: One of the most important components in reaching union is to maximize cross-sectional space of contact between the 2 fragments. Severe deformity of the right leg, exhibiting a spiral twist round its axis and related to 18 cm of shortening. Radiograph of the patient showing tibial pseudarthrosis and a hypertrophied, deformed fibula; (C) Two osteotomies done within the fibula. Surprisingly, regenerate appeared in the tibial pseudarthrosis; (E) Clinical picture of the affected person after fixator removal reveals completely corrected deformity with regeneration of the tibia. Since the regenerates of each the tibia and fibula are thinned out proximal and distal tibia-fibular fusion has been accomplished; (F) X-ray showing full correction of deformity Congenital anomalies pseudarthrosis. It requires a multidisciplinary process performed by an professional microvascular surgeon and an orthopedic surgeon. The operative process consists of harvesting of the vascularized fibula with the peroneal vascular pedicle, excision of the pseudarthrosis, fixation of the vascularized fibula in situ, anastomosis of the vessels and skin closure. The operation has its problems as follows: � Fixation of the transplanted fibula during surgery. The proximal end could also be left 1 cm distal to the proximal tibial physis to enable later advancement of the rod. Therefore, the rod is placed inside the proximal portion abutting the proximal tibial physis and the distal portion. The rationality of periosteal grafting is that periosteum is a strong bone forming construction. Periosteum is taken from the iliac crest; delicate tissue is denuded from the periosteum and is wrapped around the pseudarthrosis web site, with clean floor facing the graft. Bone grafting from the cancellous bone is first inserted across the nonunion space after which the periosteal graft is wrapped over the graft. Electrical stimulation Electrical stimulation has been used in the remedy of congenital pseudarthrosis of the tibia for the previous twenty years. The addition of electrical stimulation has improved success rates after bone grafting procedures. Use of Williams Rod for Congenital Pseudarthrosis of the Tibia the Williams rod is handed by way of the nonunion website, antegrade by way of the calcaneum after which retrograde into the proximal fragment. Strategy of where the distal end of rod ought to be as suggested by Schoenecker;13-16 � Less than 5 years old: the distal finish of rod should extend well into the body of the calcaneus. Various facilities report between 30% and 50%, however fortuitously, they do reply to remedy by reapplication of the equipment or by solid or brace. Shortening of the limb: this is common and is due to growth retardation of the distal tibial physis, as compared with the normal aspect. Follow-up radiograms present obvious distal migration of the pseudarthrosis-this is brought on by regular growth of the proximal tibial physis and progress retardation of the distal tibial physis. Other causes of shortening of the limb are lack of stimulus of weight bearing and muscular atrophy. The shortening of the affected decrease leg is commonly progressive, leading to larger quantity of shortening. Lengthening at the proximal metaphyseal-diaphyseal degree by both the Ilizarov approach or the De Bastiani callotasis technique has been profitable. Another cause of valgus ankle is the highriding fibular malleolus resulting from pseudarthrosis of the fibula. The distal fibula is attenuated, offering no lateral stability to the ankle joint. Ankle valgus deviation may be prevented by synostosis of the distal metaphysis of the fibula to that of the tibia. When the pseudarthrosis has healed, supramalleolar osteotomy may be carried out to correct the valgus deformity. Progressive anterior angulation of tibia: It occurs as a outcome of delicate tissue contracture posteriorly. In the cystic kind, Tachdjian3 recommends gently curetting the cyst in the tibia and grafting cancellous autogenous bone in the cystic cavities. The posterior bypass bone graft is performed as described for the dysplastic prepseudarthrosis sort. If spontaneous improvement within the angulation is taking place and no dysplastic changes are seen, especially on the apex of the curve, the child could be allowed to start bearing weight usually with out safety. It is likely that no surgical treatment will be needed besides maybe for any residual angulation or shortening in early adolescence. None of the three instances observed by Sharrard developed a fracture after greater than 12 years of follow-up. He also describes two sorts in the benign variety-one affecting both bones, tibia and fibula and different only tibia. This is the classical anterolateral bowing, which ultimately develops into the pseudarthrosis. Osteotomy on the apex of deformity to right the bowing have to be firmly averted since it is extremely prone to lead to pseudarthrosis. The stage of the pseudarthrosis: A more proximal stage of pseudarthrosis, on the junction of the center and decrease thirds of the tibia gives a better outcome than a really distal stage of pseudarthrosis. Prognosis is worse when the pseudarthrosis is associated with neurofibromatosis than with cystic sort. Cases that show tapering and sclerotic bone ends roentgenographically, with extreme angulation and resorb bone graft quickly postoperatively have a poor prognosis. Recommendations of Surgical Treatment Intramedullary nail can be utilized within the treatment of pseudarthrosis with simultaneous Ilizarov ring fixator by passing the nail through subtalar joint. Anterolateral Bowing: Introduction Congenital anterior or anterolateral bowing of the tibia with partial sclerosis and narrowing of its medullary cavity is susceptible to fracture and improvement of pseudarthrosis. Up till now the standard educating was that anterolateral bowing has a foul prognosis compared with the posteromedial bowing which is innocent and corrects itself2,5 and never treat surgically. Progressive type: In the second variety, the medullary cavity is narrowed and will, at one level, be almost obliterated, however the bone texture is in any other case regular. The radiological appearances are of anterolateral bowing of the tibia and fibula at the junction of the center and decrease thirds of the leg with thickening of the posterior and medial cortices. This is a vital difference from neurofibromatosis or fibrous dysplasia in which the deformity slowly increases and spontaneous fracture with pseudarthrosis develops. The New Approach to Anterolateral bowing the lesion within the anterolateral bowing is restricted to a varying length of the tibia in its middle or within the distal third. The proximal and distal metadiaphyseal areas of the tibia are healthy and regular.
Cefadroxil 250 mg buy on line
Some bony procedures to shorten lateral border is carried out along with the delicate tissue process antibiotic 1 discount cefadroxil 250 mg with visa. Although quite a few strategies have been described to shorten the lateral column of the foot antibiotic handbook cefadroxil 250 mg line, following techniques obtain the widest use. The Lichtblau (1973) procedure relies on the assumption that adaptive modifications in the calcaneocuboid joint stop sufficient reduction. The operation, which is recommended for youngsters older than 2 years of age, excises a laterally based mostly wedge from the distal finish of the calcaneus. He claimed that the resected calcaneal articular surface was replaced by fibrocartilage, and he demonstrated mobility on the calcaneocuboid joint as much as 6 years after surgical procedure. Evans, in 1961, described a process consisting of posteromedial releases at the side of lateral calcaneocuboid wedge resection and fusion. Accurate discount of the navicular on the talus is crucial, as the position of the navicular is completely stabilized by the procedure. Only a slim wedge from the calcaneocuboid joint ought to be removed; otherwise, overcorrection into valgus might occur. Goldner achieves the shortening of the lateral side of the foot by resecting a wedge of bone from the cuboid bone. This preserves the joint surfaces and is more practical than decancellation of the bone. The Ilizarov equipment has been combined with varied osteotomies to present distraction osteogenesis for the correction of residual deformity within the clubfoot and different foot deformities. Equinus, varus angulation of the hindfoot, midfoot adductus, and cavus might all be addressed with the use of a circular body and Kirschner wires. The affected person present process corrective procedure by distraction technique must understand that the final functional end result will be a cosmetically improved plantigrade foot which can be considerably stiff. However, varus, equinus, cavus, and overcorrection of the heel have all been reported following clubfoot surgery. Recurrence of one or more elements of the clubfoot deformity might result from an incomplete correction, failure to keep correction, tarsal bone reworking, and irregular scar formation with tethering of tendons, and tarsal coalition that was either iatrogenic or missed through the surgical process. A distinction has to be made between residual, and recurrent or relapsed deformity. Residual implies that though treated nonoperatively or operatively, the deformity was by no means properly corrected. Recurrent or relapsed deformity means that feet which was initially totally corrected clinically and radiologically however developed recurrence of some element of deformity or all elements of the deformity through the period of progress. Residual Forefoot Adduction Residual adduction is normally found on the midfoot and infrequently at the forefoot. Excision of the calcaneocuboid joint cartilage or cuboid enucleation is healthier choices. Cuboid decancellation preserves the articular floor of the cuboid surface proximally and distally and at the identical time decancellation of the bone shortens the lateral column and corrects adduction. Fowler described an opening-wedge osteotomy of the medial cuneiform for the treatment of residual adduction in clubfoot. The Fowler process includes an opening-wedge osteotomy of the medial cuneiform, a radical plantar release, and a switch of the tibialis anterior tendon to the dorsum of the primary metatarsal. McHale and Lenhart described a procedure for an adducted forefoot and a supinated midfoot with hindfoot varus. The procedure combines an opening-wedge osteotomy of the medial cuneiform with a closing-wedge osteotomy of the cuboid, addressing each residual forefoot adduction and midfoot supination. The authors confirmed, in a cadaver model, that a cuboid osteotomy is necessary for correction of midfoot supination. The procedure involves an opening wedge osteotomy of the medial cuneiform and dorsal, truncated wedge osteotomies of the center and lateral cuneiforms. Osteotomy of the center and lateral cuneiforms allows better correction of rotational and cavus deformities. Metatarsal osteotomies are indicated when the adduction deformity originates distal to the navicular. Care should be taken to keep away from harm to the physis of the primary metatarsal by osteotomy or by periosteal stripping; otherwise, shortening of the primary metatarsal might end result. Heyman described release of the tarsometatarsal joints for correction of resistant metatarsus adductus or for treating residual clubfoot adduction deformity. Through a dorsal incision, complete capsulotomies and ligament releases were performed. Dynamic Forefoot Supination Transfer of the tibialis anterior tendon has a task within the treatment of a supple recurrent clubfoot. The prerequisites for profitable switch of the tibialis anterior tendon are totally correctable and supple foot with younger than 6 years. The weak peroneals confirmed by electromyography, and no lively abduction or eversion are common indications for the surgical procedure. This process can additionally be recommended for dynamic supination after nonoperative remedy. Residual Tibial Torsion Supramalleolar osteotomy is required occasionally to appropriate residual tibial torsion in older baby. Complications Both nonsurgical and surgical remedies have completely different sets of issues. Complications Associated with Nonsurgical Treatment Spurious correction: Spurious correction can result in a rocker bottom deformity. The rocker bottom deformity is the outcome of a transverse breach in the midtarsal area. Mostly it occurs when hind foot equinus correction is tried first without tenotomy of tendo Achilles. It is essential to recognize the empty heel, which on palpation reveals a high position of the calcaneus contained in the heel pad. A lateral view radiograph of the foot with maximum dorsiflexion confirms hindfoot equinus and forefoot dorsiflexion with a breach at midtarsal joints. If the complication is recognized, forcible manipulation must be stopped and the foot ought to be maneuvered into plantarflexion in a cast. After few days heel cord release is carried out and additional correction is attempted. If foot continues to break again, short-term fixation of midtarsal joints with K-wire is carried out. Careful padding within the areas the place corrective forces are applied and good molding of plaster cast can stop this drawback. Four kinds of fractures are reported: (i) anterior metaphyseal compression of the distal tibia and fibula, (ii) distal tibial metaphyseal spur brought on by impaction and translation at the epiphyseal plate, (iii) torus fracture of the distal tibial metaphysis within an inch of the epiphyseal plate and (iv) distal fibular fracture. The first three sorts result from forced dorsiflexion of the foot, the fourth kind is produced by exterior rotation stress. If the child cries persistently following manipulation and forged Residual Cavus Inadequate plantar launch and muscle imbalance are both attainable causes of residual cavus deformity.
Cheap cefadroxil 250 mg online
Using an electrocautery antibiotic guide cefadroxil 250 mg order, the tight soft-tissue capsular constructions in the lateral compartment are released intraarticularly on the degree of the tibial minimize infection definition generic cefadroxil 250 mg amex. The authors advocate utilizing an electrocautery to avoid injury to the peroneal nerve, which is often located less than 1 cm from the articular side. Femoral bone cuts are made to attain the right soft-tissue balance in flexion, whereas no gentle tissue releases are accomplished. It is necessary to verify that the tibial reduce floor is perpendicular to the mechanical axis of the tibia in order to get the femoral element rotation appropriate. The block could also be shifted distally and posteriorly to correct a concomitant flexion deformity. One of the 13 patients in their collection developed pseudarthrosis on the osteotomy site and needed to be re-operated for pain. Though all patients were satisfied after the operation, some laxity continued in eight knees. All the sufferers in their collection had full union on the osteotomy website and no scientific proof of mediolateral instability. The authors concluded that laptop navigation while performing lateral femoral epicondylar osteotomy permits precise, managed, quantitative lengthening of lateral constructions and restoration of optimum soft tissue steadiness and alignment. Reference for the distal minimize have to be taken from the medial condyle, else excess bone could also be resected off the medial facet and joint line elevation may occur. If the trial element of femur is in contact with the posterior surface of the lateral condyle, distal defect can be handled as a contained one and could be left alone. The authors found important improvement in knee operate and congruent patellar monitoring in all knees. ToTal Knee arThroplasTy � Peroneal nerve palsy: Peroneal nerve, like different soft tissues on the lateral side of the knee, gets contracted in long-standing valgus knees. Lateral patellar launch may be required to guarantee centralized patellofemoral tracking. Failure to accomplish that may end in a maltracking patella that will adversely have an effect on the function and longevity of the implant. Posterior cruciate ligament results on the flexion space in complete knee arthroplasty. Total knee arthroplasty for profound varus deformity: approach and radiological results in 173 knees with varus greater than 20 degrees. Results of whole knee arthroplasty with medial epicondylar osteotomy to correct varus deformity. Computer-assisted total knee arthroplasty for arthritis with extra-articular deformity. Lateral femoral sliding osteotomy lateral launch in complete knee arthroplasty for a set valgus deformity. Lateral epicondylar osteotomy utilizing pc navigation in total knee arthroplasty for inflexible valgus deformities. Correction of ligament and bone defects in total arthroplasty of the severely valgus knee. Lateral parapatellar approach with tibial tubercle osteotomy for the treatment of non-correctable valgus knee osteoarthritis: a retrospective medical examine knee. The danger of direct peroneal nerve damage using the Ranawat "inside-out" lateral launch approach in valgus total knee arthroplasty. Use of instruments and anatomic bony land- marks allow each surgeon to implant the knee prosthesis in a perfect place. The real talent of a surgeon lies, nevertheless, in doing soft tissue release for balancing the other 3350 TexTbooK of orThopedics and Trauma patellar tendon contracture. Note of this must be taken through the surgical process as eversion of such patella could end result into patella tendon avulsion throughout surgical procedure. Hence, the expertise of a surgeon in acquiring a good gentle tissue balancing decides how nicely a deformed knee will be corrected by him throughout surgery. In this text, I will talk about the principles of soppy tissue balancing within the knee replacement surgical procedure and provides some sensible ideas for a model new surgeon, based mostly on our experiences. Factors in the Preoperation Evaluation of Patients the surgeon needs to assess the extent of deformity and its correctability, clinically and radiologically. Examination in outpatient could not give the correct idea concerning the extent of correctable component of the deformity. Examination underneath anesthesia before surgery offers the surgeon the precise amount of flexion deformity the knee has and the way much the delicate tissues release is necessary in the course of the surgery. This signifies the amount of lateral opening and stretching out of the collateral ligament on convex aspect. This also exhibits the amount of lateral translation of the tibia, which is an indication of dynamic instability of the knee. In presence of significant lateral translation or extreme opening up of convex side of the joint, potential use of constrained type of knee prosthesis needs to be thought-about, as the lateral gentle tissues could additionally be too lax. The angular correction stress view of the knee indicates the correctability of the knee deformity in coronal plane. If the surgeon fails to realize this fact, he might find yourself doing over-release of the ligaments and create an unstable knee. The shoot by way of lateral X-ray of the knee is helpful to identify the presence of osteophytes in the posterior part of the knee joint. These osteophytes cause tenting of the posterior capsule and result in flexion deformity. The second factor visualized in lateral view is the place of patella and the ratio of patella height to patella tendon length. The medial gentle tissue flap is elevated with sharp dissection from medial tibial condyle. This medial soft tissue flap includes superficial and deep collateral ligament, and the peripheral rim of medial meniscus. While reflecting this flap, the tibia is progressively rotated externally by the assistant until the posteromedial corner of the tibial plateau is exposed. Care must be exercised in patient with extreme medial tibial bone loss (in extreme varus deformities) while doing the dissection of soft tissues in a posteromedial nook of tibia. The bony loss may cause decreasing of the joint line up to the attachment of medial hamstring which can get indifferent in the course of the medial gentle tissue dissection. The medial meniscus is excised leaving the peripheral millimeter of its rim intact to preserve menisco-tibial and menisco-femoral ligaments. The medial tibial osteophytes are removed at this stage to cut back the tenting they trigger to medial gentle tissue envelop. A proper angle Hohmann retractor positioned within the lateral paratibial gutter retracts patella and infra-patella pad out of the way in which. The lateral meniscus is excised along its whole periphery as much as the posterior attachment.